Psych · Foundations — EEG and clinical neurophysiology
EEG and clinical neurophysiology in psychiatry
Also known as EEG in psychiatry · Clinical neurophysiology psychiatry · Electroencephalography psychiatric practice · qEEG psychiatry · Event-related potentials psychiatry · P300 MMN schizophrenia · Nonconvulsive status epilepticus psychiatry · Clozapine EEG seizures
Exam-exhaustive fellowship foundation on EEG and clinical neurophysiology for psychiatrists: indications and yield, frequency bands and report literacy, NCSE and continuous EEG, psychotropic and clozapine effects, ERPs (P300/MMN) and qEEG as research tools, anti-NMDA patterns, and epilepsy–psychiatry interface essentials. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
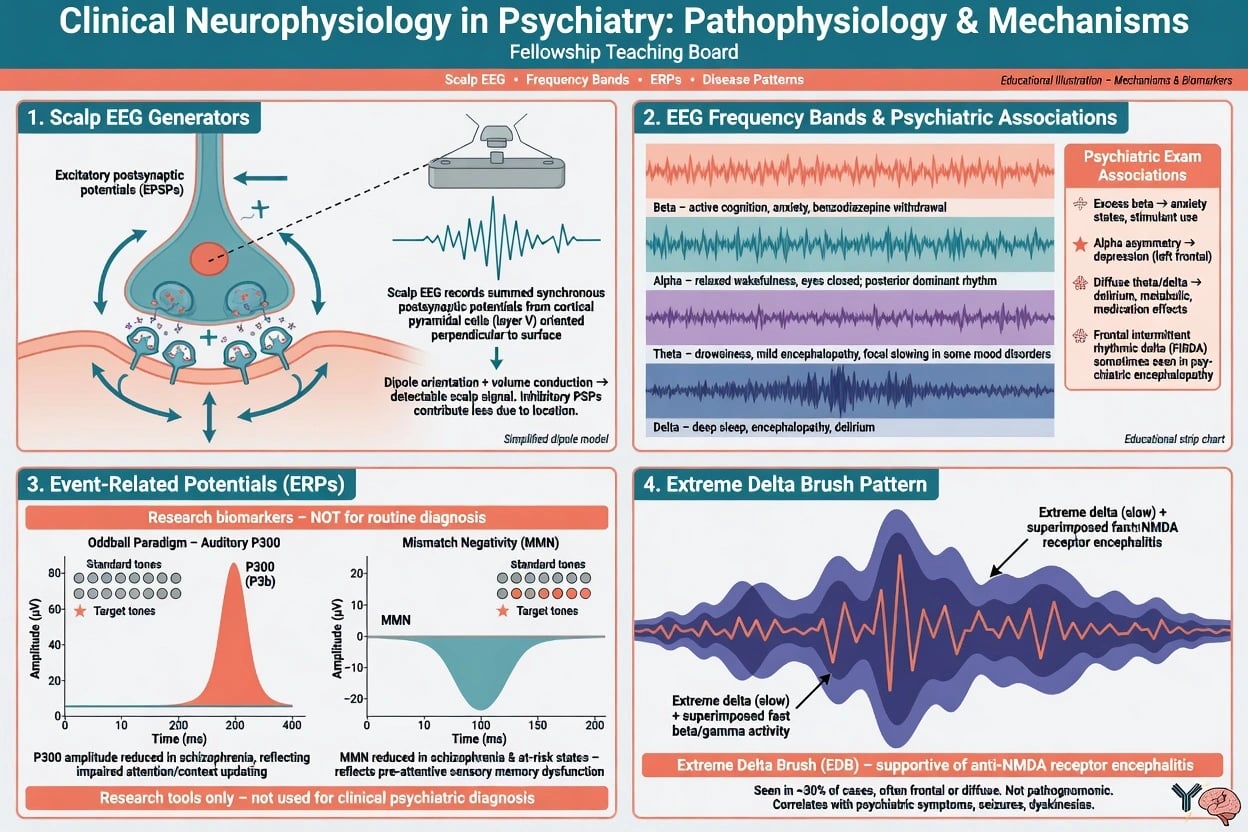
Clinical electroencephalography (EEG) records summed postsynaptic potentials from cortical pyramidal populations at the scalp. Temporal resolution is excellent; spatial resolution is coarse. In psychiatry the fellowship task is indication literacy, report translation, and knowing what EEG cannot do — not technician-level montage design. [1][2]
Clinical neurophysiology for the psychiatrist also includes continuous/ICU EEG, video-EEG for spell classification, and awareness of event-related potentials (ERPs) and quantitative EEG (qEEG) as research or specialised tools rather than routine DSM/ICD diagnostic codes. [5][12]
Service audits show EEG is frequently requested on psychiatric wards, often for possible organic syndromes, with many non-specific abnormal results when pre-test probability is low — so clinical question quality drives value. [1][3]
Classification: bands, recordings, and report language
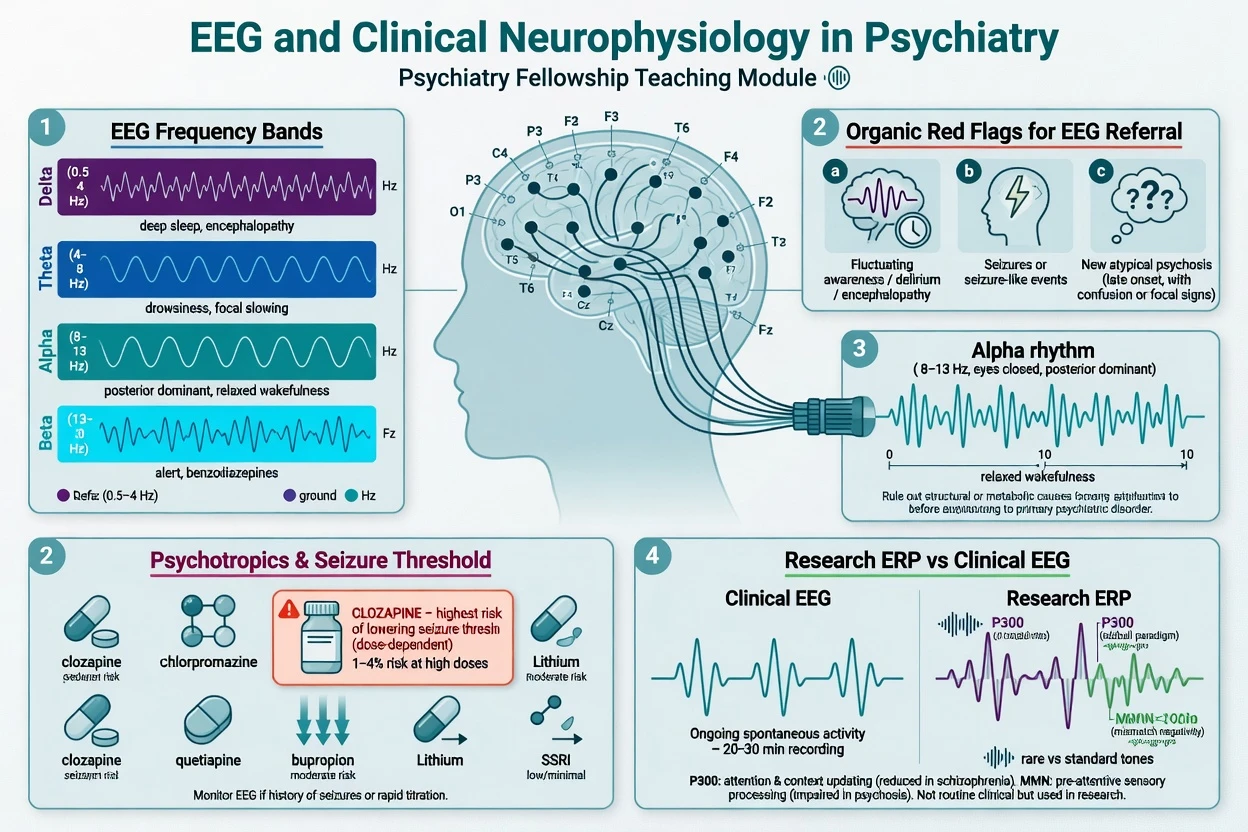
| Band | Approximate frequency | Exam-facing associations |
|---|---|---|
| Delta | less than 4 Hz | Deep sleep; pathological when diffuse awake (encephalopathy) |
| Theta | 4–7 Hz | Drowsiness; diffuse excess awake → non-specific slowing |
| Alpha | 8–12 Hz | Posterior dominant rhythm in relaxed wakefulness |
