Psych · Foundations — personality theory
Personality theory for psychiatrists
Also known as Five-factor model · Big Five personality · Temperament and character · Dimensional personality · AMPD · PID-5 · Level of personality functioning · Trait theory psychiatry
Exam-exhaustive fellowship reference on personality theory for psychiatrists — trait models (FFM/Big Five, Cloninger), psychodynamic and cognitive-interpersonal frames, continuum to personality disorder, AMPD and ICD-11 dimensional models, assessment, formulation, and clinical application. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview
Personality theory is core MRCPsych Paper A / FRANZCP foundational science and the conceptual glue between ordinary individual differences, comorbidity patterns, alliance problems, and personality disorder nosology. A candidate who masters this page should define trait systems cleanly, map a patient onto functioning plus traits, and avoid both therapeutic nihilism and premature lifelong labelling.[1][11][13]
Definition and classification
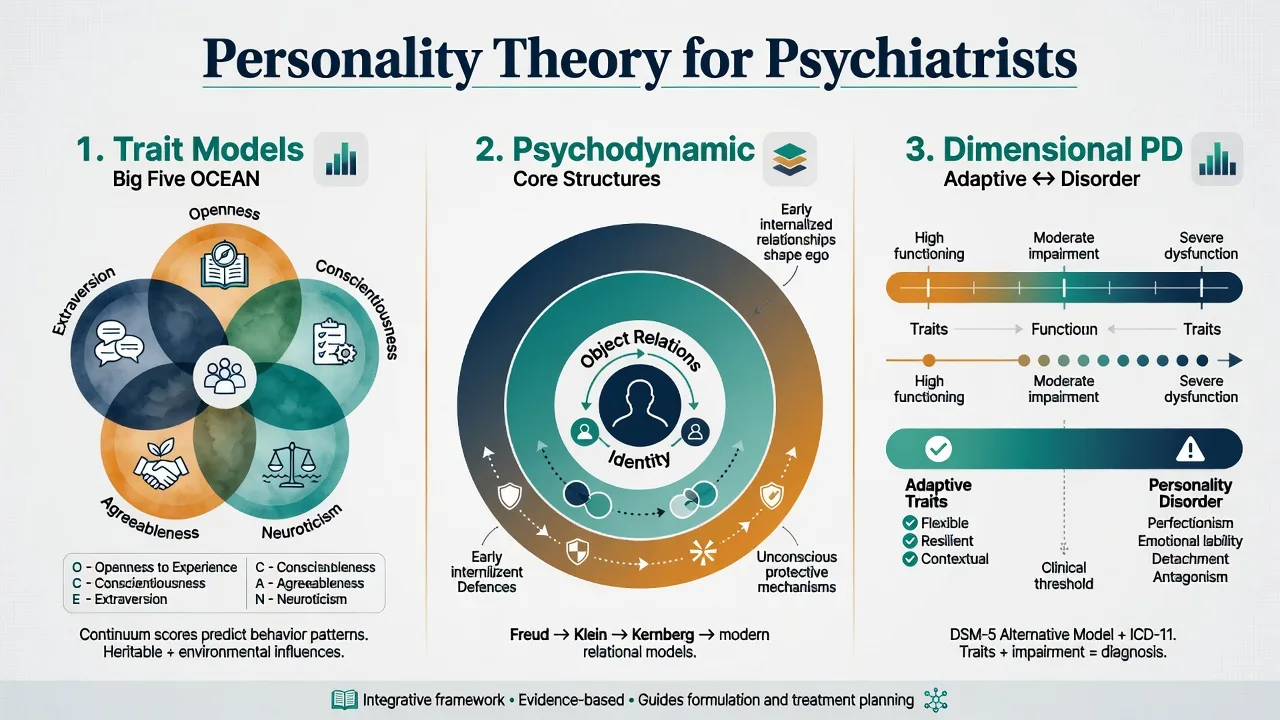
Personality denotes relatively enduring patterns of cognition, affect, impulse regulation, and interpersonal behaviour that are characteristic of the individual. Traits are dimensional individual differences that are relatively stable, situationally generalisable, and measurable by self- and informant-report. Temperament emphasises early-appearing, biologically influenced reactivity and regulation; character emphasises self-concept, goals, and values-shaped patterns (Cloninger’s distinction is examinable even when one prefers FFM language clinically).[1][2][5]
Five-Factor Model (Big Five / OCEAN)
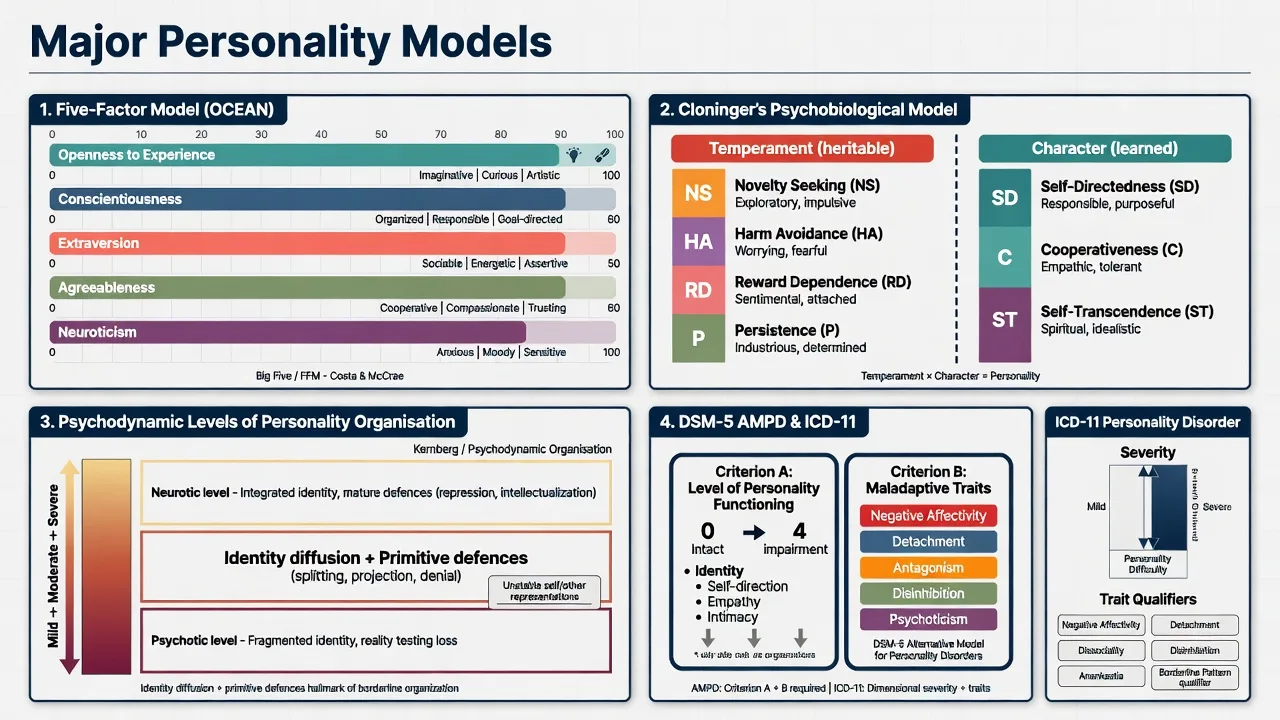
The Five-Factor Model is the dominant descriptive taxonomy of normal-range personality: Openness, Conscientiousness, Extraversion, Agreeableness, and Neuroticism. It emerged from lexical and questionnaire traditions and shows robust cross-instrument and observer agreement; trait structure appears broadly cross-cultural as a human universal at the domain level.[1][2][3][4]
| Domain | High pole (examples) | Low pole (examples) | Clinical relevance |
|---|---|---|---|
| Openness | Curious, imaginative | Conventional, concrete | Therapy engagement style; not pathology per se |
| Conscientiousness | Organised, dutiful | Disorganised, impulsive | Adherence, externalising risk when low |
| Extraversion | Sociable, assertive | Reserved, low energy | Activity scheduling; detachment spectrum |
