Psych · Foundations — physical examination and investigations
Physical examination and investigations in psychiatry
Also known as Medical work-up in psychiatry · Organic exclusion psychiatry · Baseline investigations psychotropics · Metabolic monitoring antipsychotics · QTc monitoring psychiatry · Physical health SMI · Neurological examination psychiatry · FEP medical clearance
Exam-exhaustive fellowship reference on physical examination and investigations in psychiatry — neurological exam essentials, tiered baseline and red-flag work-up, metabolic monitoring before and during psychotropics, ECG/QTc decision rules, when to order CT/MRI/LP/EEG/autoimmune testing, and organic exclusion algorithms. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Psychiatrists who treat the mental state as detachable from the body fail exams and fail patients. Excess cardiometabolic mortality in severe mental illness (SMI), drug-induced QTc risk, and missed encephalitis or delirium are examiner favourites because they are preventable with disciplined exam and monitoring.[4][5][6][16]

Definition and dual purpose
Physical examination and investigations in psychiatry are structured clinical processes that exclude secondary (organic/substance) causes of psychiatric presentations and establish a medical baseline and monitoring plan before and during psychopharmacology (metabolic, haematological, ECG, drug levels, pregnancy).[1][3]
They are not a substitute for a full medical admission when the patient is medically unstable, and they are not a rubber-stamp "medically cleared" checkbox. Freudenreich and colleagues frame first-episode psychosis (FEP) work-up as combining broad screening, selective exclusion of treatable disease informed by epidemiology and treatability, and baseline measures for future care — that triad generalises across most new and high-risk presentations.[1]
DSM-5-TR / ICD-11 secondary mental disorders due to another medical condition are endpoints after positive evidence, not default labels when you skip the exam.[1]
Investigation tiers (framework)
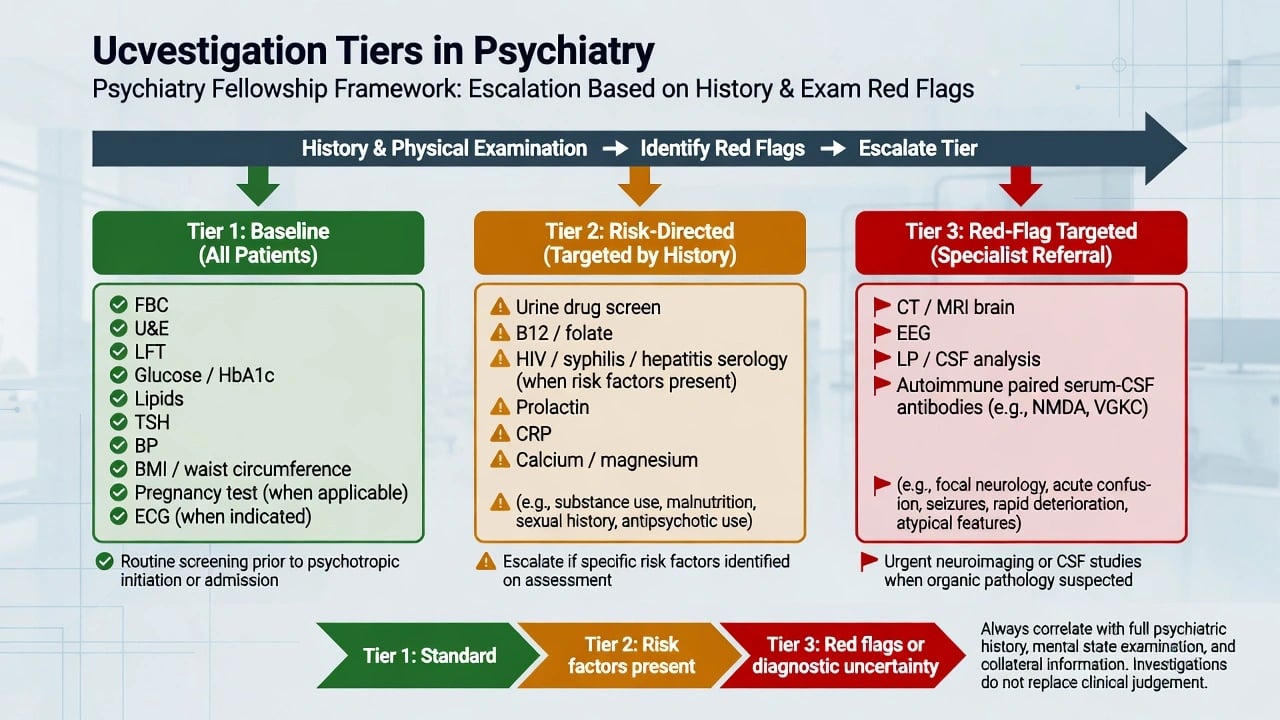
| Tier | Purpose | Typical content |
|---|---|---|
| 1 — Baseline | Screen common reversible contributors; safety before drugs | FBC, U&E (Na, K, eGFR), LFTs, glucose or HbA1c, lipids, TSH; BP, weight/BMI/waist; pregnancy test when applicable; ECG when indicated |
| 2 — Risk-directed | Targeted by history, exam, agent, or setting | Urine drug screen; B12/folate; Ca/Mg/PO4; CRP/ESR; HIV/syphilis/hepatitis when risk; prolactin if symptoms or high-risk agent |
| 3 — Red-flag | Exclude dangerous structural/inflammatory/epileptic disease | CT (urgent structural/trauma), MRI (non-urgent detail), EEG, LP/CSF, paired serum–CSF neuronal antibodies |
Epidemiology: why physical health is psychiatry
