Psych · Foundations — history
History of psychiatry
Also known as Psychiatric historiography · History of mental health care · Asylum history · Deinstitutionalisation history · Psychopharmacological revolution · Moral treatment · DSM-III history
Exam-exhaustive fellowship reference on the history of psychiatry — emergence of the specialty, moral treatment and asylum eras, Kraepelinian nosology, somatic therapies and the psychopharmacological revolution, deinstitutionalisation and community care, anti-psychiatry and Rosenhan debates, DSM-III operational criteria, recovery model, dark history and modern clinical implications. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
1 MCQ with explanations
Target exams
Red flags
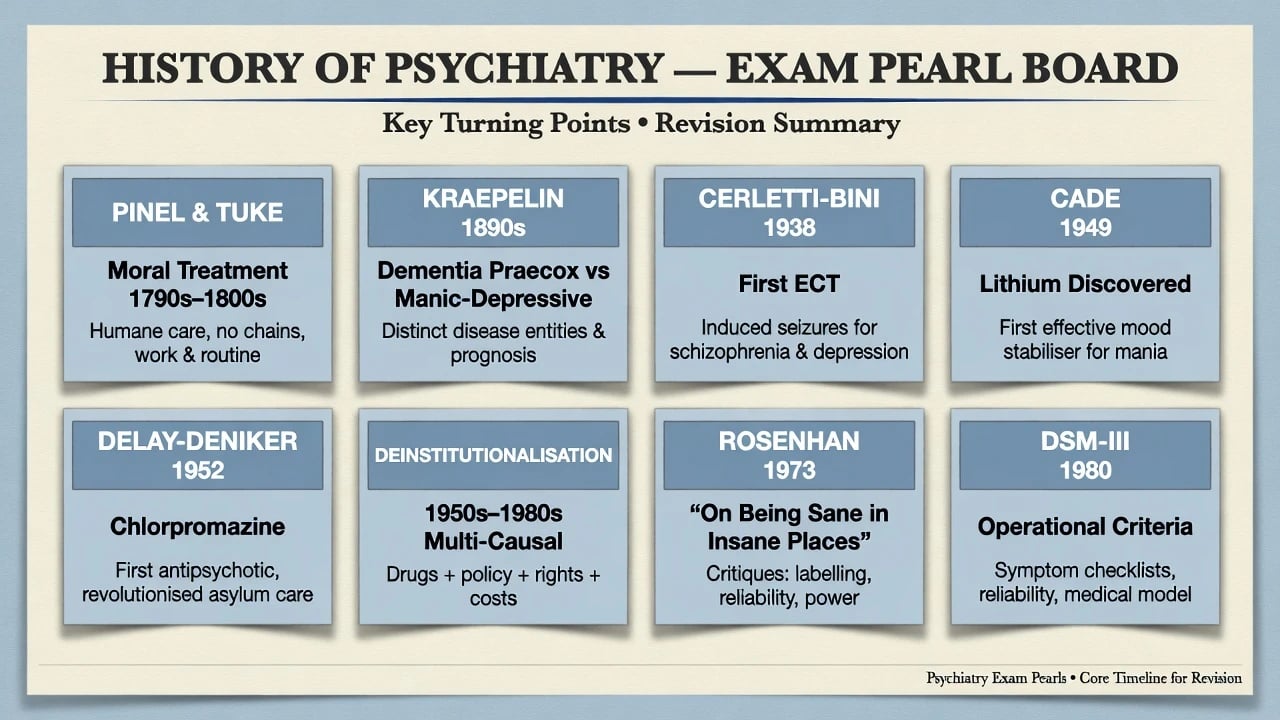
Fellowship candidates who only memorise names fail. Examiners want the why it mattered: moral treatment as humanisation of custody; Kraepelin as course-based nosology; chlorpromazine and lithium as discharge-enabling technologies; DSM-III as a reliability project; deinstitutionalisation as multi-causal policy with incomplete community replacement; recovery as a complementary vision, not anti-medicine.[3][5][11][14]
Definition and classification of the field
Psychiatry as a named medical specialty caring for the mentally ill emerged historically — it is not merely folk psychology in white coats. Kendler and colleagues locate the emergence of Western psychiatry across roughly 1650–1850, with institutional and medical consolidation in the late Enlightenment and early industrial period.[1]
Useful historiographic cuts (not mutually exclusive) track ideas, institutions, treatments, and classification systems across eras — from moral treatment and asylums through Kraepelin, RDC/DSM-III, and dual ICD/DSM practice.[1][12]
| Lens | What it tracks | Exam use |
|---|---|---|
| History of ideas | Humoral, moral, degenerationist, psychoanalytic, neurotransmitter models | Theory-driven treatments |
| History of institutions | Madhouses, asylums, general hospital units, community teams, prisons | Deinstitutionalisation stems |
| History of treatments | Moral management, ECT, lobotomy, psychotropics, psychotherapies | Landmark dates |
| History of classification | Kraepelin → Feighner/RDC → DSM-III → ICD/DSM dual systems | Nosology vivas |
| These four lenses organise fellowship teaching of the specialty’s historiography.[1][12] |