| Beta | 13–30 Hz | Alertness; often enhanced by benzodiazepines and barbiturates |
| Gamma | greater than 30 Hz | Research interest; not routine psychiatric report language |
| Frequency scaffold for viva answers. [1][4] |
Recording types examiners expect you to name. Routine outpatient EEG (typically under 1 hour with activation procedures); sleep-deprived or prolonged EEG when short-record yield is insufficient; ambulatory EEG for intermittent community events; video-EEG telemetry as gold standard for characterising epileptic versus psychogenic non-epileptic spells; continuous EEG in critically ill patients when electrographic seizures or NCSE are suspected. [5][7]
Activation procedures (hyperventilation, intermittent photic stimulation, sleep) increase yield for some epilepsies; they do not turn EEG into a screening test for primary mood disorders. [2][4]
Epidemiology and yield in psychiatric services
Classic and modern service literature agrees: EEG is most useful when the question is organic differential (delirium/encephalopathy, seizure-related syndromes, atypical first presentations), not when used as a shotgun test for every depressive episode. [1][2][3]
Practical teaching points for multi-board exams: yield rises with new-onset psychosis with atypical features, fluctuating or progressive cognitive change, seizure symptoms, and rapid mood or behaviour change with medical concern; many psychiatric EEG requests return normal or non-specific slowing that still helps redirect systemic work-up rather than over-diagnosing epilepsy; epilepsy populations carry high psychiatric comorbidity so EEG literacy is part of consultation-liaison competence. [1][3][4]
Pathophysiology and mechanism anchors
Scalp EEG is dominated by cortical synaptic currents, not axonal spikes. Diffuse slowing reflects widespread cortical/thalamocortical dysfunction (metabolic, toxic, infectious, hypoxic, neurodegenerative stages). Focal slowing raises structural concern and should trigger imaging correlation. Epileptiform discharges reflect hypersynchronous cortical networks; they are not a diagnosis of schizophrenia. [1][6]