| Agreeableness | Cooperative, trusting | Antagonistic, suspicious | Alliance, aggression risk when low |
| Neuroticism | Anxious, mood-reactive | Emotionally stable | Broad internalising vulnerability |
Other trait systems examiners still test
- Eysenck PEN (summary): Psychoticism, Extraversion, Neuroticism — historically important; modern practice largely migrated to FFM/hierarchical models.[1][2]
- Cloninger psychobiological model: Temperament dimensions — novelty seeking, harm avoidance, reward dependence, persistence — and character dimensions — self-directedness, cooperativeness, self-transcendence. Low self-directedness and cooperativeness were linked conceptually to personality disorder liability in the original framework.[5]
- Affective temperament links: High negative affectivity / neuroticism and low positive affectivity / extraversion map onto mood and anxiety vulnerability in the tripartite and temperament literature.[6][7]
Psychodynamic and cognitive-interpersonal frames
Psychodynamic teaching for exams is mechanism-focused, not school loyalty; Level of Personality Functioning work explicitly synthesises psychodynamic self and interpersonal constructs for dimensional assessment.[15]
- Levels of personality organisation (Kernberg tradition): identity integration vs diffusion; mature vs primitive defences (splitting, projective identification); reality-testing continuum from neurotic through borderline to psychotic organisation — concepts that feed modern functioning scales.[15]
- Attachment templates as enduring relational expectations that colour transference and help-seeking, relevant to intimacy and empathy domains of functioning.[15]
- Cognitive-interpersonal: early maladaptive schemas, interpersonal circumplex (agency and communion), and social-cognitive person variables that maintain interpersonal cycles and map onto trait–disorder associations.[8][12]
These frames explain why interviews feel stormy or empty even when DSM criteria are still being counted, and why Criterion A functioning is assessed separately from trait lists.[15]
From categories to dimensions (PD nosology)
DSM-5-TR retains categorical Section II personality disorders (clusters A/B/C), while dimensional alternatives address comorbidity and severity more cleanly.[13][14] Parallel dimensional systems are now examinable essentials:
- AMPD (Alternative Model for Personality Disorders): Criterion A — Level of Personality Functioning (identity, self-direction, empathy, intimacy); Criterion B — pathological personality traits. Maladaptive trait domains were operationalised in the PID-5 inventory (negative affectivity, detachment, antagonism, disinhibition, psychoticism).[10][15]
