Psych · foundations
Neuroanatomy and neural circuits for psychiatrists
Also known as Neural circuits psychiatry · Frontal-subcortical loops · Mesolimbic pathway · Mesocortical pathway · Default mode network · Salience network · Papez circuit · Limbic system psychiatry · Clinical localisation neuropsychiatry
Exam-exhaustive circuit neuroanatomy for FRANZCP/MRCPsych/ABPN: prefrontal zones, limbic and Papez frameworks, Alexander–DeLong basal-ganglia loops, four dopamine pathways, Menon triple network (DMN/salience/CEN), and clinical localisation of psychosis, mood, OCD, addiction, and frontal syndromes. Landmark PMIDs verified.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Why this topic exists at fellowship depth
Examiners use circuit language to test whether you can (i) map a vignette to a plausible network, (ii) name landmark models without phrenology, and (iii) know when imaging/EEG/autoimmune work-up trumps theory. MRCPsych Paper A and FRANZCP written/viva stems repeatedly hit dopamine pathways, frontal syndromes, and resting-state networks.[10][16]
Definition and classification framework
Circuit-based psychiatry treats symptoms as emergent properties of interacting nodes (cortex, striatum, thalamus, limbic nuclei, midbrain) rather than isolated lesions. Modern practice pairs classical anatomy with network concepts from resting-state fMRI.[13][16]
| System | Core nodes | High-yield psychiatric linkage |
|---|---|---|
