Psych · foundations — social determinants of mental health
Social determinants of mental health
Also known as Social determinants of mental health · SDH mental health · Structural determinants psychiatry · Social gradient mental disorders · Poverty and mental illness · ACE social psychiatry · Housing homelessness mental health · Equity mental health · Social psychiatry determinants
Exam-exhaustive social determinants of mental health for FRANZCP and MRCPsych: Marmot/Allen/Lund frameworks; structural vs intermediate determinants; life-course and ACE pathways; poverty, inequality, housing, education, employment, racism, migration, urbanicity; Rose population strategy; stigma as structural force; clinical social needs screening; multi-level interventions and equity. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
4 MCQs with explanations
Target exams
Red flags
1. Definitions and frameworks
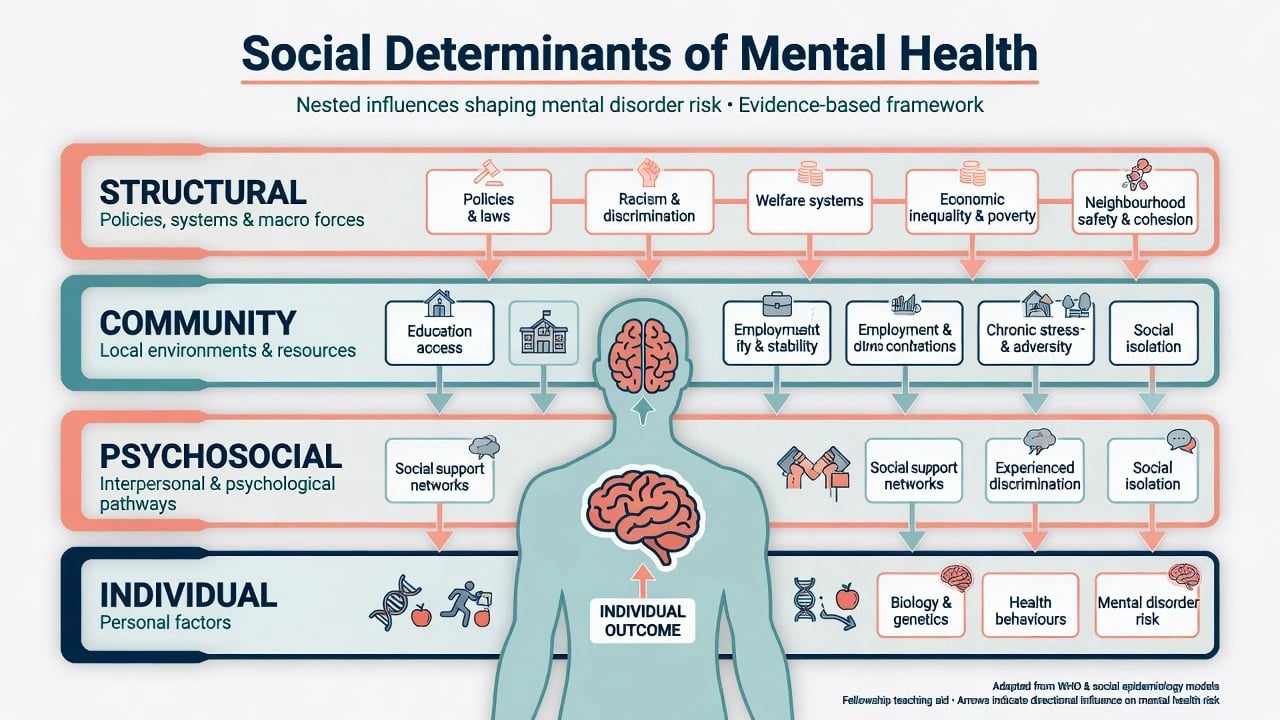
Social determinants of health are the conditions in which people are born, grow, live, work, and age, and the wider systems of power that shape those conditions. Marmot's inequalities agenda makes the social gradient central: health tracks stepwise with socioeconomic position, not only a poor-versus-rich binary.[3]
Social determinants of mental health apply that architecture specifically to mental wellbeing, common mental disorders (CMD), severe mental illness, substance use, and suicide-related outcomes. Allen and colleagues synthesise a life-course, multi-level agenda for mental health policy and practice.[1] Lund and colleagues map determinants of mental disorders onto the Sustainable Development Goals, giving examiners a structured checklist: poverty, education, employment, housing, food insecurity, violence, discrimination, conflict, environment, and health-system access among others.[2]
