Psych · foundations
Descriptive psychopathology and phenomenology
Also known as Phenomenology psychiatry · Descriptive psychopathology · Formal thought disorder · First-rank symptoms · Schneiderian symptoms · Self-disorders · Passivity phenomena
Exam-exhaustive fellowship atlas on descriptive psychopathology and phenomenology — disorders of perception, thought form and content, speech, mood and affect, self and agency (including first-rank symptoms and self-disorders), cognition, and motor behaviour; MSE language; multi-board exam pearls. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
12 MCQs with explanations
Target exams
Red flags
Overview and definition
Descriptive psychopathology is the technical language of psychiatry: a set of operational terms for how mental phenomena present, independent of any single aetiological theory. It underwrites the Mental State Examination (MSE), research scales, and viva answers. Phenomenology in this curriculum sense is not armchair philosophy alone — it is the skilled description of lived form (what it is like for the person) before causal speculation. [15][17]
| Construct | What it answers | What it is not |
|---|---|---|
| Descriptive psychopathology | What is the form of the experience? | A diagnosis code |
| Phenomenological understanding | How is the experience structured for the subject? | Proof of aetiology |
| Explanatory psychopathology | Why might this occur (neurobiology, psychodynamics, social)? | A substitute for accurate description |
| Classification (DSM-5-TR / ICD-11) | Does this pattern meet criteria? | A complete map of form |
Andreasen warned that criterion-check approaches can erode phenomenological skill if trainees never learn form distinctions — a live exam risk when candidates list symptoms without defining them. [15]
Classification of domains
A fellowship domain set that maps cleanly onto MSE teaching: [17]
- Perception — hallucination, illusion, pseudohallucination, hypnagogic/hypnopompic phenomena
- Thought form (process) — how thinking is linked and expressed
- Thought content — what thinking is about (delusions, overvalued ideas, obsessions, risk ideas)
- Speech and language — the audible vehicle of form
- Mood and affect — subjective vs observed emotion
- Self and agency — depersonalisation, passivity, self-disorders
- Cognition — orientation, attention, memory, executive function
- Motor behaviour — psychomotor change and catatonia
These are descriptors. Diagnosis follows after history, risk, organic exclusion, and criteria — never from a single exotic term. [4][5][17]
Epidemiology and clinical stakes