Psychotropic effects. Antipsychotics differ in EEG disruption; clozapine produces EEG abnormalities more often than many other agents and carries clinically important dose-related seizure risk documented in large series. [9][10] Benzodiazepines commonly increase beta activity — a medication signature, not "anxiety on the trace." FDA-summary analyses of clinical trials inform relative seizure incidence across psychotropic classes and temper exaggerated fears about all antidepressants equally. [11]
ERPs. The classic oddball P300 (Sutton) indexes attention/context updating; reduced amplitude is a robust research finding in schizophrenia samples but is not a bedside diagnostic criterion. [12] Mismatch negativity (MMN) indexes automatic auditory deviance detection; meta-analysis shows robust MMN reduction in chronic schizophrenia and links conceptually to NMDA/glutamate models — again research-grade, not a DSM replacement. [12]
Anti-NMDA encephalitis. Psychiatric and behavioural presentations are common; extreme delta brush is a distinctive EEG pattern described in adults with anti-NMDA receptor encephalitis and is supportive when present, not pathognomonic. Diagnosis rests on clinical syndrome, antibodies, and multidisciplinary work-up. [13][14]
Clinical presentation that should change your EEG threshold
Raise pre-test probability when history or MSE shows fluctuating attention or arousal, staring spells, or unexplained mutism; new psychosis with seizures, fever, autonomic instability, or focal neurology; catatonia where medical or organic differentials remain open (including NCSE mimics); known epilepsy with new psychiatric syndrome timed to seizures (peri- or postictal); fluctuating or rapid cognitive decline; or when spell characterisation is needed for possible psychogenic non-epileptic seizures. [2][4][6]
