Psych · foundations
Philosophy of mind and psychiatry
Also known as Mind-body problem psychiatry · Philosophy of psychiatry · Explanatory pluralism · Biopsychosocial model philosophy · Free will psychiatry · Phenomenology and mind · Values-based practice
Exam-exhaustive fellowship atlas on philosophy of mind applied to psychiatry — dualism and monism, consciousness, free will and responsibility, explanatory pluralism and levels of explanation (Kendler), biopsychosocial model (Engel and Ghaemi), Jaspersian phenomenology, values-based practice, capacity, and multi-board exam pearls. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Philosophy of mind is the systematic study of consciousness, intentionality, personal identity, free will, and the mind-body relation. Philosophy of psychiatry applies those tools to psychiatric kinds, explanation, values, and clinical ethics. It is not a substitute for descriptive psychopathology or for organic medicine: it disciplines how registrars talk about cause, self, and responsibility when the stakes are formulation, capacity, teaching, and forensic interfaces. [4][9]
| Domain | Core question | Clinical pay-off |
|---|---|---|
| Philosophy of mind | What is a mental state? How does mind relate to brain? | Avoid crude dualism or crude biologism in explanations |
| Philosophy of psychiatry | What is mental disorder? How should psychiatry explain and value? | Sharper formulation, capacity talk, teaching |
| Descriptive psychopathology | What is the form of this experience? | MSE language before theory |
| Classification (DSM/ICD) | Does this pattern meet criteria? | Shared codes, not metaphysics |

Classification of mind-body positions
Dualism and monism
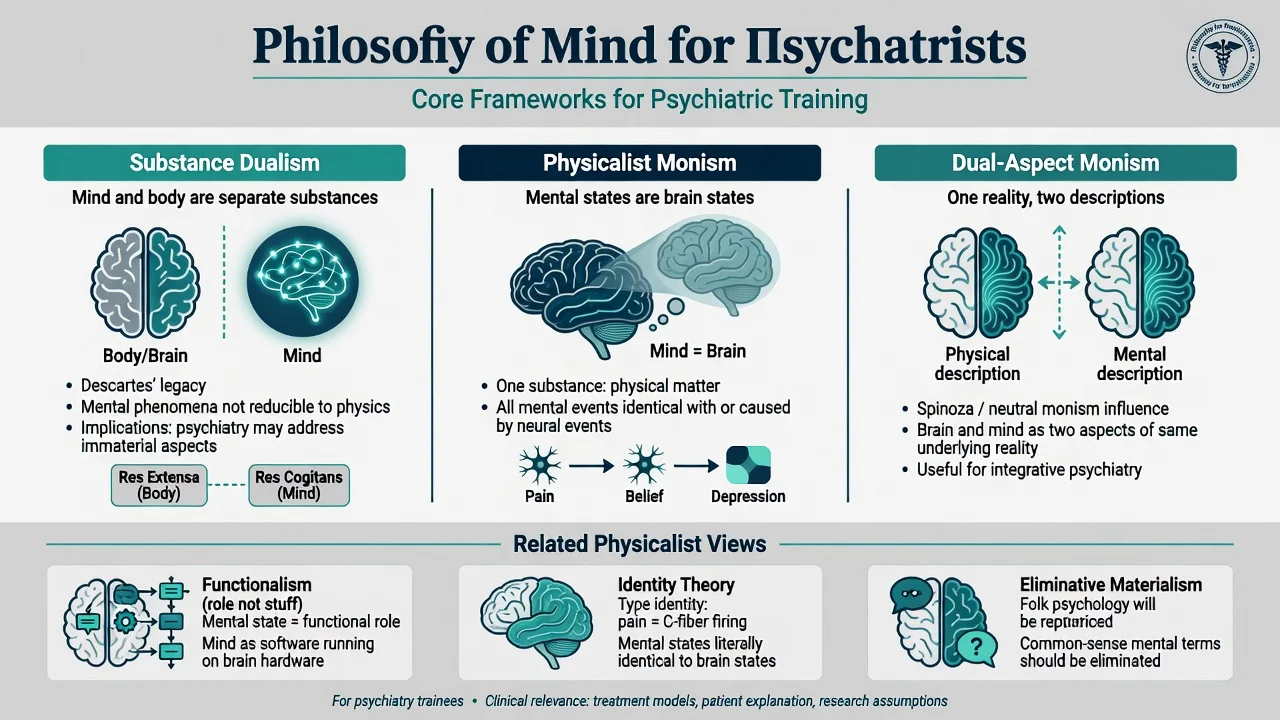
- Substance dualism — mind and body as distinct kinds of substance (classical Cartesian teaching frame). Clinically rare as explicit metaphysics; common as folk dualism ("the body is sick or the mind is sick").