People with SMI have substantially worse cardiovascular and metabolic outcomes and reduced life expectancy; physical disease, not only suicide, drives excess deaths.[4][18] Antipsychotic treatment — especially higher metabolic-liability agents — amplifies risk; CATIE and related effectiveness work made metabolic burden clinically unavoidable in agent choice discussions.[19][2]
Despite ADA/APA, Marder, EPA, NICE, and RANZCP guidance, real-world metabolic monitoring remains concerningly incomplete (Mitchell systematic review/meta-analysis) — a quality-of-care fact examiners use to probe systems thinking.[5][3][20]
Pathophysiology examiners expect (concise)
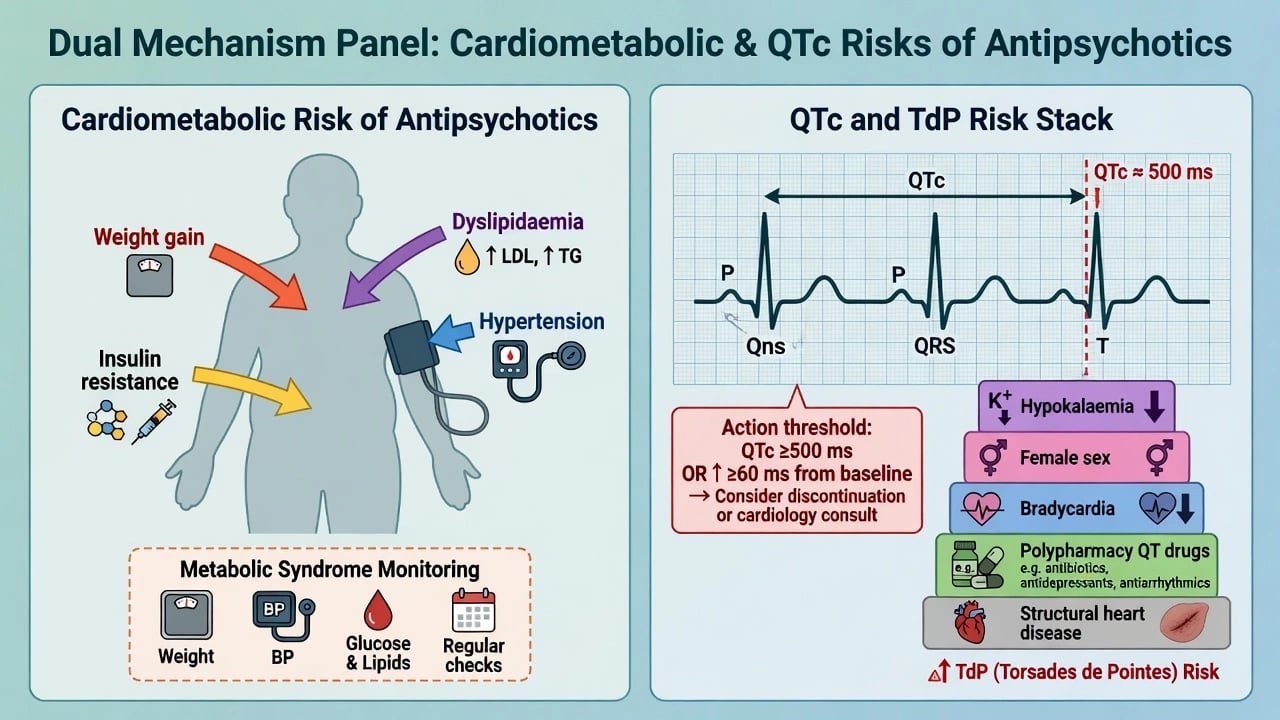
- Metabolic: antipsychotic-related weight gain, insulin resistance, and dyslipidaemia raise diabetes and cardiovascular risk; liability differs by agent (classically higher with clozapine/olanzapine than with aripiprazole/ziprasidone in consensus rankings).[2][19]
- QTc / TdP: many psychotropics block IKr (hERG); risk is multiplicative with hypokalaemia/hypomagnesaemia, bradycardia, female sex, structural heart disease, and QT polypharmacy.[6][8][11]
- Organic mental syndromes: systemic inflammation, hypoxia, metabolic derangement, autoimmune synaptic disruption (e.g. anti-NMDAR), and structural lesions alter arousal, attention, affect, and perception — producing secondary psychiatric phenotypes.[14][16]
Bedside physical and neurological examination
Process
Consent, dignity, chaperone where intimate examination needed, safety of the environment, and documentation of what was observed versus inferred. Combine with collateral and a systems review focused on neuro, infection, endocrine, cardiac, substance, and nutritional domains.[1][3]
Core elements the fellowship candidate can perform
Vitals: temperature, heart rate, respiratory rate, BP (postural if relevant), SpO2, capillary glucose when indicated. Abnormal vitals reframe "psychiatric agitation" as possible medical emergency.[16]
General: hydration, nutritional status, BMI/waist, stigmata of liver disease, thyroid, injection sites, self-harm scars, skin (rash, neuroleptic malignant syndrome [NMS] context), trauma.[3][18]
Cardiovascular / respiratory / abdomen: as required by history; auscultation before QT-risk drugs if cardiac symptoms; abdominal exam for constipation on clozapine/opioids.[8][3]
Neurological essentials (psychiatrist level): level of consciousness and attention (months backward, digit span); meningism screen when fever/headache; pupils (size, reactivity, asymmetry) and eye movements; cranial nerves screen; tone, power, deep tendon reflexes, plantars; coordination and gait; extrapyramidal signs (parkinsonism, akathisia, dystonia, tardive movements with AIMS-style observation); catatonic motor signs when suspected.[16][1]