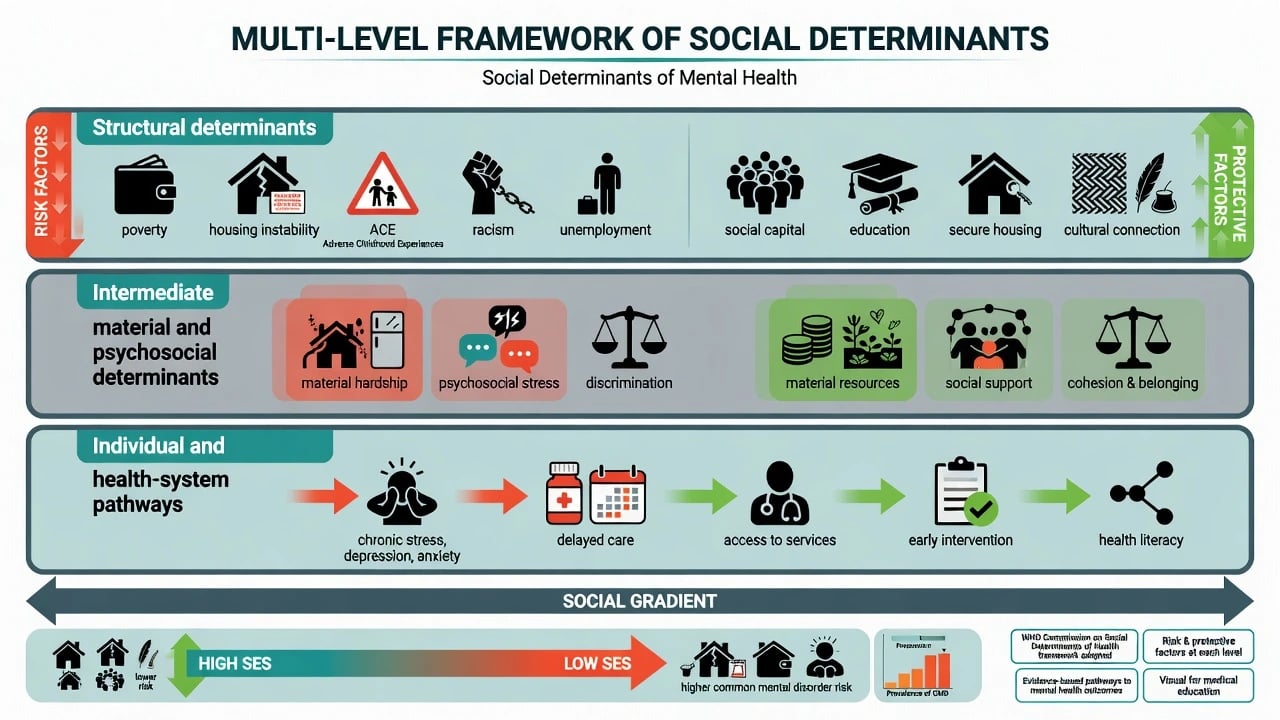
| Level | Examples | Exam use |
|---|---|---|
| Structural | Welfare regimes, racism, gender inequity, labour markets, colonial legacies | Essay openers; equity viva |
| Intermediate material | Income, housing quality, neighbourhood safety, food security | Clinical social history |
| Intermediate psychosocial | Control, status threat, isolation, discrimination experiences | Formulation language |
| Individual/health system | Stress biology, behaviours, literacy, access, quality of care | Care plans and service design |
Protective factors (secure attachment/support, education, cultural connection, social capital, fair employment) are as examinable as risks — prevention is not only risk reduction.[1][9]
2. Epidemiology and the social gradient
2.1 Gradient and burden
Mental disorders contribute substantial global disability burden; social patterning means that burden is unequally distributed within and between countries.[20][3] The gradient appears for distress and many CMDs across socioeconomic indicators (education, income, occupation, area deprivation). Inequality itself — not only absolute poverty — is linked to population mental health narratives examiners recognise from Wilkinson and Pickett.[18]
2.2 Poverty and common mental disorders