Formal thought disorder, first-rank-like experiences, and auditory verbal hallucinations are transdiagnostic to varying degrees; Mellor's classic empiric work measured frequency of first-rank symptoms in admitted schizophrenics, but later evidence dismantled pathognomonic status. [3][4][5]
Misapplied language carries risk: calling a cultural belief a delusion; missing delirium because visual hallucinations were "psychologised"; or treating first-rank symptoms as automatic schizophrenia. High-stakes arenas include first-episode assessment, forensic notes, CASC stations, and any documentation read in tribunals. [4][5][18]
Pathophysiology and phenomenological models
Form before mechanism
Always describe form first. Mechanism talk that cannot be anchored to a named phenomenon fails viva. High-level models examiners accept: [7][11]
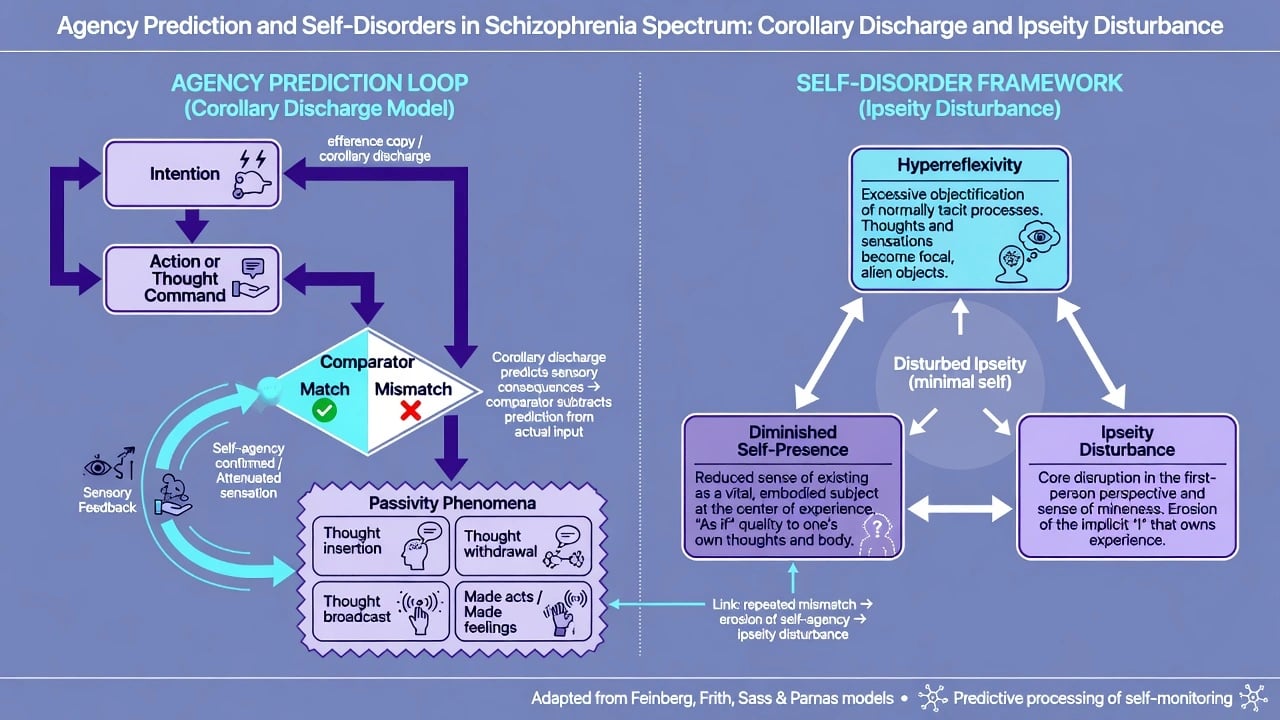
- Agency / corollary-discharge style accounts — mismatch between predicted and actual sensory consequences of self-generated acts or thoughts is one framework for passivity phenomena and some auditory verbal hallucinations (conceptual, not a single proven lesion).
- Language and associative network disruption — formal thought disorder (derailment, incoherence, neologisms). [1][2]
- Positive vs negative process thinking (Crow) — historical framing that positive phenomena (e.g. delusions, hallucinations) and negative phenomena may reflect more than one disease process within the schizophrenia concept. [11]
- Self-disorder (ipseity) model (Sass and Parnas) — disturbance of minimal self (hyperreflexivity, diminished self-presence) as a core organising phenomenology of schizophrenia-spectrum experience. [7]
Organic states (delirium, encephalitis, intoxication, sensory deprivation) rewrite perception and attention and can mimic primary psychosis — mechanism here is medical until proven otherwise. [17]
Clinical presentation by domain
Disorders of perception
| Term | Core form | Exam discriminator |
|---|---|---|
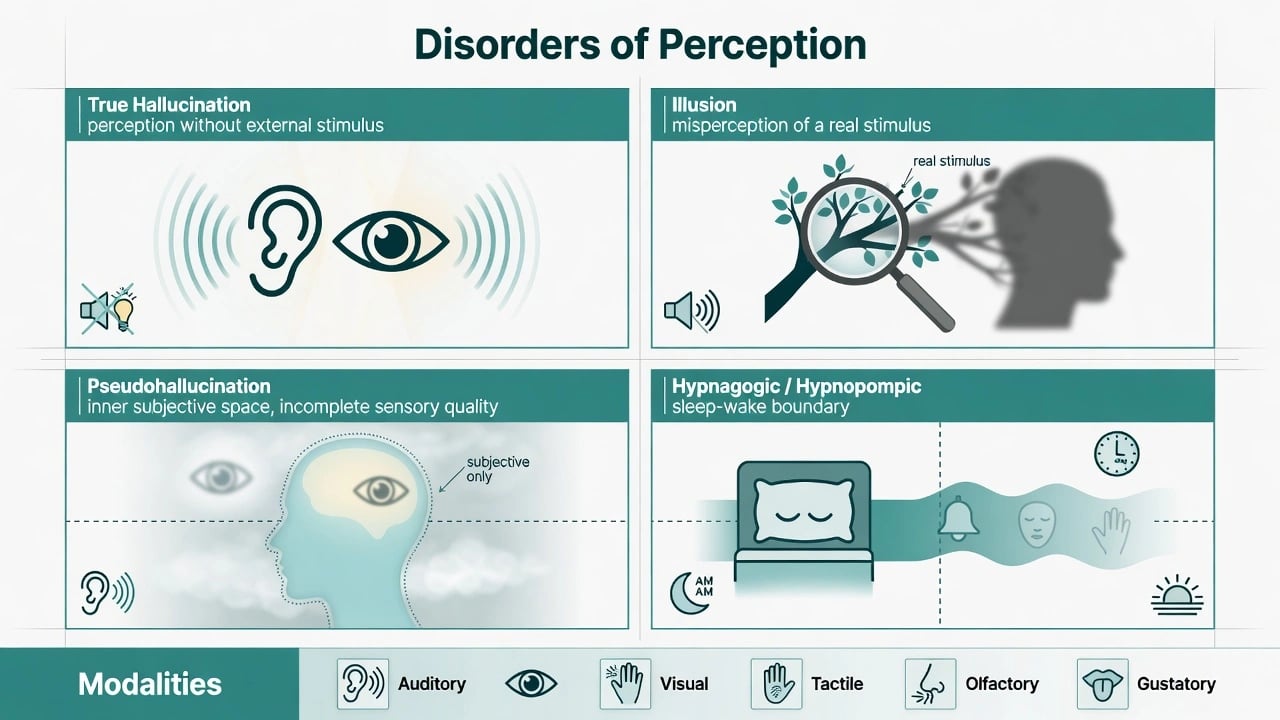
| True hallucination | Perception-like experience without corresponding external stimulus | Full sensory quality; classically experienced in external space (definitional debates exist — document the patient's report) |
| Illusion | Misinterpretation of a real external stimulus | Real stimulus present (e.g. coat as person) |
| Pseudohallucination | Percept-like but incomplete sensory quality and/or located in subjective inner space | Not identical to "insight present"; do not use as a throwaway label |
| Hypnagogic / hypnopompic | At sleep onset / on waking | Boundary with normality; not automatically psychotic |