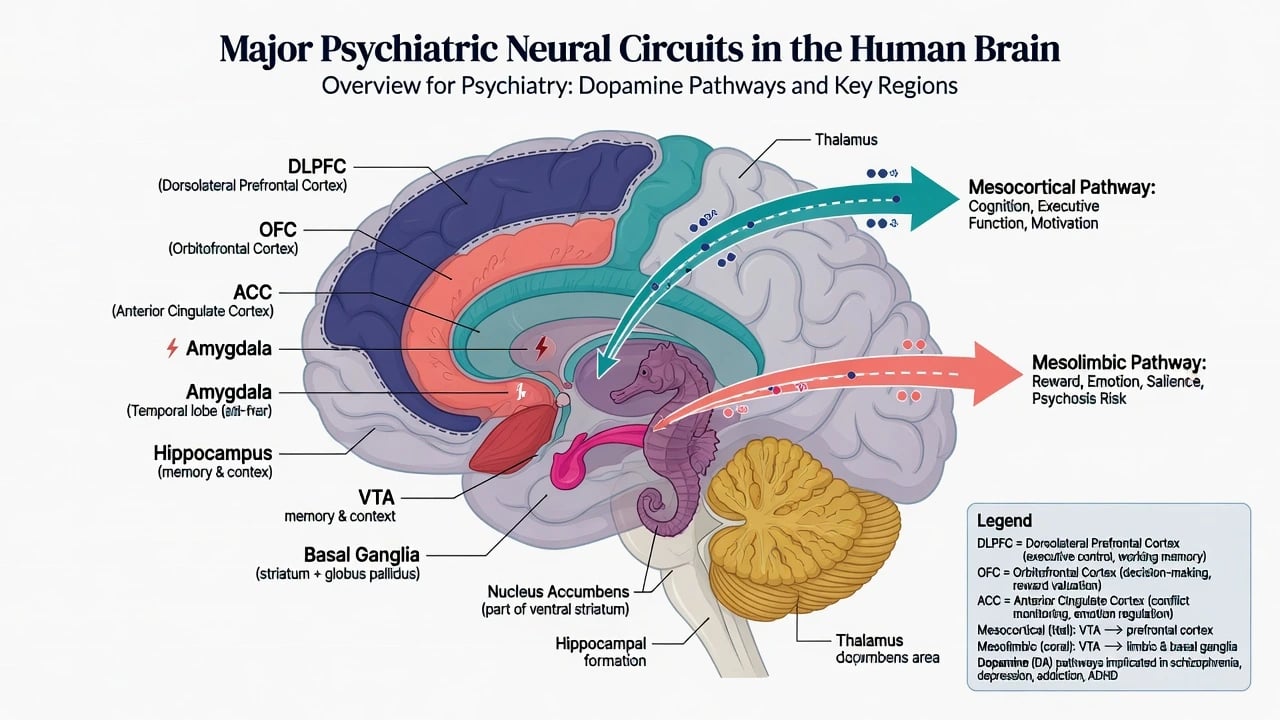
| Prefrontal | DLPFC, OFC/VMPFC, ACC | Executive control, valuation, motivation/conflict |
| Limbic | Amygdala, hippocampus, cingulate | Threat, context memory, affect integration |
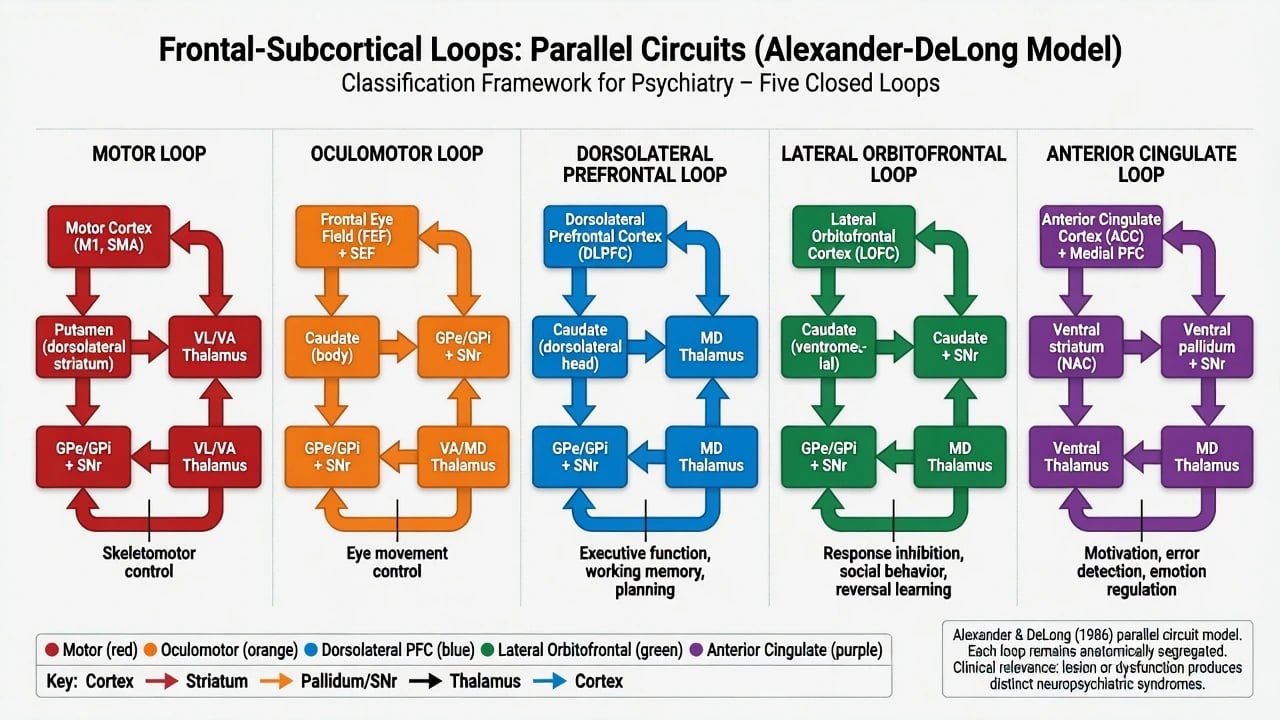
| Basal ganglia loops | Cortex–striatum–pallidum/SNr–thalamus–cortex | Motor + three “psychiatric” cognitive-affective loops |
| Midbrain DA | VTA, SNc, arcuate (TIDA) | Psychosis/reward, cognition, EPS, prolactin |
| Triple network | DMN, SN, CEN | Self-reference, salience switching, goal-directed control |
| Core systems for fellowship localisation teaching | — | See Alexander–DeLong, Cummings, Menon |
Prefrontal cortex — zones examiners expect
Dorsolateral prefrontal cortex (DLPFC)
Supports cognitive control and working-memory representations that bias behaviour toward goals (Miller–Cohen integrative model).[4] Clinical signature: dysexecutive syndrome — poor planning, concrete thought, impaired set-shifting, reduced fluency, working-memory failure.
Orbitofrontal and ventromedial / orbital–medial PFC
Architectonic work subdivides human orbital and medial prefrontal cortex (OMPFC) into networks tied to visceral, sensory, and associative processing — critical for valuation, extinction learning, and social-affective regulation.[5] Clinical signature: disinhibition, utilising behaviour, tactless impulsivity, reduced empathy, “pseudopsychopathic” frontal personality change after OFC injury.
