Psych · Foundations — learning theory and behavioural science
Learning theory and behavioural science
Also known as Classical conditioning · Operant conditioning · Social learning theory · Extinction learning · Inhibitory learning · Exposure mechanisms · Behavioural activation theory · Reinforcement schedules
Exam-exhaustive fellowship reference on learning theory and behavioural science for psychiatrists — classical, operant, and observational learning; reinforcement schedules; extinction and relapse phenomena; inhibitory-learning exposure; behavioural roots of CBT and BA; clinical applications across anxiety, OCD, PTSD, depression, and addiction. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview
Behavioural science is core MRCPsych Paper A / FRANZCP foundational theory and the mechanism language for almost every exposure-based and activation-based stem. A candidate who masters this page should design an exposure that maximises inhibitory learning, discriminate classical from operant maintenance of the same symptom, and explain why clinic-only successes fail at the shopping centre on Saturday.[3][4][5][6]
Definition and classification
Learning is a relatively enduring change in behaviour or behavioural potential due to experience (distinct from maturation, fatigue, or transient state change). Social-cognitive accounts further emphasise modelled experience and self-efficacy as determinants of behaviour change.[1]
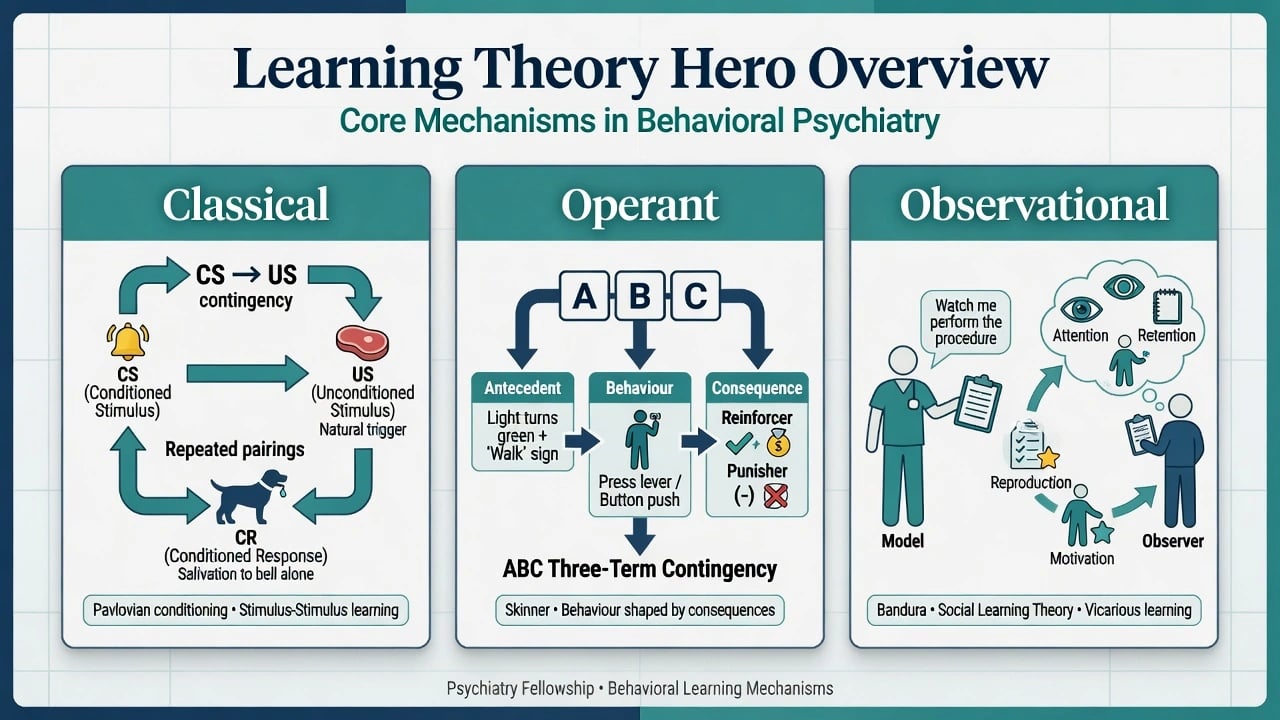
Three systems examiners test
| System | Core unit | Clinical anchor |
|---|---|---|
| Classical (Pavlovian) | CS predicts US → CR | Cue-triggered panic, trauma reminders, interoceptive fear |
| Operant (instrumental) | Behaviour → consequence (ABC) | Escape, avoidance, rituals, substance seeking, inactivity |
| Observational (social) | Model → observer via attention, retention, reproduction, motivation | Vicarious fear, self-harm contagion, skill acquisition, self-efficacy |
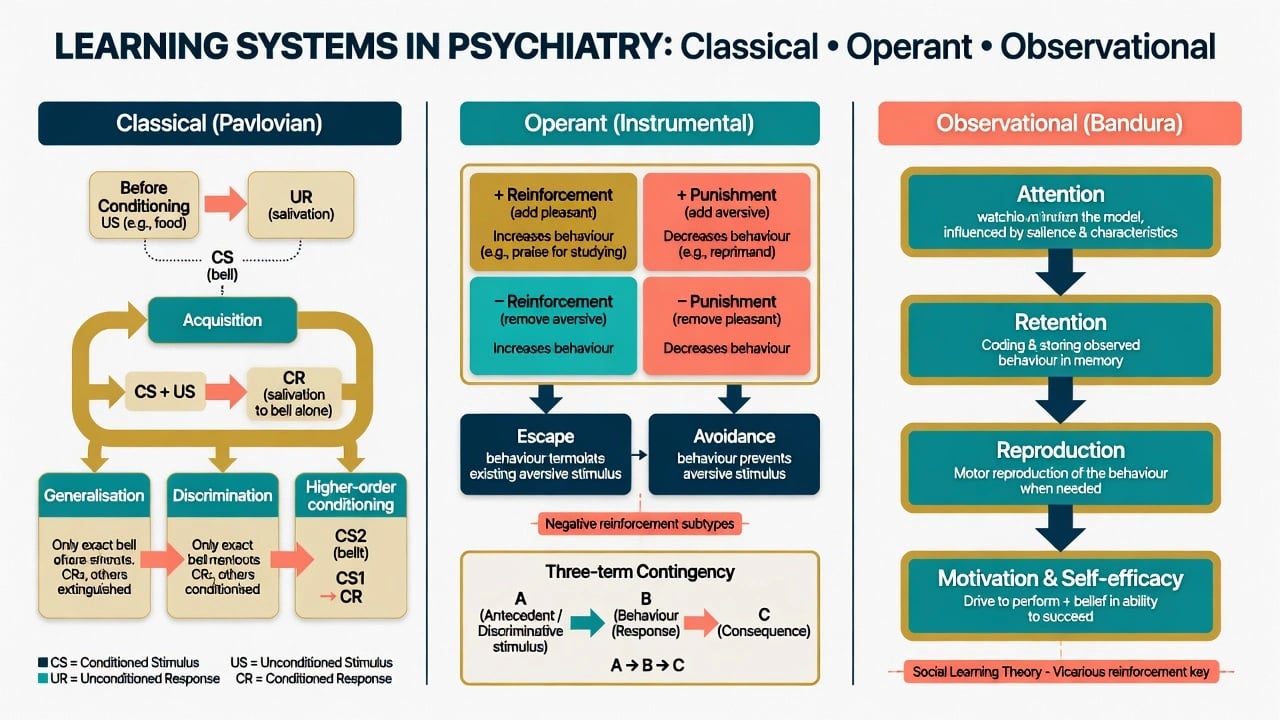
Classical conditioning — high-yield terms
- US / UR: unconditioned stimulus / response (e.g. true threat → fear).
- CS / CR: conditioned stimulus / response after pairing (e.g. lift → panic).
- Acquisition, extinction, spontaneous recovery, generalisation, discrimination, higher-order conditioning.
- Contiguity vs contingency: modern accounts emphasise predictive contingency, not mere co-occurrence — and extinction of the CR remains context-sensitive after training.[3][4]
Operant conditioning — four cells and escape/avoidance
- Positive reinforcement: add pleasant → behaviour increases (praise, drug high, social media likes).
- Negative reinforcement: remove aversive → behaviour increases (escape terminates ongoing aversive stimulus; avoidance prevents it).
- Positive punishment: add aversive → behaviour decreases.
