Psych · Foundations — rating scales and measurement-based care
Rating scales and measurement-based care
Also known as Measurement-based care · MBC psychiatry · Symptom rating scales · Outcome monitoring psychiatry · PHQ-9 GAD-7 PANSS · Routine outcome measurement
Exam-exhaustive fellowship reference on psychiatric rating scales and measurement-based care — PHQ-9, GAD-7, HAM-D, MADRS, PANSS, YMRS, CGI, MoCA/MMSE caveats, reliability and validity, carefully cited cut-offs, MBC evidence (Guo, STAR*D, Fortney, Lewis), and implementation pitfalls. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definitions
A psychiatric rating scale is a standardised instrument that assigns numbers to symptoms, behaviours, or global clinical state. It is not a diagnosis, not a full Mental State Examination (MSE), and not a substitute for risk or capacity assessment. Scales support screening, severity grading, change tracking, trial endpoints, and team communication. [1][5][10]
Measurement-based care (MBC) is the systematic, repeated administration of validated measures before or during encounters, with results used in the session to inform shared decisions (continue, optimise, switch, add, step up). Collecting scores that never alter care is measurement-based charting, not MBC. [10][17]
| Concept | What it is | Common exam trap |
|---|---|---|
| Screening cut-point | Threshold optimising sensitivity/specificity for further assessment | Equating positive screen with disorder |
| Severity band | Ordinal severity ranges on a continuous score | Ignoring function and MSE |
| Response | Relative improvement (often ≥50% reduction from baseline) | Using wrong baseline or wrong scale version |
| Remission | Absolute low score near wellness (definition scale-specific) | Claiming universal cut-offs without citation |
| MBC | Measure → share → discuss → act → remeasure | Measuring without acting |
Classification of instruments
By informant
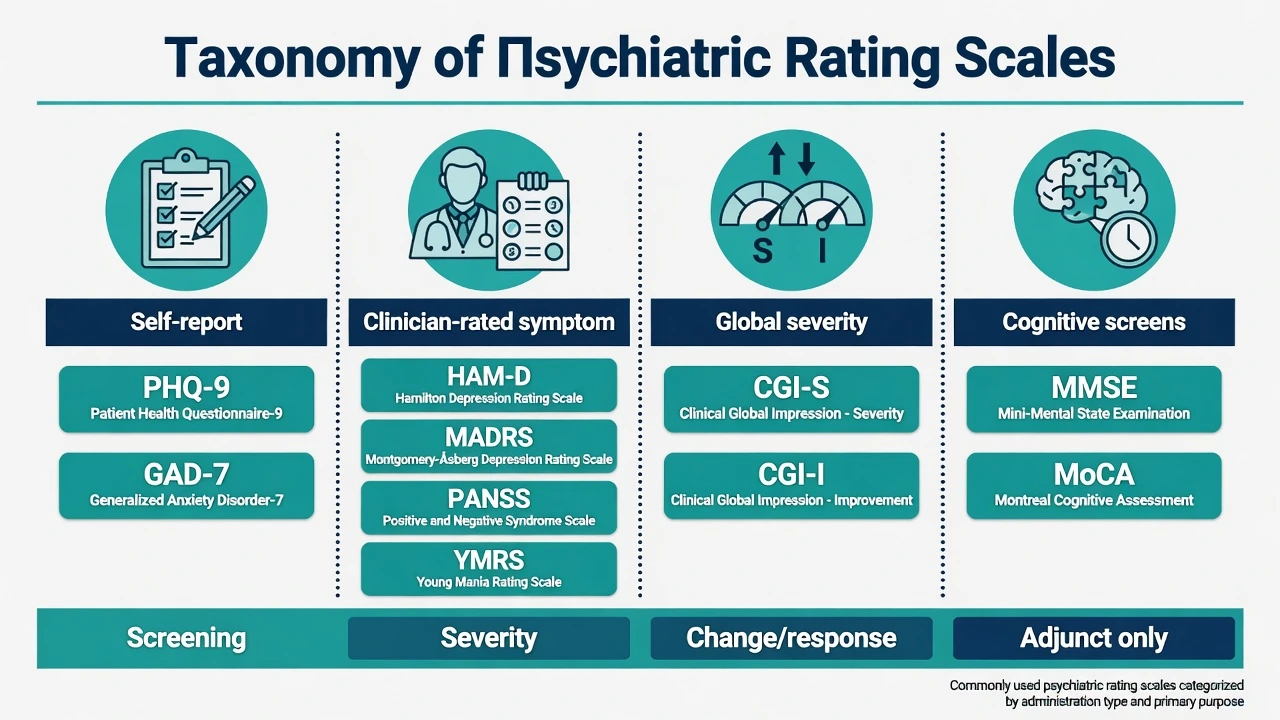