Modalities: auditory, visual, tactile, olfactory, gustatory. For auditory verbal hallucinations, record person (second/third), content (including commands), frequency, emotional impact, perceived power, resistance, and acting. Command content is a risk feature, not an automatic detention criterion. [17]
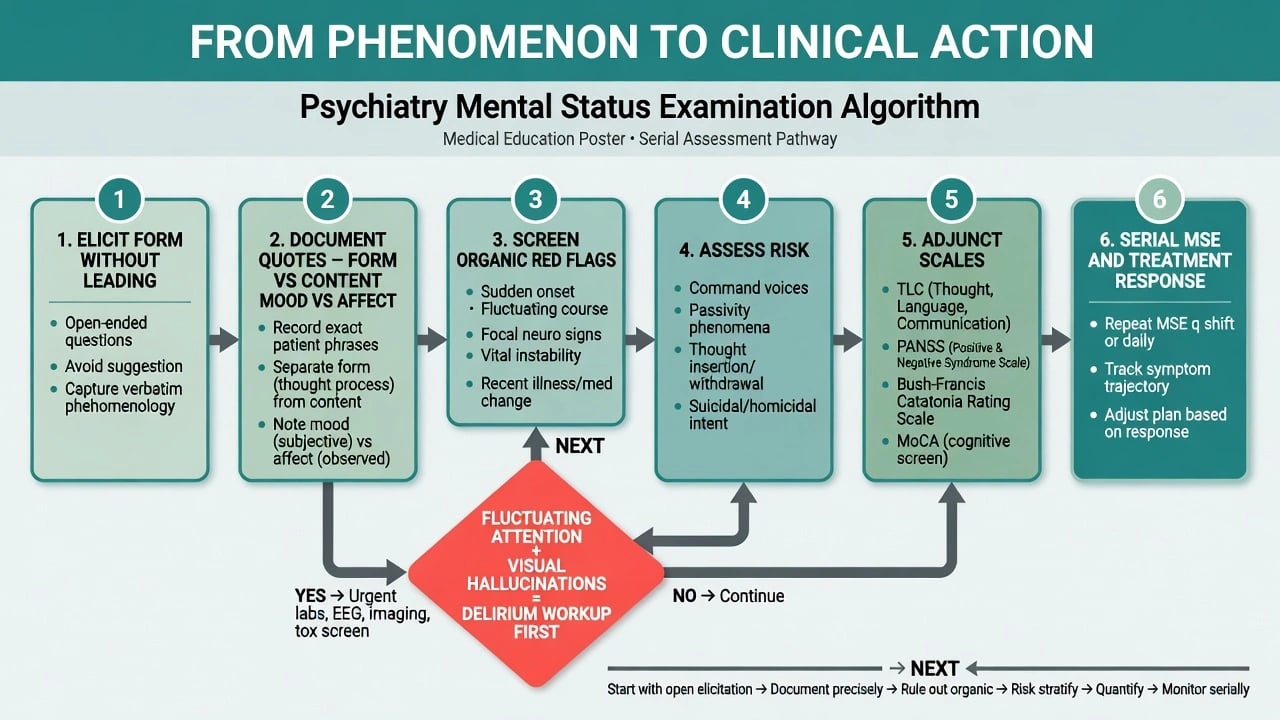
Visual predominance plus fluctuating attention shifts probability toward organic states (e.g. delirium) until excluded. [17]
Thought form (process)
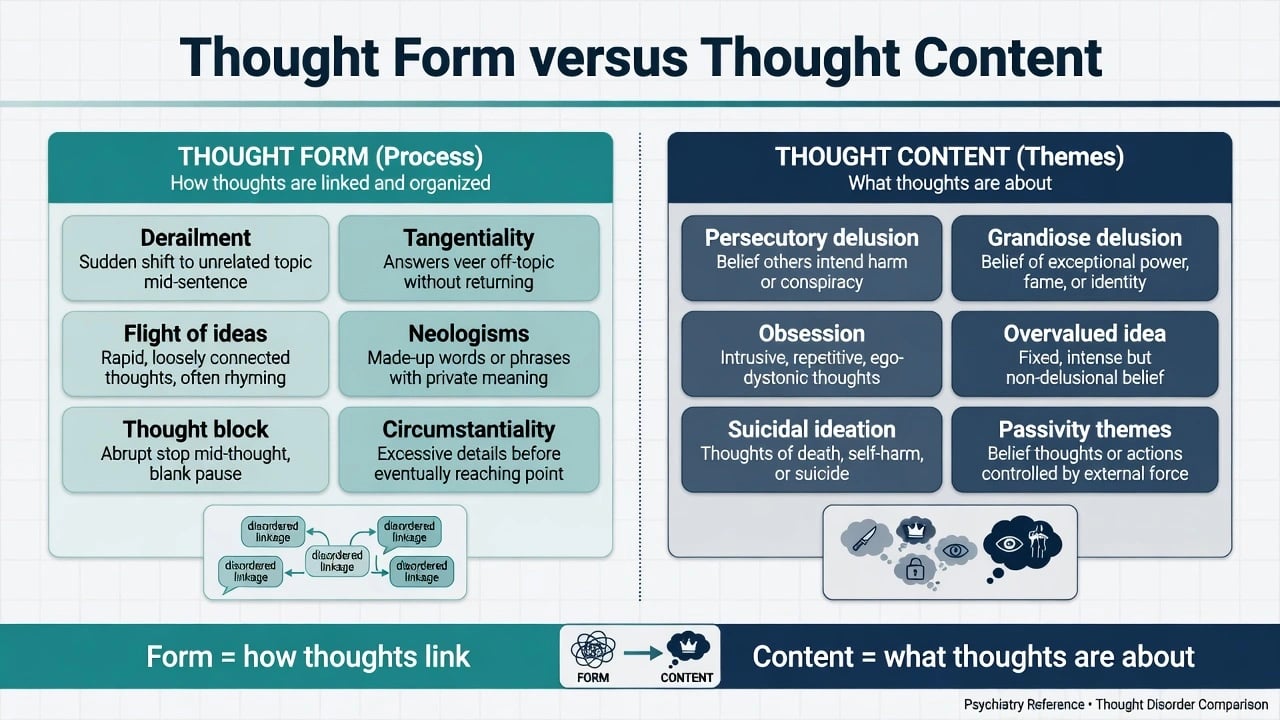
Andreasen's Thought, Language, and Communication (TLC) system remains the reliability gold standard for teaching definitions: poverty of speech, poverty of content, pressure, distractible speech, tangentiality, derailment, incoherence, illogicality, clanging, neologisms, word approximations, circumstantiality, loss of goal, perseveration, echolalia, blocking, stilted speech, self-reference, and related terms. [1][2]
Flight of ideas (classically manic): rapid sequential associations that often retain understandable links (clang, pun, theme) with pressure of speech. Derailment / loosening: topic shifts lose goal-directed bridges. Tangentiality: answers oblique, never reach the point. Thought block: abrupt cessation subjectively experienced as interruption. [1][2]
TLC abnormalities are not exclusive to schizophrenia; diagnostic significance is probabilistic and context-bound. [2]
Thought content
- Delusion — fixed false belief held with conviction, not amenable to reason, out of keeping with cultural/educational background (classical teaching triad; cultural caveat is mandatory).
- Overvalued idea — emotionally overinvested belief short of delusional fixity.
- Obsession — intrusive, ego-dystonic, typically resisted; insight usually better than in delusion.
- Bizarre delusion — definitions vary; reliability of "bizarre" is imperfect — examiners reward caution. [14]
Types of delusional theme: persecutory, referential, grandiose, somatic, nihilistic, erotomanic, jealous, religious, and control/passivity themes. Record onset, systematisation, mood congruence, and distress, not only the theme label. [14][17]
Speech
Document rate, rhythm, volume, prosody, latency, spontaneity, dysarthria, mutism, and pressure. Speech is observed behaviour; thought form is inferred from speech and writing. Do not equate non-native language, aphasia, or deafness-related communication with formal thought disorder. [1][17]
Mood versus affect
Mood = subjective emotional state (quote the person). Affect = observed emotional expression: range (full, restricted, blunted, flat), reactivity, appropriateness, congruence with stated mood, and lability. [17]