- Negative punishment: remove pleasant → behaviour decreases (response cost, time-out). Functional analyses of depression likewise treat reduced reinforcement and escape as maintaining processes.[2]
Two-factor theory of avoidance (exam staple): classical acquisition of fear to cues + operant avoidance maintained by negative reinforcement (anxiety reduction). Avoidance never lets the person learn that the CS is now safe — the extinction problem in miniature.[3][4]
Observational learning and self-efficacy
Bandura’s social cognitive model: observers learn by modelling; self-efficacy (belief in capacity to execute a behaviour) mediates initiation, effort, and persistence under threat — central to exposure homework and behaviour-change programmes.[1]
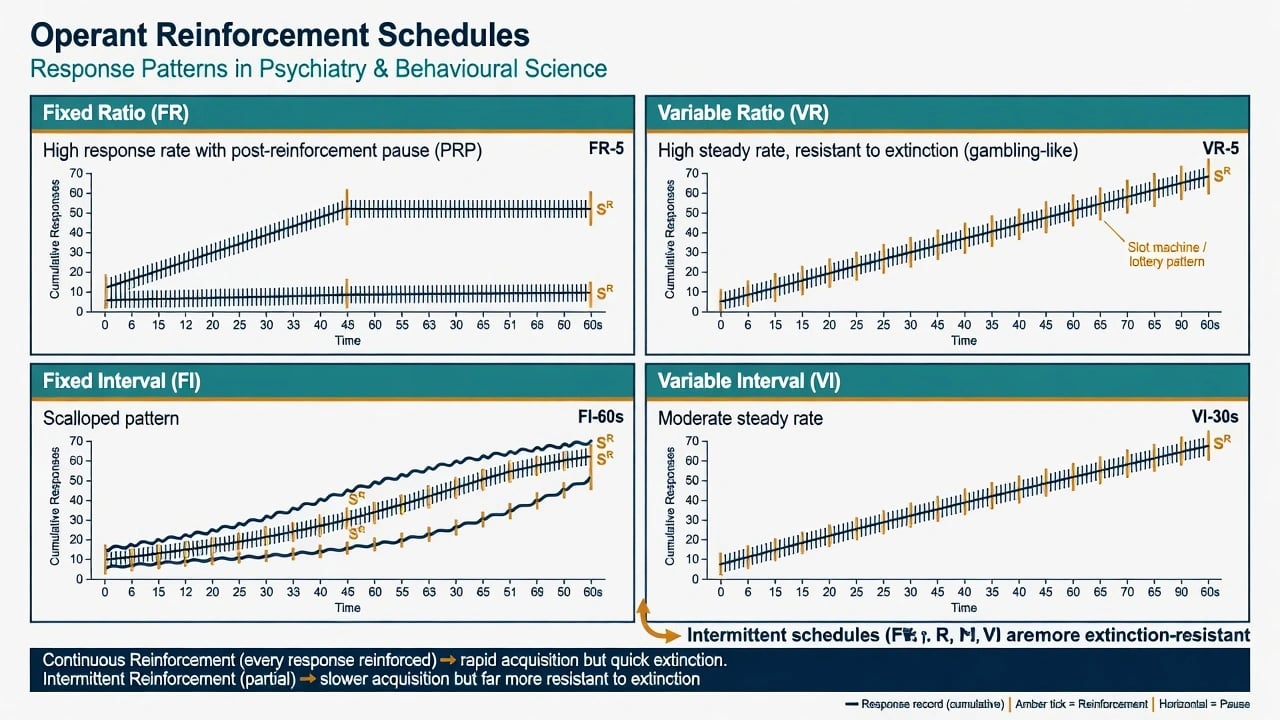
Reinforcement schedules
Intermittent schedules acquire more slowly but resist extinction more than continuous reinforcement — the gambling / variable-ratio clinical pearl. Self-efficacy still shapes whether a person initiates the responses that contact those schedules under threat or low mood.[1][2]
| Schedule | Pattern | Clinical note |
|---|---|---|
| Continuous (CRF) | Every response reinforced | Fast acquisition; rapid extinction when stopped |
| Fixed ratio (FR) | High rate + post-reinforcement pause | Piece-rate work analogies |
| Variable ratio (VR) | High steady rate; highly extinction-resistant | Gambling, some digital rewards, intermittent parental attention to tantrums |