- Self-report (PROMs): PHQ-9, GAD-7 — fast, scalable, patient voice; vulnerable to literacy, insight, and secondary agenda. [1][2]
- Clinician-rated: HAM-D/HRSD, MADRS, PANSS, YMRS — need training and time; better when insight is poor or psychosis/mania is severe. [3][4][5][6]
- Global clinician impression: CGI-S / CGI-I — single-item global anchors useful in clinic and trials. [12]
- Cognitive screens: MMSE, MoCA — screens, not full neuropsychological batteries. [7][8]
By purpose
Screening (case-finding) ≠ severity tracking ≠ diagnostic interview. Many tools do more than one job (PHQ-9 is both a severity metric and a widely used screen), but purpose still dictates interpretation. [1][10]
Psychometrics examiners expect (reliability and validity)
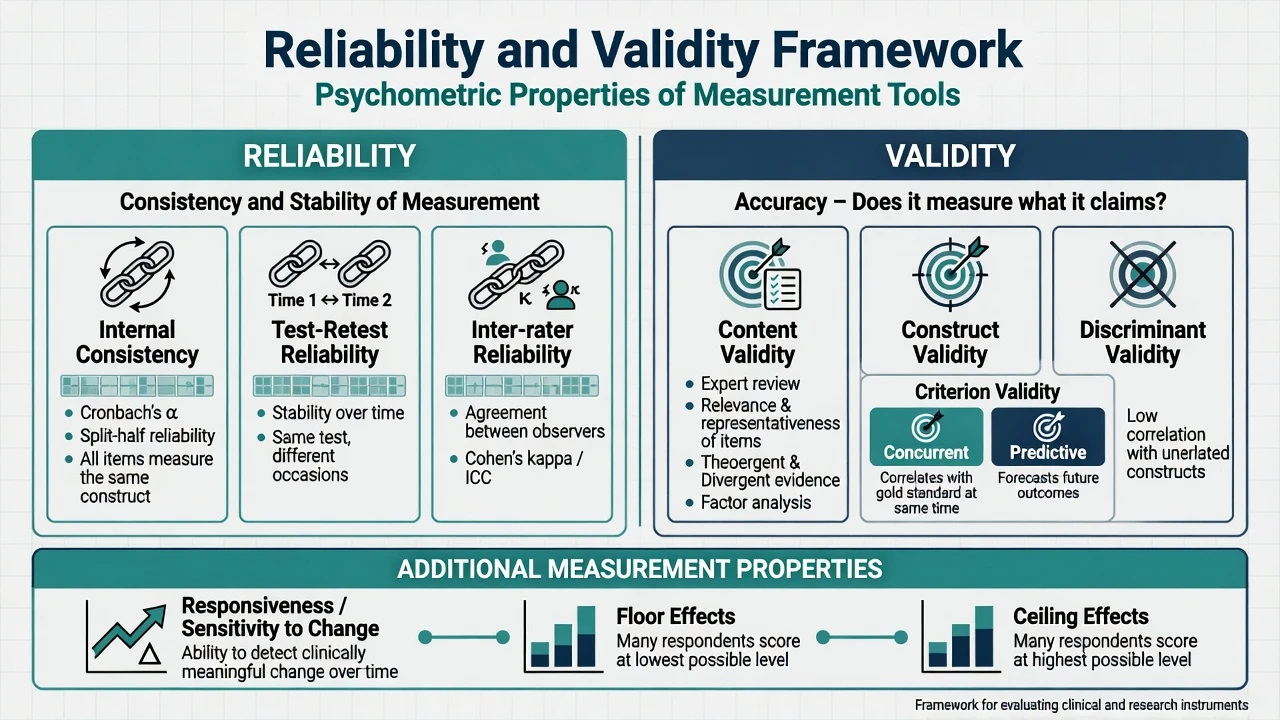
Reliability — reproducibility of scores (internal consistency, test–retest, inter-rater) underpins every validated instrument examiners quote for HAM-D, MADRS, PANSS, YMRS, and CGI. [3][4][5][6][12]
- Internal consistency (items hang together; Cronbach α often discussed) [1][2]
- Test–retest (stability when clinical state is stable) [1][6]
- Inter-rater (critical for HAM-D, MADRS, PANSS, YMRS, CGI) [3][5][12]
Validity — does the tool measure what it claims? Validation programmes for PHQ-9, GAD-7, PANSS, and related scales explicitly test content coverage and criterion relationships. [1][2][5]
- Content (item coverage of the construct) [1][5]
- Construct (converges with related measures; diverges from unrelated) [1][2]
- Criterion (concurrent and predictive relationships with gold standards or outcomes) [1][2]
- Discriminant (separates groups) [1][8]
Responsiveness (sensitivity to change) matters for outcome monitoring. MADRS was explicitly designed to be sensitive to change in antidepressant trials; classic HAM-D remains historically dominant but is more heavily somatic-weighted. [3][4]
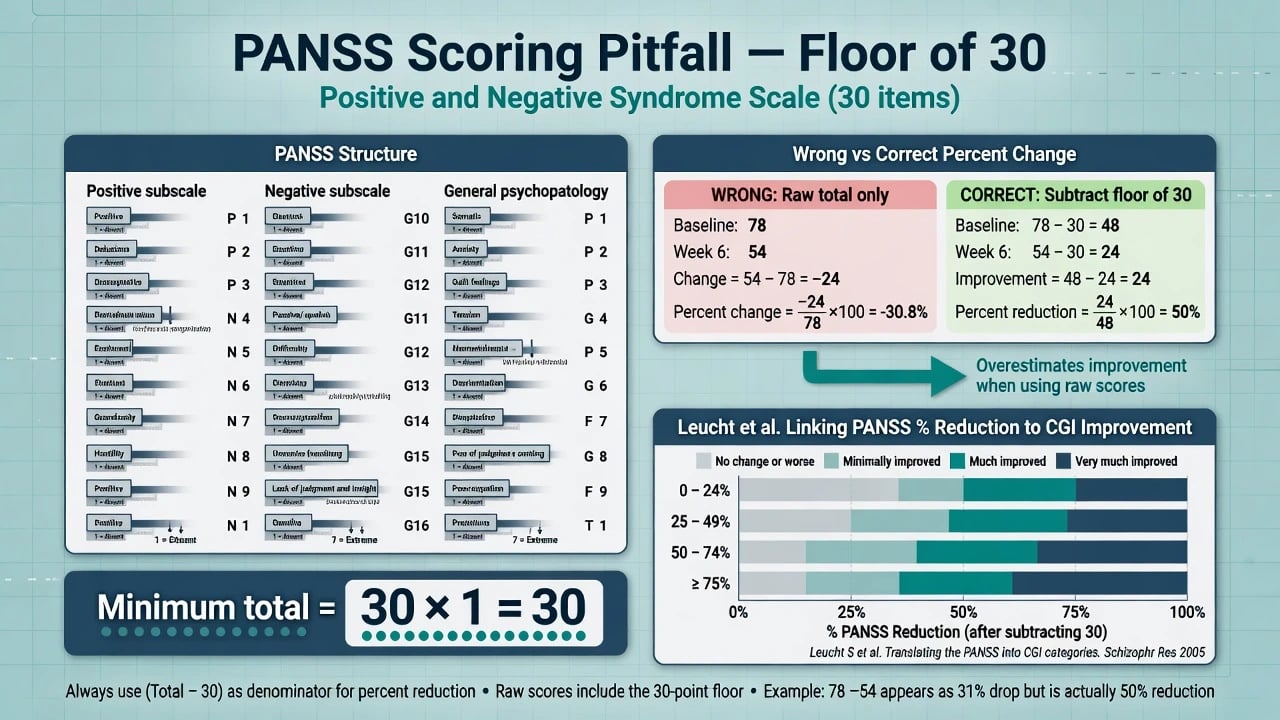
Floor and ceiling effects distort change scores. PANSS items are scored 1–7, so the theoretical minimum total is 30, not 0 — percent improvement must account for this floor. [5][18]