Iatrogenic clusters to recognise on exam: anticholinergic toxicity; serotonin syndrome (hyperreflexia, clonus, hyperthermia); NMS (rigidity, fever, autonomic instability); lithium toxicity (coarse tremor, ataxia, confusion).[16][8]
Organic MSE clues that force investigation escalation
Fluctuating attention, altered arousal, predominant visual hallucinations, new seizures, speech reduction, dyskinesias, autonomic instability, fever, and demography/tempo mismatch for primary FEP.[15][16][17]
Differential: primary vs secondary
| Feature | Favours primary psychiatric | Favours organic/secondary |
|---|---|---|
| Onset | Days–weeks in typical age band | Hyperacute, fluctuating, or very late/very early atypical |
| Attention/arousal | Relatively preserved (outside severe mania/catatonia) | Inattention, fluctuation, clouding (delirium) |
| Hallucinations | Often auditory in primary psychosis | Visual more suggestive of organic/delirium (not absolute) |
| Exam | Soft signs only | Focal neurology, meningism, fever, autonomic crisis |
| Course | Follows expected syndrome | Progressive multi-stage (e.g. anti-NMDAR) or medical tempo |
Classic viva organic list (not exhaustive): delirium, substance intoxication/withdrawal, thyroid disease, B12 deficiency, HIV, neurosyphilis, SLE, autoimmune encephalitis, space-occupying lesion, stroke, epilepsy/NCSE, Wilson disease, porphyria, hepatic/renal encephalopathy, steroid and other iatrogenic causes.[1][12]
Baseline laboratory package (before psychotropics)
Near-universal baseline (adapt to urgency and capacity for fasting): FBC; U&E with sodium and potassium and eGFR; LFTs; fasting glucose or HbA1c; lipids; TSH; weight, BMI, waist circumference, and BP; pregnancy test in anyone who could become pregnant before teratogenic agents; ECG when indicated (see next section).[2][3][18][20]
Common add-ons: urine drug screen; alcohol markers; B12/folate; calcium, magnesium, phosphate (especially if QT risk or malnutrition); CRP; prolactin if galactorrhoea, amenorrhoea, sexual dysfunction, or high-risk agent; infection serologies by risk (HIV, syphilis, hepatitis B/C).[1][18]
Agent-specific programmes: lithium (eGFR, electrolytes, TSH, levels); valproate (LFTs, FBC, levels/pregnancy risk counselling); carbamazepine (FBC, LFTs, sodium, interactions); clozapine (baseline and serial ANC/FBC per protocol — cross-reference clozapine monograph).[18][20]
Metabolic monitoring schedule
ADA/APA consensus remains the structural backbone many guidelines echo: baseline, 4 weeks, 8 weeks, 12 weeks, then quarterly weight review early, with glucose, lipids, and BP at baseline, 12 weeks, and annually (intensify if high-risk agent or abnormality).[2][3] NICE-style annual comprehensive physical health checks and RANZCP physical health consensus emphasise shared care and sustained cardiometabolic attention across the illness course.[18][20]