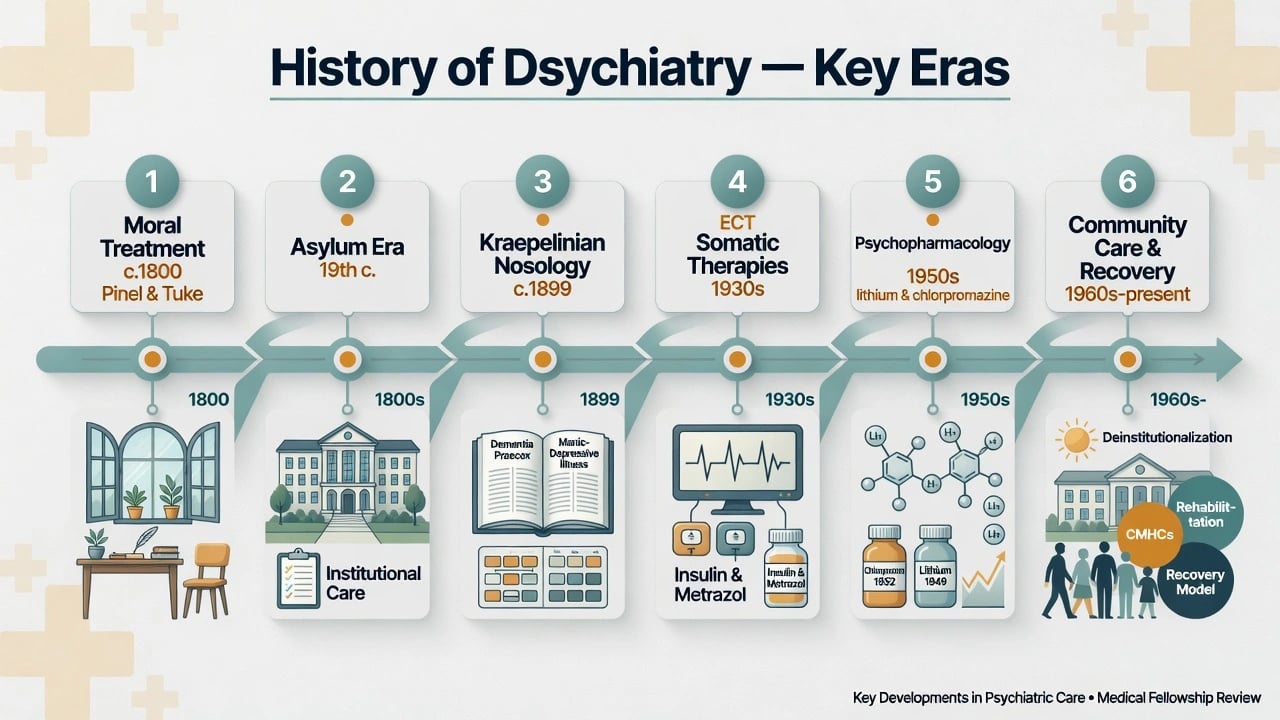
Moral treatment means the late-18th/early-19th-century humane psychosocial regime associated with Philippe Pinel (and Jean-Baptiste Pussin) in France and William Tuke at the York Retreat in England — kindness, occupation, orderly environment, reduced restraint — not a modern lecture on patient morality.[1][2]
Epidemiology and institutional scale
Reform cycles repeatedly reorganise where care happens and who is counted as a patient. George and colleagues describe successive US psychosis-treatment reform waves: moral treatment asylums; mental hygiene; community mental health; and later recovery/early-intervention framings — each with over-promise and incomplete implementation.[2]
Mid-20th-century state hospital censuses peaked before antipsychotics and policy shifts produced dramatic bed reductions. Exam pearl: bed closure is an outcome metric, not proof of better lives; underfunded community care, homelessness, and transinstitutionalisation into prisons and emergency departments are the critical counter-metrics.[2]
Classification eras also change recorded prevalence. The post-DSM-III operational culture expanded categorical diagnosis and research sampling; that is a nosological and service-planning effect, not pure biological change.[11][12]
Mechanisms: shifting models of mind and illness
Aetiology stories drive treatment fashions across eras, from pre-modern humoral and moral-religious frames through moral/psychological environmental models and organic/degenerationist (including eugenic) programmes to later psychoanalytic, pharmacologic, and recovery frameworks.[1][2][12]
- Pre-modern — supernatural, humoral, and moral-religious frames (context for later medicalisation).[1]
- Moral/psychological — disorder of passions and habits remediable by environment (moral treatment).[1]
- Organic/degenerationist — 19th-century biological fatalism and, darkly, eugenic programmes.[2]
- Psychoanalytic — mid-20th-century US dominance in DSM-I/II language of reaction and neurosis.[11][12]
- Psychopharmacological / monoamine-era — after chlorpromazine and related discoveries, chemical theories gained cultural power.[4][5]
- Biopsychosocial + recovery — multi-level formulation with hope, roles, and rights alongside clinical treatment.[14]
Clinical presentation through historical lenses