Core instruments (exam depth)
PHQ-9 (Patient Health Questionnaire-9)
- Construct: depression symptom severity over the past 2 weeks; 9 items aligned with DSM major depressive episode symptoms. [1]
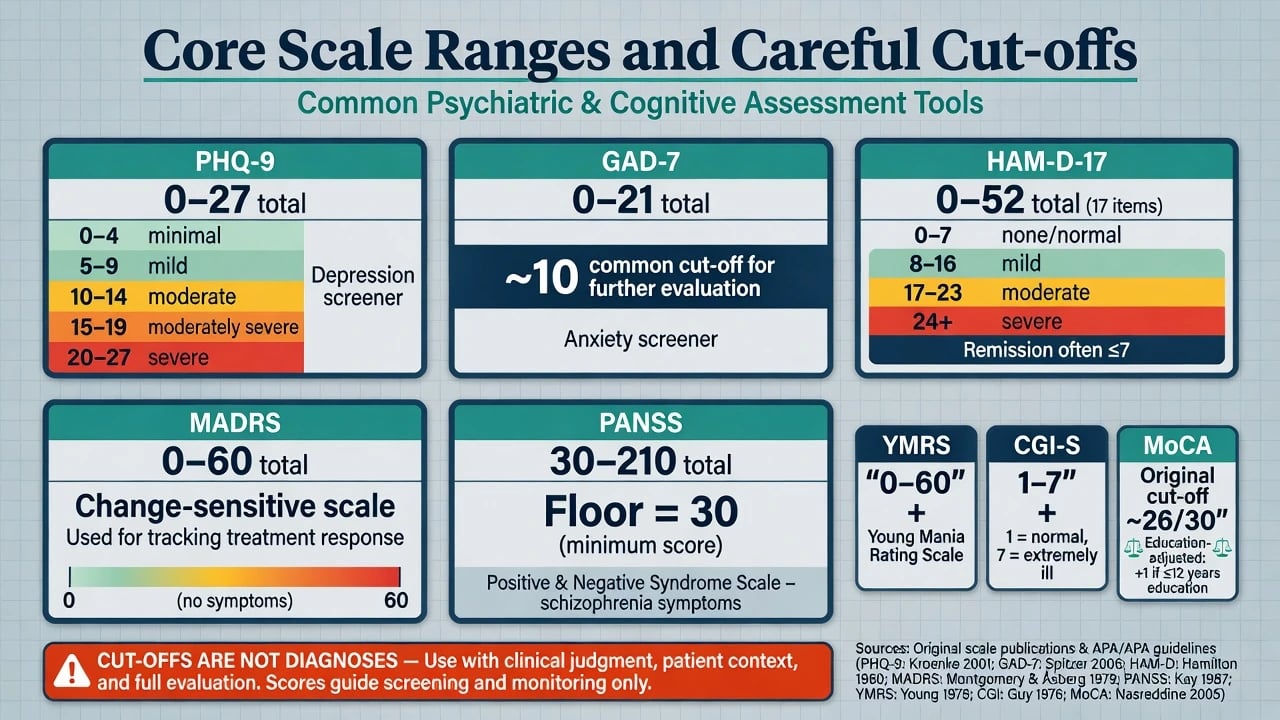
- Score range: 0–27 (each item 0–3). [1]
- Severity bands (Kroenke): scores of 5, 10, 15, and 20 represented cut-points for mild, moderate, moderately severe, and severe depression in the validation work. [1]
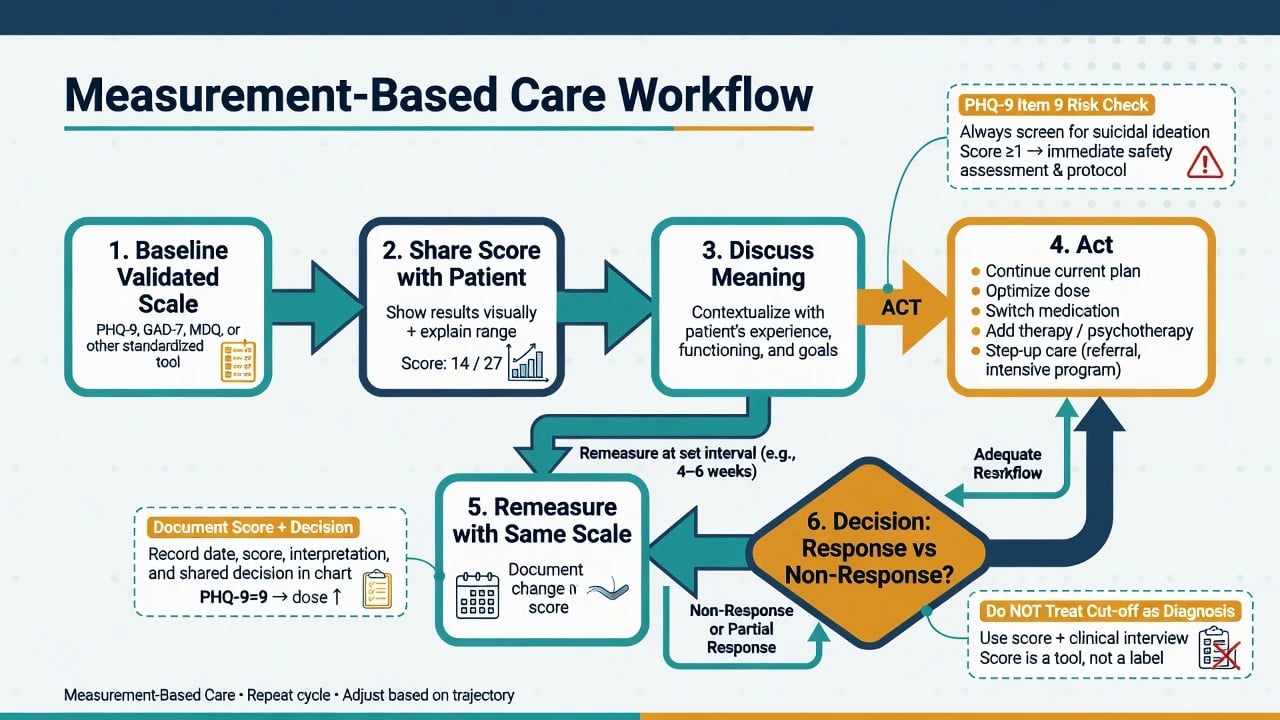
- Item 9 asks about thoughts of being better off dead or of hurting oneself — a positive item mandates structured suicide risk assessment, not reassurance from a falling total score alone. [1]
- Use: primary care and specialty screening/severity tracking; excellent for MBC loops. [1][10]
GAD-7
- Construct: generalised anxiety symptom severity (also elevates in other anxiety presentations). [2]
- Score range: 0–21. [2]
- Screening: a cut-point of 10 was identified as optimising sensitivity/specificity for GAD in the original primary-care validation; severity interpretation uses ordered bands in clinical practice, but always confirm diagnosis clinically. [2]
- Trap: high GAD-7 is not pathognomonic for GAD — consider PTSD, panic, OCD, medical causes, substance. [2]
HAM-D / HRSD (Hamilton Depression Rating Scale)
- Classic clinician-rated depression severity scale; multiple versions (17-item scoring is common in trials). [3]
- Remission in many trials/consensus discussions uses HAM-D ≤7 as a low-score threshold (supportive normative work exists; still operational, not metaphysical wellness). [14]
- Severity bands (Zimmerman outpatient study recommendation): no depression 0–7; mild 8–16; moderate 17–23; severe ≥24 — cite this source when quoting these numbers; other schemes exist. [14]
- Somatic/anxiety items can inflate scores in medical illness and older adults. [3][14]
MADRS (Montgomery–Åsberg Depression Rating Scale)
