Psych · Foundations — psychological and neuropsychological testing
Psychological and neuropsychological testing
Also known as Neuropsychological assessment psychiatry · Cognitive testing psychiatry · Psychometrics for psychiatrists · MATRICS MCCB · MoCA MMSE FAB · Performance validity testing
Exam-exhaustive fellowship reference on psychological and neuropsychological testing for psychiatrists — bedside screens (MMSE, MoCA, FAB, CAM), DSM-5 cognitive domains, formal NP referral, intelligence and personality testing principles, schizophrenia batteries (MATRICS MCCB, BACS, RBANS, HVLT-R), effort/validity (Slick/Sherman, TOMM), Green cognition–function evidence, practice effects and cultural pitfalls. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview and definitions
A psychological test is a standardised, norm-referenced (or criterion-referenced) procedure that samples behaviour to estimate latent constructs (cognition, intellect, personality, effort). A neuropsychological assessment is a hypothesis-driven evaluation of brain–behaviour relationships, usually integrating history, observation, performance-based tests, validity indices, and functional implications. Neither replaces diagnosis, capacity determination, or risk assessment. [7][8][16]
| Tool class | What it does | What it does not do |
|---|---|---|
| Psychiatric rating scale (PHQ-9, PANSS) | Quantifies symptom constructs | Characterise domain-level cognition |
| Bedside cognitive screen | Rapid case-finding / severity snapshot | Full profile or dementia diagnosis alone |
| Formal NP battery | Domain profile vs premorbid estimate | Stand-alone capacity or forensic verdict |
| Personality inventory | Trait/symptom patterns + validity scales | Sole personality disorder diagnosis |
| Effort / performance validity | Supports score interpretability | Proves criminal intent by itself |

Classification framework
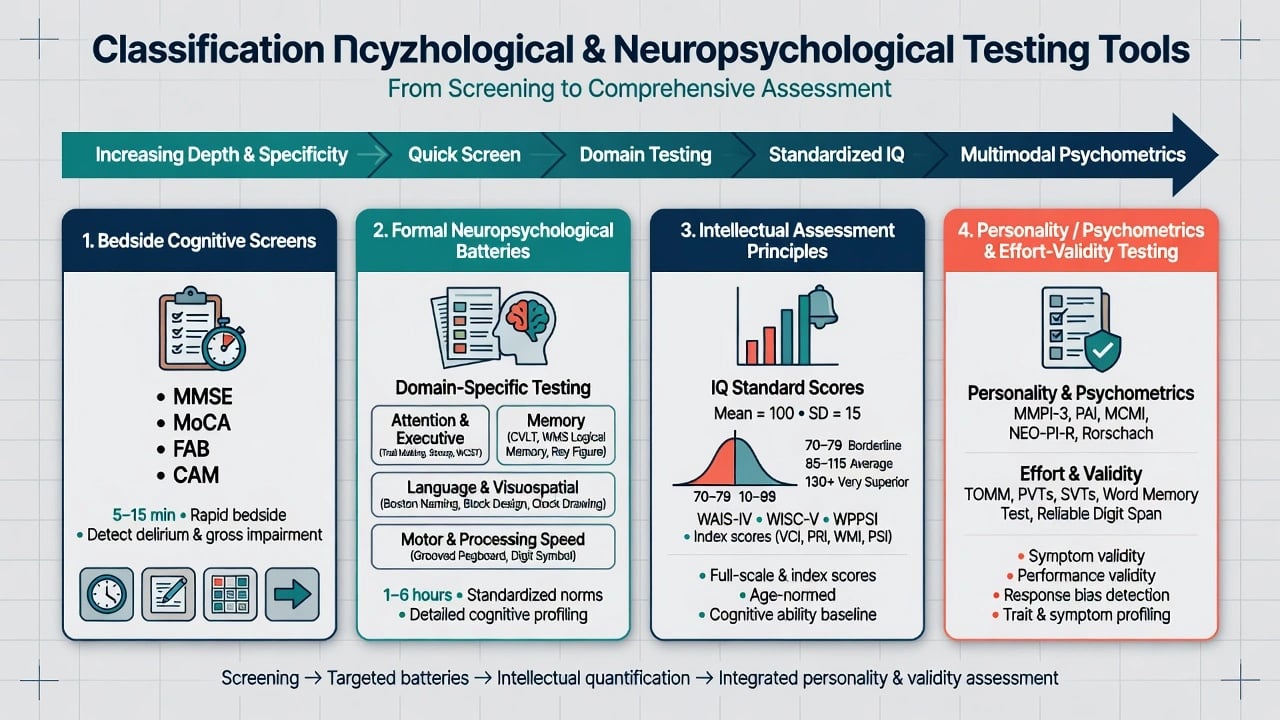
By clinical purpose
- Screening / triage — MMSE, MoCA, FAB, CAM when cognitive concern arises. [1][2][4][5]
- Syndrome characterisation — formal NP for mild vs major NCD patterns, TBI, post-stroke, progressive aphasia, executive-predominant decline. [7][14]
- Illness-specific cognition endpoints — MATRICS MCCB, BACS in schizophrenia research and specialised clinics. [8][13]