- Property dualism — one substance (often physical) with irreducible mental properties.
- Physicalist monism (materialism) — mental states are, or wholly depend on, physical states.
- Idealism — reality fundamentally mental (rarely exam-operational in clinical stations).
- Dual-aspect monism — one underlying reality described under mental and physical aspects.
Theories of mental states (exam sentences)
| Theory | One-line claim | Psychiatric use / trap |
|---|---|---|
| Type-identity | Mental state types are brain state types | Supports biomarker hopes; overclaims if "type" identity is treated as already solved |
| Functionalism | Mental states are defined by causal roles, not by what they are made of | Fits multilevel interventions (drug and psychotherapy can share functional targets differently) |
| Eliminative materialism | Folk-psychological terms (belief, desire) will be eliminated by mature neuroscience | Risk: erases first-person experience and MSE language |
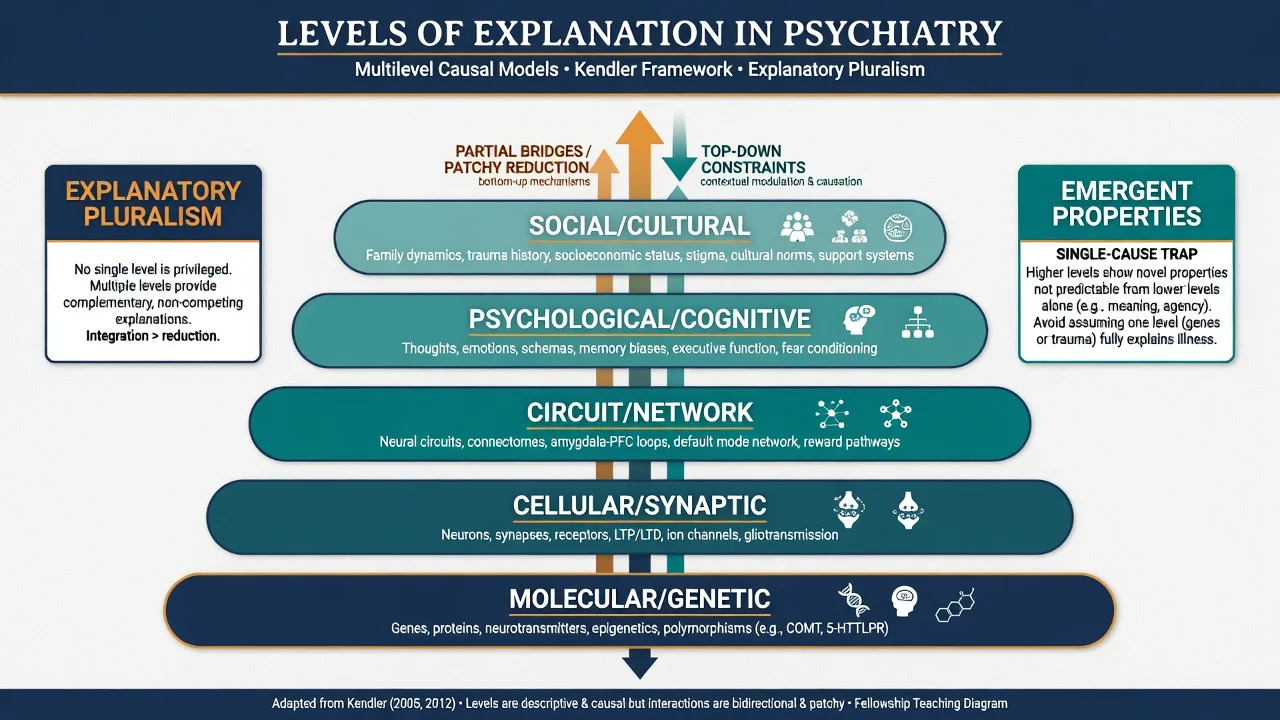
Kendler argued psychiatry needs an explicit philosophical structure: reject pure dualism and pure reductionist monism as practice guides; prefer a scientifically literate physicalism that still permits multiple levels of explanation and only patchy reduction across levels. [4]
Epidemiology of philosophical error (clinical stakes)
Philosophy fails clinically not by exam MCQ wrong answers but by error modes that change care — crude dualism (medical symptoms ignored as "psychological," or distress dismissed as "not real"), strong reductionism, empty biopsychosocial checklists, neuro-determinist overclaim, and checklist culture without phenomenological form. [3][5][6][9][11]
- Crude dualism — medical symptoms ignored as "psychological"; or psychological distress dismissed as "not real." [4]