What clinicians “see” is partly theory-shaped across historical lenses of institution, course-based nosology, phenomenology, and labeling critique.[7][12]
- Asylum era — chronic institutional syndromes, long-stay disability, institutionalisation itself as phenotype.[2]
- Kraepelinian — course and outcome split dementia praecox from manic-depressive illness (still scaffolds schizophrenia vs bipolar thinking).[12]
- First-rank / phenomenological — German descriptive traditions (Schneider, Jaspers lineage) still structure MSE language.[12]
- Anti-psychiatry era — labeling theory and total-institution critiques reshaped public trust and legal rights debates.[7]
A strong viva presentation pairs historical constructs with modern discriminators: organic/substance differentials, risk, capacity, and cultural formulation — history explains stigma and patient fear of hospitals; it does not cancel medical assessment or the utility of working diagnoses.[7][13]
Differential frameworks (how to think, not lists of diseases)
Examiners test contrasts — progress vs critical historiography, moral treatment ideals vs custodial overcrowding, psychoanalytic vs DSM-III operational eras, planned community care vs dumping, and Rosenhan’s impact vs methodological critiques — not disease lists alone.[2][8][11]
| Contrast | Left pole | Right pole | Exam trap |
|---|---|---|---|
| Historiography | Whig progress story | Critical history of power and harm | Either pure celebration or pure condemnation |
| Asylum reform | Moral treatment ideal | Later custodial overcrowding | Assuming Pinel solved institutionalisation forever |
| Mid-century US | Psychoanalytic hegemony | Neo-Kraepelinian DSM-III | Claiming DSM was always operational |
| Community shift | Planned deinstitutionalisation | Dumping without services | Celebrating bed cuts alone |
| Rosenhan legacy | Labeling/reliability crisis | Methodological and integrity critiques | Treating 1973 Science as gospel |
| Use the table as a viva map: every contrast ends in a modern clinical implication (safeguards, dual manuals, community capacity, or critique literacy).[2][8][11] |
Rosenhan’s 1973 “On being sane in insane places” claimed pseudopatients were not recognised as sane once labeled; it accelerated public distrust and diagnostic reform pressure.[7] Spitzer argued the paper was pseudoscience as science and defended the case for psychiatric diagnosis.[8] Scull’s later historiography frames the episode as successful scientific fraud in parts — examiners expect both the cultural impact and the critiques.[9]