In low- and middle-income countries, systematic review evidence links poverty indicators with higher odds of CMD, with heterogeneity by measure and setting.[5] Ridley and colleagues assemble causal evidence that poverty and depression/anxiety influence each other through material stress, cognitive bandwidth, and illness-related productivity loss — the bidirectional poverty trap is a high-yield viva phrase.[6]
2.3 Migration, urbanicity, neighbourhood
Meta-analytic evidence shows elevated schizophrenia risk among migrant groups compared with host populations, with social defeat, discrimination, and selection/causation debates as mechanistic candidates — not genetic essentialism about ethnicity.[17] Urban and neighbourhood disadvantage patterns for psychosis risk sit alongside migration findings as classic social psychiatry epidemiology.[17][2]
2.4 Treatment gap multiplies inequity
Large treatment gaps mean disadvantaged groups both have higher need and lower effective coverage; resources are scarce, inequitably distributed, and often inefficiently used.[12][11] Stigma further suppresses help-seeking.[16]
3. Mechanisms and life-course pathways
3.1 Adverse childhood experiences
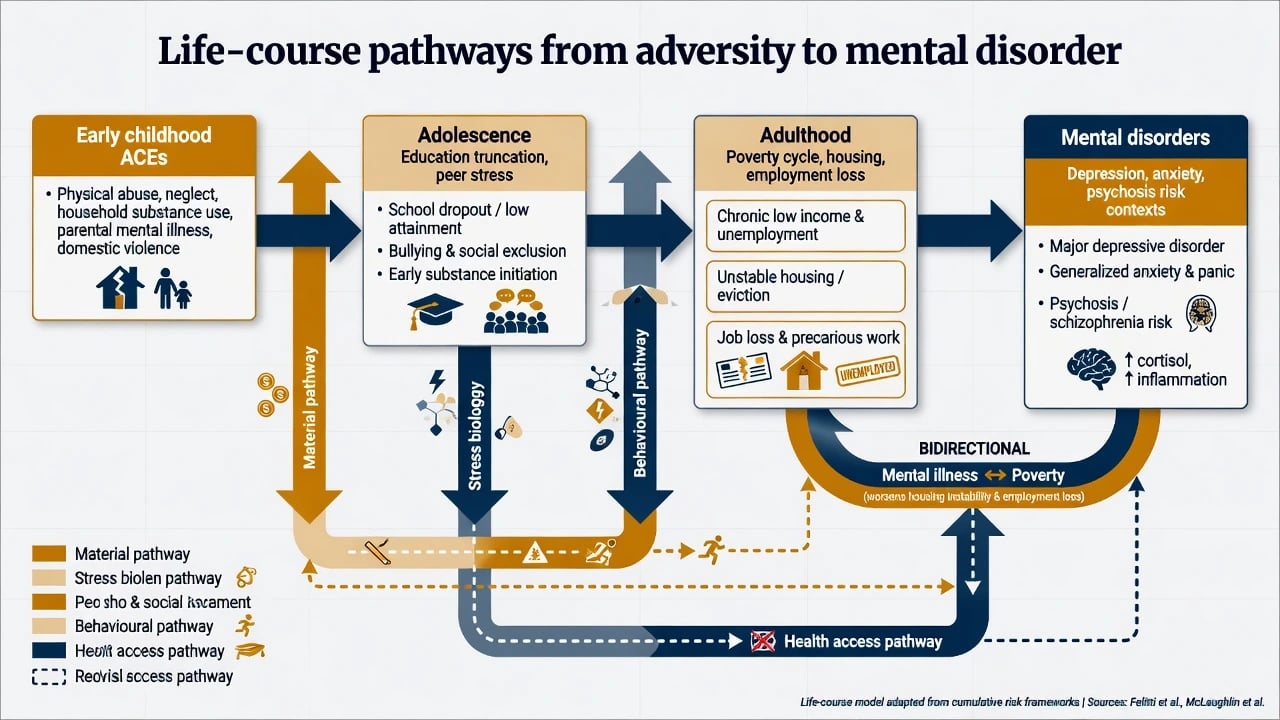
The ACE study demonstrated a graded relationship between childhood abuse/household dysfunction and adult health risk behaviours and disease outcomes, including mental health pathways. Examiners expect the dose–response concept, not a single cut-score fetish.[4]
3.2 Pathway model
- Material: income shortfalls, cold or overcrowded housing, food insecurity, transport barriers to care.[1][2]
- Psychosocial: low control, chronic threat, racism, humiliation, loneliness, caregiving overload.[3][14]