- Intellectual assessment — WAIS-class instruments for premorbid ability estimates, learning disability interface, and discrepancy analysis (principles: mean 100, SD 15).
- Personality and psychopathology measurement — objective inventories with validity scales; projective methods are adjunctive and not sole diagnostic evidence.
- Effort / symptom validity — performance validity tests (PVTs) and criteria frameworks when scores may be invalid. [16][17][18]
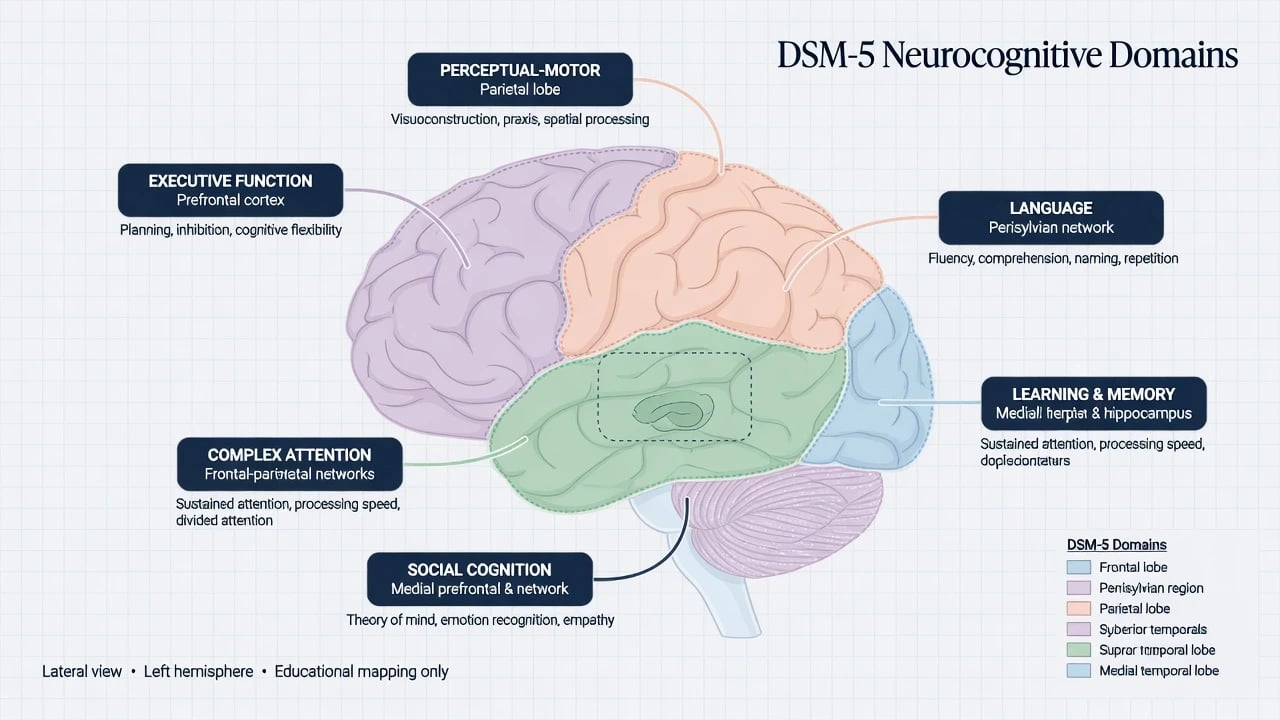
DSM-5 neurocognitive domains
DSM-5 reorganised cognitive disorders around six domains: complex attention, executive function, learning and memory, language, perceptual-motor, and social cognition — then mild vs major neurocognitive disorder by functional independence. [7]
Psychometrics examiners expect
- Reliability — consistency (internal, test–retest, inter-rater for observational tools). [8][13]
- Validity — content, construct, criterion; concurrent and predictive relationships with real-world function matter clinically (Green). [11][12]
- Standard scores — raw scores converted using age (and often education) norms to z, T, scaled scores, or percentiles with confidence intervals.
- Practice effects — retest improvement can mimic recovery; use alternate forms and appropriate retest intervals when available. [8][14]
- Floor / ceiling and base rates — extreme raw scores and low base-rate impairments require Bayesian humility.
- Premorbid estimate — demographic formulae, hold tests, or historical academic/occupational data to interpret decline vs lifelong low ability.
Bedside cognitive instruments (exam depth)
MMSE (Mini-Mental State Examination)
Classic brief bedside cognitive grading tool (orientation, registration, attention/calculation, recall, language, construction). Practical for serial grading in moderate–severe impairment; limited sensitivity for mild cognitive impairment relative to MoCA in many samples. Score range 0–30. Education and language heavily influence performance. Never diagnose dementia from MMSE alone. [1][2]
MoCA (Montreal Cognitive Assessment)
Developed as a brief screen more sensitive to mild cognitive impairment than MMSE in the original validation programme. Commonly taught cut-off around 26/30, but Carson and colleagues re-examined cut-offs and caution that lower thresholds may be more appropriate in some populations — do not treat 26 as universal law. Adjust interpretation for education, language, culture, sensory limits, and practice effects. Still a screen, not a full battery or sole dementia diagnosis. [2][3]
