Psych · Foundations — prevention and early intervention
Prevention and early intervention in mental health
Also known as Preventive psychiatry · Early intervention mental health · Universal selective indicated prevention · Clinical staging psychiatry · Duration of untreated psychosis · Youth mental health prevention · Indicated prevention depression psychosis
Exam-exhaustive fellowship reference on prevention and early intervention in mental health: Gordon and Caplan frameworks, Rose population strategy, life-course and ACE-informed selective programmes, school-based and perinatal prevention, indicated prevention of depression and clinical high-risk for psychosis, DUP reduction, multi-element early intervention services (OPUS/RAISE), clinical staging, ethics and implementation. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
6 MCQs with explanations
Target exams
Red flags
1. Definitions and examiner map
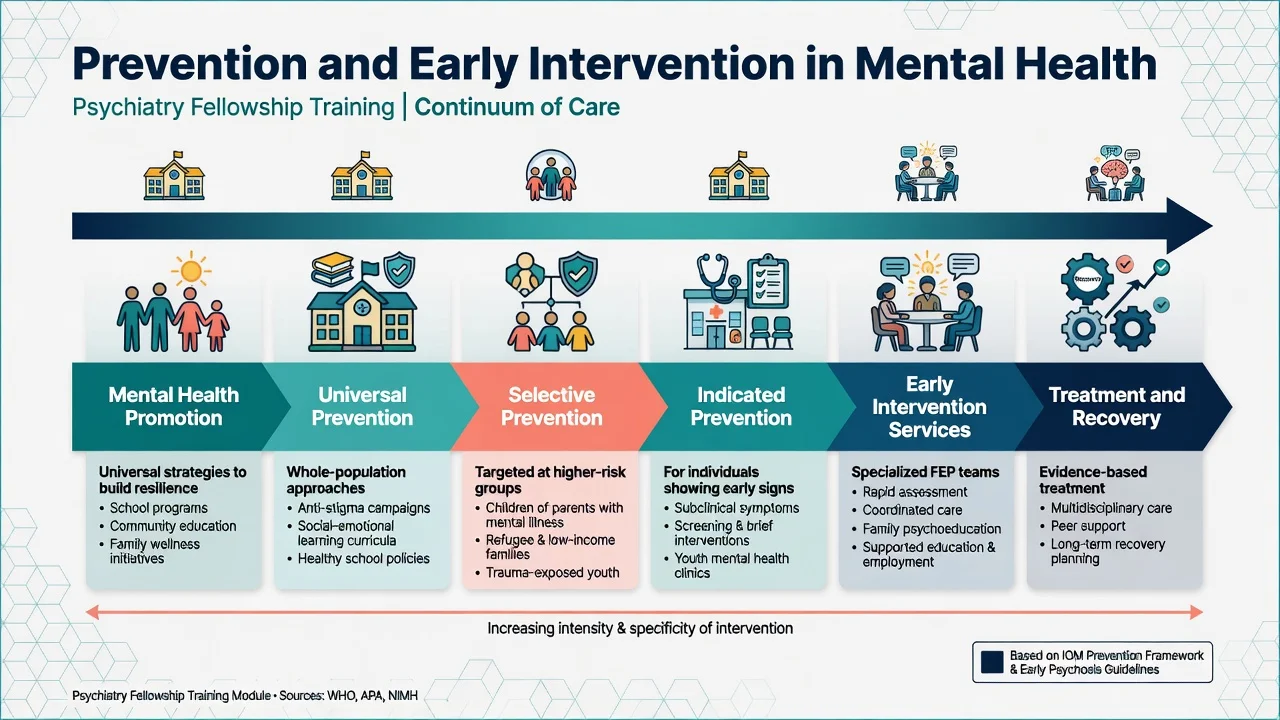