- ICD-11: diagnose personality disorder by severity of self and interpersonal dysfunction, then apply trait domain qualifiers (and, where used, a borderline pattern qualifier). Clinical application papers emphasise severity-first thinking and reduced artificial comorbidity of multiple categorical labels.[13][14]
Personality pathology is best understood as extreme, inflexible trait configurations plus impairment, continuous with normal-range individual differences rather than a separate species of person. Meta-analytic work links FFM domains/facets systematically to DSM categorical PD constructs.[12]
Epidemiology and risk (theory lens)
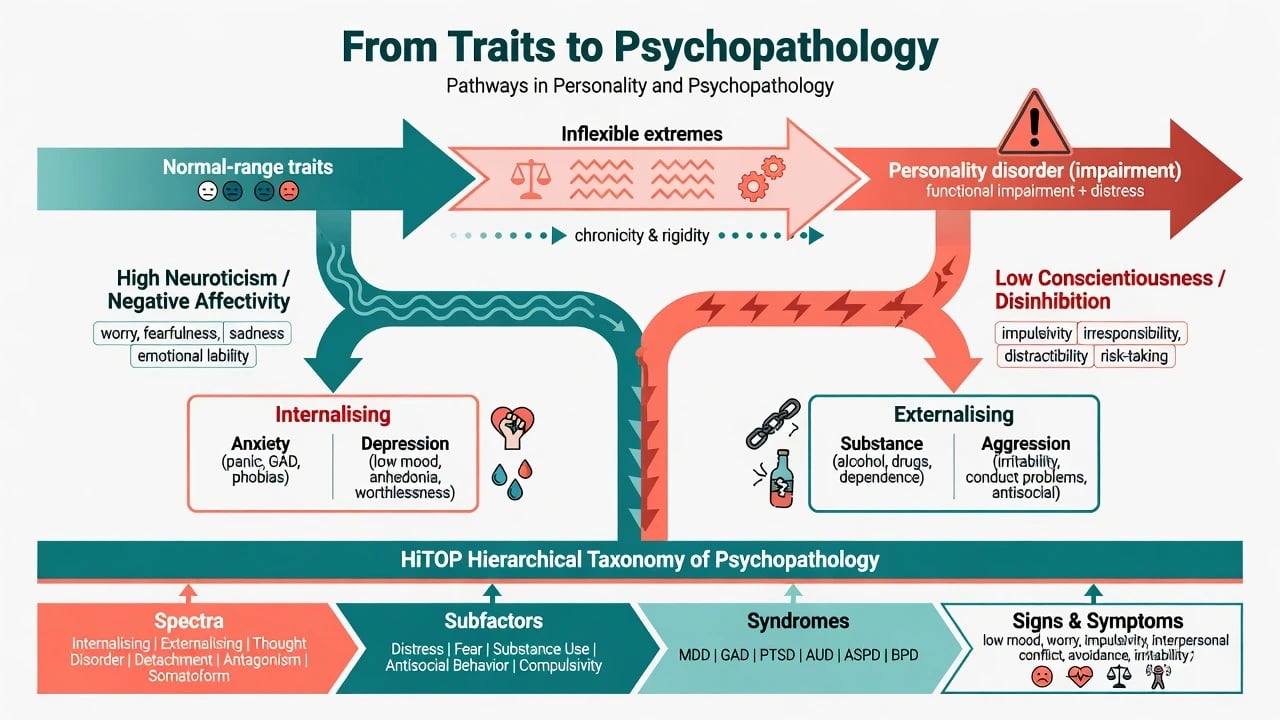
Personality theory predicts non-random comorbidity. Meta-analysis links high neuroticism strongly to anxiety and depressive disorders, with conscientiousness and other domains showing patterned associations including substance-related outcomes.[8] Common mental disorders show internalising–externalising structure that personality dimensions help explain.[9][11]
Lifespan: traits show substantial rank-order stability in adulthood, yet mean-level change continues — the so-called maturity principle pattern of mean increases in agreeableness and conscientiousness and decreases in neuroticism across much of adult development in longitudinal meta-analysis.[16] This undercuts fatalistic “personality never changes” viva answers.
Service risk: high N, low A, and low C configurations predict interpersonal conflict, missed appointments, and alliance rupture — formulation targets, not moral judgements.[8][12]
Pathophysiology and mechanisms
Descriptive structure, not one biology
FFM domains summarise phenotypic covariance; they are not a complete molecular theory, but they are robust descriptive structure across instruments and cultures.[1][3][4] Useful clinical mechanism language includes:
- Negative affectivity / neuroticism as a shared liability for internalising syndromes.[6][7][8]
- Disinhibition / low conscientiousness as a liability toward externalising behaviour and substance problems.[8][9]
- Hierarchical quantitative models (HiTOP) placing syndromes and personality pathology in spectra rather than siloed categories.[11]
Continuum to disorder
Moving from adaptive trait variation to personality disorder requires inflexibility, pervasiveness, and clinically significant impairment or distress, not eccentricity alone. Severity of self and interpersonal dysfunction is the organising axis in ICD-11 and AMPD Criterion A.[13][14][15]