FAB (Frontal Assessment Battery)
Bedside battery sensitive to frontal / dysexecutive dysfunction (conceptualisation, mental flexibility, motor programming, sensitivity to interference, inhibitory control, environmental autonomy). Useful when executive change is suspected (e.g. frontotemporal spectrum hypotheses, vascular executive patterns) but does not replace formal frontal–subcortical testing. [4]
CAM (Confusion Assessment Method)
Standardised tool enabling non-psychiatric clinicians to detect delirium using core features (acute onset/fluctuation, inattention, disorganised thinking, altered consciousness). Delirium must be excluded before attributing low scores to progressive dementia. Systematic reviews support wide clinical use when scored with attention to operational criteria. [5][6]
Quick domain probes (not batteries)
Clock draw, trail-making principles, digit span, category fluency, and three-word recall are rapid probes that generate hypotheses. They lack the reliability and normative depth of formal tests and should not be over-interpreted in isolation. [1][2][4]
Formal neuropsychological assessment
When to refer
Refer (or arrange) formal NP when diagnostic uncertainty remains after screens, functional decline is subtle or domain-specific, after significant TBI/stroke/neurosurgery, for treatment-resistant cognitive complaints, for forensic or capacity-adjacent characterisation needing validity testing, or for standardised schizophrenia cognitive profiles. [7][8][14][16]
How to read an NP report
Read validity and effort first — if performance is invalid, stop severe impairment inferences — then compare premorbid estimate with the current domain profile, map encoding versus retrieval and executive versus amnestic patterns, and translate findings into functional recommendations and differential hypotheses rather than aetiology alone. [7][16][17]
Schizophrenia-relevant cognitive batteries
Cognitive impairment in schizophrenia is common, relatively stable, and more tightly linked to community function than residual positive symptoms alone. Green’s reviews established verbal memory, vigilance/working memory, and executive domains as functionally relevant. [11][12]