| Fixed interval (FI) | Scalloped responding near interval end | Waiting for fixed review times |
| Variable interval (VI) | Moderate steady rate | Unpredictable checking opportunities |
Pathophysiology and mechanisms
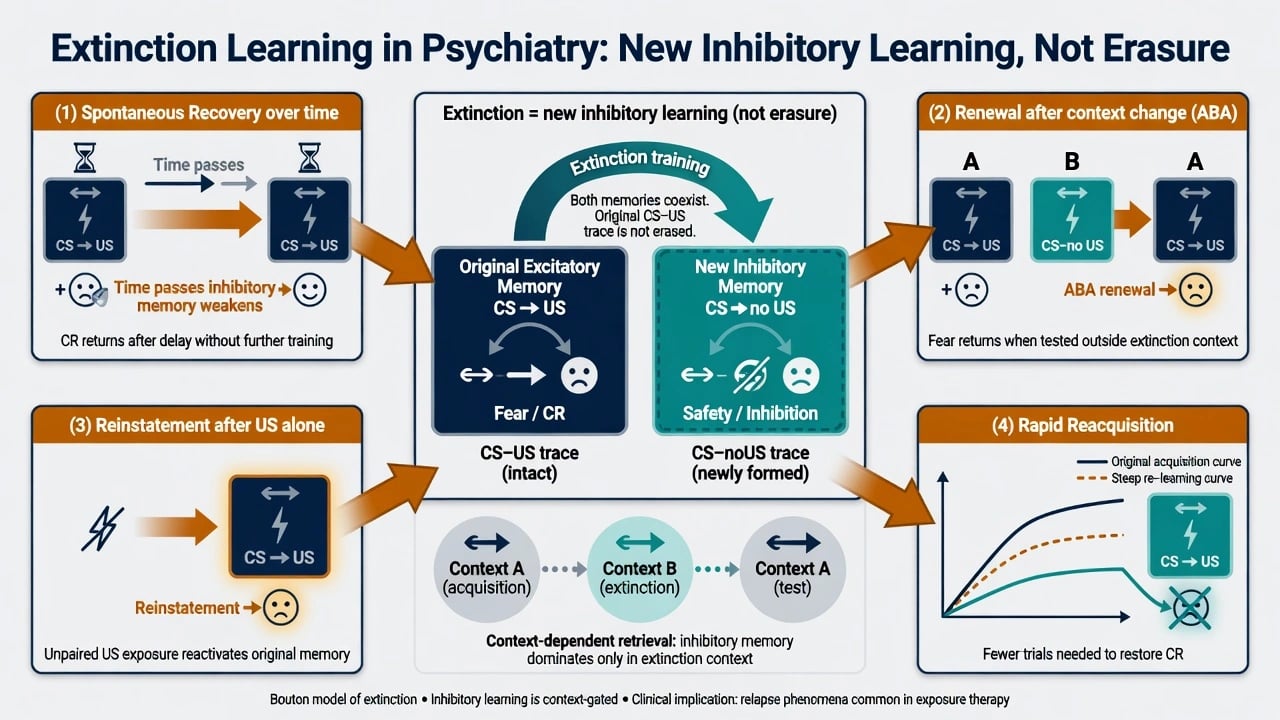
Fear conditioning and extinction
Conditioned fear is a laboratory and clinical model of threat learning. Extinction training (CS without US) does not erase the original CS–US association. A new inhibitory CS–noUS memory is formed; which memory is retrieved depends on context and time.[3][4]
Bouton’s core relapse sources after extinction are central to relapse prevention teaching.[3][4]
- Spontaneous recovery — CR returns after time passes.
- Renewal — CR returns when context changes (classic ABA: acquire in A, extinguish in B, test in A).
- Reinstatement — unpaired US presentations restore CR to the CS.
- Rapid reacquisition — fewer pairings needed to restore the CR after extinction. These forms motivate multi-context exposure and booster planning rather than assuming one-shot unlearning.[3][4]
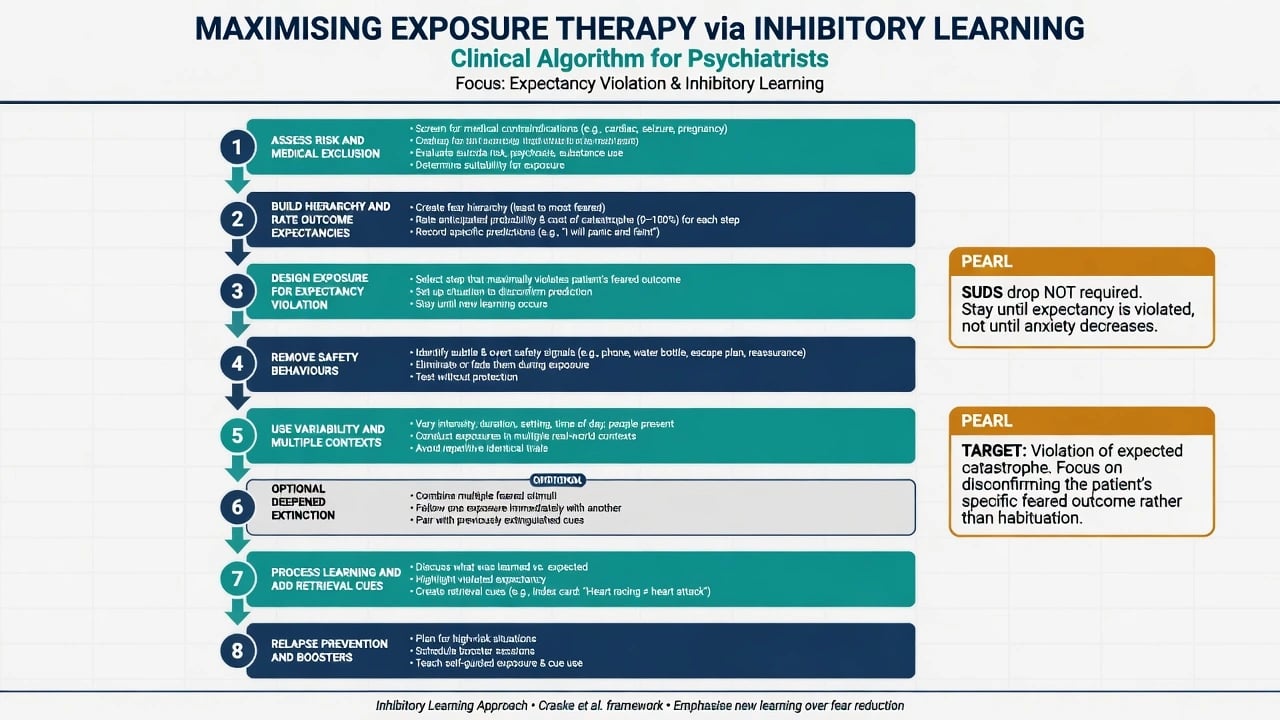
Inhibitory learning model of exposure
Craske and colleagues reframed exposure away from “stay until anxiety habituates” toward maximising inhibitory learning and its retrieval.[5][6] Design targets include:
- Expectancy violation — set a specific predicted catastrophe; arrange experience that violates it; process the mismatch.
- Removal of safety signals/behaviours — phone, water bottle, reassurance, subtle rituals that prevent full tests.