- Behavioural: substance use as coping, sleep loss, deferred help-seeking under stigma.[16]
- Biological embedding: stress-system dysregulation and developmental disruption as plausible mediators (state mechanisms carefully; avoid speculative overclaim).[4][1]
- Health-system: delayed recognition, lower quality care, cultural unsafety, over-use of coercive pathways in some minoritised groups.[11][14]
3.3 Selection versus social causation
Does mental illness cause downward drift, or does adversity cause illness? For many disorders both operate. Ridley's causal review is the modern citation for bidirectional mechanisms in depression/anxiety and poverty.[6] For psychosis, social causation and social selection debates remain examinable; migration meta-analyses keep social risk on the table without discarding biology.[17]
4. Clinical presentation and assessment
4.1 How determinants walk into clinic
Expect housing instability, benefits stress, food insecurity, IPV, workplace bullying/racism, digital exclusion (telehealth failure), and missed appointments that are access failures until proven otherwise.[1][2] Crisis pathways and ED use may substitute for absent primary care access.[11]
4.2 Structured social history (must ask)
- Housing — tenure, overcrowding, eviction threat, homelessness, safety of temporary accommodation.
- Income and food — work, benefits, debt, food insecurity.
- Education and employment — literacy, job insecurity, workplace discrimination.
- Safety — IPV, community violence, elder abuse.
- Belonging — social support, isolation, cultural connection, migration/legal status.