MATRICS Consensus Cognitive Battery (MCCB)
The MATRICS initiative selected a consensus battery for clinical trials of cognition-enhancing interventions: test selection, reliability, and validity (part 1) and co-norming/standardisation (part 2). Domains classically cover speed of processing, attention/vigilance, working memory, verbal learning, visual learning, reasoning/problem solving, and social cognition. Functional co-primary measures were studied alongside MCCB so trials capture real-world relevance, not only psychometric change. [8][9][10]
BACS (Brief Assessment of Cognition in Schizophrenia)
Keefe and colleagues developed BACS as a shorter battery targeting domains most impaired and most linked to outcome in schizophrenia, with reliability and sensitivity comparable to longer batteries in validation work. Useful when full MCCB is impractical. [13]
RBANS and HVLT-R
- RBANS — compact multi-domain battery originally validated for detecting and characterising abnormal cognitive status; practical in older adults and as a shorter NP screen. [14]
- HVLT-R — list-learning measure of verbal learning/memory with construct and concurrent validity support; widely used in dementia and psychiatric cognition contexts. [15]
Intelligence testing principles (without test-kit memorisation)
WAIS-class instruments yield Full-Scale IQ and index scores (verbal comprehension, perceptual reasoning/visual spatial, working memory, processing speed — labels evolve by edition). Population mean 100, SD 15. IQ estimates relative standing, not moral worth or capacity; index scatter needs reliability and base-rate context; cultural, educational, language, and sensory factors distort scores; and low IQ must not be equated with inability to hold preferences or participate in supported decision-making. These psychometric principles sit alongside formal NP domain profiling rather than replacing it. [8][14]
Personality testing principles
Objective inventories (MMPI-class and similar) include validity scales detecting under-reporting, over-reporting, and inconsistent responding — these are clinical data, not mere technical footnotes. Projective techniques (e.g. Rorschach, TAT traditions) may generate hypotheses in specialist hands but must never be the sole basis for diagnosis or risk conclusions in exams or practice. Integrate with longitudinal history, MSE, collateral, and performance-validity frameworks when over-reporting or secondary gain is plausible. [16][17]