Mental health promotion strengthens protective factors and wellbeing (connectedness, skills, equity) without requiring a disorder diagnosis. Prevention aims to reduce incidence, delay onset, or reduce severity/disability of disorders. Early intervention detects emerging illness early and delivers evidence-based care promptly — including multi-element first-episode services. Treatment and recovery supports continue once disorder is established.[3][16]
| Construct | Core aim | Exam trap |
|---|---|---|
| Promotion | Build protective factors / wellbeing | Not the same as treating depression |
| Universal prevention | Whole population, no risk screen | Not "only healthy people" rhetoric — everyone is included |
| Selective prevention | Elevated-risk groups | Not yet full disorder required |
| Indicated prevention | Subthreshold symptoms / high-risk mental states | Not equal to diagnosing schizophrenia |
| Early intervention (FEP) | Shorten DUP; multi-element care after onset | Not only "start any antipsychotic fast" |
| Secondary prevention (Caplan) | Early case-finding and treatment | Often confused with Gordon indicated |
| Tertiary prevention (Caplan) | Limit disability, prevent relapse | Overlaps maintenance treatment |
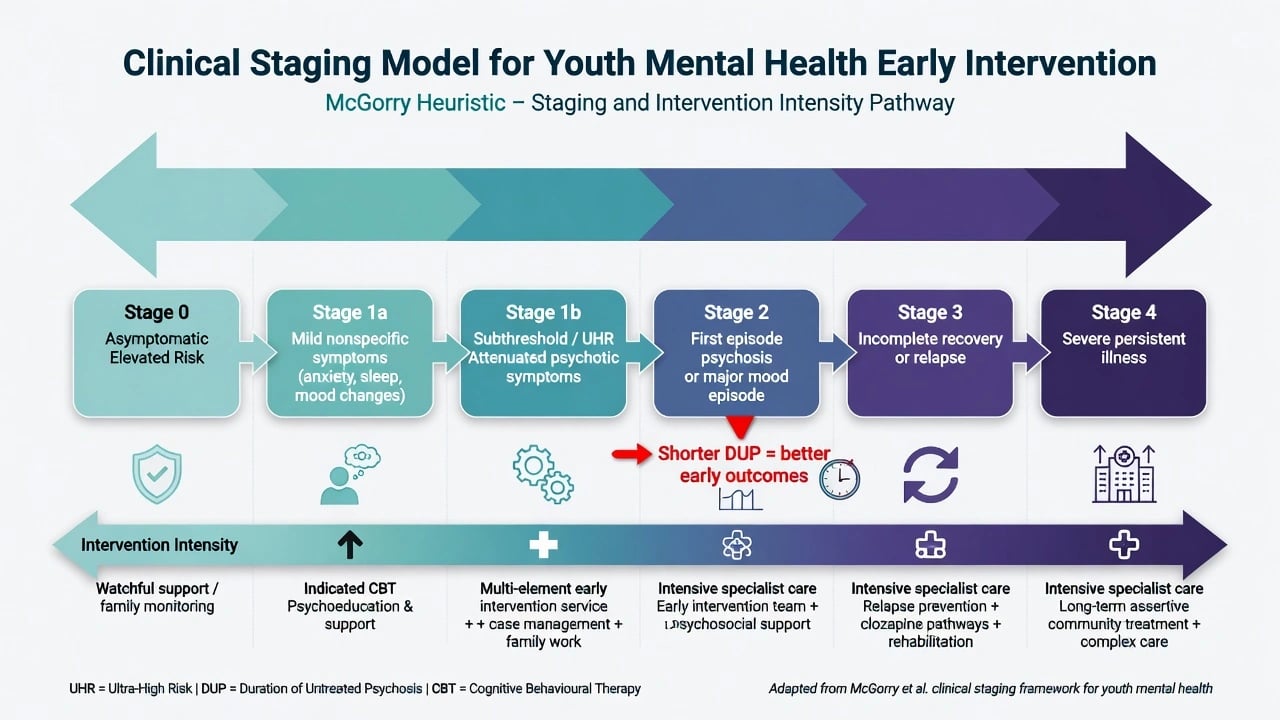
Duration of untreated psychosis (DUP) is the interval from onset of frank psychotic symptoms to adequate treatment initiation; longer DUP associates with poorer short-term outcomes in observational syntheses — a core rationale for detection campaigns and easy-entry youth pathways.[9]
2. Classification frameworks (must master both)
2.1 Gordon: universal / selective / indicated
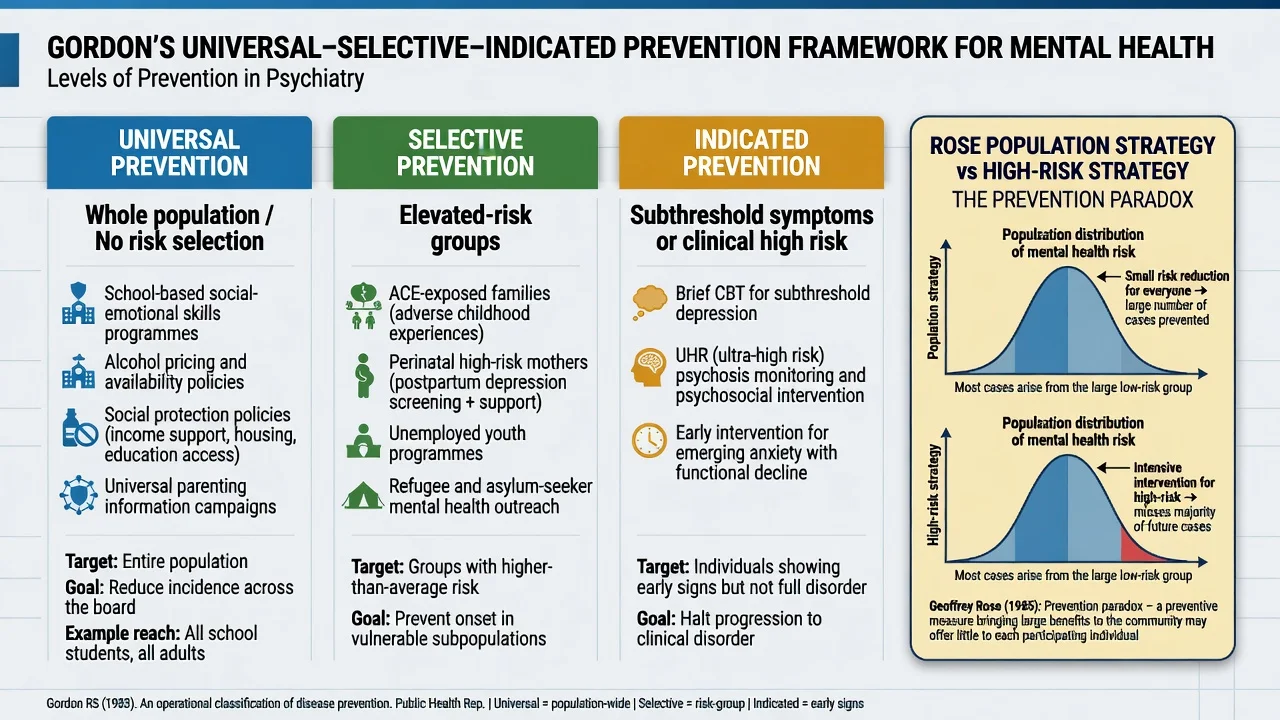
Gordon's operational classification is the default FRANZCP/MRCPsych answer structure.[1]
- Universal: whole population (school social-emotional learning, alcohol pricing/availability policy, anti-bullying, population suicide means restriction advocacy).
- Selective: groups with elevated risk but not yet the target disorder (ACE-exposed families, high-risk perinatal mothers, unemployed youth, refugee cohorts).
- Indicated: individuals with early/subthreshold signs (subthreshold depression; clinical high risk / ultra-high risk for psychosis).