Document who owns monitoring (psychiatry team vs GP) in the care plan; Mitchell's data show systems fail without intentional ownership.[5]
ECG and QTc
When to obtain ECG
Obtain ECG before or early on agents with meaningful QT liability or in high-risk patients (cardiac history, syncope, family sudden death, electrolyte disorder, overdose, polypharmacy QT drugs, methadone, elderly, female with stacked risks); at baseline for many inpatient starts and rapid-tranquillisation pathways when feasible; with new cardiac symptoms, after significant dose changes of QT-active drugs, or when electrolytes are deranged; and per local formulary for specific agents (e.g. high-dose IV antipsychotics, citalopram/escitalopram ceiling contexts).[8][9][10]
Measurement and action
Correct QT for rate carefully; Bazett overcorrects at high heart rates — know that alternative formulae exist and that lead quality and manual review matter for borderline values.[8][9]
Operational action thresholds used in psychotropic safety teaching (Beach/Funk framing aligned with hospital TdP prevention): QTc around 500 ms or an increase of about 60 ms from baseline — stop or switch culprits, replete potassium and magnesium, continuous monitoring as indicated, cardiology liaison, avoid stacking more QT-active drugs.[8][9][11]
Ray and colleagues linked atypical antipsychotics to increased sudden cardiac death risk in a large cohort — risk is not theoretical, and dose-response patterns matter in viva discussion.[7] Glassman and Bigger established the modern psychiatric narrative linking antipsychotics, QTc, TdP, and sudden death.[6] Reilly and colleagues showed QTc abnormalities associate with specific psychotropic exposures in psychiatric inpatients.[10]
Organic exclusion algorithm
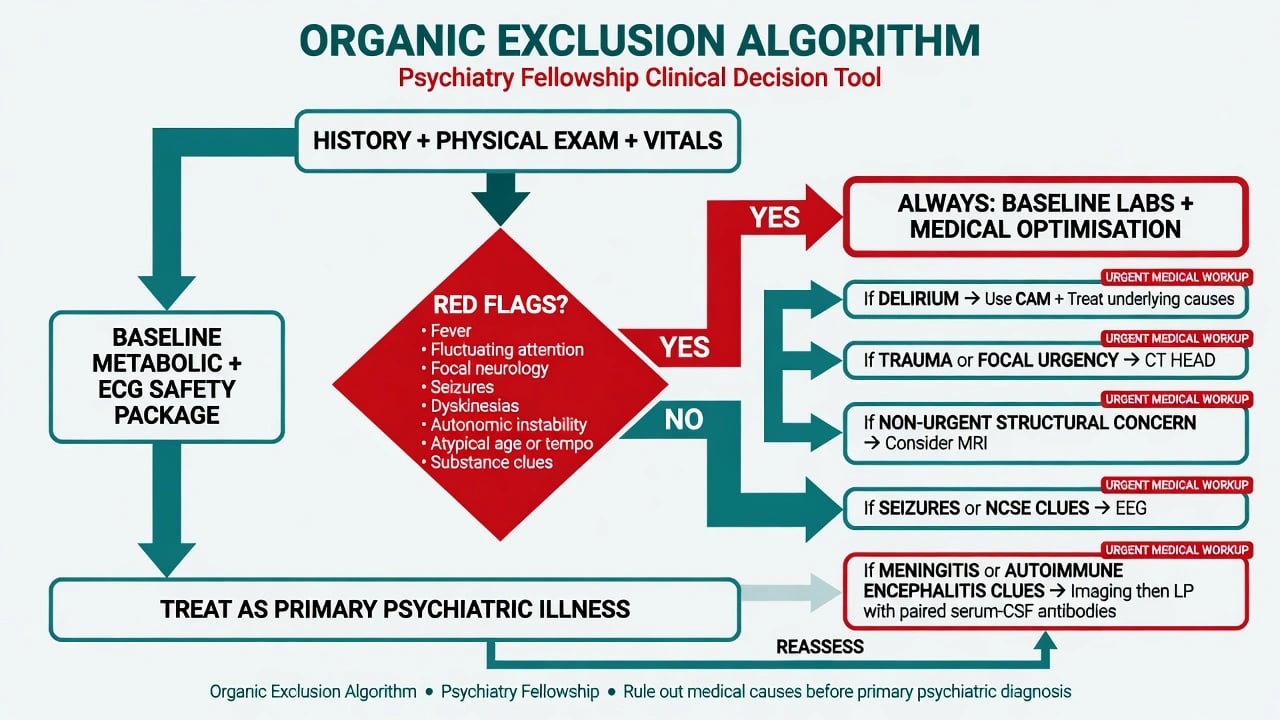
Always
History (tempo, substances, systemic symptoms, head injury, pregnancy), physical/neuro exam, vitals, and a baseline lab package appropriate to the setting. Optimise oxygen, glucose, hydration, and stop deliriogenic drugs when delirium is possible.[1][16]
Delirium pathway
Use CAM logic: acute onset and fluctuating course and inattention and (disorganised thinking or altered level of consciousness). Treat causes; do not use scheduled high-dose antipsychotics as "clearance".[17][16]
CT vs MRI
CT head is for urgency — trauma, sudden severe headache with red flags, focal neurology suggesting stroke/bleed, rapid deterioration when MRI is inaccessible. MRI brain is preferred for non-urgent structural detail (suspected tumour, inflammatory/AE support, white-matter disease, late-onset atypical psychosis with cognitive decline) when clinically indicated.[1][21]
Routine imaging for every calm, typical FEP with normal neurological examination is controversial. Yield of management-changing findings is often low; health-technology assessment (Albon) questions routine scanning economics; practices and guidelines vary regionally. Defend a selective high-yield strategy while never refusing imaging when red flags exist.[21][1]