Effort, performance validity, and malingering frameworks
Performance validity tests (PVTs) and embedded validity indicators assess whether obtained cognitive scores are likely to reflect true ability. The TOMM (Test of Memory Malingering) is a well-studied recognition-based effort measure; normative work includes cognitively intact, impaired, and dementia groups — interpretation still requires clinical context (severe dementia can lower scores; do not use blindly). [18]
Slick, Sherman, and Iverson (1999) proposed diagnostic criteria for malingered neurocognitive dysfunction (MND) integrating psychometric, behavioural, and collateral evidence into possible / probable / definite categories. Sherman and colleagues later updated multidimensional malingering criteria for contemporary practice. [16][17]
Exam discipline: invalid performance is not automatic criminal malice — consider factitious presentation, somatoform exaggeration, disengagement, severe psychosis, delirium, and coaching — while valid low performance can coexist with genuine psychiatric illness. Document inconsistencies such as claimed dense amnesia with intact conversation or near-chance forced-choice recognition, using Slick/Sherman-style multimodal criteria rather than a single test failure. [16][17][18]
Clinical algorithm
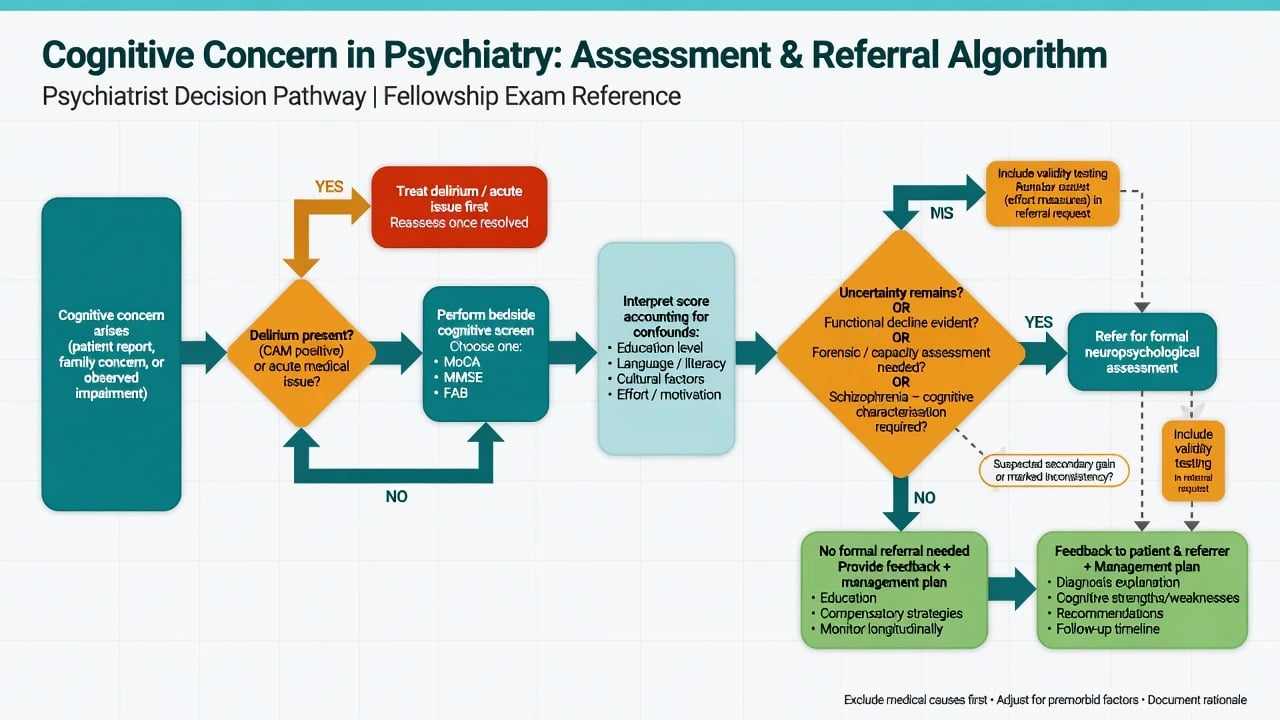
- Define the question (screen? differential? baseline? capacity-adjacent? forensic?).
- Exclude delirium and acute medical drivers (CAM; observations; basic labs as indicated). [5][6]
- Bedside screen (MoCA preferred for mild complaints; MMSE for known moderate impairment tracking; FAB if dysexecutive hypothesis). [1][2][4]
- Interpret confounds — education, language, culture, hearing/vision, depression, medication, sleep, substances, effort. [2][3][16]
- Decide formal NP if uncertainty, functional stakes, atypical pattern, or specialised service need. [7][14]
- Request validity testing when secondary gain or inconsistency is plausible. [16][17][18]
- Feedback and act — education, cognitive remediation referral, occupational planning, organic work-up escalation, serial monitoring.