- Discrimination — racism, stigma related to mental illness, sexuality, disability.[1][2][14]
4.3 Formulation
Place SDMH in the social column of BPS and across 4Ps (predisposing ACEs/poverty; precipitating eviction/job loss; perpetuating overcrowding/debt; protective cultural/family capital). Avoid moral language ('lifestyle choice') for structural constraints.[1][4]
4.4 Risk and capacity interfaces
Homelessness, isolation, and IPV change absolute risk of harm and the feasibility of safety plans. Capacity assessment must account for language, literacy, coercion in relationships, and power imbalance — support decision-making rather than defaulting to paternalism or neglect.[10][14]
5. Differential traps
| Trap | Better framing |
|---|---|
| "Just social problems" vs "real illness" | Adversity and threshold disorders co-exist and interact |
| Non-adherence as character flaw | Cost, transport, side-effects, stigma, chaotic housing |
| Culture as pathology | Structural racism and unsafe services drive inequity |
| Area statistics prove individual causation | Ecological fallacy; still use area data for service planning |
| Only high-risk clinics will fix population burden | Rose prevention paradox — need population strategy too |
6. "Investigations" of the social world
Treat social data as essential information: housing status, income source, interpreter need, child protection concerns, immigration status (with confidentiality ethics). Still perform indicated medical workup (delirium, substance, infection, endocrine) — social formulation never replaces organic vigilance, especially in homeless and dual-diagnosis populations.[1][13]
Service-level metrics (DNA by postcode, seclusion by ethnicity, wait times by deprivation) are quality tools for equity, not optional politics.[11][14]
7. Acute and definitive management
7.1 Acute / emergency
Stabilise medical and psychiatric risk first. Parallel-process safety (IPV pathways, child protection principles by jurisdiction — do not invent statute numbers), emergency housing, food, and crisis follow-up. Avoid solitary hospital discharge of high-risk homeless patients.[19][11]
7.2 Multi-level care plan
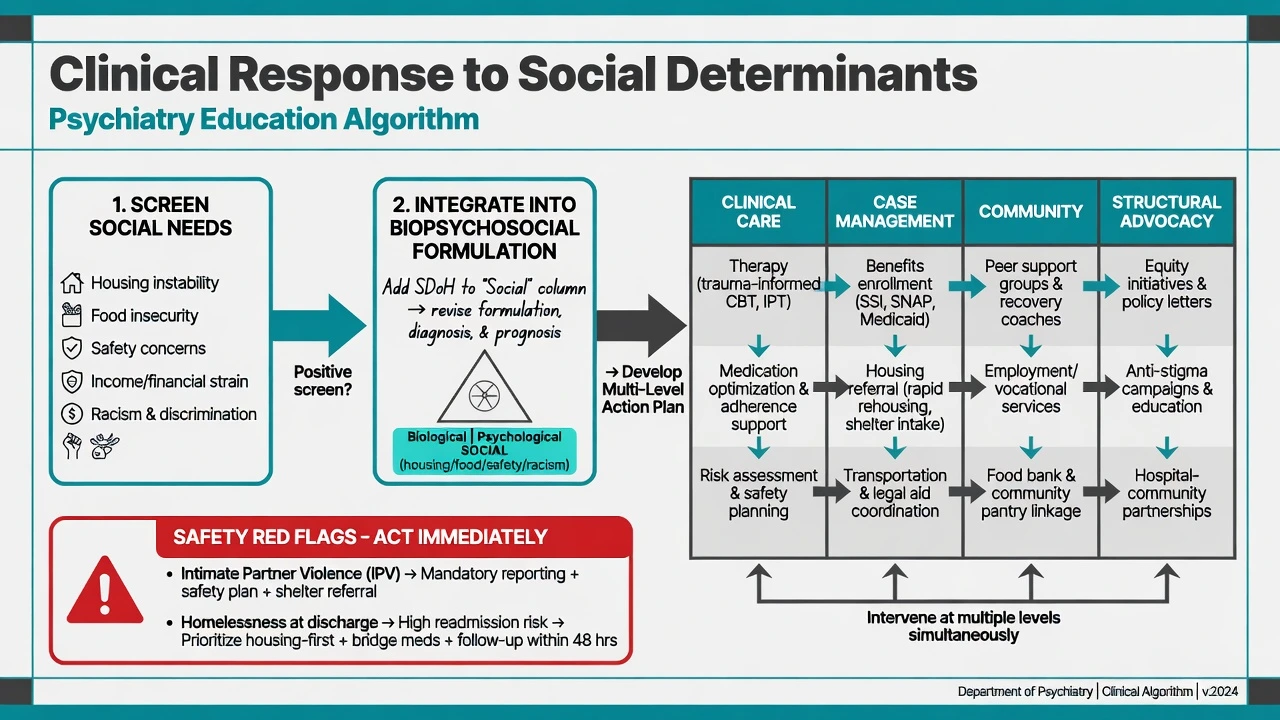
- Clinical care — evidence-based psychological therapies and medication when indicated; trauma-informed engagement; address dual diagnosis.