Anterior cingulate cortex (ACC)
Bridges motivation, conflict monitoring, and affect. Dysfunction maps to abulia, reduced initiation, and contributions to mood and OCD models.[7][17]
Limbic system and the Papez scaffold
Classical Papez circuit
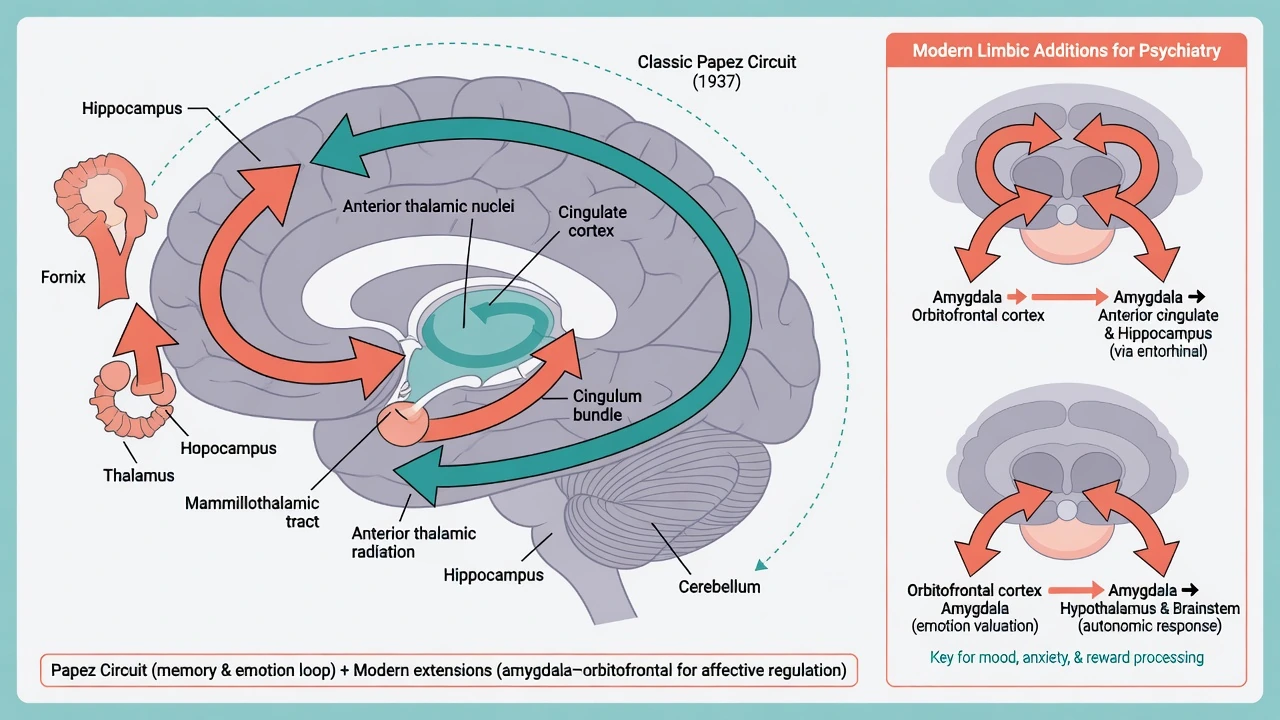
Papez proposed a closed loop: hippocampus → fornix → mammillary bodies → anterior thalamus → cingulate → back toward hippocampus as a mechanism of emotion.[1] Exam utility: historical scaffold for memory–affect integration. Exam trap: treating Papez as the complete modern limbic map.
Modern limbic additions psychiatrists actually use
- Amygdala: threat detection, vigilance, fear conditioning and expression.[2][3]
- Hippocampus: contextual memory; stress–HPA interface; volume loss associations in untreated depression are classic imaging-era findings (associative, not diagnostic alone).[17]
- OFC–amygdala–hypothalamic links: valuation of emotional stimuli and autonomic output.[2][5]
Emotion-perception models emphasise distributed cortical–subcortical routes rather than a single “emotion centre.” Clinical disorders of anxiety, PTSD, depression, and bipolar illness are framed as biased rather than uniquely destroyed circuits.[2][17]
Basal ganglia and reward circuitry
Parallel organisation of basal-ganglia–cortical circuits remains the skeleton of movement-disorder psychiatry and of OCD/Tourette/impulse-control discussions.[6][8]
Reward circuit anatomy links primate tract-tracing to human imaging: midbrain DA neurons, ventral striatum (including nucleus accumbens), ventral pallidum, and prefrontal targets support reinforcement learning and motivated behaviour.[9]
Clinical hooks (frontal–subcortical and reward-circuit interfaces):
- OCD-spectrum and classic PET-era caudate/OFC hyperactivity narratives (historical landmark; interpret with modern network nuance).