- 10-item clinician-rated scale designed to be sensitive to change in antidepressant treatment. [4]
- Score range 0–60. Preferred in many modern trials for change sensitivity relative to older HAM-D profiles. [4]
- Still not a diagnostic test; needs trained raters for reliability. [4]
PANSS (Positive and Negative Syndrome Scale)
- 30 items (positive, negative, general psychopathology), each 1–7; total 30–210. [5]
- Gold-standard research severity tool in schizophrenia trials; structured interview training improves inter-rater reliability. [5]
- Percent change pitfall: because the minimum score is 30, calculating percent reduction on the raw total without subtracting 30 underestimates improvement; correct practice uses (score − 30) as the effective symptom span. [13][18]
- Leucht and colleagues linked PANSS totals/changes to CGI anchors so clinicians can translate trial language into global clinical meaning. [13]
YMRS (Young Mania Rating Scale)
- Clinician-rated mania severity scale with demonstrated reliability, validity, and sensitivity to change. [6]
- Tracks severity, not bipolar diagnosis. Use alongside depressive measures when mixed features or polarity switch is a concern. [6]
CGI (Clinical Global Impressions)
- CGI-S (severity) and CGI-I (improvement), typically 1–7 anchors, applicable across diagnoses. [12]
- Fast common language for teams; risk of vagueness if not mentally anchored to specific symptoms and function. [12]
- Busner and Targum describe practical clinical use of this research-derived tool. [12]
MoCA and MMSE — cognitive screens (caveats)
- MMSE: brief bedside cognitive grading tool; limited sensitivity for mild cognitive impairment (MCI) relative to MoCA in many samples. [7][8]
- MoCA: developed as a brief screen for MCI; original work commonly cited a cut-off around 26. [8]
- Carson re-examination: lower cut-offs may be more appropriate in some populations — do not treat 26 as universal law, adjust for education/language, and never diagnose dementia from a single screen. [9]