NCSE can look psychiatric. Nonconvulsive status may present with confusion, behavioural change, or reduced responsiveness without tonic-clonic movements. Salzburg-style criteria formalise combining EEG patterns with clinical context for NCSE diagnosis. [6] Continuous EEG detects far more electrographic seizures than brief spot recordings in critically ill populations. [5][7]
Differential diagnosis (discriminators)
| Problem | Discriminators | Neurophysiology role |
|---|---|---|
| Primary psychosis | Clear sensorium between symptoms; no fever/focal signs | EEG selective, not universal |
| Delirium/encephalopathy | Fluctuating attention, medical drivers | Diffuse slowing common; treat cause |
| NCSE | Impaired awareness, subtle motor, medical setting | Urgent/continuous EEG; treat |
| Postictal psychosis | Seizure cluster → lucid interval → psychosis | Clinical diagnosis; EEG may show postictal change |
| Anti-NMDA encephalitis | Subacute psychiatric + movement/autonomic/seizure features | EEG often abnormal; extreme delta brush if present |
| PNES vs epilepsy | Inconsistency of events; eyes closed typical patterns vary | Video-EEG gold standard |
| Drug effect | Clozapine, benzos, toxins | Correlate medications with report |
| Discriminators for fellowship differentials. [6][9][13][14] |
Routine psychiatric EEG
- Best when organic red flags present
- Often normal or non-specific slowing
- Not a screen for MDD or GAD
- Write a clear clinical question
Continuous / critical-care EEG
- Suspected NCSE or unexplained AMS
- Detects electrographic seizures missed clinically
- Uses standardised critical-care terminology
- Neurology/ICU partnership
ERP / qEEG research tools
- P300 and MMN group findings
- qEEG spectral maps experimental/specialist
- Not standalone DSM diagnosis
- Do not overclaim in court or consent
Assessment before you order