- Variability — intensity, duration, stimuli, timing (not identical graded steps only).
- Multiple contexts — prevent ABA renewal after office-only extinction.
- Deepened extinction — compound cues / sequential CS combinations where appropriate.
- Occasional reinforced extinction (lab-informed) and retrieval cues for home practice.
- Affect labelling as an optional enhancer in some protocols. These tactics aim to strengthen inhibitory learning and its retrieval across time and place, not merely to produce within-session calm.[5][6]
Within-session SUDS reduction is neither necessary nor sufficient for long-term outcome under this model; what matters is new learning that the expected disaster does not occur (or is tolerable).[5][6]
Safety behaviours and panic
Clark’s cognitive model of panic: catastrophic misinterpretation of bodily sensations plus safety behaviours that block disconfirmation of threat beliefs — a behavioural-science mechanism wearing a cognitive coat.[9] The same logic generalises to social anxiety rituals, OCD compulsions (negative reinforcement), and many phobic coping strategies.
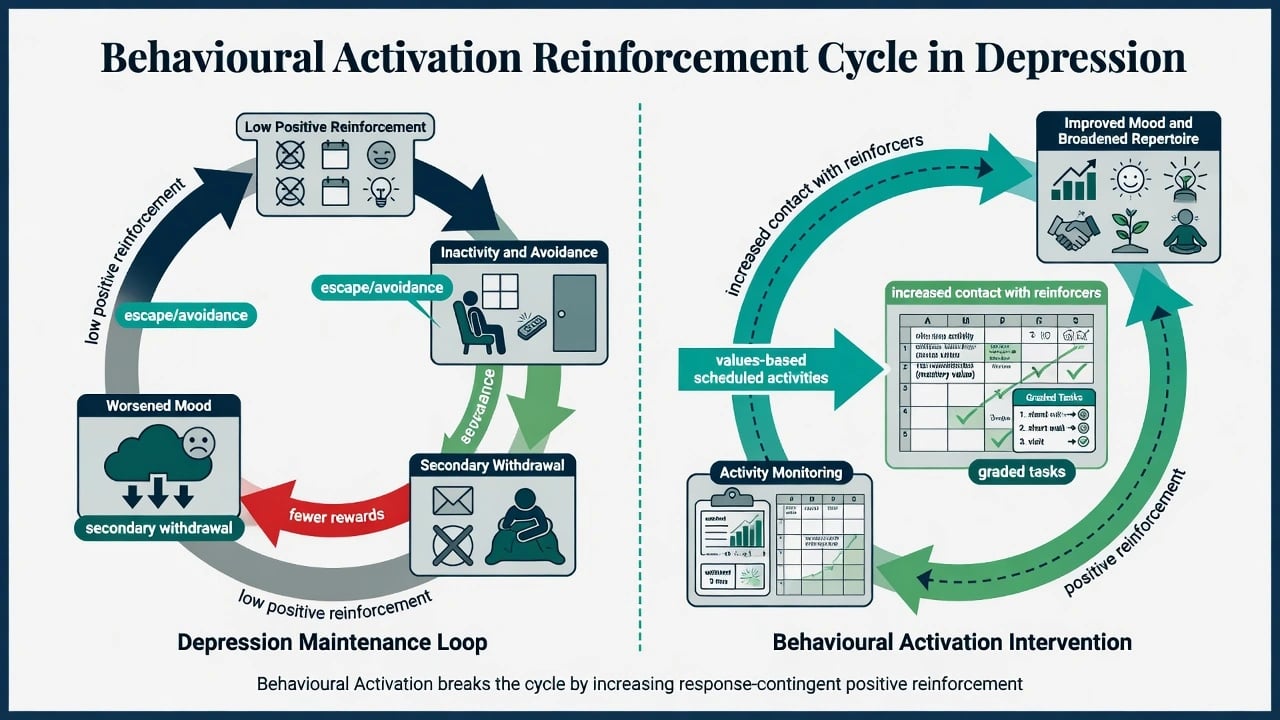
Depression as a reinforcement problem
Ferster’s functional analysis and later behavioural activation (BA) models: depression is maintained by low rates of response-contingent positive reinforcement, narrowed repertoires, and escape/avoidance of aversive tasks that further reduce reward contact.[2][18] BA reverses the loop via monitoring, values-based scheduling, and graded activation — not merely “keeping busy.”