- Practice effects, delirium, depression, hearing/vision, and non-native language all confound scores. [7][8][9]
Comparison tables (high-yield)
| Scale | Type | Range | Core exam numbers |
|---|---|---|---|
| PHQ-9 | Self | 0–27 | Bands 5 / 10 / 15 / 20; item 9 = suicide item [1] |
| GAD-7 | Self | 0–21 | Screen cut-point often 10 [2] |
| HAM-D-17 | Clinician | version-dependent | Remission often ≤7; Zimmerman severity 0–7 / 8–16 / 17–23 / ≥24 [14] |
| MADRS | Clinician | 0–60 | Built for change sensitivity [4] |
| PANSS | Clinician | 30–210 | Floor 30; fix percent change [5][18] |
| YMRS | Clinician | 0–60 | Mania severity tracking [6] |
| CGI-S/I | Clinician global | 1–7 | Cross-diagnostic common language [12] |
| MoCA | Screen | 0–30 | Original ~26; Carson caveats [8][9] |
| MMSE | Screen | 0–30 | Limited MCI sensitivity [7] |
Measurement-based care — definition, evidence, workflow
Definition and core loop
Fortney and colleagues frame MBC as systematic use of symptom scales to drive clinical decision-making — a practice with a growing evidence and policy "tipping point." [10]
Operational loop (measure → share → discuss → act → remeasure) is the practical heart of MBC as framed by Fortney and implementation reviews: [10][17]
- Measure with a validated tool at clinically sensible intervals [10]
- Share the score (and trend) with the patient [10][17]
- Discuss meaning in context of function, side effects, goals [10]
- Act — continue, optimise dose/adherence, switch, augment, add psychotherapy, intensify level of care [11][16]
- Remeasure and close the feedback loop [10][17]
If step 4 never happens, MBC has failed. [10][17]
Landmark evidence
- Guo et al. (2015): RCT of MBC versus standard care in outpatients with moderate–severe major depression, using blind raters — demonstrated feasibility and effectiveness advantages for MBC. [11]
- STAR*D: large real-world sequenced depression programme using measurement-based care algorithms; Trivedi et al. reported citalopram step-1 outcomes under MBC (remission roughly high-20s% on HAM-D and low-30s% on QIDS-SR definitions in the analysed sample). [16]