- Case management — benefits advocacy, housing referral, transport, legal aid liaison.
- Community — peer support, vocational rehabilitation, cultural healers/supports where appropriate and safe.
- Structural — anti-stigma work, service redesign, advocacy for income/housing policy; rights-based practice.[10][15][19]
Housing First logic (stable housing without requiring pre-abstinence for access) is a high-yield principle for homeless SMI discussions — state as model/principle and local implementation variation, not as a universal statute.[10][11]
Collaborative care / primary care integration improves CMD outcomes at scale in under-resourced systems; task-sharing appears in global mental health commissions for specialist scarcity settings.[10][12]
Poverty-alleviation and mental health interventions can reinforce each other when material stress is a maintaining factor.[6][5]
7.3 Prevention stack
- Gordon: universal (school wellbeing, social protection policies), selective (ACE-exposed families, unemployed, perinatal isolation), indicated (subthreshold depression; clinical high-risk states).[8][9]
- Rose: shifting population risk (poverty reduction, anti-bullying, alcohol policy, anti-discrimination) prevents cases from the average-risk middle; high-risk clinics alone leave the prevention paradox unaddressed.[7]
8. Stigma as structural determinant
Stigma is not merely public misunderstanding. Hatzenbuehler, Phelan, and Link argue stigma functions as a fundamental cause of population health inequalities by restricting access to resources, power, and opportunity.[14] Anticipated and experienced stigma reduce help-seeking.[16] Multi-level anti-stigma interventions with contact-based elements have the strongest evidence signals.[15]
9. Special populations
- Children/youth: ACE prevention and school platforms; early onset of many disorders makes early social protection high yield.[4][9]
- Perinatal: financial strain, IPV, isolation drive CMD risk and infant outcomes.[1][2]
- Older adults: isolation, poverty, elder abuse; under-detection of depression.[1]
- Indigenous peoples (ANZ focus): colonisation, racism, land dispossession, intergenerational trauma, and culturally unsafe services — cultural safety and co-design are clinical standards, not optional extras.[2][3]
- Migrants/refugees: elevated psychosis risk contexts; detention and discrimination are determinants, not background colour.[17][2]
- Homeless and forensic interfaces: criminalisation of poverty and untreated illness; diversion and housing are clinical tools.[11][10]
- LGBTQ+: minority stress as a social pathway to mental ill-health.[14]
10. Evidence, guidelines, and public mental health action
Landmark frames: Allen SDMH review;[1] Marmot inequalities;[3] Lund SDG mapping and poverty–CMD review;[2][5] Felitti ACE;[4] Rose and Gordon prevention;[7][8] Arango preventive psychiatry;[9] Lancet Commission global mental health and SDGs;[10] Prince 'no health without mental health';[13] Saxena resource triad;[11] Kohn treatment gap;[12] stigma fundamental-cause and intervention evidence;[14][15] Campion public mental health implementation (including COVID-era shocks).[19]
Implementation failure — not absence of ideas — is the recurring public mental health problem: promotion, prevention, early intervention, treatment coverage, and recovery supports must be resourced and measured.[19][10]
11. Complications and pitfalls
- Ecological fallacy when applying area rates to one person.
- Token social history without actions.
- Recovery rhetoric used to cut beds without community investment.[11]
- Ignoring bidirectional illness–poverty loops.[6]
- Racial stereotyping under equity language.
- Inventing local legal section numbers in viva.