| Pitfall | Correction |
|---|---|
| Writing only "affect low" | Quote mood; describe affect range and congruence |
| Calling EPS hypomimia "blunted affect" only | Note medication/motor contribution |
| Equating restricted affect with autism alone | Need developmental history |
Self and agency
Depersonalisation — detachment from self; derealisation — detachment from surroundings. The Cambridge Depersonalization Scale operationalises severity measurement. [16]
Passivity / made experiences (classic Schneiderian cluster): thought insertion, thought withdrawal, thought broadcast; made feelings, made impulses, made acts; somatic passivity. These are disorders of ownership and agency, not merely "intrusive worries." [3][4]
Self-disorders (Sass/Parnas; EASE instrument): anomalous self-experience across domains of cognition, stream of consciousness, self-awareness, presence, corporeality, demarcation, and existential orientation — richer than a yes/no first-rank checklist. [7][8]
Cognition
Describe arousal/consciousness, orientation, attention, memory, language, and executive function in free text. Scales (e.g. MMSE/MoCA in clinical practice) are adjuncts, not replacements for descriptive cognitive MSE language. Fluctuating attention is an organic alarm. [17]
Motor behaviour and catatonia
Psychomotor retardation, agitation, mannerisms, stereotypies, tics, and catatonic signs. The Bush-Francis Catatonia Rating Scale provides a standardised examination and item set (e.g. excitement, immobility, mutism, staring, posturing, grimacing, echopraxia/echolalia, stereotypy, mannerisms, negativism, waxy flexibility, automatic obedience). [10]
Differential diagnosis with discriminators
| Confusion pair | Discriminators |
|---|---|
| Hallucination vs illusion | External stimulus absent vs present |
| Delusion vs overvalued idea | Fixity, incorrigibility, cultural fit, functional impact |
| Delusion vs obsession | Ego-syntonic conviction vs ego-dystonic resistance |
| Derailment vs flight of ideas | Lost links vs rapid retained links + mood/pressure context |
| Thought insertion vs OCD intrusion | Alien ownership/agency vs recognised as own unwanted thought |
| Blunted affect vs EPS vs depression | Motor exam, history of antipsychotics, subjective mood |
| Passivity vs dissociation | Full clinical context; trauma history; not automatic equivalence |
| Primary psychosis vs delirium | Attention fluctuation, arousal, visual bias, medical signs |
Clinical and bedside assessment
- Frame — privacy, safety, role, permission to take notes.