Structure assessment around history (onset, fluctuation, seizures, head injury, substances, infection symptoms, pregnancy); medications and timing (clozapine dose and plasma level if available, bupropion, lithium, benzodiazepines, antiseizure medicines, recent withdrawals); full MSE with attention tests, focal neurology, vital signs, and catatonic signs; a request form that states the clinical question (for example exclude NCSE versus encephalopathy in fluctuating mutism on clozapine); and collateral including witness descriptions of spells. Phone video can help but does not replace video-EEG when diagnosis is high-stakes. Risk of suicide or violence is not measured by EEG — neurophysiology never replaces structured risk assessment. [1][3][9]
Investigations: what to order and what not to order
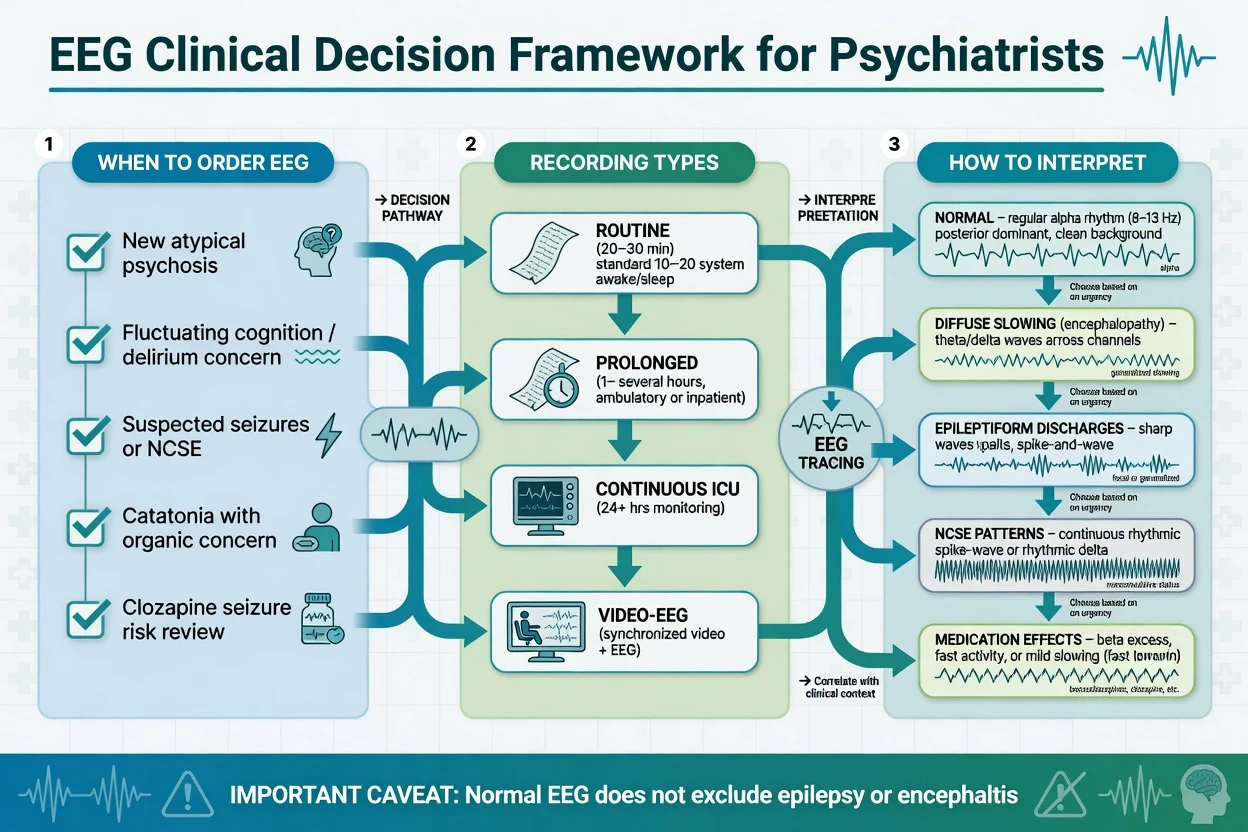
Reasonable psychiatric indications (not exhaustive): atypical first-episode psychosis with organic concern; fluctuating cognition; suspected seizures or NCSE; unexplained catatonia with medical differentials; selected monitoring contexts in high-seizure-risk pharmacology; spell characterisation pathway toward video-EEG. [2][4]
Continuous EEG indications in the critically ill are consensus-based (coma, unexplained AMS, seizure detection, treatment titration of refractory status pathways) — psychiatrists on CL/ICU teams must know when to escalate. [5][7][8]
Pairing tests. Suspected encephalitis: MRI, LP (when safe), autoimmune encephalitis panel including NMDA receptor antibodies, plus EEG — EEG is supportive, not sufficient alone. [13][14]
Not routine: commercial qEEG "brain maps" to diagnose ADHD, depression, or to select antidepressants as a sole decision tool in ordinary clinics. Historical neurometric claims require evidence-based humility in viva. [1][12]
Acute management (neurophysiology interface)
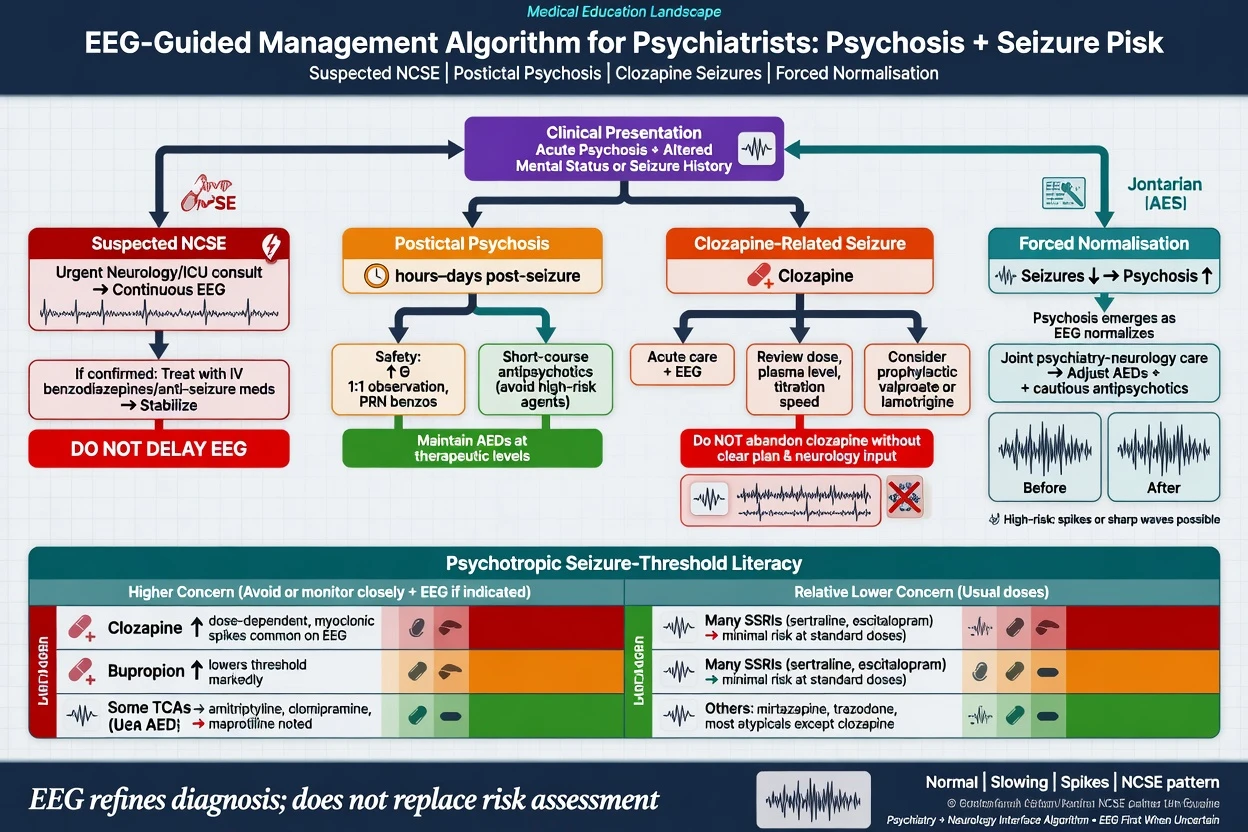
For postictal psychosis use a safety-first environment, short-course antipsychotics as clinically needed, maintain antiseizure medicines, and plan for high short-term violence and self-harm risk. For clozapine-related seizure provide acute seizure care; check recent dose escalations, plasma level, interacting