- Parkinson / Huntington mood, apathy, and impulse-control syndromes as loop disruptions.
- Dopamine-agonist impulse-control disorders as iatrogenic reward-circuit overdrive. [8] [9]
Dopamine pathways — the four-path viva set piece
| Pathway | Course | Excess / agonist bias | Blockade / deficit bias |
|---|---|---|---|
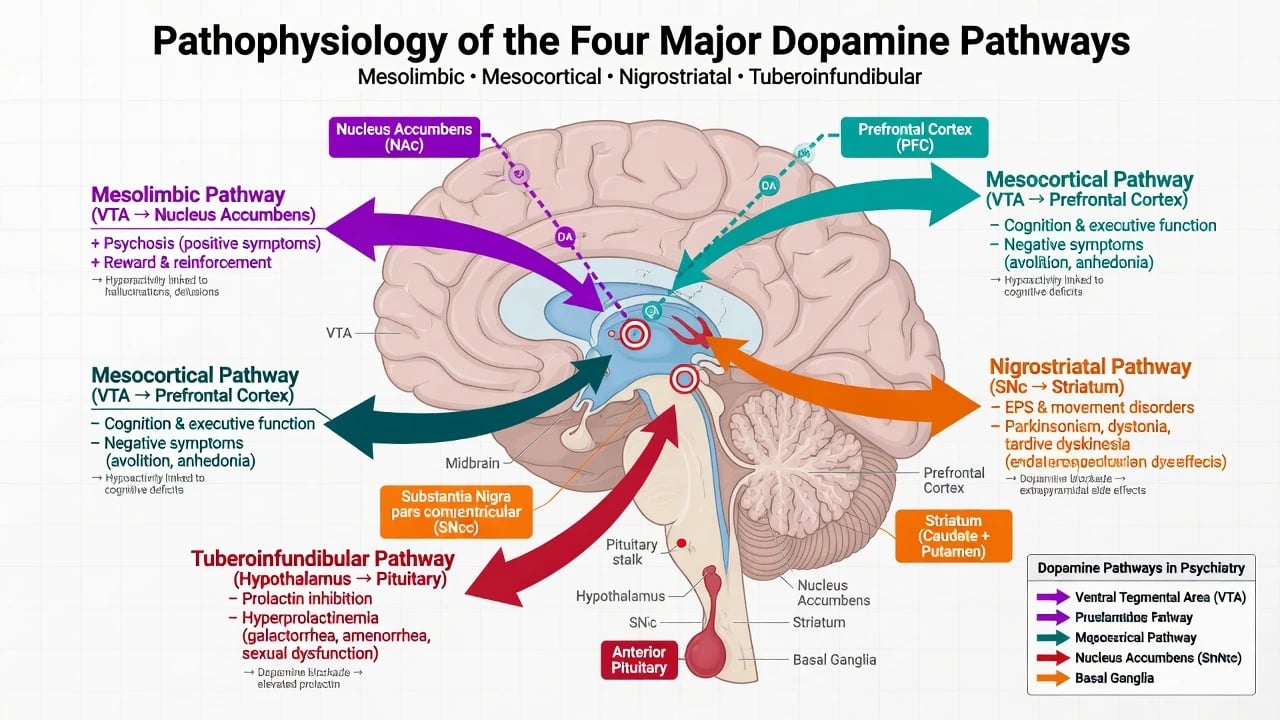
| Mesolimbic | VTA → nucleus accumbens | Aberrant salience, positive psychotic symptoms, craving | Reduced drive (oversimplified if global) |
| Mesocortical | VTA → PFC | — | Cognitive deficits, negative-symptom overlap models |
| Nigrostriatal | SNc → dorsal striatum | Dyskinesia (agonist/PD treatment context) | EPS, parkinsonism, dystonia, TD risk with chronic D2 blockade |
| Tuberoinfundibular | Arcuate → pituitary | — | Hyperprolactinaemia (galactorrhoea, amenorrhoea, sexual dysfunction) |
Howes and Kapur version III reframes dopamine as a final common pathway to psychosis: multiple upstream risks (genes, development, drugs, stress) converge on striatal dopamine dysregulation and aberrant salience assignment to stimuli.[10]
Grace phasic versus tonic dopamine: altered regulation of burst (phasic) versus baseline (tonic) firing modulates system responsivity and offers a mechanistic bridge between prefrontal regulation and striatal DA output relevant to schizophrenia models.[11]
Monoamine–glutamate–GABA interactions (Carlsson lineage) remind examiners that DA is not solo: cortical glutamate and GABA shape midbrain–striatal dynamics.[12]
L–C–N–T dopamine map
Large-scale networks — DMN, salience, CEN
Default mode network (DMN)