- Crude reductionism — one transmitter or one scan treated as the illness; psychosocial causation erased. [5][6]
- Empty biopsychosocialism — three boxes ticked without hypotheses or priorities. [3]
- Neuro-determinist overclaim — imaging used to assert that free will and responsibility are myths. [11]
- Phenomenology death — criteria checklists without form of experience. [9]
High-stakes arenas: first-episode formulation, capacity and consent, forensic reports, CASC values stations, and teaching that shapes the next cohort of MSE skills. [9][10][11]
Pathophysiology as levels of explanation
Not one mechanism monologue
For this topic, "pathophysiology" means how psychiatrists should structure causal talk. Kendler distinguishes levels of explanation (for example molecular, cellular, neural system, psychological, and social) and shows that psychiatric causes are typically dappled — many kinds of cause, incomplete cross-level mapping, not a clean hardware/software split. [6][7]
Explanatory models for psychiatric illness must state which level a claim lives on, what evidence would support it, and what would not follow (for example a heritability estimate does not by itself dictate drug versus psychotherapy). [5]
Reductionism, pluralism, emergence
- Strong reductionism — higher-level talk is dispensable once lower-level mechanisms are known.
- Explanatory pluralism — legitimate explanations coexist at multiple levels; partial reduction is possible ("patchy") without full collapse of psychology into molecular biology. [4][5]
- Emergence — higher-level regularities not usefully eliminated even if dependent on lower levels.
Pluralism is not relativism: each hypothesis still needs methods appropriate to its level. [5][7]
Consciousness and self