- Assuming clinic samples represent community social risk distributions.[12]
12. Prognosis and disposition
Social collapse (eviction, IPV, benefit sanction, detention) can worsen course faster than a rating-scale point change. Step up intensity and multi-agency support when determinants destabilise, even if MSE is 'only moderately' abnormal. Equity of outcome — who recovers and who is left behind — is a legitimate quality metric.[10][11][14]
13. Exam pearls (rapid-fire)
- Levels: structural → intermediate → individual/health system.[1][3]
- ACE graded relationship is classic.[4]
- Poverty ↔ depression/anxiety bidirectional mechanisms.[6][5]
- Rose + Gordon answer prevention stations.[7][8]
- Migration–schizophrenia meta-analysis is a social psychiatry staple.[17]
- Stigma = structural determinant, not only attitudes.[14]
- Treatment gap + resource triad explain why need is unmet.[12][11]
- Clinical plan without housing/income action is often incomplete.[1][2]
- ANZ: Indigenous equity and cultural safety always on the table.[2][3]
- No health without mental health remains citable rhetoric with a real paper.[13]
SOCIAL-MH (social determinants stack)
14. Related topics
Pair with epidemiology and public mental health for measures and GBD; formulation for 4Ps/BPS technique; stigma/recovery/rights for structural stigma depth; cultural formulation and Indigenous mental health for equity practice; collaborative care and prevention/early intervention for service models; disorder topics for diagnosis-specific treatment once the social architecture is named.[10][19][15]
References
- [1]Allen J, Balfour R, Bell R, Marmot M Social determinants of mental health Int Rev Psychiatry, 2014.PMID 25137105
- [2]Lund C, Brooke-Sumner C, Baingana F, et al. Social determinants of mental disorders and the Sustainable Development Goals: a systematic review of reviews Lancet Psychiatry, 2018.PMID 29580610
- [3]Marmot M Social determinants of health inequalities Lancet, 2005.PMID 15781105
- [4]Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study Am J Prev Med, 1998.PMID 9635069
- [5]Lund C, Breen A, Flisher AJ, et al. Poverty and common mental disorders in low and middle income countries: A systematic review Soc Sci Med, 2010.PMID 20621748
- [6]Ridley M, Rao G, Schilbach F, Patel V Poverty, depression, and anxiety: Causal evidence and mechanisms Science, 2020.PMID 33303583
- [7]Rose G Sick individuals and sick populations Int J Epidemiol, 2001.PMID 11416056
- [8]Gordon RS Jr An operational classification of disease prevention Public Health Rep, 1983.PMID 6856733
- [9]Arango C, Díaz-Caneja CM, McGorry PD, et al. Preventive strategies for mental health Lancet Psychiatry, 2018.PMID 29773478
- [10]Patel V, Saxena S, Lund C, et al. The Lancet Commission on global mental health and sustainable development Lancet, 2018.PMID 30314863
- [11]Saxena S, Thornicroft G, Knapp M, Whiteford H Resources for mental health: scarcity, inequity, and inefficiency Lancet, 2007.PMID 17804062
- [12]Kohn R, Saxena S, Levav I, Saraceno B The treatment gap in mental health care Bull World Health Organ, 2004.PMID 15640922
- [13]Prince M, Patel V, Saxena S, et al. No health without mental health Lancet, 2007.PMID 17804063
- [14]Hatzenbuehler ML, Phelan JC, Link BG Stigma as a fundamental cause of population health inequalities Am J Public Health, 2013.PMID 23488505
- [15]Thornicroft G, Mehta N, Clement S, et al. Evidence for effective interventions to reduce mental-health-related stigma and discrimination Lancet, 2016.PMID 26410341
- [16]Clement S, Schauman O, Graham T, et al. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies Psychol Med, 2015.PMID 24569086
- [17]Cantor-Graae E, Selten JP Schizophrenia and migration: a meta-analysis and review Am J Psychiatry, 2005.PMID 15625195
- [18]Wilkinson R, Pickett K Inequality and mental illness Lancet Psychiatry, 2017.PMID 28552499
- [19]Campion J, Javed A, Lund C, et al. Public mental health: required actions to address implementation failure in the context of COVID-19 Lancet Psychiatry, 2022.PMID 35065723
- [20]Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010 Lancet, 2013.PMID 23993280