Assessment implications today
Historical literacy improves bedside work by linking stigma, course-based thinking, operational criteria, and dual-manual coding to everyday assessment.[10][11][12]
- Alliance — patients and families carry asylum, coercion, and stigma narratives; acknowledge without colluding with treatment refusal when risk is high.[2][7]
- Longitudinal history — Kraepelinian inheritance: course still discriminates syndromes.[12]
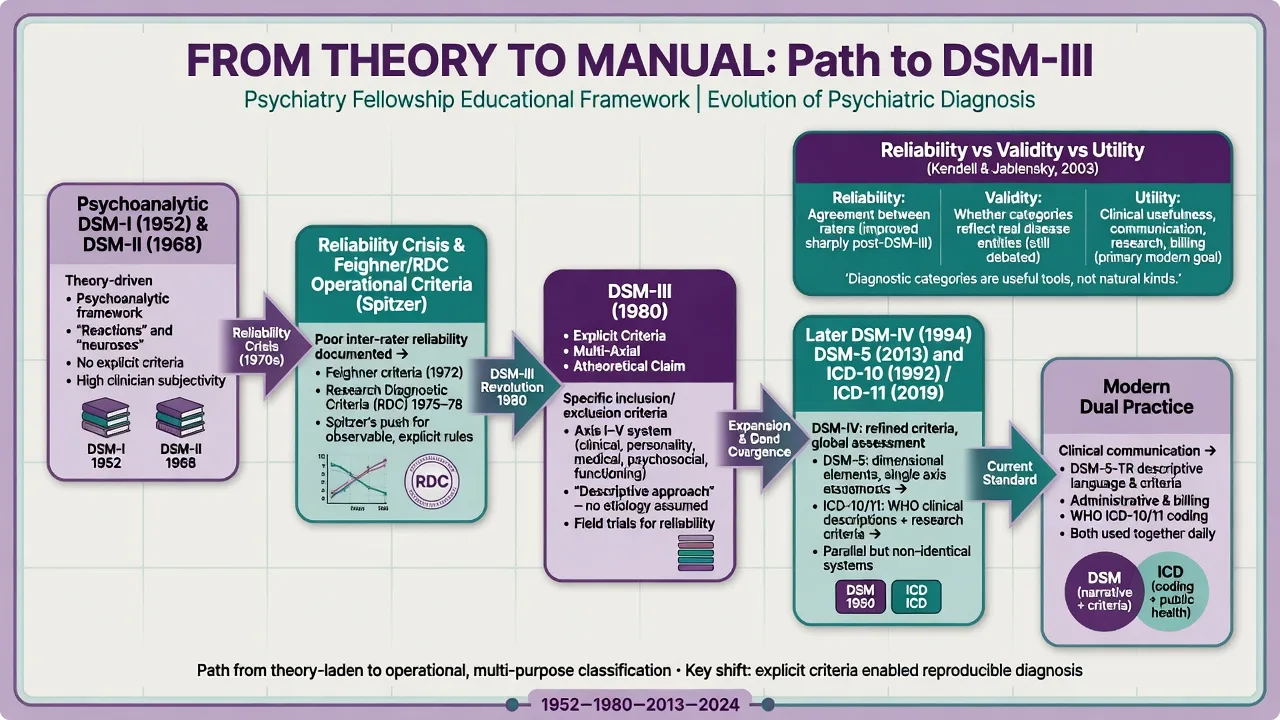
- Operational criteria culture — Research Diagnostic Criteria (RDC) formalised reliable inclusion/exclusion rules that fed DSM-III; use criteria without abandoning phenomenology and formulation.[10][11]
- Dual manuals — ICD for statistics/coding, DSM for much clinical research language; history of DSM-III explains the dual-system present.[11][12]
Investigations: what history teaches about “tests”
There is no laboratory test for a historical claim. Clinically, history warns against overclaiming biomarkers while defending hypothesis-driven organic exclusion in psychosis, delirium, and late-onset presentations. ECT’s origin story (Cerletti and Bini, 1938, after Meduna’s chemoconvulsive work) matters for consent conversations: modern modified ECT is not 1930s unmodified practice, but stigma often freezes on the origin myth.[6] Lithium and antipsychotic eras created monitoring cultures (levels, metabolic panels, EPS surveillance) that are safety lessons from iatrogenic discovery.[3][5]
Acute and emergency management — historical contrast
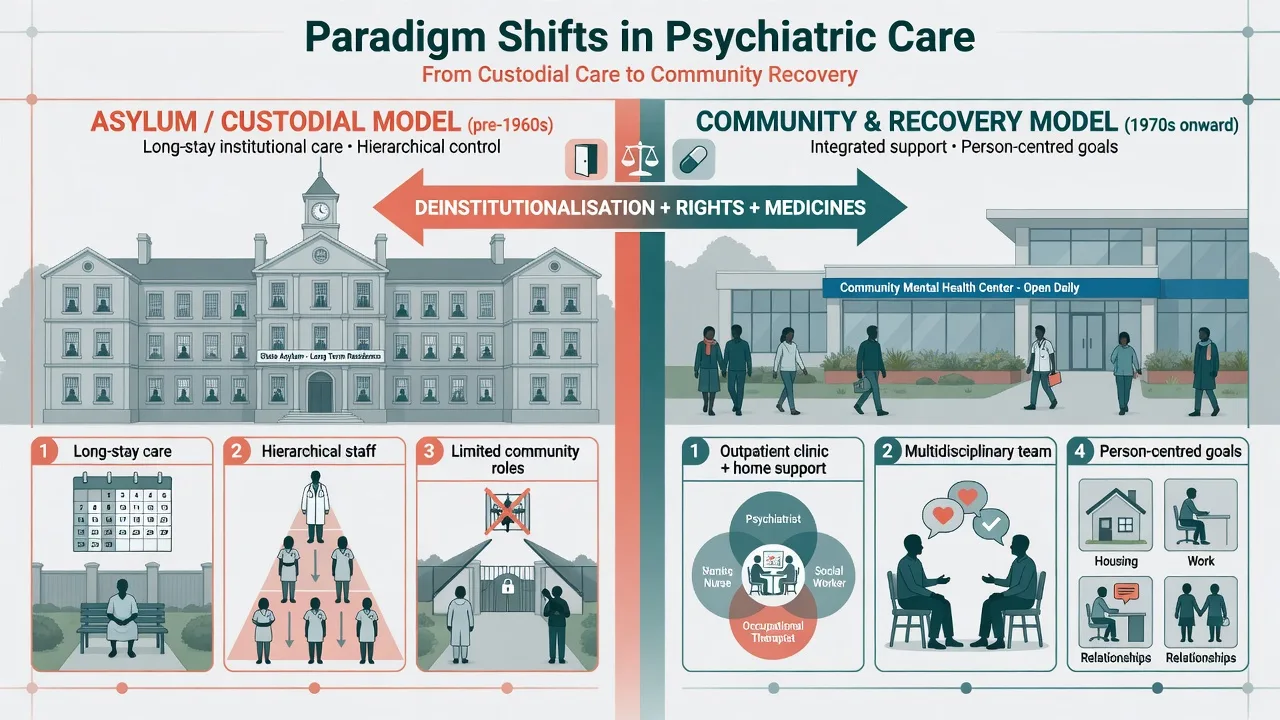
Historical acute control relied on restraint, seclusion, and asylum custody. Modern fellowship standard is de-escalation, least-restrictive legal pathways, and evidence-based rapid tranquillisation with medical monitoring — history is the foil, not the protocol. Life-threatening catatonia and severe melancholia still may require urgent ECT within contemporary consent/capacity frameworks; knowing ECT’s contested history helps explain and destigmatise without minimising cognitive risk discussions.[6]
Definitive management lineages
Moral treatment → milieu and recovery roots