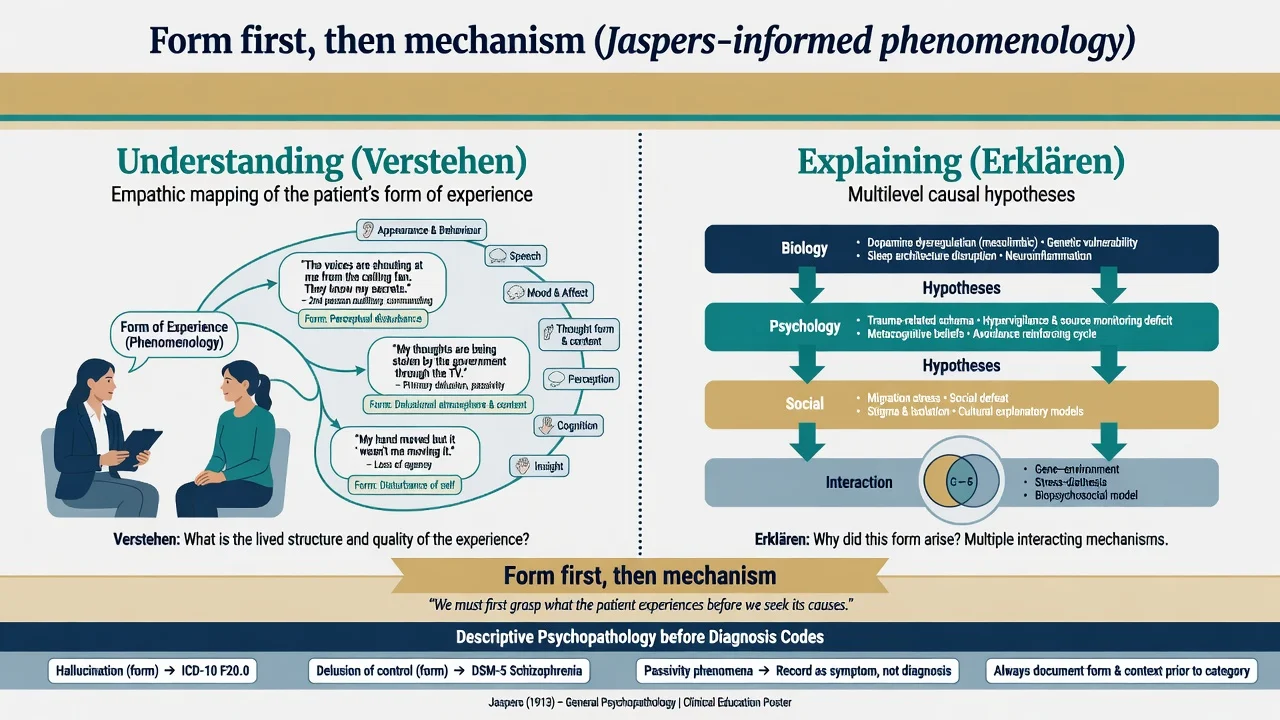
The "hard problem" of consciousness (why physical processing is accompanied by experience) is a research and conceptual problem; clinically, psychiatry works with access to reportable mental contents, with disorders of self and agency, and with first-person form. Sass and Parnas frame schizophrenia-spectrum experience as disturbance of minimal self (ipseity) — hyperreflexivity and diminished self-affection — a phenomenological model of consciousness and self, not a completed neurocircuit proof. [8]
Andreasen warned that operational criteria without phenomenological training can hollow out the skill of describing experience — an unintended consequence of checklist culture. [9]
Clinical presentation: how philosophy shows up at the bedside
| Presentation pattern | Philosophical reading | Clinical move |
|---|---|---|
| "Either my body is broken or I am weak-minded" | Folk dualism | Validate distress; explain multilevel causation without shaming |
| "Scan will find the chemical and that is the whole story" | Strong reduction hope | Share what biomarkers can and cannot settle |
| Passivity, thought insertion, depersonalisation | Agency and self as lived structure | Describe form first; then multilevel hypotheses [8] |
| Values clash over treatment goals | Fact-value entanglement | Values-based shared decisions [12] |
| "My brain made me do it, so I am not responsible" | Hard determinism claim | Separate scientific causation from legal/moral responsibility frameworks [11] |
Insight (philosophical undertone)
Insight is not a single on/off metaphysical property of the person. Multidimensional clinical insight (awareness of illness, relabelling of experiences, attitude to treatment) sits at the intersection of epistemology (what is believed true) and evaluation (what help is needed). Lack of insight is not identical to incapacity. [10]