Differential interpretation table
| Pattern | Prefer | Less likely alone |
|---|---|---|
| Acute fluctuation + inattention | Delirium (CAM+) [5] | Stable progressive dementia |
| Amnestic encoding failure, gradual | Alzheimer-type major NCD hypothesis [7] | Pure depression without organic work-up |
| Executive/behavioural lead | FTD spectrum / vascular / schizophrenia residual [4][11] | Isolated "anxiety" |
| Language-led progressive | Primary progressive aphasia work-up | "Functional" word-finding only |
| Near-chance recognition + secondary gain | Invalid effort differential [16][18] | Verified dense amnesia without further proof |
| Schizophrenia with slow processing + verbal learning deficit | Illness-related cognitive phenotype [11][12] | Medication-only explanation without assessment |
Investigations triggered by cognitive testing
Testing is not a laboratory assay, but abnormal or progressive patterns should trigger targeted medical work-up: metabolic panel, B12, TSH, infection serologies as indicated, medication review, neuroimaging when focal/atypical/progressive features appear, EEG if seizures or encephalopathy suspected. Formal NP refines which questions imaging and labs must answer. [7]
Management implications
- Schizophrenia services: baseline and serial cognition (MCCB/BACS/RBANS) inform rehab, supported employment, and family psychoeducation; functional co-primary measures keep focus on real-world outcomes. [8][10][13]
- Old-age psychiatry: MoCA/MMSE as entry; formal NP for MCI vs major NCD boundary cases; always re-check delirium. [2][5][7]
- CL / TBI: early screens, later formal batteries after acute confounds settle; serial testing tracks recovery vs plateau. [14]
- Feedback: strengths-based, plain language, written summary, avoid deterministic fatalism.
Special populations
- Older adults: education effects; sensory limits; delirium first; Carson MoCA caution. [3][5]
- Youth: age-normed paediatric instruments; adult batteries mislead.
- Intellectual disability / autism: floor effects; multi-informant adaptive function; avoid over-pathologising difference.
- Non-English primary language: interpreters do not automatically validate standardised tests; use bilingual examiners and local norms when possible.
- Indigenous and culturally diverse ANZ populations: interpret scores cautiously; prioritise function, collateral, and culturally safe assessment pathways.
Regional practice notes
Complications and examiner traps
- Ignoring effort when stakes are high. [16][17]
- Practice effects called "recovery."
- Cultural/education bias called "impairment."
- Equating IQ with capacity.
- Ordering a full battery without a question.
- Missing delirium. [5]
- Treating projective tests as gold-standard diagnosis.
Prognosis and disposition
Cognitive trajectories shape prognosis in schizophrenia, dementia, and TBI. Green’s work links specific cognitive domains to community function, supporting investment in cognitive remediation and psychosocial rehabilitation, not only antipsychotic titration. [11][12] Disposition (independent living, supported work, guardianship pathways) rests on function + risk + values, informed by — never replaced by — test scores.
Evidence anchors (memorise for viva)
| Anchor | Take-home |
|---|---|
| Folstein MMSE [1] | Practical bedside grading tool |
| Nasreddine MoCA [2] | MCI-oriented screen |
| Carson MoCA cut-offs [3] | Do not universalise 26 |
| Dubois FAB [4] | Bedside frontal screen |
| Inouye CAM + Wei review [5][6] | Delirium detection structure |
| Sachdev DSM-5 NCD [7] | Six domains; mild vs major |
| Nuechterlein/Kern MCCB [8][9] | Consensus schizophrenia battery |
| Green function papers [10][11][12] | Cognition → real-world function |
| Keefe BACS [13] | Brief schizophrenia battery |
| Randolph RBANS [14] | Compact multi-domain battery |
| Shapiro HVLT-R [15] | Verbal learning validity |
| Slick / Sherman [16][17] | Invalid performance criteria |
| Teichner TOMM norms [18] | Effort test context including dementia |
Exam pearls
- Screen ≠ battery ≠ diagnosis.