Dignity, occupation, predictable environment, and respectful staff–patient relations remain relevant to ward culture and psychosocial rehabilitation even when pharmacology is central.[1][2]
Somatic therapies
- ECT (1938) — electrical seizure induction by Cerletti and Bini; still among the most effective treatments for selected severe mood and catatonic presentations when modern technique and consent standards are used.[6]
- Lobotomy and insulin coma — examinable as historical iatrogenic cautionary tales, not current practice; they anchor consent and evidence standards in modern somatic therapy teaching.[6]
Psychopharmacological revolution
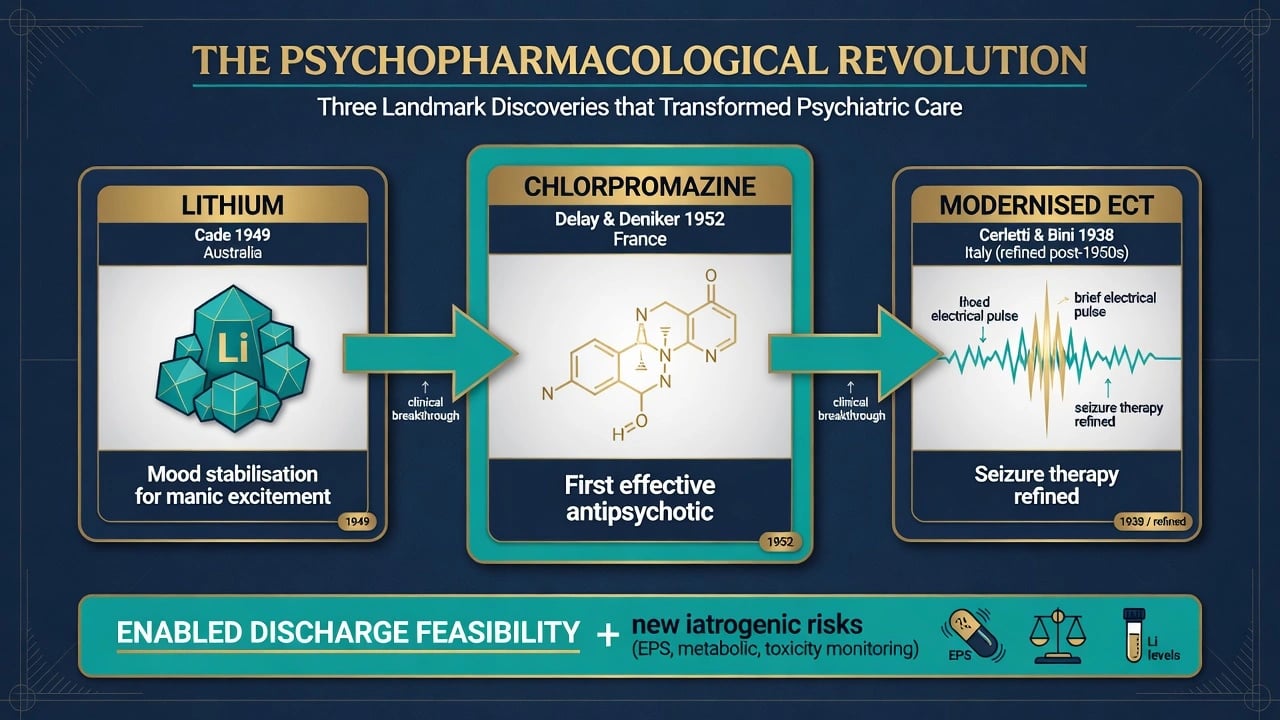
- Lithium (Cade, 1949) — Australian classic: lithium salts for manic (“psychotic”) excitement, published in the Medical Journal of Australia. ANZ exams love this stem.[3]
- Chlorpromazine (1952 psychiatric introduction) — synthesis and anaesthetic/lytic-cocktail path (Laborit and colleagues) then psychiatric trials at Sainte-Anne (Delay and Deniker); foundational antipsychotic enabling calmer wards and discharge feasibility, with later EPS and metabolic lessons.[4][5]
Doses for modern lithium or antipsychotics belong in drug monographs with contemporary product information and guidelines; history papers establish who/when/why, not your ward titration chart. Always pair agent + dose + route + monitoring with a nearby citation when prescribing content is clinical rather than historical — a safety lesson of the psychopharmacological era itself.[3][5]
Nosological reform as “management of knowledge”
DSM-III (1980) under Spitzer reoriented American psychiatry toward explicit diagnostic criteria, multiaxial assessment, and a claim of theoretical neutrality — a political-scientific transformation as much as a scientific one.[11] RDC supplied reliability rationale immediately beforehand.[10] Shorter traces nosology from Kraepelin through psychoanalytic blotting-out to the DSM series rise.[12] Kendell and Jablensky separate validity from clinical utility — the mature post-history position for viva defence of diagnosis without reification.[13]
Community care and recovery
Deinstitutionalisation was multi-causal: antipsychotics, civil rights, cost containment, and community mental health legislation (e.g. US Community Mental Health Act era) — not a single hero narrative.[2] Recovery-oriented care reframes outcomes beyond symptom checklists toward hope, identity, housing, work, and community membership as complementary to clinical treatment, not a replacement for it.[14]