- Open narrative — free speech exposes form and content.
- Focused elicitation without leading — "Have you had experiences that are hard to explain?" before "Do you hear voices?"
- Explore delusions without collusion or humiliation — understand function and distress; do not argue metaphysics.
- Separate documentation columns in your mind — form vs content; mood vs affect; observation vs inference.
- Quote key phrases; timestamp the MSE.
- Insight — use David's multidimensional model (awareness of illness; relabelling of symptoms; treatment attitude). Components dissociate. [9]
- Culture — use Cultural Formulation Interview principles when explanatory models could be misread as pathology. [18]
Investigations and structured instruments
When phenomenology forces organic work-up: first episode; late or atypical onset; fluctuation; fever; seizure; focal neurology; catatonia; new visual hallucinations; severe new cognitive change; substance unknowns. [10][17]
| Instrument | Phenomenological role |
|---|---|
| TLC terms (Andreasen) | Reliable formal thought disorder vocabulary [1] |
| SANS conceptual framework | Negative symptom domains [12] |
| PANSS | Dimensional positive/negative/general ratings [13] |
| Bush-Francis CRS | Catatonic motor phenomenology [10] |
| Cambridge Depersonalization Scale | Depersonalisation severity [16] |
| EASE | Anomalous self-experience interview structure [8] |
Collateral history is an investigation of longitudinal form when the cross-section is incomplete. [17]
Acute / emergency interface
Phenomena that change management now: [10][17]
- Command hallucinations with high perceived power and low resistance, or history of acting on them
- Severe agitation or violence risk content
- Catatonic compromise (nutrition, autonomy, autonomic instability risk)
- Delirium signature (fluctuating attention, altered consciousness)
Legal status uses jurisdiction-specific mental health law; descriptive terms document grounds — they are not themselves section numbers (never invent statutes). Capacity remains a decision-specific functional assessment, related to but not identical with insight. [9]
Definitive use of descriptive skill
Precise description guides treatment choice only indirectly (e.g. catatonia pathway vs primary psychosis pathway) but guides monitoring directly: serial MSE tracks which domains improve first. Psychoeducation and CBT for psychosis both require accurate form language. Teaching programmes that neglect phenomenology produce checklist clinicians. [15][17]
Specific scenarios
Schneider first-rank symptoms — history and modern status