EEG
Order when seizures, non-convulsive status epilepticus (NCSE) suspicion, unexplained fluctuating encephalopathy, or as supportive data in AE work-up — not as a fishing expedition for every FEP without clues.[12][1]
LP and autoimmune testing
LP when meningitis/encephalitis is plausible, or as part of AE work-up after imaging if raised intracranial pressure risk is addressed. Pair clinical syndrome with serum and CSF cell-based assays for neuronal surface antibodies when AE is suspected; normal MRI does not exclude anti-NMDAR encephalitis.[12][14][15]
Use Graus AE criteria and Pollak autoimmune-psychosis consensus as structured frameworks for possible/probable/definite disease — escalate immunotherapy discussion with neurology when probable criteria are met rather than waiting weeks for serology alone.[12][13] Herken and Prüss-style red flags (seizures, movement disorders, autonomic instability, speech change, catatonia, fever, memory loss, fluctuation) trigger the AE pathway.[15]
Avoid unselected antibody panels in every uncomplicated primary psychosis without red flags — false positives and false reassurance both harm.[13]
Acute / emergency medical interface
ABCDE first. Correct hypoglycaemia, hypoxia, sepsis, Wernicke risk (thiamine in alcohol-risk patients before glucose when indicated), hypertensive emergency, and arrhythmia. Psychiatric legal pathways do not replace emergency medical care. Rapid tranquillisation still requires attention to airway, oxygen, monitoring, and QT/electrolyte risk when injectable antipsychotics or combinations are used.[16][8]
Definitive physical-health management
- Choose lower metabolic-liability antipsychotics when efficacy allows in high-risk metabolic patients.[2][19]
- Run scheduled metabolic and physical health reviews; intervene early on weight, BP, lipids, and dysglycaemia.[2][18]
- Integrate lifestyle, smoking cessation, and primary care collaboration (RANZCP physical health consensus; Castle Australian Prescriber synthesis).[20][18]
- Treat confirmed organic disease (AE immunotherapy, infection, endocrine replacement) as the primary disease-modifying plan; psychotropics are supportive bridges only when needed for safety or symptom control.[12][13]
Subtypes and scenarios
| Scenario | Emphasis |
|---|---|
| FEP | Freudenreich triad: broad screen + selective exclusion + baseline |
| Late-onset psychosis | Higher organic prior; lower imaging/EEG threshold |
| Delirium | CAM + cause map; limited antipsychotics |
| Rapid tranquillisation | Vitals, ECG/electrolytes when feasible, monitoring |
| Clozapine / lithium | Protocolised lab programmes |
| Perinatal | Pregnancy test, ECG, metabolic care; avoid unnecessary radiation |