Landmark trial evidence: Dimidjian and colleagues found behavioural activation comparable to antidepressant medication and superior to cognitive therapy among more severely depressed adults in acute treatment; follow-up work examined relapse prevention among responders.[7][8][18]
CBT behavioural roots
Beck’s cognitive model integrated with behavioural methods became modern CBT; meta-analyses support CBT across many disorders, with exposure-based methods central for anxiety-related conditions.[10][11][12][13][14] Exposure efficacy for OCD and PTSD is supported by mechanism-aware reviews and PE meta-analysis.[15][16][17]
Clinical presentation (how learning shows up)
- Cue-bound fear: lifts, needles, trauma reminders, interoceptive triggers.
- Operant chains in the MSE/history: “I left the mall and felt better” (negative reinforcement of escape); ritual hours that “must” be completed.
- Covert safety: checking pulse, carrying benzodiazepines “just in case,” only going out with a partner — strategies that block disconfirmation of threat beliefs.
- Depression: cancelled plans, bed as escape, loss of mastery and pleasure activities (low positive reinforcement).
- Modelling: anxious parental modelling; peer self-harm scripts in youth networks. These patterns map directly onto classical, operant, and observational mechanisms used in formulation and therapy planning.[1][2][9]
Differential — mechanism discrimination
| Feature | Classical emphasis | Operant emphasis |
|---|---|---|
| Unit of analysis | CS–US prediction / CR | Antecedent–behaviour–consequence |
| Panic attack example | Heartbeat CS → catastrophe CR | Leaving situation negatively reinforces escape |
| OCD ritual | Obsession as threat CS | Ritual negatively reinforced by anxiety drop |
| Treatment lever | Extinction / inhibitory CS–noUS learning | Response prevention; change contingencies |
| Exam trap | Calling all anxiety 'classical' | Ignoring cue conditioning and only talking about 'secondary gain' |
Also contrast habituation model of exposure (stay until anxiety falls) with inhibitory learning (violate expectancies; generalise inhibitory retrieval).[5][6]
Assessment (bedside behavioural science)
- Functional analysis (ABC): antecedents, behaviour topography, short- and long-term consequences.
- Avoidance and safety-behaviour inventory — overt and subtle.
- Hierarchy + expectancy ratings — predicted probability and cost of catastrophe, not only SUDS.
- Activity monitoring for BA (hour-by-hour mastery/pleasure or values contact).
- Risk, capacity, medical red flags before interoceptive or trauma exposure (true cardiac disease, seizure risk, pregnancy considerations, substance intoxication/withdrawal, dissociation, acute psychosis).
- Outcome metrics: disorder scales (e.g. Y-BOCS, PCL, PDSS) plus behavioural targets (ritual hours, avoidance days, completed exposures). Assessment thus operationalises learning mechanisms before technique choice.[2][5][6][9]
Investigations
No lab test diagnoses “faulty learning.” Investigate medical mimics when panic, trauma sequelae, or substance withdrawal could explain symptoms; baseline metabolic/ECG work when pharmacotherapy is combined with behavioural programmes. Session data (homework quality, expectancy violation logs) test the formulation continuously and mirror the collaborative empiricism of CBT/exposure packages.[5][6][12]
Acute / emergency management
Mid-session escape: contain distress, re-contract for a manageable inhibitory-learning trial, avoid ending only with total avoidance reinforced as the sole outcome — otherwise negative reinforcement of escape is strengthened again.[5][6]
Definitive management (application)
Exposure and ERP
- Modalities: in vivo, imaginal, interoceptive, VR-assisted where available.