Differential: conceptual discriminators
| Confusion pair | Discriminator |
|---|---|
| Substance dualism vs clinical "mind or body" talk | Metaphysics vs patient explanatory model; treat the latter as clinical data |
| Reductionism vs eliminativism | Reduction keeps higher-level terms as derived; eliminativism scraps them |
| Understanding (Verstehen) vs explaining (Erklären) | Empathic grasp of meaning/form vs causal mechanism (Jaspers-informed teaching) |
| Hard determinism vs compatibilism | Whether responsibility language can survive causal explanation of action [11] |
| Empty BPS vs multilevel formulation | Boxes vs prioritised, testable hypotheses at named levels [2][3] |
| Insight vs capacity | Multidimensional illness attitudes vs decision-specific abilities [10] |
Bedside assessment
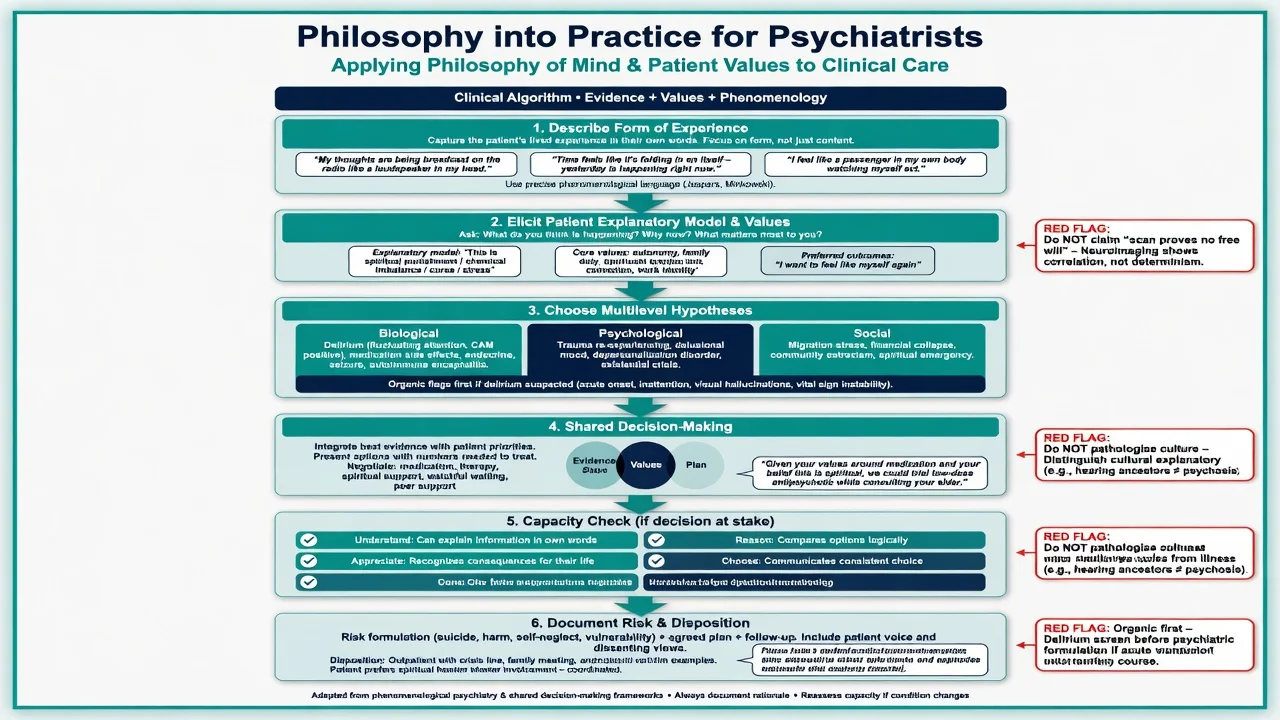
- Describe form with quotes (perception, thought form/content, self/agency, mood/affect) before theory. [9]
- Elicit explanatory models — what the person thinks is happening in mind and body — without collusion or humiliation.
- Map levels you will use in formulation (biological, psychological, social) with at least one concrete hypothesis each when relevant. [2][5]
- Capacity when a decision is at stake — Appelbaum clinical frame: ability to understand relevant information, appreciate its significance for oneself, reason about options, and express a choice. Capacity is decision-specific and can fluctuate. [10]
- Values — what outcomes matter to this person; integrate with evidence rather than smuggling clinician values as pure facts. [12]
- Organic first if phenomenology forces it (fluctuating attention, fever, focal signs) — philosophy never postpones medicine.