Subtypes and regional scenarios
ANZ. Cade’s lithium paper is a regional pride stem and a global classic.[3] Australian and New Zealand systems moved from colonial asylums through large psychiatric hospitals to community-oriented services; Indigenous historical trauma, stolen generations, and culturally unsafe institutional practices are obligatory ethics context when discussing history and trust. Hospital coding typically tracks ICD; clinical discourse often uses DSM language — dual-system fluency is everyday practice.[3][11]
UK / Ireland. Tuke and the York Retreat; Lunacy legislation; Care in the Community; frequent exam comparison with Italian Basaglia reform (Law 180) as contrasting deinstitutionalisation styles within the broader moral-treatment-to-community arc.[1][2]
US / Canada. Dorothea Dix and state hospital expansion; mid-century psychoanalytic culture; CMHA-era community centres; Medicaid financing effects on institutions; DSM-III’s global export of operational criteria.[2][11]
Continental Europe. Pinel; Kraepelin; Cerletti–Bini in Rome; French chlorpromazine origin story.[1][4][6]
Complications and pitfalls
- Iatrogenic history — unmodified ECT fear, lobotomy, tardive dyskinesia after first-generation antipsychotics, lithium toxicity: each teaches monitoring and consent culture.[5][6]
- Eugenics and forced sterilisation — psychiatry participated; exams test ethical ownership, not evasion, within critical reform historiography.[2]
- Pathologisation of difference — homosexuality’s diagnostic history; racialised diagnoses; colonial psychiatry misuses; manuals change under social and scientific pressure.[11][12]
- Reform failure mode — close beds without housing, ACT-equivalent intensity, or substance/forensic pathways → crisis cycling.[2]
Prognosis and disposition thinking across eras
Asylum-era chronicity fatalism (dementia praecox legacy) shifted toward early intervention optimism and recovery language — both extremes can harm. Disposition today: least-restrictive appropriate level driven by risk, support, and illness severity, not nostalgia for long-stay beds or denial of need for intensive care when community supports fail.[2][14]
Special populations (historical attention points)