- OCD: response prevention extinguishes the negative reinforcement of rituals.[15]
- PTSD: prolonged exposure and related protocols rest on emotional processing and extinction-related learning; meta-analytic support for PE vs control conditions.[16][17]
- Optimise with Craske principles above; plan multi-context generalisation from day one.[5][6]
Behavioural activation
Activity monitoring → values-based activity scheduling → graded tasks → problem-solve barriers → relapse prevention. Evidence supports BA as a standalone behavioural treatment with medication-comparable effects in more severe depression in a landmark RCT and theoretical lineage from reinforcement models.[2][7][8][18]
Behavioural experiments
Predict → test → review updates beliefs under collaborative empiricism; they are not vague “try this homework.” Same inhibitory-learning DNA as well-designed exposure.[5][6][12]
Contingency management and schedules
In addiction and behavioural programmes, structured reinforcement (vouchers, privileges) leverages operant principles; intermittent natural schedules that previously maintained use (cue + variable drug reward) must be understood to design competing reinforcers. Self-efficacy and modelled alternatives further support sustained behaviour change.[1][2]
Combining with medication
SSRIs/SNRIs and other agents often run in parallel for anxiety, OCD, PTSD, and depression. Behavioural work is not a reason to stop indicated pharmacotherapy; shared goals and monitoring prevent split formulations (“the pill vs the homework”), consistent with combined-care evidence pathways for CBT-era treatments.[7][12][13]
Guidelines (regional deltas)
NICE / APA / RANZCP-aligned practice prioritises exposure-based CBT for anxiety disorders, ERP for OCD, trauma-focused therapies including exposure-based protocols for PTSD, and CBT/BA pathways for depression. Exact stepped-care thresholds and commissioning routes differ by jurisdiction; quote local pathways in viva, but mechanism language is shared.[12][13][14][15]
Subtypes and scenarios
| Scenario | Dominant learning levers |
|---|---|
| Specific phobia | Classical fear + operant avoidance; in vivo exposure |
| Panic / agoraphobia | Interoceptive CS; safety behaviours; multi-context exposure |
| Social anxiety | Safety behaviours; self-focused attention; behavioural experiments |
| OCD | Negative reinforcement of rituals; ERP |
| PTSD | Trauma-cue conditioning; PE / TF-CBT mechanisms |
| Depression | Low positive reinforcement; BA |
| Substance use | Cue reactivity + operant drug seeking; contingency management |
| Child/adolescent | Modelling; parent-mediated contingencies; school reinforcers |
| Intellectual disability | Applied behaviour analysis principles with dignity and capacity focus |
| Shared principle | Extinction/inhibitory learning, reinforcement repair, and modelling remap to protocols with efficacy support |
| Across scenarios, the same learning levers (extinction/inhibitory learning, reinforcement repair, modelling) are remapped to disorder-specific protocols with supporting efficacy syntheses.[6][7][12][15] |
Complications and pitfalls
- Therapist drift: dropping exposure, overusing distraction, chasing only SUDS drop.
- Safety behaviours smuggled in as “coping skills.”
- Context-bound gains without renewal planning.
- Punishment-heavy behaviour plans → alliance rupture, covert avoidance.
- Historical aversive conditioning abuses — modern standard is collaborative, reinforcement-based, consent-centred.
- Vicarious harm in poorly moderated groups (self-harm methods, eating pathology). Each pitfall either blocks expectancy violation, re-strengthens escape, or fails to generalise inhibitory learning.[3][5][6]
Prognosis and disposition
Extinction memories remain context-sensitive; plan boosters and high-risk situation rehearsals.[3][4] Homework quality (not mere quantity) predicts behavioural CBT outcomes in related literature. Step up to intensive ERP/day programmes when outpatient inhibitory learning fails due to severity, accommodation, or access barriers; step down to self-guided exposure with retrieval cues when stable.
Special populations
- Children: simpler expectancy language; caregiver contingencies and modelling.
- Older adults: medical comorbidity may limit interoceptive intensity — grade, do not abandon exposure.
- Pregnancy: behavioural interventions often preferred when appropriate; trauma work needs robust support.
- Cultural formulation: what the family system reinforces/punishes; co-design hierarchies that are culturally meaningful.