Raichle and colleagues described a default mode of brain function — organised intrinsic activity prominent at rest, attenuated during goal-directed tasks — with medial PFC and posterior cingulate among core nodes.[13] Buckner and colleagues mapped DMN anatomy and disease relevance (self-referential thought, memory, mind-wandering).[14]
Psychosis relevance: hyperconnectivity/hyperactivity of default-network components has been reported in schizophrenia and relatives (group-level finding — not a bedside test).[14][19]
Salience network
Seeley and colleagues dissociated a salience network (anterior insula, dorsal ACC) from an executive-control network, linking salience processing to homeostatic and affective relevance.[15]
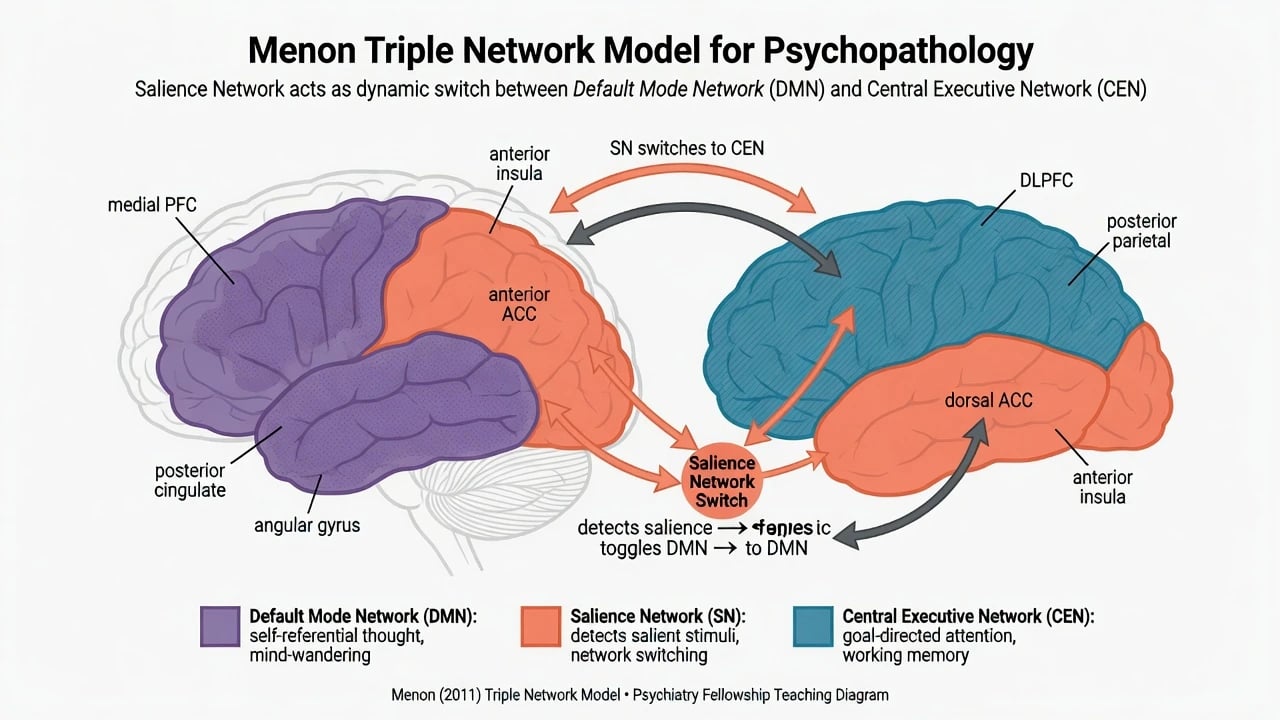
Triple-network model (Menon)
Menon unifies psychopathology as disordered interactions among DMN, salience network (SN), and central executive network (CEN), with the SN acting as a switch that engages CEN and suppresses DMN (and vice versa) depending on task demands.[16] Depression rumination, ADHD control failures, and psychosis self-monitoring models are often taught through this lens.
Schizophrenia dysconnection theories (Stephan, Friston, Frith) emphasise abnormal synaptic plasticity and hierarchical prediction/self-monitoring failures across networks — a conceptual upgrade from pure DA excess.[19]
Mood, anxiety, addiction — circuit vignettes
Depression
Mayberg’s limbic–cortical dysregulation model and Price–Drevets mood neurocircuitry integrate subgenual/subcallosal cingulate, PFC, amygdala, and related nodes.[17][18] This lineage underpins discussions of subcallosal cingulate deep brain stimulation as a network-modulating, highly selected intervention — not routine first-line care.