- Six DSM-5 cognitive domains. [7]
- MoCA ~26 original teaching cut-off — Carson cautions lower cuts in some samples. [2][3]
- CAM before chronic dementia labelling in acute care. [5]
- MATRICS MCCB is the trial-standard schizophrenia cognitive battery. [8]
- Green: neurocognition predicts function. [11][12]
- Validity first (Slick/Sherman). [16][17]
- IQ mean 100, SD 15 — not capacity.
- Always state education/language/effort confounds when quoting scores.
CASC / communication micro-skills
Explain testing as a way to understand strengths and difficulties so supports can be tailored — not a pass/fail intelligence humiliation. Prepare the patient for duration, breaks, and that some tasks feel hard by design. When feeding back, lead with strengths, then limitations, then practical strategies and next steps. [8][14]
References
- [1]Folstein MF, Folstein SE, McHugh PR "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician J Psychiatr Res, 1975.PMID 1202204
- [2]Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment J Am Geriatr Soc, 2005.PMID 15817019
- [3]Carson N, Leach L, Murphy KJ A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores Int J Geriatr Psychiatry, 2018.PMID 28731508
- [4]Dubois B, Slachevsky A, Litvan I, et al. The FAB: a Frontal Assessment Battery at bedside Neurology, 2000.PMID 11113214
- [5]Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium Ann Intern Med, 1990.PMID 2240918
- [6]Wei LA, Fearing MA, Sternberg EJ, et al. The Confusion Assessment Method: a systematic review of current usage J Am Geriatr Soc, 2008.PMID 18384586
- [7]Sachdev PS, Blacker D, Blazer DG, et al. Classifying neurocognitive disorders: the DSM-5 approach Nat Rev Neurol, 2014.PMID 25266297
- [8]Nuechterlein KH, Green MF, Kern RS, et al. The MATRICS Consensus Cognitive Battery, part 1: test selection, reliability, and validity Am J Psychiatry, 2008.PMID 18172019
- [9]Kern RS, Nuechterlein KH, Green MF, et al. The MATRICS Consensus Cognitive Battery, part 2: co-norming and standardization Am J Psychiatry, 2008.PMID 18172018
- [10]Green MF, Nuechterlein KH, Kern RS, et al. Functional co-primary measures for clinical trials in schizophrenia: results from the MATRICS Psychometric and Standardization Study Am J Psychiatry, 2008.PMID 18172017
- [11]Green MF What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry, 1996.PMID 8610818
- [12]Green MF, Kern RS, Braff DL, et al. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the "right stuff"? Schizophr Bull, 2000.PMID 10755673
- [13]Keefe RS, Goldberg TE, Harvey PD, et al. The Brief Assessment of Cognition in Schizophrenia: reliability, sensitivity, and comparison with a standard neurocognitive battery Schizophr Res, 2004.PMID 15099610
- [14]Randolph C, Tierney MC, Mohr E, et al. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): preliminary clinical validity J Clin Exp Neuropsychol, 1998.PMID 9845158
- [15]Shapiro AM, Benedict RH, Schretlen D, et al. Construct and concurrent validity of the Hopkins Verbal Learning Test-revised Clin Neuropsychol, 1999.PMID 10726605
- [16]Slick DJ, Sherman EM, Iverson GL Diagnostic criteria for malingered neurocognitive dysfunction: proposed standards for clinical practice and research Clin Neuropsychol, 1999.PMID 10806468
- [17]Sherman EMS, Slick DJ, Iverson GL Multidimensional Malingering Criteria for Neuropsychological Assessment: A 20-Year Update of the Malingered Neuropsychological Dysfunction Criteria Arch Clin Neuropsychol, 2020.PMID 32377667
- [18]Teichner G, Wagner MT The Test of Memory Malingering (TOMM): normative data from cognitively intact, cognitively impaired, and elderly patients with dementia Arch Clin Neuropsychol, 2004.PMID 15033228