- Rush et al.: acute and longer-term outcomes fall as more treatment steps are required — measurement enables recognition of non-remission and orderly step-up. [15]
- Lewis et al. (2019): implementation science review — MBC uptake depends on training, workflow, leadership, health-IT, and feedback culture, not evidence alone. [17]
- Fortney et al. (2017): synthesis arguing psychiatry has reached an actionable tipping point for MBC. [10]
Response and remission language (use carefully)
- Response: often ≥50% reduction from baseline on the chosen severity scale (context-specific; trial protocols vary). [13][16]
- Remission: absolute low score (e.g. HAM-D ≤7 widely used operationally). [14][16]
- PHQ-9: track toward low scores (many services treat scores less than 5 as remission-like recovery bands, while Kroenke’s original severity cut-points start at 5 for mild) — always state your operational definition. [1]
- Schizophrenia trials: percent PANSS reduction thresholds (e.g. 20% vs 50%) have different clinical meanings; Leucht’s CGI linkage helps translation. [13]
*Original GAD-7 validation optimised cut-point — not a diagnosis. [2]
Clinical assessment integration
How to use scales at the bedside
- Introduce the purpose: "These questions help us track how symptoms change with treatment."
- Prefer the same instrument and version over time.
- Record date, scale, raw score, key items (especially PHQ-9 item 9), interpretation, and decision. [1][10]
- Combine with free-text MSE, risk assessment, side-effect review, and functioning — never scores alone.
Discordance
Self-report high / clinician low (or reverse) is clinically informative: denial, alexithymia, cultural under-reporting, secondary gain, rater bias, or true mixed insight. Explore; do not average mindlessly. [1][3]
Acute / emergency settings
Prioritise safety and brief clinician tools (CGI, targeted risk questions, focused MSE). Long self-report batteries may wait until arousal and medical stability allow. Positive PHQ-9 item 9 or suicidal content on any tool triggers structured risk assessment immediately. [1][10]