Anxiety / PTSD
Amygdala-centric threat circuitry plus failed prefrontal regulation of extinction is the standard teaching frame.[2][3]
Addiction
Koob and Volkow stage neurocircuitry: binge/intoxication (reward), withdrawal/negative affect (extended amygdala stress systems), and preoccupation/anticipation (craving, PFC control failure).[20][9]
Clinical localisation algorithm
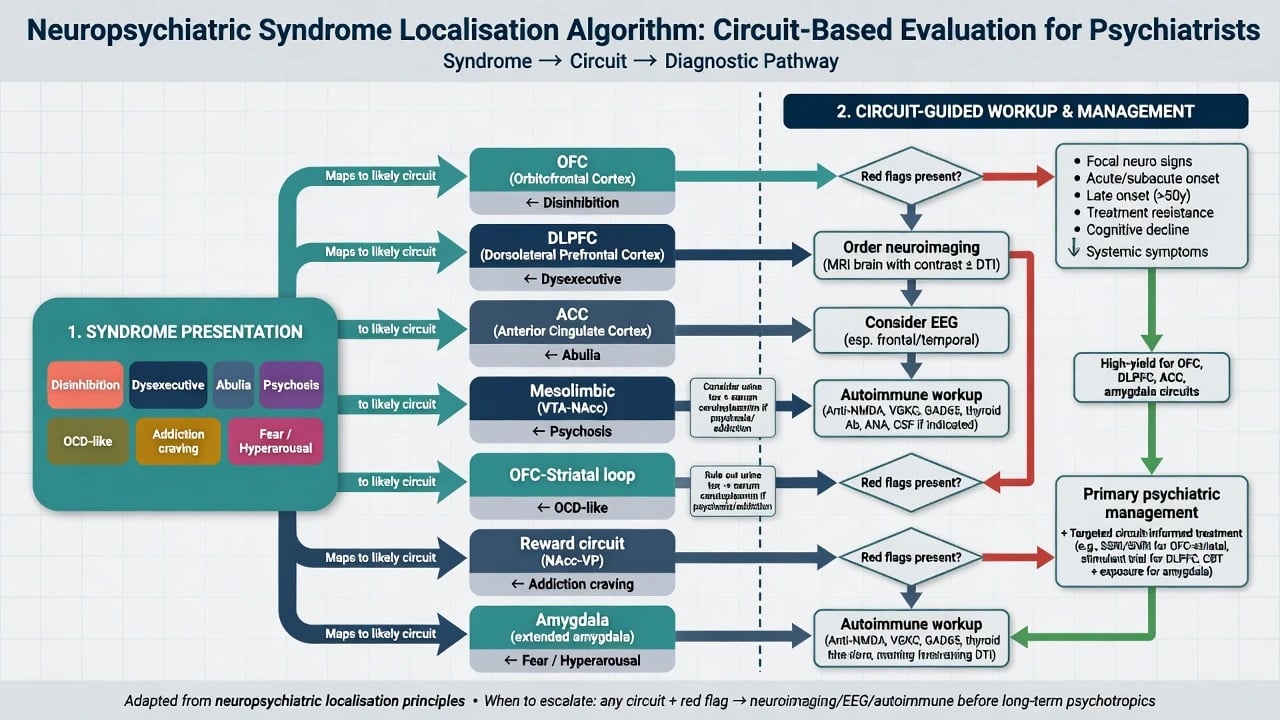
When circuit thinking must trigger investigation
| Clue | Preferential concern | Action |
|---|---|---|
| Late/atypical onset psychosis, seizures, fever, focal signs | Encephalitis, mass, epilepsy, metabolic | MRI ± EEG, autoimmune/infectious panel as indicated |
| Stepwise personality change, utilisation behaviour | OFC lesion, bvFTD, TBI | Imaging + neurology/neuropsych |
| Fluctuating attention + visual hallucinations | Delirium | Medical work-up first |
| New movement disorder + psychiatric change | Basal ganglia disease, drug effect | Neurology + med review |
| Post-stroke mood/apathy | Frontal–basal ganglia vascular | Stroke pathway + psychiatry liaison |
Bedside assessment mapped to circuits
- History: head injury, stroke, seizures, cancer/immunotherapy, substance surges, dopamine agonists.
- MSE: insight/judgement (PFC), affect/threat (limbic–PFC), thought disorder (language networks), perception (temporal/limbic + delirium screen).