Kurt Schneider emphasised a set of experiences he considered highly characteristic of schizophrenia in the absence of organic disease (classic teaching lists include audible thoughts, voices arguing/commenting, thought insertion/withdrawal/broadcast, and passivity phenomena). Mellor quantified frequency in clinical samples. [3][6]
Modern position for exams: historically foundational, diagnostically non-pathognomonic. Nordgaard and colleagues and Peralta and Cuesta show limited diagnostic value and no clear superiority of clinical validity versus other delusions/hallucinations. DSM editions have transformed Schneiderian concepts unevenly — know the history, do not weaponise FRS as a gold test. [4][5][6]
Mania vs schizophrenia-spectrum thought disorder
Flight of ideas with elevated/irritable mood and pressure of speech favours mania; derailment with bizarre content and passivity may favour schizophrenia-spectrum — but mixed states and schizoaffective presentations exist; do not over-call from form alone. [1][2]
Negative symptoms and affective blunting
SANS foundations distinguish affective flattening, alogia, avolition-apathy, anhedonia-asociality, and attention — still examinable vocabulary even when using PANSS in practice. [12][13]
Catatonia
Treat catatonic signs as a syndrome across diagnoses (mood, psychotic, medical, NMS overlap). Use structured examination (Bush-Francis) rather than a single "looks catatonic" impression. [10]
Self-disorders vs dissociation
Self-disorder research targets schizophrenia-spectrum ipseity disturbance; dissociative phenomena have overlapping surface language (detachment) but different clinical packages. Do not force synonymy in viva — compare form, history, and course. [7][8][16]
Complications and pitfalls
- First-rank symptoms treated as pathognomonic. [4][5]
- Leading questions manufacturing "voices."
- Collusion or humiliating confrontation with delusions.
- Pejorative notes ("manipulative," "attention-seeking") instead of behaviour + quotes.
- Equating poor insight with incapacity. [9]
- Cultural pathologising without CFI-informed exploration. [18]
- Confusing mood/affect and form/content.
- Calling every strong belief "bizarre" despite poor reliability of that adjective. [14]
- Neglecting organic signatures while collecting exotic labels.
Prognosis and disposition
Disposition depends on risk, supports, treatability, and legal thresholds — not on the raw number of first-rank items. Serial descriptive MSE is the outcome language of inpatient and community care: which domains changed, which remain. Handover should be form-focused, quoted, and timestamped. [4][17]
Special populations
| Population | Phenomenological caveats |