Differential and interpretive pitfalls
| Finding | Do not assume | Consider |
|---|---|---|
| PHQ-9 ≥10 | MDD proven | Bipolar depression, medical illness, grief, substance, adjustment [1] |
| GAD-7 ≥10 | GAD only | Other anxiety disorders, PTSD, stimulants, thyrotoxicosis [2] |
| High HAM-D | Pure depression | Medical somatic load, anxious distress [3][14] |
| Rising PANSS | Only primary psychosis | Non-adherence, substance, organic, depression on general scale [5] |
| Low MoCA | Dementia | Delirium, depression, education/language, sensory limits [8][9] |
Management: making MBC change outcomes
Practical clinic protocol (depression/anxiety example)
- Baseline PHQ-9 ± GAD-7 at intake. [1][2]
- Review item 9 every time; document risk actions if positive. [1]
- Re-measure at each visit or every 2–4 weeks during active titration. [10][16]
- If minimal improvement by roughly 4–6 weeks of adequate trial, change something (dose, adherence support, switch, augment, psychotherapy intensity) — STAR*D logic of measured non-remission driving next steps. [15][16]
- In specialty mood services, add HAM-D or MADRS for clinician-rated triangulation. [3][4]
Psychosis / mania services
- Serial PANSS (or shorter validated derivatives in some services) and CGI for psychosis programmes; YMRS for mania. [5][6][12]
- Always pair with adherence, substance, metabolic monitoring, and free-text MSE.
Implementation (exam + service design)
Lewis and colleagues emphasise that evidence is necessary but not sufficient: workflow design, training, electronic prompts, leadership priority, and using data in supervision determine whether MBC sticks. [17]
Special populations
- Older adults: somatic items on PHQ-9/HAM-D may rise with medical illness; prefer careful item review; MoCA/MMSE need education/language context. [1][9][14]
- Youth: use age-validated instruments (beyond this topic’s core adult set).