- Executive probes: reverse digit span, verbal fluency, simple go/no-go or Luria sequences — then full neuropsychology when stakes are high.
- Neurological screen: always in first-episode/atypical presentations. [4] [7]
Differential diagnosis using circuits (discriminators)
- Primary psychosis vs temporal lobe epilepsy: stereotyped sensory auras, impaired awareness seizures, post-ictal states, EEG/MRI yield.
- Disinhibition vs mania: mania has elevated/irritable mood episode structure, reduced need for sleep, and often family/course clues; OFC lesions lack classic bipolar periodicity.
- Apathy vs melancholic depression: apathy lacks pervasive anhedonia/guilt/diurnal mood as defining; medial frontal signs and imaging may diverge.
- OCD vs frontal-striatal neurodegeneration: age, progressive cognitive/motor signs, lack of ego-dystonic insight patterns.
- Craving/compulsivity in addiction vs goal-directed mania: substance timing, withdrawal physiology, Koob–Volkow stage features. [7] [20] [19]
Management implications (mechanism map, not a drug monograph)
Psychotropics are circuit modulators (mechanism map, not a dose table):
- Antipsychotic D2 blockade targets mesolimbic hyperactivity models of positive symptoms but risks nigrostriatal EPS and tuberoinfundibular prolactin effects — separate pathways, separate monitoring mindsets.[10]
- Antidepressants and psychotherapies both aim, in complementary languages, to restore prefrontal regulation over limbic threat and self-referential loops.[17][18]
- CBT exposure engages extinction circuitry (PFC–amygdala).[2]
- Neuromodulation: ECT broadly perturbs networks; rTMS protocols often target DLPFC in depression; DBS (e.g., subcallosal cingulate lineage) is specialised, consent-heavy, and guideline-gated — know the concept for viva, not as community first step.[18]
Doses, titration, and product-specific monitoring belong in drug monographs and local protocols — do not invent numbers from circuit diagrams.[10][18]
- FRANZCP / RANZCP training: organic differential and formulation remain mandatory; circuit language supports viva depth but does not replace Mental Health Act principles (jurisdiction-specific statutes — do not invent section numbers).
- MRCPsych: Paper A loves pathway diagrams (DA four paths, frontal syndromes, networks); CASC still demands communication, not lecture-mode neuroanatomy.
- ABPN / MD-DNB: blueprint items mix behavioural neurology localisation with DSM/ICD clinical care. [10] [16]
Special populations
- Adolescents: ongoing PFC maturation shifts risk–reward balance; substance exposure hits developing mesocorticolimbic systems hard.
- Older adults: vascular frontal–subcortical syndromes, degenerative network failure, delirium super-sensitivity.
- Intellectual disability: interpret behaviour against baseline; still hunt pain, epilepsy, and medication toxicity.
- Cultural care: biological circuits are incomplete explanations of meaning, stigma, and help-seeking — use cultural formulation alongside neuroscience. [7] [9]
Complications and pitfalls
- Phrenology: one voxel ≠ diagnosis.
- Equating research fMRI with clinical tests.
- Confusing EPS with negative symptoms (nigrostriatal vs mesocortical).
- Ignoring prolactin while obsessing over mesolimbic theory.
- Teaching Papez without amygdala/OFC updates.