2.2 Caplan: primary / secondary / tertiary
Primary prevents occurrence; secondary finds and treats early; tertiary reduces disability and relapse. Caplan maps poorly if forced onto Gordon without translation — examiners love catching the mix-up.[3]
2.3 Rose: sick individuals and sick populations
When risk is continuous, shifting the population mean (population strategy) can prevent more cases than only treating the high-risk tail. The prevention paradox: many cases arise from average-risk people, so clinic-only plans are necessary but insufficient.[2]
3. Epidemiology and why prevention windows exist
Age-of-onset distributions show many anxiety disorders and substantial lifetime burden begin in childhood or adolescence, with mood disorders often starting by early adulthood — so youth platforms are not optional extras for prevention policy.[15] Arango and colleagues synthesise developmental preventive strategies across risk-factor reduction, high-risk detection, and stage-specific intervention.[3]
CHR/UHR cohorts convert to frank psychosis in a minority over 2–3 years in meta-analyses (historically often cited in the low-to-mid tens of percent range, with heterogeneity and secular decline in some services) — base rates drive NNT and false-positive risk for aggressive biomedical intervention.[12]
4. Mechanisms and life-course logic
Population risk reflects cumulative adversity, sensitive developmental periods, and social determinants, not only "brain disease waiting to declare."[3][16] Selective early-life programmes (e.g. nurse home visitation) target parenting, maternal life course, and child maltreatment pathways that cascade into later mental health risk.[8]
Psychosis prevention science sits on a continuum from attenuated phenomena to frank illness; indicated interventions aim to reduce transition and treat current comorbidity without equating risk state with schizophrenia diagnosis.[12][13] Stigma and structural barriers prolong untreated illness — anti-stigma and access redesign are prevention-relevant, not soft add-ons.
5. Clinical presentation of prevention problems (exam stems)
- Policy: "Build more tertiary beds only" ignoring universal/selective layers.[2][16]
- School: request for a one-off talk expected to abolish youth depression — overpromise trap.[7]
- UHR youth: attenuated psychotic symptoms, functional drop, high anxiety/depression comorbidity — indicated pathway, not automatic long-acting antipsychotic.[12][14]
- FEP with long DUP: delayed help-seeking, cannabis use, family minimisation — detection + multi-element EIS.[9][10]
- Perinatal high-risk: prior severe mental illness or current psychosocial adversity — selective pathway with mother–infant focus.[3]
6. Assessment for prevention intensity
- Population need metrics: 12-month prevalence, severity, treatment coverage, wait times, DUP audits — not admissions alone.[16]
- Individual risk stack: ACE/maltreatment history, family history, substance use (especially high-potency cannabis for psychosis risk discussions), perinatal factors, subthreshold symptom load, functioning (education/work).[3][15]
- Stage assignment: asymptomatic elevated risk → nonspecific distress → subthreshold/UHR → first episode → incomplete recovery/relapse → persistent severe illness.[4]
- Imminent risk screen: suicide, violence, severe neglect, frank psychosis — exit prevention track into acute care immediately.[16]
- Appraisal literacy: cluster RCTs, contamination in schools, short follow-up, and absolute vs relative risk reductions.[5][7]
7. "Investigations" in prevention science
There is no blood test for prevention readiness. Evaluate reach, equity, fidelity, outcomes that matter (incidence where measurable, symptom change, function, education, employment, conversion rates, relapse, coercive care rates), and unintended harms (stigma from labels, metabolic burden of premature antipsychotics).[10][14][16]
8. Acute system response (not ACLS)
During disasters or pandemics, population mental health demand surges. Maintain stepped capacity, protect high-risk groups, and avoid dismantling community early-intervention pathways to fund beds alone.[16] Any prevention contact that uncovers imminent self-harm, frank psychosis, or severe maltreatment must escalate — rights-based care is not neglect of harm.
9. Definitive management by prevention level
9.1 Universal
School-based psychological prevention programmes show small average benefits for depression and anxiety symptoms versus controls; skills-based designs outperform information-only approaches in broader prevention literature, and fidelity/implementation determine real-world impact.[7] Structural measures (alcohol policy, poverty reduction, anti-bullying, social protection) operate on Rose logic.[2][3]
9.2 Selective
Nurse home visitation for high-risk first-time parents shows long-term benefits on maternal life course and child abuse/neglect outcomes in landmark trials — selective prevention with developmental return on investment.[8] Perinatal mental health pathways, targeted family support after ACE exposure, and culturally safe programmes for minoritised populations sit here.[3]
9.3 Indicated — depression
Psychological interventions aimed at people with subthreshold or high-risk depression reduce incidence of major depressive disorder in meta-analyses; Cuijpers and colleagues reported a mean incidence rate ratio of about 0.78 (roughly 22% relative reduction) — meaningful at population scale, not a guarantee for any single person.[5][6] Programme content is typically CBT- or IPT-informed, brief, and delivered in primary care, schools, or digital stepped formats.