Historical institutions and manuals shaped care for women, children, older adults, people with intellectual disability, LGBTIQ+ communities, and colonised peoples — often with pathologisation, warehousing, or control rather than partnership; modern cultural safety and rights-based care are corrective responses, not optional courtesy.[2][11][14]
- Women — hysteria constructs, reproductive control, higher rates of certain historical institutionalisations.[2]
- Children — from moral imbecility constructs to developmental psychiatry and safeguarding.[2]
- Older adults — asylums as dementia warehouses; rise of old-age psychiatry.[2]
- Intellectual disability — parallel institutionalisation/deinstitutionalisation with distinct policy tracks.[2]
- LGBTIQ+ — depathologisation as classification ethics case (manuals change; people are not “cured” by votes).[11][12]
- Indigenous and colonised peoples — psychiatry as instrument of control in some colonial systems; cultural safety is corrective practice, not optional courtesy.[2][14]
Evidence, guidelines, and what “counts” as a landmark
Primary landmarks for exams — each row is a high-yield paper or discovery chain you should be able to date and apply.[1][12]
| Landmark | Take-home |
|---|---|
| Kendler et al. specialty emergence | Psychiatry as historical medical specialty[1] |
| George et al. reform cycles | Multi-wave reform with incomplete implementation[2] |
| Cade 1949 | Lithium for manic excitement — ANZ classic[3] |
| López-Muñoz / Ban on CPZ | Chlorpromazine discovery chain and 50-year perspective[4][5] |
| Gazdag on ECT | 1938 origin and modern persistence[6] |
| Rosenhan + Spitzer + Scull | Labeling crisis and critique stack[7][8][9] |
| Spitzer RDC; Wilson DSM-III; Shorter nosology | Reliability project and manual history[10][11][12] |
| Kendell and Jablensky | Validity vs utility split[13] |
| Jacob recovery | Recovery complementary to clinical care[14] |
| Modern RANZCP / NICE / APA guidelines sit on a post-operational-criteria evidence culture. History explains why trials, operational eligibility, and guideline development look the way they do — it does not replace current dosing tables.[10][11] |
Exam pearls
Synthesis for practice
History equips the fellow to integrate landmarks, nosology humility, service design, and recovery without either presentist arrogance or therapeutic nihilism.[2][13][14]