| Child/adolescent | Growth charts, prolactin, metabolic early |
| ID / ASD | Adapted exam; lower threshold for organic causes |
| Eating disorders | Medical risk panel (cross-ref specialty topics) |
Special populations
Older adults: delirium risk, polypharmacy, QTc, falls — new psychosis is organic until considered carefully.[16]
Youth: early metabolic injury has decades of consequence; monitor weight aggressively after SGAs.[2]
Pregnancy/lactation: investigate and prescribe with obstetric partnership; pregnancy testing is non-negotiable before teratogens.[18]
Indigenous and culturally diverse communities: higher cardiometabolic burden in many groups and access barriers — culturally safe examination and assertive physical-health outreach are clinical duties, not optional extras.[20]
Intellectual disability: communication adaptations for consent to exam; medical causes of behaviour change are common.[1][20]
Complications and pitfalls
Key pitfalls include skipping exam because "it is psych"; equating normal MRI with non-organic disease; serum-only autoimmune testing without a clinical syndrome; never repeating metabolic labs after a single baseline; stacking QT drugs with hypokalaemia; failing pregnancy testing; using CT as default without indication or refusing CT when focal signs are present; and pejorative notes that block medical teams from taking physical complaints seriously.[1][5][8][12][14]
Prognosis and disposition
Physical-health monitoring intensity should match agent risk and patient vulnerability. Disposition decisions (medical ward vs psychiatric unit) follow medical stability and nursing needs, not convenience. Reassess organicity if the course turns atypical after a "primary" label.[4][18][1]
Evidence and regional deltas
| Source | Practical take-home |
|---|---|
| ADA/APA 2004 | Structured metabolic monitoring skeleton still taught globally |
| Marder 2004 AJP | Outpatient physical health monitoring consensus for schizophrenia |
| De Hert EPA 2009 | CVD/diabetes as core SMI care with endocrinology/cardiology partnership |
| Mitchell 2012 | Monitoring adherence is a systems failure, not a trivia fact |
| Freudenreich 2009 | Conceptual FEP medical work-up |
| Beach 2013 / Funk 2020 | QTc risk stratification and psychotropic tables for clinicians |
| Graus 2016 / Pollak 2020 | AE and autoimmune psychosis frameworks |
| RANZCP Lambert 2017 / Castle 2023 | ANZ physical health consensus and practical monitoring |
| Albon HTA 2008 | Limits of routine structural neuroimaging economics |
ANZ (RANZCP): strong emphasis on physical health consensus for enduring psychosis, shared care, and metabolic monitoring; Castle summarises practical Australian monitoring priorities.[20][18]
UK (NICE / Lester-type tools): annual physical health checks for psychosis/SMI registers; selective imaging culture more common than automatic FEP MRI.