9.4 Indicated — psychosis risk (CHR/UHR)
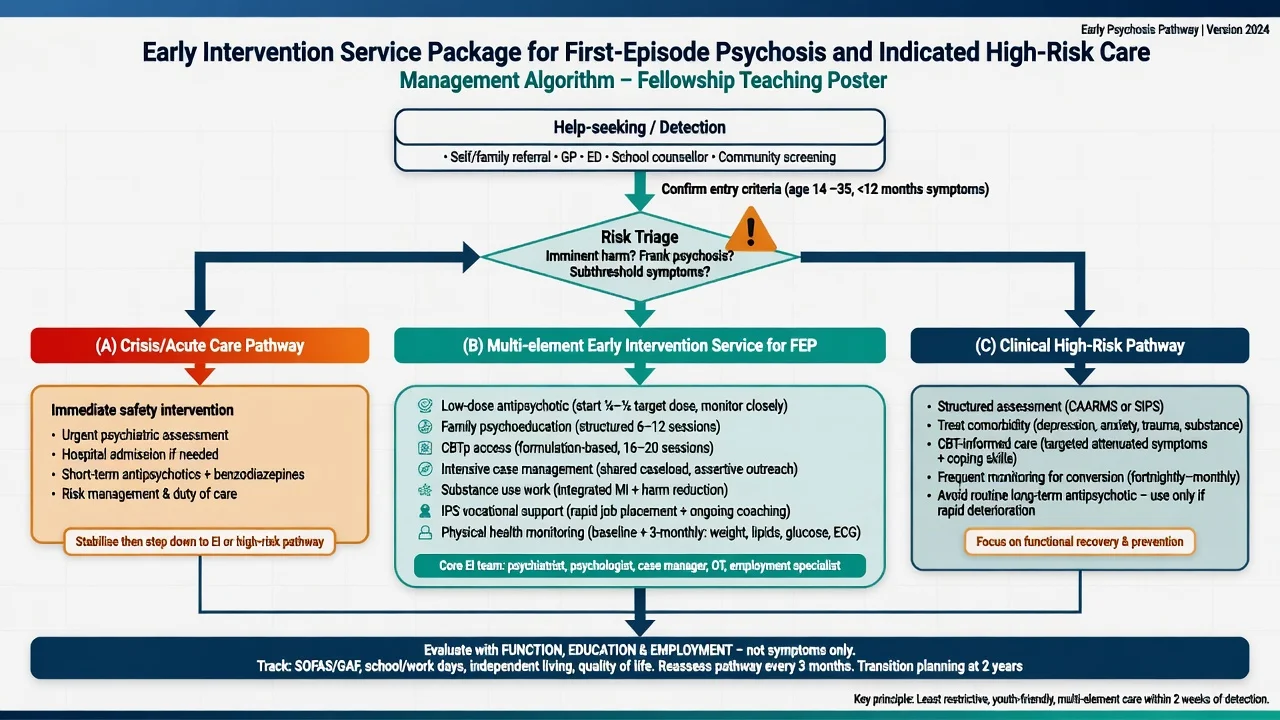
Prioritise structured assessment, treatment of anxiety/depression, sleep, substance reduction, family support, and CBT-informed care with monitoring for conversion.[12][13] Meta-analysis of preventive trials suggested reduced transition risk with indicated interventions overall, but network meta-analysis has not robustly crowned a single superior specific biomedical preventive package — humility required.[13][14] Antipsychotics are not first-line default for non-converting risk states given metabolic harm and false-positive burden; reserve for specialist rationale, severe distress with near-threshold psychosis, or frank conversion (detail in CHR and FEP topics).