- Explain why manuals exist and why reliability projects happened.[10][11]
- Defend diagnosis with utility without reification.[13]
- Prescribe and recommend ECT/psychotropics with informed historical humility and modern safety standards.[3][5][6]
- Design services that avoid repeating underfunded community promises.[2]
- Practise recovery-compatible care that treats symptoms and supports roles and rights.[14]
Fellowship standard: hold both — know the dates, honour effective discoveries (lithium, antipsychotics, modern ECT technique), and refuse to forget the harmed.[3][5][6][2]
References
- [1]Kendler KS, Tabb K, Wright J The Emergence of Psychiatry: 1650-1850 Am J Psychiatry, 2022.PMID 35331024
- [2]George P, Jones N, Goldman H, et al. Cycles of reform in the history of psychosis treatment in the United States SSM Ment Health, 2023.PMID 37388405
- [3]Cade JF Lithium salts in the treatment of psychotic excitement Med J Aust, 1949.PMID 18142718
- [4]López-Muñoz F, Alamo C, Cuenca E, et al. History of the discovery and clinical introduction of chlorpromazine Ann Clin Psychiatry, 2005.PMID 16433053
- [5]Ban TA Fifty years chlorpromazine: a historical perspective Neuropsychiatr Dis Treat, 2007.PMID 19300578
- [6]Gazdag G, Ungvari GS Electroconvulsive therapy: 80 years old and still going strong World J Psychiatry, 2019.PMID 30631748
- [7]Rosenhan DL On being sane in insane places Science, 1973.PMID 4683124
- [8]Spitzer RL On pseudoscience in science and the case for psychiatric diagnosis. A critique of Rosenhan's "On Being Sane in Insane Places" Arch Gen Psychiatry, 1976.PMID 938183
- [9]Scull A Rosenhan revisited: successful scientific fraud Hist Psychiatry, 2023.PMID 36737877
- [10]Spitzer RL, Endicott J, Robins E Research diagnostic criteria: rationale and reliability Arch Gen Psychiatry, 1978.PMID 655775
- [11]Wilson M DSM-III and the transformation of American psychiatry: a history Am J Psychiatry, 1993.PMID 8434655
- [12]Shorter E The history of nosology and the rise of the Diagnostic and Statistical Manual of Mental Disorders Dialogues Clin Neurosci, 2015.PMID 25987864
- [13]Kendell R, Jablensky A Distinguishing between the validity and utility of psychiatric diagnoses Am J Psychiatry, 2003.PMID 12505793
- [14]Jacob KS Recovery model of mental illness: a complementary approach to psychiatric care Indian J Psychol Med, 2015.PMID 25969592