|---|---|
| Children / adolescents | Imaginary companions and developmental fantasy vs hallucination; suggestibility; caregiver collateral |
| Older adults | Sensory impairment, Charles Bonnet-type visual phenomena, delirium risk |
| Intellectual disability | Baseline comparison; behavioural equivalents; avoid diagnostic overshadowing |
| Non-English speakers | Interpreter mandatory before diagnosing thought disorder from speech |
| Cultural / Indigenous contexts | Explanatory models; CFI; avoid pathologising normative spiritual experience [18] |
| Perinatal | Content themes involving infant; shame may suppress disclosure of risk ideas |
Evidence, guidelines, and regional notes
- Thought disorder: Andreasen TLC reliability and diagnostic significance remain core citations. [1][2]
- First-rank symptoms: Mellor empiric frequency; Nordgaard diagnostic status review; Peralta/Cuesta modern invalidation of pathognomonic claim; 2024 historiography of Schneider vs DSM wording. [3][4][5][6]
- Self: Sass/Parnas ipseity model; EASE. [7][8]
- Insight: David multidimensional model. [9]
- Motor: Bush-Francis catatonia examination. [10]
- Positive/negative framing: Crow; SANS foundations; PANSS. [11][12][13]
- Phenomenology skill risk under DSM culture: Andreasen 2007. [15]
- Culture: CFI evidence base. [18]
FRANZCP expects consultant-level descriptive vocabulary in MSE, formulation, and viva. MRCPsych Paper A/B tests definitions (illusion vs hallucination; FRS lists; thought disorder terms); CASC tests elicitation skill. ABPN expects interview description and organic discrimination. MD/DNB / NEET-SS favour classical definitions plus Schneider history. Regional clinical guidelines (RANZCP, NICE, APA) set treatment pathways for syndromes — they do not replace form description. [15][17]
Exam pearls
- FRS: historically important, not pathognomonic. [4][5]
- Always separate mood/affect and form/content. [1][17]
- Flight of ideas retains links; derailment loses them. [1]
- Thought insertion is an agency/ownership disorder, not ordinary worry. [3][7]
- Command AVH: content, power, resistance, acting — risk formulation, not automatic detention. [17]
- "Bizarre" has imperfect reliability — define what you mean. [14]
- Quote the patient; timestamp; never invent Mental Health Act section numbers. [17]
- Organic first if fluctuation + inattention + visual hallucinations. [17]
- Insight is three-dimensional (David), never only good/poor. [9]
- Culture first when content is religious or communal. [18]
PERCEPT-MAP domains
References