9.5 Early intervention services (after onset)
Multi-element early intervention services for early-phase psychosis (assertive case management, low-dose antipsychotic strategy with monitoring, family work, psychological therapy access, substance intervention, vocational support such as IPS principles) outperform treatment-as-usual across multiple outcomes in meta-analysis; RAISE demonstrates comprehensive community care gains versus usual care in US systems; OPUS is the classic Scandinavian RCT lineage examiners name.[10][11] Pair with DUP reduction (public education, GP liaison, low-threshold entry).[9]
When antipsychotics are indicated for FEP, use low effective doses, oral initiation in most first-episode contexts, baseline and serial metabolic parameters (weight/BMI, glucose/HbA1c, lipids), blood pressure, and ECG when risk factors or drug choice warrant — exact agent selection lives in FEP/antipsychotic monographs; the prevention/EI pearl is timely multi-element care, not polypharmacy.[10][11]
9.6 Clinical staging
McGorry's staging heuristic assigns earlier, safer, more benign interventions to earlier stages and intensifies with progression or non-response — a bridge between prevention science and clinical service design.[4]
10. Scenarios and subtypes
| Scenario | Dominant level | Core package |
|---|---|---|
| Whole-school SEL / CBT skills | Universal | Curriculum + teacher fidelity; evaluate small effects honestly |
| High-risk first-time mothers | Selective | Nurse home visitation / intensive parenting support |
| Subthreshold depression in primary care | Indicated | Brief psychological prevention; stepped care |
| UHR attenuated symptoms | Indicated | CBT-informed + comorbidity + monitor; AP not default |
| First-episode psychosis | Early intervention | Multi-element EIS + shorten DUP |
| Youth substance use | Universal + selective + indicated | Policy + skills programmes + brief intervention |
| Post-disaster surge | Mixed | Population supports + protect high-risk + surge treatment |
11. Complications and pitfalls
- High-risk only design ignores Rose and under-delivers population impact.[2]
- Overmedicalising UHR with routine long-term antipsychotics harms non-converters.[14]
- Overclaiming school programmes as cures rather than small-effect contributors.[7]
- Confusing Caplan secondary prevention (early treatment) with Gordon indicated prevention.
- Equity failure: programmes captured by the least disadvantaged.
- Implementation collapse: manuals without workforce, fidelity, or funding.[16]
- Using recovery rhetoric to deny evidence-based medication after established FEP.
12. Prognosis and disposition
Most CHR individuals do not convert within typical follow-up windows; they still deserve care for current psychopathology and function.[12] EIS advantages may attenuate after the specialised phase ends — plan step-down, open re-entry, and continuity with community teams.[10] Population prevention horizons are long; demand appropriate evaluation windows. Late presenters with long DUP still warrant full EIS intensity — do not therapeutic nihilism.[9]
13. Special populations
- Children/adolescents: school and family platforms; developmental assessment before pathologising behaviour.[7][15]
- Transition-age youth: soft-entry youth mental health services; psychosis EIS age criteria vary by jurisdiction.
- Perinatal: selective high yield for mother and infant outcomes.[3]
- Older adults: late-life depression prevention and social isolation; "EIS" branding less central than collaborative care and physical comorbidity.
- Indigenous and culturally diverse communities: self-determination, cultural safety, and structural determinants — do not import one-size programmes.[16]
- Intellectual disability: dual diagnosis under-detected; adapt communication and pathways.