Investigations (epistemic role)
Investigations test level-specific hypotheses (metabolic panel for delirium risk; imaging when indicated; cognitive testing as adjunct). They do not settle whether free will exists, whether the person is a "mere machine," or whether first-person reports are unreal. [6][11]
Neuroscience findings can constrain psychological stories and vice versa under pluralism; they do not licence forensic overclaim. [6][11]
Acute and emergency management
Philosophy does not change the emergency ladder: medical stabilisation and delirium pathway when indicated; risk containment for self-harm, violence, or severe neglect; and urgent capacity-related decisions that use functional abilities rather than a viva on determinism. [10][11]
Definitive management as applied philosophy
Multilevel formulation (operational pluralism)
Engel argued for a medical model that includes biological, psychological, and social determinants in clinical method — not as soft decoration but as part of scientific medicine. [1][2] Ghaemi later argued the biopsychosocial label often became an unfalsifiable eclecticism that avoided hard choices among models. [3] Fellowship synthesis: keep multilevel thinking, demand prioritised hypotheses, and reject empty checklists. [3][5]
Pharmacotherapy and psychotherapy
Under pluralism, drugs and psychological therapies can target different levels or different aspects of the same functional problem. Choosing both is not dualist inconsistency; claiming they "cancel" because mind is "really just chemistry" is a philosophical error, not a pharmacology result. [4][5]
Values-based practice
Evidence-based care needs explicit work with patient values in shared decision-making; Fulford and colleagues provide resources for bringing values into clinical decisions without abandoning science. [12]
Teaching and serial MSE
Defend phenomenological skill: serial form-focused MSE tracks change at the level of experience while biomarkers, if used, track other levels. [9]
Subtypes and high-yield scenarios
Biopsychosocial formulation stations
State Engel's clinical intent, name Ghaemi's critique, then produce a non-empty multilevel plan with priorities and what would change management if a hypothesis were wrong. [2][3]
Forensic free will
Pierre reviews neuroscience of free will debates for psychiatrists: experimental work on volition is often over-read; clinical and legal responsibility frameworks typically need compatibilist literacy (actions can be caused and still be attributable to agents under law) rather than claiming neuroscience dissolved responsibility. Do not invent local statute numbers. [11]
Psychosis and the self
Self-disorder frameworks test theories of minimal self and consciousness in the clinic; they deepen description, they do not replace risk assessment or criteria-based diagnosis. [8]
Nosology as philosophy of science
Classification systems encode practical and scientific commitments about kinds, thresholds, and utility. Philosophy of nosology asks whether psychiatric categories are natural kinds, practical kinds, or hybrids — relevant when examiners ask "what is a disorder?" [4][5]
Complications and pitfalls
| Pitfall | Correction |
|---|---|
| BPS as three empty boxes | Prioritised, level-tagged hypotheses [3] |
| Scan proves no free will | Overclaim; separate science of volition from legal responsibility [11] |
| Checklist without form | Rebuild phenomenological skill [9] |
| Insight = incapacity | Use decision-specific abilities [10] |
| Cultural mind-body models as delusion | Formulation and cultural humility before label |
| Metaphysics delays CT/LP when indicated | Medicine first |
Prognosis and disposition
Philosophical literacy improves quality of formulation, alliance, and teaching; it is not a prognostic biomarker. Disposition still follows syndrome severity, risk, capacity, supports, and treatability. Handover structure: form (quotes) → risk → multilevel hypotheses → plan and values. [5][10]
Special populations
- Children and adolescents — developing agency language; avoid adult free-will rhetoric; caregivers' explanatory models matter.
- Older adults — capacity and values in dementia and depression treatment choices; fluctuating capacity. [10]
- Intellectual disability — supported decision-making; respect values; do not equate cognitive impairment with global incapacity. [10]
- Cultural and Indigenous contexts — mind-body and spiritual models require formulation skill, not automatic pathologising.