drugs (for example smoking cessation raising levels), and electrolytes; consider antiseizure prophylaxis discussion (often valproate in practice) and whether dose reduction is feasible without abandoning uniquely effective therapy. For anti-NMDA pathways make early neurology and immunotherapy referral, with psychiatric symptom control as supportive care while disease-modifying treatment proceeds. [9][10][14]
Definitive management and psychotropic seizure literacy
EEG findings refine diagnosis and co-management; they do not replace formulation, psychotherapy, or recovery planning. [1][9]
Seizure threshold literacy (exam-safe framing). Large FDA clinical-trial summary data show differences in seizure incidence across psychotropic agents and doses; clozapine is a standout clinical concern among antipsychotics, while many SSRIs at usual doses have relatively lower reported trial seizure incidence than older high-risk agents — still individualise for prior epilepsy, dose, and combinations. [10][11] Centorrino and colleagues showed higher rates of EEG abnormalities with clozapine than with several other antipsychotics in treated patients. [9]
qEEG/ERP in care pathways. Research biomarkers may eventually stratify risk (e.g. MMN in clinical high-risk samples in research settings) but current routine care still diagnoses syndromes clinically. [12]
Subtypes and high-yield scenarios
- First-episode psychosis — EEG when atypical/organic features present, not as mandatory universal test in every straightforward primary psychosis. [2][4]
- Delirium — diffuse slowing supports encephalopathy; treat causes.
- Clozapine clinic — counsel seizure risk; EEG sometimes used when clinical suspicion of seizures or marked dose escalation contexts per local practice. [9][10]
- Epilepsy CL — postictal psychosis timing; forced normalisation when psychiatry worsens as seizures/EEG improve.
- Catatonia — keep NCSE and encephalitis on the differential. [6]
- PNES — video-EEG, not a single normal routine EEG alone.