Object-relations mechanisms (exam depth)
When identity is diffuse and defences are primitive, relationships oscillate between idealisation and devaluation; teams split; risk can escalate quickly under abandonment cues. This is compatible with trait elevations (e.g. negative affectivity, antagonism, disinhibition) but adds a structural account of interpersonal chaos that pure trait lists under-specify — the clinical rationale for measuring self and interpersonal functioning alongside traits.[10][15]
State versus trait
Acute depression, mania, psychosis, intoxication, and withdrawal distort self-report and interviewer impression of neuroticism, impulsivity, and suspiciousness. Stabilise first; reassess enduring patterns with collateral and longitudinal data.[7][8]
Clinical presentation (how theory shows up)
- High N: chronic worry, mood reactivity, catastrophic appraisal, reassurance seeking, intolerance of uncertainty.
- Low E / detachment: sparse relationships, anhedonic social withdrawal (discriminate from major depression episode).
- Low A / antagonism: entitlement, callousness, conflict with staff, legal friction.
- Low C / disinhibition: non-adherence, chaotic planning, impulsive self-harm or substance use.
- High O: sometimes mistaken for thought disorder when metaphorical speech is culturally or creatively normal — context matters.
- Criterion A failures: unstable self-image, aimlessness, empathy deficits, intimacy instability — AMPD language for what older notes called “personality structure.”[10][15]
Differential — discriminators
| Question | Favours enduring personality pattern | Favours alternative |
|---|---|---|
| Onset | Adolescence/early adulthood, long course | Abrupt mid/late life change → organic/substance |
| Pervasiveness | Across roles and relationships | Only in one relationship or workplace conflict |
| State illness | Persists after mood/psychosis remits | Tracks episode and remits with it |
| Neurodevelopment | No early social-communication disorder story | Lifelong autism/ADHD features explain social style |
| Culture | Impairment within cultural norms | Normative reserve/assertiveness misread as pathology |
| Functioning | Clear self/interpersonal dysfunction (LPFS/ICD-11) | Trait eccentricity without impairment |
Assessment (bedside personality science)
- Longitudinal history and collateral — onset, cross-context pervasiveness, work/relationship patterns.