- Over-confident localisation without collaterals and serial MSE. [1] [2] [10]
Prognosis and disposition
Lesional syndromes follow etiology and rehab intensity. Primary psychiatric network disorders follow illness course, treatment engagement, and cognition. Co-manage with neurology when structural, epileptic, autoimmune, or movement-disorder drivers dominate; psychiatry leads when organic screen is negative and syndrome matches primary illness.[7][19]
Exam pearls
- Name four DA pathways with clinical pairs (psychosis/EPS/prolactin/cognition).[10]
- Name five Alexander–DeLong loops and which three are “psychiatric.”[6]
- OFC disinhibition / DLPFC dysexecutive / ACC abulia triad.[7]
- Menon: SN switches DMN ↔ CEN.[16]
- Howes–Kapur: DA final common pathway + aberrant salience.[10]
- Papez = history; amygdala/OFC = modern emotion map.[1][2]
- fMRI group maps ≠ individual blood tests.[13][14]
- Organic red flags beat elegant circuitry every time.[19]
| Syndrome pattern | Lead circuit hypothesis | Do not miss |
|---|---|---|
| Auditory hallucinations, delusions, aberrant salience | Mesolimbic DA dysregulation + network dysconnection | Encephalitis, epilepsy, stimulants |
| Rumination, anhedonia, negative self-focus | Limbic–cortical (subgenual–PFC) + DMN bias | Hypothyroid, post-stroke, PD depression |
| Obsessions/compulsions | OFC–striatal–thalamic loop | Sydenham/PANDAS-like context in youth; neurodegeneration late |
| Fear hyperarousal, PTSD re-experiencing models | Amygdala excess / PFC extinction failure | TBI, substance withdrawal |
| Craving, binge, relapse preoccupation | Reward + extended amygdala + PFC control (Koob–Volkow stages) | Pain, untreated ADHD, bipolar mislabel |
| Disinhibition after head injury | OFC / ventral frontal | Subdural, FTD mimic, alcohol |
Evidence anchors (what to cite in viva)
- Anatomy loops: Alexander–DeLong; Cummings/Tekin frontal–subcortical clinical synthesis.[6][7][8]
- PFC theory: Miller–Cohen; Ongür–Price OMPFC architecture.[4][5]
- Emotion: LeDoux; Davis–Whalen; Papez historical.[1][2][3]
- DA/psychosis: Howes–Kapur; Grace; Carlsson interactions; Friston dysconnection.[10][11][12][19]
- Networks: Raichle DMN; Buckner; Seeley salience; Menon triple network.[13][14][15][16]
- Mood/addiction: Mayberg; Price–Drevets; Haber–Knutson; Koob–Volkow.[17][18][9][20]
References
- [1]Papez JW A proposed mechanism of emotion. 1937 J Neuropsychiatry Clin Neurosci, 1995.PMID 7711480
- [2]LeDoux JE Emotion circuits in the brain Annu Rev Neurosci, 2000.PMID 10845062
- [3]Davis M, Whalen PJ The amygdala: vigilance and emotion Mol Psychiatry, 2001.PMID 11244481
- [4]Miller EK, Cohen JD An integrative theory of prefrontal cortex function Annu Rev Neurosci, 2001.PMID 11283309
- [5]Ongür D, Ferry AT, Price JL Architectonic subdivision of the human orbital and medial prefrontal cortex J Comp Neurol, 2003.PMID 12692859
- [6]Alexander GE, DeLong MR, Strick PL Parallel organization of functionally segregated circuits linking basal ganglia and cortex Annu Rev Neurosci, 1986.PMID 3085570
- [7]Cummings JL Frontal-subcortical circuits and human behavior Arch Neurol, 1993.PMID 8352676
- [8]Tekin S, Cummings JL Frontal-subcortical neuronal circuits and clinical neuropsychiatry: an update J Psychosom Res, 2002.PMID 12169339
- [9]Haber SN, Knutson B The reward circuit: linking primate anatomy and human imaging Neuropsychopharmacology, 2010.PMID 19812543
- [10]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164
- [11]Grace AA Phasic versus tonic dopamine release and the modulation of dopamine system responsivity: a hypothesis for the etiology of schizophrenia Neuroscience, 1991.PMID 1676137
- [12]Carlsson A, Waters N, Holm-Waters S, Tedroff J, Nilsson M, Carlsson ML Interactions between monoamines, glutamate, and GABA in schizophrenia: new evidence Annu Rev Pharmacol Toxicol, 2001.PMID 11264457
- [13]Raichle ME, MacLeod AM, Snyder AZ, Powers WJ, Gusnard DA, Shulman GL A default mode of brain function Proc Natl Acad Sci U S A, 2001.PMID 11209064
- [14]Buckner RL, Andrews-Hanna JR, Schacter DL The brain's default network: anatomy, function, and relevance to disease Ann N Y Acad Sci, 2008.PMID 18400922
- [15]Seeley WW, Menon V, Schatzberg AF, et al. Dissociable intrinsic connectivity networks for salience processing and executive control J Neurosci, 2007.PMID 17329432
- [16]Menon V Large-scale brain networks and psychopathology: a unifying triple network model Trends Cogn Sci, 2011.PMID 21908230
- [17]Price JL, Drevets WC Neurocircuitry of mood disorders Neuropsychopharmacology, 2010.PMID 19693001
- [18]Mayberg HS Limbic-cortical dysregulation: a proposed model of depression J Neuropsychiatry Clin Neurosci, 1997.PMID 9276848
- [19]Stephan KE, Friston KJ, Frith CD Dysconnection in schizophrenia: from abnormal synaptic plasticity to failures of self-monitoring Schizophr Bull, 2009.PMID 19155345
- [20]Koob GF, Volkow ND Neurocircuitry of addiction Neuropsychopharmacology, 2010.PMID 19710631