- ICU CL — advocate for cEEG when NCSE is plausible. [5][7]
- Exam research literacy — quote MMN/P300 group findings without claiming individual diagnosis. [12]
Complications and pitfalls
Common failures include using a normal EEG as proof of functional-only illness; over-calling non-specific theta as epilepsy; ignoring benzodiazepine beta or clozapine effects on the report; ordering endless EEGs without a question; missing NCSE because convulsions are absent; commercial qEEG overclaim; and abrupt antiseizure drug withdrawal for behaviour alone. [1][3][6][7][9]
Prognosis and disposition
Disposition is driven by clinical diagnosis, risk, and support, not by an isolated EEG adjective. NCSE outcomes depend on aetiology and time to treatment. Postictal psychosis is often time-limited but high-risk acutely. If clinical suspicion of epilepsy remains high despite a normal routine EEG, refer to neurology rather than closing the case. [1][5][6]
Special populations
In children and adolescents incidental epileptiform findings are more common and need CAP plus neurology context; older adults show more non-specific slowing so prioritise delirium and neurocognitive differentials; intellectual disability carries higher epilepsy comorbidity and behavioural change may be seizure-related; pregnancy EEG is non-invasive and generally safe with careful medication correlation; forensic settings must not treat EEG as determining criminal responsibility. [1][2][4]
Evidence, guidelines, and regional deltas
Landmark anchors for answers: O'Sullivan and Boutros on psychiatric EEG role/indications; Jefsen on modern service use; Herman/Claassen on continuous EEG; Beniczky Salzburg NCSE criteria; Hirsch ACNS terminology; Centorrino and Devinsky on antipsychotic/clozapine EEG and seizures; Alper on trial seizure incidence; Umbricht on MMN; Schmitt and Dalmau on anti-NMDA EEG/clinical series. [1][2][5][6][9][10][12][13][14]
Exam pearls
EEG ORDER (psychiatric)
Rapid viva checklist
Be ready to define what scalp EEG measures and its spatial limit; list frequency bands with one clinical association each; name five high-yield psychiatric indications; state the normal-EEG exclusion fallacy; distinguish routine versus continuous versus video-EEG; give the Salzburg-style NCSE concept; teach clozapine EEG abnormalities and seizure risk; name two ERPs (P300, MMN) and their research status; link extreme delta brush to the anti-NMDA pathway; and state one regional guideline stance (RANZCP, NICE, or APA framing). [1][5][6][9][12][13]
Bottom line for multi-board exams
Master when to order, how to read categories of findings, drug confounds, and emergency pathways (NCSE, encephalitis, clozapine seizures). Reject both nihilism ("EEG never helps psychiatry") and magical thinking ("qEEG diagnoses depression"). That balance is the fellowship answer. [1][5][6][9][12]
References
- [1]O'Sullivan SS, Mullins GM, Cassidy EM, et al. The role of the standard EEG in clinical psychiatry Hum Psychopharmacol, 2006.PMID 16783810
- [2]Boutros NN A review of indications for routine EEG in clinical psychiatry Hosp Community Psychiatry, 1992.PMID 1516903
- [3]Jefsen OH, et al. The clinical use of electroencephalography in a general psychiatric setting Nord J Psychiatry, 2023.PMID 36927234
- [4]Sand T, Bjørk MH, Vaaler AE Is EEG a useful test in adult psychiatry? Tidsskr Nor Laegeforen, 2013.PMID 23759782
- [5]Herman ST, Abend NS, Bleck TP, et al. Consensus statement on continuous EEG in critically ill adults and children, part I: indications J Clin Neurophysiol, 2015.PMID 25626778
- [6]Beniczky S, Hirsch LJ, Kaplan PW, et al. Unified EEG terminology and criteria for nonconvulsive status epilepticus Epilepsia, 2013.PMID 24001066
- [7]Claassen J, Mayer SA, Kowalski RG, et al. Detection of electrographic seizures with continuous EEG monitoring in critically ill patients Neurology, 2004.PMID 15159471
- [8]Hirsch LJ, Fong MWK, Leitinger M, et al. American Clinical Neurophysiology Society's Standardized Critical Care EEG Terminology: 2021 Version J Clin Neurophysiol, 2021.PMID 33475321
- [9]Centorrino F, Price BH, Tuttle M, et al. EEG abnormalities during treatment with typical and atypical antipsychotics Am J Psychiatry, 2002.PMID 11772698
- [10]Devinsky O, Honigfeld G, Patin J Clozapine-related seizures: experience with 5,629 patients Neurology, 1994.PMID 7991106
- [11]Alper K, Schwartz KA, Kolts RL, Khan A Seizure incidence in psychopharmacological clinical trials: an analysis of Food and Drug Administration (FDA) summary basis of approval reports Biol Psychiatry, 2007.PMID 17223086
- [12]Umbricht D, Krljes S Mismatch negativity in schizophrenia: a meta-analysis Schizophr Res, 2005.PMID 15927795
- [13]Schmitt SE, Pargeon K, Frechette ES, et al. Extreme delta brush: a unique EEG pattern in adults with anti-NMDA receptor encephalitis Neurology, 2012.PMID 22933737
- [14]Dalmau J, Gleichman AJ, Hughes EG, et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies Lancet Neurol, 2008.PMID 18851928