- LMIC settings: task-sharing and primary care packages expand reach of both prevention-adjacent and treatment functions.[16]
14. Evidence, guidelines, and regional deltas
Named evidence examiners expect: Gordon;[1] Rose;[2] Arango preventive strategies;[3] McGorry staging;[4] Cuijpers/van Zoonen depression incidence prevention;[5][6] Werner-Seidler school programmes;[7] Olds home visitation;[8] Marshall DUP;[9] Correll EIS meta-analysis;[10] RAISE;[11] Fusar-Poli transition;[12] van der Gaag psychosis prevention trials;[13] Davies network meta-analysis caution;[14] Kessler age-of-onset;[15] Campion implementation.[16]
15. Exam pearls (rapid-fire)
- Always name Gordon three with one example each.[1]
- Always name Rose + prevention paradox when service design is the stem.[2]
- Caplan ≠ Gordon — translate if forced to use both.[3]
- Depression indicated prevention: IRR ~0.78 classic framing — relative, not absolute cure rates.[5]
- School effects are small on average — do not oversell.[7]
- CHR: minority convert; treat comorbidity; AP not default.[12][14]
- FEP: shorten DUP + multi-element EIS (OPUS/RAISE/Correll).[9][10][11]
- Staging justifies earlier safer care.[4]
- Implementation is the bottleneck.[16]
PREVENT-EI (prevention and early intervention stack)
References
- [1]Gordon RS Jr An operational classification of disease prevention Public Health Rep, 1983.PMID 6856733
- [2]Rose G Sick individuals and sick populations Int J Epidemiol, 2001.PMID 11416056
- [3]Arango C, Díaz-Caneja CM, McGorry PD, et al. Preventive strategies for mental health Lancet Psychiatry, 2018.PMID 29773478
- [4]McGorry PD, Hickie IB, Yung AR, et al. Clinical staging of psychiatric disorders: a heuristic framework for choosing earlier, safer and more effective interventions Aust N Z J Psychiatry, 2006.PMID 16866756
- [5]Cuijpers P, van Straten A, Smit F, et al. Preventing the onset of depressive disorders: a meta-analytic review of psychological interventions Am J Psychiatry, 2008.PMID 18765483
- [6]van Zoonen K, Buntrock C, Ebert DD, et al. Preventing the onset of major depressive disorder: a meta-analytic review of psychological interventions Int J Epidemiol, 2014.PMID 24760873
- [7]Werner-Seidler A, Perry Y, Calear AL, et al. School-based depression and anxiety prevention programs for young people: A systematic review and meta-analysis Clin Psychol Rev, 2017.PMID 27821267
- [8]Olds DL, Eckenrode J, Henderson CR Jr, et al. Long-term effects of home visitation on maternal life course and child abuse and neglect. Fifteen-year follow-up of a randomized trial JAMA, 1997.PMID 9272895
- [9]Marshall M, Lewis S, Lockwood A, et al. Association between duration of untreated psychosis and outcome in cohorts of first-episode patients: a systematic review Arch Gen Psychiatry, 2005.PMID 16143729
- [10]Correll CU, Galling B, Pawar A, et al. Comparison of Early Intervention Services vs Treatment as Usual for Early-Phase Psychosis: A Systematic Review, Meta-analysis, and Meta-regression JAMA Psychiatry, 2018.PMID 29800949
- [11]Kane JM, Robinson DG, Schooler NR, et al. Comprehensive Versus Usual Community Care for First-Episode Psychosis: 2-Year Outcomes From the NIMH RAISE Early Treatment Program Am J Psychiatry, 2016.PMID 26481174
- [12]Fusar-Poli P, Bonoldi I, Yung AR, et al. Predicting psychosis: meta-analysis of transition outcomes in individuals at high clinical risk Arch Gen Psychiatry, 2012.PMID 22393215
- [13]van der Gaag M, Smit F, Bechdolf A, et al. Preventing a first episode of psychosis: meta-analysis of randomized controlled prevention trials of 12 month and longer-term follow-ups Schizophr Res, 2013.PMID 23870806
- [14]Davies C, Cipriani A, Ioannidis JPA, et al. Lack of evidence to favor specific preventive interventions in psychosis: a network meta-analysis World Psychiatry, 2018.PMID 29856551
- [15]Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication Arch Gen Psychiatry, 2005.PMID 15939837
- [16]Campion J, Javed A, Lund C, et al. Public mental health: required actions to address implementation failure in the context of COVID-19 Lancet Psychiatry, 2022.PMID 35065723