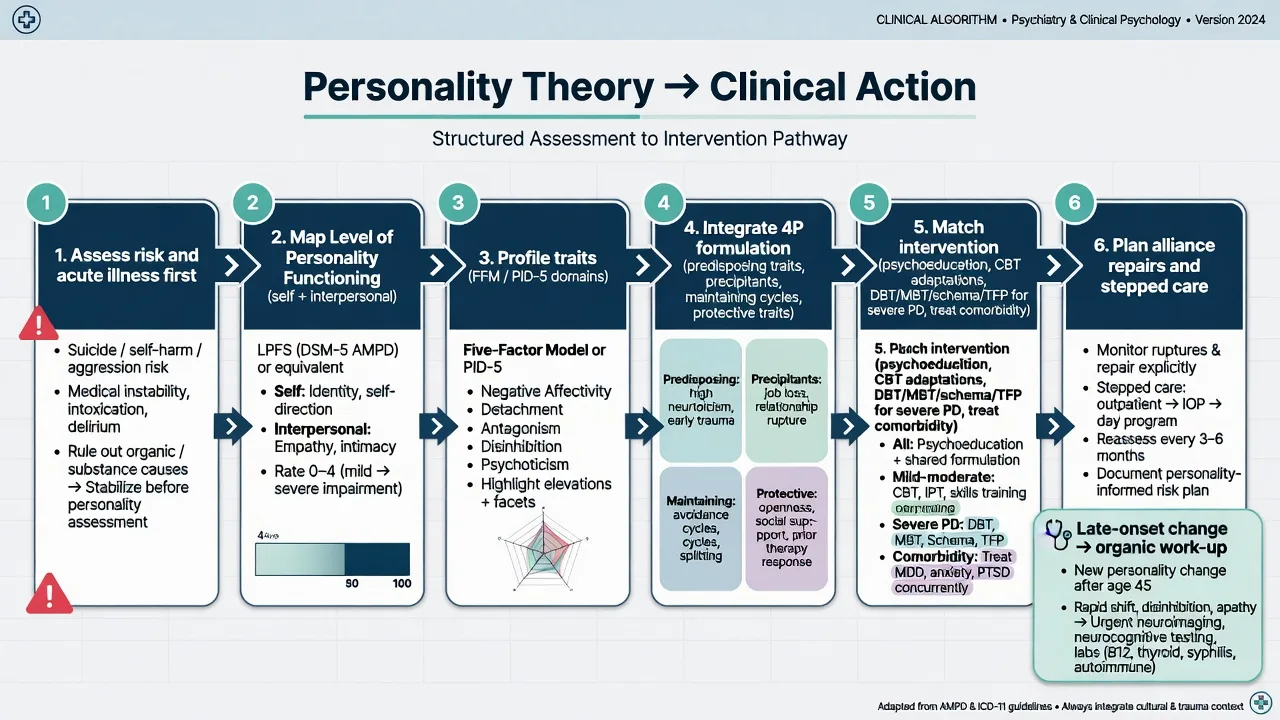
- Level of Personality Functioning — identity, self-direction, empathy, intimacy (AMPD Criterion A lineage).[15]
- Trait profile — clinical estimate of FFM domains and/or AMPD/PID-5 domains (negative affectivity, detachment, antagonism, disinhibition, psychoticism).[1][10]
- Categorical tools when required — SCID-5-PD / IPDE for coding, research, or service criteria that still demand Section II labels.
- Interview process data — idealisation/devaluation, entitlement, dependency, mentalisation failures.
- Always screen risk, trauma, substances, neurodevelopment, and medical contributors before locking the formulation.