- Perinatal: still useful to track; interpret sleep/energy/appetite items against perinatal norms. [1]
- Intellectual disability / severe cognitive impairment: informant scales and behavioural observation; standard self-report may be invalid. [17]
- Cross-cultural: use validated translations; cut-offs may not transfer; explore idioms of distress. [17]
Complications and examiner traps
Common examiner traps include cut-off worship without interview; ignoring suicide items on PHQ-9; wrong PANSS percent change (forgetting the floor of 30); mixing scale versions; untrained raters; treating MoCA as a capacity or dementia verdict; and questionnaire burden without feeding results back to the patient or changing care. [1][5][8][9][10][18]
Prognosis and disposition
Measured residual symptoms predict ongoing disability and relapse risk; STAR*D shows diminishing remission probability across steps — argument for earlier recognition of non-response via measurement rather than unstructured "seems a bit better." [15][16] Disposition and step-up (GP collaborative care → specialist → intensive programmes) should reference trajectory, not single snapshots. [10]
Evidence and guidelines posture
Primary literature anchors this topic: validation papers for each scale; Guo RCT for MBC efficacy signal in depression; STAR*D for algorithmic MBC in real-world depression; Fortney and Lewis for system-level rationale and implementation. [1][11][16][10][17] Board answers should name instruments, cite operational cut-offs from named sources, and state regional guideline principles (monitor outcomes, collaborative decisions) without fabricating guideline clause numbers.
Exam pearls
MBC-ACT
Summary
Fellowship candidates must select the right tool for the construct, administer and score it correctly, interpret cut-offs with cited humility, integrate scores with MSE and risk, and run a true MBC loop that changes treatment when scores stall. Scales sharpen clinical vision; they do not replace it. [1][5][10][11][17]
References
- [1]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941
- [2]Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7 Arch Intern Med, 2006.PMID 16717171
- [3]Hamilton M A rating scale for depression J Neurol Neurosurg Psychiatry, 1960.PMID 14399272
- [4]Montgomery SA, Asberg M A new depression scale designed to be sensitive to change Br J Psychiatry, 1979.PMID 444788
- [5]Kay SR, Fiszbein A, Opler LA The positive and negative syndrome scale (PANSS) for schizophrenia Schizophr Bull, 1987.PMID 3616518
- [6]Young RC, Biggs JT, Ziegler VE, et al. A rating scale for mania: reliability, validity and sensitivity Br J Psychiatry, 1978.PMID 728692
- [7]Folstein MF, Folstein SE, McHugh PR "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician J Psychiatr Res, 1975.PMID 1202204
- [8]Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment J Am Geriatr Soc, 2005.PMID 15817019
- [9]Carson N, Leach L, Murphy KJ A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores Int J Geriatr Psychiatry, 2018.PMID 28731508
- [10]Fortney JC, Unützer J, Wrenn G, et al. A Tipping Point for Measurement-Based Care Psychiatr Serv, 2017.PMID 27582237
- [11]Guo T, Xiang YT, Xiao L, et al. Measurement-based care versus standard care for major depression: a randomized controlled trial with blind raters Am J Psychiatry, 2015.PMID 26315978
- [12]Busner J, Targum SD The clinical global impressions scale: applying a research tool in clinical practice Psychiatry (Edgmont), 2007.PMID 20526405
- [13]Leucht S, Kane JM, Kissling W, et al. What does the PANSS mean? Schizophr Res, 2005.PMID 15982856
- [14]Zimmerman M, Martinez JH, Young D, et al. Severity classification on the Hamilton Depression Rating Scale J Affect Disord, 2013.PMID 23759278
- [15]Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report Am J Psychiatry, 2006.PMID 17074942
- [16]Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice Am J Psychiatry, 2006.PMID 16390886
- [17]Lewis CC, Boyd M, Puspitasari A, et al. Implementing Measurement-Based Care in Behavioral Health: A Review JAMA Psychiatry, 2019.PMID 30566197
- [18]Obermeier M, Schennach-Wolff R, Meyer S, et al. Is the PANSS used correctly? a systematic review BMC Psychiatry, 2011.PMID 21767349