- Forensic — responsibility, intent, and the limits of neuroprediction; document clinical findings, not metaphysical verdicts. [11]
Evidence and guidelines (named anchors)
| Anchor | Claim for exams |
|---|---|
| Engel 1977 / 1980 | BPS as challenge to narrow biomedicine; clinical method including multilevel data [1][2] |
| Ghaemi 2009 | BPS often failed as vague eclecticism [3] |
| Kendler 2005 / 2008 / 2012 | Philosophical structure; explanatory models; levels; dappled causes [4][5][6][7] |
| Sass and Parnas 2003 | Consciousness/self framework for schizophrenia-spectrum phenomenology [8] |
| Andreasen 2007 | Phenomenology erosion under pure operationalism [9] |
| Appelbaum 2007 | Competence/capacity abilities for treatment consent [10] |
| Pierre 2014 | Free will neuroscience implications for psychiatry [11] |
| Fulford and Handa 2021 | Patient values in shared clinical decisions [12] |
FRANZCP — essay/viva depth on models of mind, formulation philosophy, ethics of responsibility and capacity. MRCPsych — Paper A history and philosophy of psychiatry; CASC values and explanation. ABPN — ethics, capacity, and conceptual literacy. MD/DNB — viva definitions of dualism, BPS, free will, and phenomenology. Always pair concept with clinical application; never invent jurisdiction-specific section numbers. [4][10][11][12]
Exam pearls
- Form → mechanism → metaphysics is the safe order. [9]
- Explanatory pluralism means multiple legitimate levels, not "anything goes." [4][5]
- BPS: defend multilevel method (Engel); attack empty triad (Ghaemi). [1][3]
- Dappled causes beat single-cause slogans. [6]
- Compatibilism literacy for free will stations; neuroscience of volition is not a guilt machine. [11]
- Capacity = understand, appreciate, reason, choose (decision-specific). [10]
- Values are data for shared decisions, not noise. [12]
- Self-disorder language deepens psychosis phenomenology when asked. [8]
- Do not equate insight failure with incapacity. [10]
- Do not let dualism talk delay organic pathways.
Summary
Philosophy of mind and psychiatry is fellowship infrastructure: dualism and monism name the mind-body options; Kendler-style explanatory pluralism and levels of explanation structure formulation; Engel's biopsychosocial method survives only if rescued from Ghaemi's empty-triad critique; phenomenology protects first-person form; values and capacity operationalise ethics; and free will literacy prevents neuro-rhetoric from replacing clinical and legal responsibility talk. Master the discriminators, cite the named anchors, and always return to safe care. [1][3][4][9][10][11][12]
References
- [1]Engel GL The need for a new medical model: a challenge for biomedicine Science, 1977.PMID 847460
- [2]Engel GL The clinical application of the biopsychosocial model Am J Psychiatry, 1980.PMID 7369396
- [3]Ghaemi SN The rise and fall of the biopsychosocial model Br J Psychiatry, 2009.PMID 19567886
- [4]Kendler KS Toward a philosophical structure for psychiatry Am J Psychiatry, 2005.PMID 15741457
- [5]Kendler KS Explanatory models for psychiatric illness Am J Psychiatry, 2008.PMID 18483135
- [6]Kendler KS The dappled nature of causes of psychiatric illness: replacing the organic-functional/hardware-software dichotomy Mol Psychiatry, 2012.PMID 22230881
- [7]Kendler KS Levels of explanation in psychiatric and substance use disorders: implications for the development of an etiologically based nosology Mol Psychiatry, 2012.PMID 21670729
- [8]Sass LA, Parnas J Schizophrenia, consciousness, and the self Schizophr Bull, 2003.PMID 14609238
- [9]Andreasen NC DSM and the death of phenomenology in america: an example of unintended consequences Schizophr Bull, 2007.PMID 17158191
- [10]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [11]Pierre JM The neuroscience of free will: implications for psychiatry J Psychiatr Pract, 2014.PMID 24330830
- [12]Fulford KWM, Handa A New resources for understanding patients' values in the context of shared clinical decision-making World Psychiatry, 2021.PMID 34505360