Investigations
No laboratory assay diagnoses a personality type. Investigate organic personality change when onset is late or abrupt (traumatic brain injury, frontotemporal syndromes, epilepsy, endocrine, autoimmune encephalitis, substance-related). Psychometrics are adjuncts: interpret with validity concerns and state effects. Order metabolic/ECG baselines when pharmacotherapy for comorbidity is planned — not because traits require blood tests.[13]
Acute / emergency management
Definitive management (using theory)
Formulation before technique
Integrate personality into a 4P map: predisposing traits (e.g. high N, low C), precipitants (loss, rejection, status threat), maintaining interpersonal cycles (avoidance, antagonism, reassurance traps), protective traits (conscientiousness facets, adaptive agreeableness, support). HiTOP/internalising–externalising language can organise comorbidity without endless dualism debates.[8][9][11]
Matching interventions to mechanisms
- Psychoeducation about traits as tendencies, not moral verdicts — improves alliance and self-efficacy for change, consistent with viewing traits as dimensional liabilities rather than moral defects.[1][8]
- Axis I protocols adapted for traits: high N needs emotion-regulation scaffolding; low C needs graded structure and problem-solving; low A needs firm, respectful boundaries, reflecting trait–disorder linkage patterns.[8][12]
- Specialist PD psychotherapies (DBT, MBT, TFP, schema therapy, good psychiatric management) when severity of personality dysfunction is moderate–severe — mechanisms target emotion dysregulation, mentalising failure, identity diffusion, and maladaptive schemas rather than “fixing a type.” Severity guides intensity of care.[13][14]
- Pharmacotherapy treats comorbid syndromes and cross-cutting symptom domains; it is not a primary treatment for “being an introvert” or “having high N.” Personality classification reviews emphasise psychosocial and structured therapies as core for PD-level dysfunction.[13]
Alliance engineering
Predict ruptures from antagonism, detachment, and rejection sensitivity. Name process early; repair explicitly; keep multi-agency messages consistent so the care system does not re-enact object-relations splits — a practical implication of impaired interpersonal functioning on Criterion A / ICD-11 severity axes.[13][15]
Guidelines (regional deltas)
ICD-11 is the WHO dimensional clinical standard many jurisdictions will increasingly code against (severity + traits). DSM-5-TR keeps categorical Section II for everyday US-influenced coding while AMPD remains an official alternative model. NICE / RANZCP / APA guidance for borderline and related presentations emphasises structured psychological therapies and risk-aware continuity of care; quote local commissioning pathways in viva, but mechanism language (functioning + traits + evidence-based psychotherapy) is shared.[13][14]
Subtypes and scenarios
| Scenario | Theory lever | Clinical move |
|---|---|---|
| Recurrent depression + high N | Internalising diathesis | Relapse prevention, emotion regulation, not only episode care |
| Substance relapse + low C | Disinhibition / externalising | Contingency structure, skills before insight-only work |
| Team splits + idealisation/devaluation | Borderline organisation / low mentalising | Consistent team, MBT/DBT elements, boundary clarity |
| Forensic assessment | Traits inform, do not replace risk tools | Structured risk + personality formulation |
| Perinatal crisis | Attachment activation + trait vulnerability | Risk, mother–infant focus, sleep and support |
| “Difficult patient” stigma | Formulation failure | Re-map functioning/traits/comorbidity; restore care |
Complications and pitfalls
- Diagnostic overshadowing of mood, bipolar, PTSD, ADHD, autism, and substance use.
- State–trait confusion during acute illness.
- Cultural pathologising of normative interpersonal styles.
- Reifying one cluster when a dimensional profile is cleaner.
- Therapeutic nihilism — mean-level trait change and functioning gains occur; specialist therapies exist for severe PD.[13][16]
- System splits mirroring patient object relations.