- [1]Andreasen NC Thought, language, and communication disorders. I. Clinical assessment, definition of terms, and evaluation of their reliability Arch Gen Psychiatry, 1979.PMID 496551
- [2]Andreasen NC Thought, language, and communication disorders. II. Diagnostic significance Arch Gen Psychiatry, 1979.PMID 496552
- [3]Mellor CS First rank symptoms of schizophrenia. I. The frequency in schizophrenics on admission to hospital. II. Differences between individual first rank symptoms Br J Psychiatry, 1970.PMID 5479324
- [4]Nordgaard J, Arnfred SM, Handest P, et al. The diagnostic status of first-rank symptoms Schizophr Bull, 2008.PMID 17562695
- [5]Peralta V, Cuesta MJ Schneider's first-rank symptoms have neither diagnostic value for schizophrenia nor higher clinical validity than other delusions and hallucinations in psychoses Psychol Med, 2023.PMID 32943125
- [6]Moritz S, Gawęda Ł, Carpenter WT, et al. What Kurt Schneider Really Said and What the DSM Has Made of it in Its Different Editions: A Plea to Redefine Hallucinations in Schizophrenia Schizophr Bull, 2024.PMID 37738451
- [7]Sass LA, Parnas J Schizophrenia, consciousness, and the self Schizophr Bull, 2003.PMID 14609238
- [8]Parnas J, Møller P, Kircher T, et al. EASE: Examination of Anomalous Self-Experience Psychopathology, 2005.PMID 16179811
- [9]David AS Insight and psychosis Br J Psychiatry, 1990.PMID 2207510
- [10]Bush G, Fink M, Petrides G, et al. Catatonia. I. Rating scale and standardized examination Acta Psychiatr Scand, 1996.PMID 8686483
- [11]Crow TJ Molecular pathology of schizophrenia: more than one disease process? Br Med J, 1980.PMID 6101544
- [12]Andreasen NC The Scale for the Assessment of Negative Symptoms (SANS): conceptual and theoretical foundations Br J Psychiatry Suppl, 1989.PMID 2695141
- [13]Kay SR, Fiszbein A, Opler LA The positive and negative syndrome scale (PANSS) for schizophrenia Schizophr Bull, 1987.PMID 3616518
- [14]Spitzer RL, First MB, Kendler KS, et al. The reliability of three definitions of bizarre delusions Am J Psychiatry, 1993.PMID 8494062
- [15]Andreasen NC DSM and the death of phenomenology in america: an example of unintended consequences Schizophr Bull, 2007.PMID 17158191
- [16]Sierra M, Berrios GE The Cambridge Depersonalization Scale: a new instrument for the measurement of depersonalization Psychiatry Res, 2000.PMID 10725532
- [17]Daza C, Mauriziano C, Liberona A, et al. Mapping the Mental Status Examination: Insights from a Scoping Review of Popular Psychiatry Textbooks Acad Psychiatry, 2025.PMID 40495096
- [18]Lam PC, Lewis-Fernández R, Aggarwal NK The Cultural Formulation Interview: Building the Case for Cultural Competence in Clinical Care Psychiatr Serv, 2023.PMID 36722093