US (APA-influenced practice): more variable use of routine FEP neuroimaging in some centres; still defend low yield when neuro exam is normal and red flags absent while never missing indicated scans.[21]
Always follow local formulary, infection-control, and mental health act procedures; do not invent statute section numbers.
Exam pearls
Physical examination and investigations are fellowship-core clinical methods. A candidate who can perform a focused neuro exam, write a tiered investigation plan, act on QTc and metabolic data, and defend when not to scan has mastered this topic across FRANZCP, MRCPsych, ABPN, and MD/DNB formats.[1][2][8]
References
- [1]Freudenreich O, Schulz SC, Goff DC Initial medical work-up of first-episode psychosis: a conceptual review Early Interv Psychiatry, 2009.PMID 21352170
- [2]American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity Consensus development conference on antipsychotic drugs and obesity and diabetes Diabetes Care, 2004.PMID 14747245
- [3]Marder SR, Essock SM, Miller AL, et al. Physical health monitoring of patients with schizophrenia Am J Psychiatry, 2004.PMID 15285957
- [4]De Hert M, Dekker JM, Wood D, et al. Cardiovascular disease and diabetes in people with severe mental illness position statement from the European Psychiatric Association (EPA), supported by the European Association for the Study of Diabetes (EASD) and the European Society of Cardiology (ESC) Eur Psychiatry, 2009.PMID 19682863
- [5]Mitchell AJ, Delaffon V, Vancampfort D, et al. Guideline concordant monitoring of metabolic risk in people treated with antipsychotic medication: systematic review and meta-analysis of screening practices Psychol Med, 2012.PMID 21846426
- [6]Glassman AH, Bigger JT Jr Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death Am J Psychiatry, 2001.PMID 11691681
- [7]Ray WA, Chung CP, Murray KT, et al. Atypical antipsychotic drugs and the risk of sudden cardiac death N Engl J Med, 2009.PMID 19144938
- [8]Beach SR, Celano CM, Noseworthy PA, et al. QTc prolongation, torsades de pointes, and psychotropic medications Psychosomatics, 2013.PMID 23295003
- [9]Funk MC, Beach SR, Bostwick JR, et al. QTc Prolongation and Psychotropic Medications Am J Psychiatry, 2020.PMID 32114782
- [10]Reilly JG, Ayis SA, Ferrier IN, et al. QTc-interval abnormalities and psychotropic drug therapy in psychiatric patients Lancet, 2000.PMID 10744090
- [11]Drew BJ, Ackerman MJ, Funk M, et al. Prevention of torsade de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation Circulation, 2010.PMID 20142454
- [12]Graus F, Titulaer MJ, Balu R, et al. A clinical approach to diagnosis of autoimmune encephalitis Lancet Neurol, 2016.PMID 26906964
- [13]Pollak TA, Lennox BR, Müller S, et al. Autoimmune psychosis: an international consensus on an approach to the diagnosis and management of psychosis of suspected autoimmune origin Lancet Psychiatry, 2020.PMID 31669058
- [14]Dalmau J, Gleichman AJ, Hughes EG, et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies Lancet Neurol, 2008.PMID 18851928
- [15]Herken J, Prüss H Red Flags: Clinical Signs for Identifying Autoimmune Encephalitis in Psychiatric Patients Front Psychiatry, 2017.PMID 28261116
- [16]Marcantonio ER Delirium in Hospitalized Older Adults N Engl J Med, 2017.PMID 29020579
- [17]Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium Ann Intern Med, 1990.PMID 2240918
- [18]Castle D, Li A Physical health monitoring for people with schizophrenia Aust Prescr, 2023.PMID 38152317
- [19]Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia N Engl J Med, 2005.PMID 16172203
- [20]Lambert TJ, Reavley NJ, Jorm AF, et al. Royal Australian and New Zealand College of Psychiatrists expert consensus statement for the treatment, management and monitoring of the physical health of people with an enduring psychotic illness Aust N Z J Psychiatry, 2017.PMID 28343435
- [21]Albon E, Tsourapas A, Frew E, et al. Structural neuroimaging in psychosis: a systematic review and economic evaluation Health Technol Assess, 2008.PMID 18462577