Prognosis and disposition
Trait rank-order stability coexists with meaningful mean-level change and treatment-related functional improvement.[16] Severity of personality dysfunction predicts intensity of need more than any single colourful trait. Protective conscientiousness and supportive relationships improve adherence and recovery capital. Match follow-up intensity to severity, comorbidity, and risk — not to pejorative reputation.[13][14]
Special populations
- Adolescents: emerging patterns; intervene on impairment without premature lifelong identity as “disorder only,” while still recognising that PD-level dysfunction can present in youth services.[13]
- Older adults: late change is an organic red flag; lifelong traits may express differently with frailty and loss, and mean-level trait change continues across adulthood.[13][16]
- Intellectual disability: adapt language; separate behavioural phenotypes from moralised “personality,” and assess functioning with developmental context.[13][15]
- Cultural and Indigenous contexts: co-define healthy relatedness; use cultural formulation — FFM structure is broadly cross-cultural, but expression and impairment thresholds require local partnership.[4][13]
- Minority stress: do not pathologise identity; measure discrimination-related distress separately from trait structure and avoid pejorative PD labelling that blocks care.[13]
Evidence pearls (named)
- McCrae and John 1992; Goldberg 1993; McCrae and Costa 1987/1997 — FFM description, phenotypic structure, validation, cross-cultural generality.[1][2][3][4]
- Cloninger 1993 — temperament and character psychobiological model.[5]
- Clark and Watson 1991; Clark, Watson, and Mineka 1994 — tripartite affect and temperament–psychopathology links.[6][7]
- Kotov 2010 — meta-analytic Big Trait–disorder links; Krueger 1999 — common mental disorder structure; Kotov 2017 HiTOP — hierarchical alternative.[8][9][11]
- Krueger 2012 PID-5; Bender 2011 LPFS; Samuel and Widiger 2008 — maladaptive traits, functioning assessment, FFM–PD meta-links.[10][12][15]
- Tyrer 2015; Bach and First 2018 — PD classification/prevalence impact and ICD-11 application.[13][14]
- Roberts 2006 — lifespan mean-level trait change meta-analysis.[16]
Exam pearls
Classic stem traps
- Equating introversion with schizoid personality disorder without impairment criteria.[1][13]
- Diagnosing PD during untreated major depression (state–trait confusion).[7][8]
- Listing five categorical PDs instead of one severity rating plus traits.[13][14]
- Claiming personality is immutable despite lifespan change data and therapy evidence.[16][13]
- Inventing drug doses “for personality type” without a comorbid target syndrome.[13]
Related topics
Borderline PD, cluster A/C, narcissistic/cluster B spectrum, ICD-11 dimensional PD, biopsychosocial formulation, attachment theory, MBT, DBT/third-wave therapies, and psychodynamic supportive work are the natural clinical extensions of this foundations map.[13][15]
References
- [1]McCrae RR, John OP An introduction to the five-factor model and its applications J Pers, 1992.PMID 1635039
- [2]Goldberg LR The structure of phenotypic personality traits Am Psychol, 1993.PMID 8427480
- [3]McCrae RR, Costa PT Validation of the five-factor model of personality across instruments and observers J Pers Soc Psychol, 1987.PMID 3820081
- [4]McCrae RR, Costa PT Personality trait structure as a human universal Am Psychol, 1997.PMID 9145021
- [5]Cloninger CR, Svrakic DM, Przybeck TR A psychobiological model of temperament and character Arch Gen Psychiatry, 1993.PMID 8250684
- [6]Clark LA, Watson D Tripartite model of anxiety and depression: psychometric evidence and taxonomic implications J Abnorm Psychol, 1991.PMID 1918611
- [7]Clark LA, Watson D, Mineka S Temperament, personality, and the mood and anxiety disorders J Abnorm Psychol, 1994.PMID 8040472
- [8]Kotov R, Gamez W, Schmidt F, Watson D Linking "big" personality traits to anxiety, depressive, and substance use disorders: a meta-analysis Psychol Bull, 2010.PMID 20804236
- [9]Krueger RF The structure of common mental disorders Arch Gen Psychiatry, 1999.PMID 10530634
- [10]Krueger RF, Derringer J, Markon KE, Watson D, Skodol AE Initial construction of a maladaptive personality trait model and inventory for DSM-5 Psychol Med, 2012.PMID 22153017
- [11]Kotov R, Krueger RF, Watson D, et al. The Hierarchical Taxonomy of Psychopathology (HiTOP): A dimensional alternative to traditional nosologies J Abnorm Psychol, 2017.PMID 28333488
- [12]Samuel DB, Widiger TA A meta-analytic review of the relationships between the five-factor model and DSM-IV-TR personality disorders: a facet level analysis Clin Psychol Rev, 2008.PMID 18708274
- [13]Tyrer P, Reed GM, Crawford MJ Classification, assessment, prevalence, and effect of personality disorder Lancet, 2015.PMID 25706217
- [14]Bach B, First MB Application of the ICD-11 classification of personality disorders BMC Psychiatry, 2018.PMID 30373564
- [15]Bender DS, Morey LC, Skodol AE Toward a model for assessing level of personality functioning in DSM-5, part I: a review of theory and methods J Pers Assess, 2011.PMID 22804672
- [16]Roberts BW, Walton KE, Viechtbauer W Patterns of mean-level change in personality traits across the life course: a meta-analysis of longitudinal studies Psychol Bull, 2006.PMID 16435954