- Indigenous and minority contexts: community modelling, historical trauma, and culturally safe engagement — avoid pathologising protective avoidance without partnership. Developmental and cultural context changes which reinforcers, models, and exposure hierarchies are feasible, but the core learning mechanisms remain the clinical frame.[1][6][12]
Evidence pearls (named)
- Bandura 1977 — self-efficacy and social cognitive behaviour change.[1]
- Ferster 1973 — functional analysis of depression.[2]
- Bouton 2002/2004 — extinction context and relapse forms.[3][4]
- Craske 2008/2014 — inhibitory learning optimisation of exposure.[5][6]
- Dimidjian 2006 / Dobson 2008 / Dimidjian review 2011 — BA efficacy and lineage.[7][8][18]
- Clark 1986 — panic model and safety behaviours.[9]
- Beck 1964/2008; Butler 2006; Hofmann 2008/2012 — cognitive model and CBT efficacy maps.[10][11][12][13][14]
- Foa / Powers PE line — exposure efficacy OCD/PTSD.[15][16][17]
Exam pearls
RENEW — relapse after extinction
- Classical = CS predicts US; operant = behaviour produces consequence.
- Variable ratio → persistent, extinction-resistant responding.
- Drop safety behaviours or expectancy never gets tested.[6][9]
- Legal frameworks for involuntary treatment remain jurisdiction-specific — do not invent section numbers; capacity and least-restrictive principles still apply inside behavioural programmes. These pearls compress Bouton, Craske, and operant maintenance into viva-ready lines.[3][5][6]
Summary
Master three learning systems, four operant cells, reinforcement schedules, and Bouton relapse forms. Deliver exposure as inhibitory learning design, BA as reinforcement repair, and always fuse behavioural precision with risk, medical exclusion, and collaborative consent. That combination is what fellowship examiners reward.[3][6][7]
References
- [1]Bandura A Self-efficacy: toward a unifying theory of behavioral change Psychol Rev, 1977.PMID 847061
- [2]Ferster CB A functional anlysis of depression Am Psychol, 1973.PMID 4753644
- [3]Bouton ME Context, ambiguity, and unlearning: sources of relapse after behavioral extinction Biol Psychiatry, 2002.PMID 12437938
- [4]Bouton ME Context and behavioral processes in extinction Learn Mem, 2004.PMID 15466298
- [5]Craske MG, Kircanski K, Zelikowsky M, et al. Optimizing inhibitory learning during exposure therapy Behav Res Ther, 2008.PMID 18005936
- [6]Craske MG, Treanor M, Conway CC, et al. Maximizing exposure therapy: an inhibitory learning approach Behav Res Ther, 2014.PMID 24864005
- [7]Dimidjian S, Hollon SD, Dobson KS, et al. Randomized trial of behavioral activation, cognitive therapy, and antidepressant medication in the acute treatment of adults with major depression J Consult Clin Psychol, 2006.PMID 16881773
- [8]Dobson KS, Hollon SD, Dimidjian S, et al. Randomized trial of behavioral activation, cognitive therapy, and antidepressant medication in the prevention of relapse and recurrence in major depression J Consult Clin Psychol, 2008.PMID 18540740
- [9]Clark DM A cognitive approach to panic Behav Res Ther, 1986.PMID 3741311
- [10]Beck AT Thinking and depression. II. Theory and therapy Arch Gen Psychiatry, 1964.PMID 14159256
- [11]Beck AT The evolution of the cognitive model of depression and its neurobiological correlates Am J Psychiatry, 2008.PMID 18628348
- [12]Butler AC, Chapman JE, Forman EM, Beck AT The empirical status of cognitive-behavioral therapy: a review of meta-analyses Clin Psychol Rev, 2006.PMID 16199119
- [13]Hofmann SG, Asnaani A, Vonk IJ, et al. The Efficacy of Cognitive Behavioral Therapy: A Review of Meta-analyses Cognit Ther Res, 2012.PMID 23459093
- [14]Hofmann SG, Smits JA Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials J Clin Psychiatry, 2008.PMID 18363421
- [15]Foa EB, McLean CP The Efficacy of Exposure Therapy for Anxiety-Related Disorders and Its Underlying Mechanisms: The Case of OCD and PTSD Annu Rev Clin Psychol, 2016.PMID 26565122
- [16]Powers MB, Halpern JM, Ferenschak MP, et al. A meta-analytic review of prolonged exposure for posttraumatic stress disorder Clin Psychol Rev, 2010.PMID 20546985
- [17]Foa EB Prolonged exposure therapy: past, present, and future Depress Anxiety, 2011.PMID 22134957
- [18]Dimidjian S, Barrera M Jr, Martell C, et al. The origins and current status of behavioral activation treatments for depression Annu Rev Clin Psychol, 2011.PMID 21275642