Psych · Foundations — social psychology and group dynamics
Social psychology and group dynamics
Also known as Conformity and obedience · Attribution theory · Bystander effect · Groupthink and polarisation · Social identity theory · Cognitive dissonance · Expressed emotion family · Mental illness stigma · Team psychological safety · Group dynamics psychiatry
Exam-exhaustive fellowship reference on social psychology and group dynamics for psychiatrists — attribution, attitudes and dissonance, conformity, obedience, bystander processes, social identity, groupthink and polarisation, stigma, family expressed emotion, and applications to teams, groups, and formulation. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview
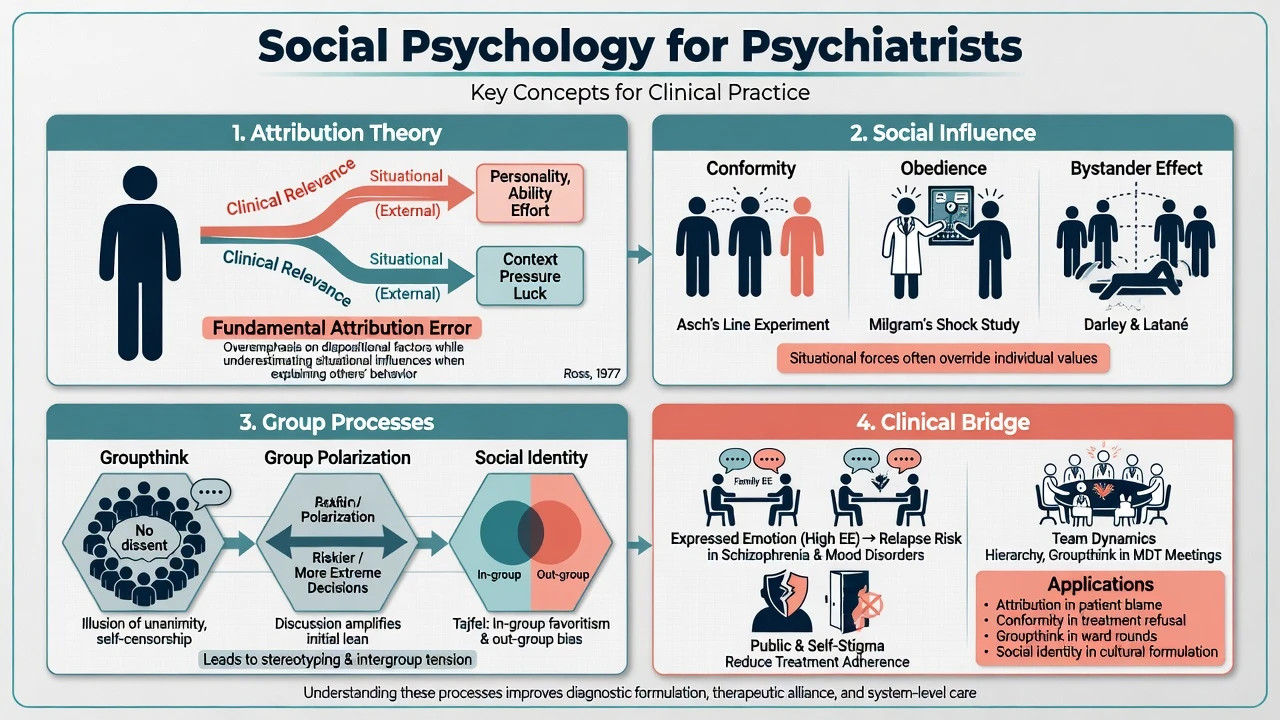
MRCPsych Paper A and FRANZCP foundation theory still examine social psychology hard. The clinical payoff is not trivia about line lengths: it is why juniors stay silent in MDT, why relatives sound “critical,” why patients delay care, and why groups can heal or harm. This page maps core constructs to formulation, family work, teams, and public mental health without undergraduate padding.[5][10][12][14]
Definition and classification
Social psychology studies how the presence of others (real or imagined) influences the individual. For psychiatry, classify the field into examinable clusters that map classic influence research onto clinical bridges (attribution and EE, stigma, teams, and groups).[5][11][12]
| Cluster | Core constructs | Clinical bridge |
|---|---|---|
| Person perception | Attribution; fundamental attribution error; self-serving and actor–observer biases | Blame, formulation of “non-compliance,” carer criticism |
| Attitudes | ABC of attitudes; cognitive dissonance; forced compliance | Ambivalence, motivational work, attitude change after forced treatment |
| Social influence | Conformity, compliance, obedience; normative vs informational influence | MDT hierarchy, consent under pressure, peer norms |
| Prosocial / bystander | Notice–interpret–responsibility–skills–act; diffusion of responsibility | Ward escalation, community overdose response |
| Groups and identity | Social identity, in-group/out-group, polarisation, groupthink | Culture, gangs, therapeutic groups, team decisions |
| Stigma | Public, self, structural, courtesy stigma | Help-seeking, discrimination, recovery culture |
Attribution
People explain behaviour with dispositional (internal) or situational (external) causes. The fundamental attribution error (correspondence bias) is the tendency to over-weight disposition when explaining others’ behaviour while under-weighting situation — a daily trap when notes read “attention-seeking” or “lazy non-attender” without access, stigma, poverty, or fear of services.[11][12]
Carer blaming attributions (symptoms as voluntary, controllable, and intentional) link to criticism and hostility, key components of high expressed emotion.[11]
Attitudes and cognitive dissonance
Attitudes have affective, behavioural, and cognitive components. Cognitive dissonance is aversive tension from inconsistent cognitions or from behaviour that contradicts private attitude. Festinger and Carlsmith’s forced-compliance study: participants paid a small reward ($1) to praise a dull task later rated it more favourably than those paid a large reward ($20) — insufficient external justification drives private attitude change to reduce dissonance.[4]
Clinical pearls: post-decision rationalisation; “I took the depot so it must be helping”; motivational interviewing works with ambivalence rather than forcing compliance that may produce only public agreement without private acceptance — the forced-compliance lesson in reverse.[4]
Conformity, compliance, obedience
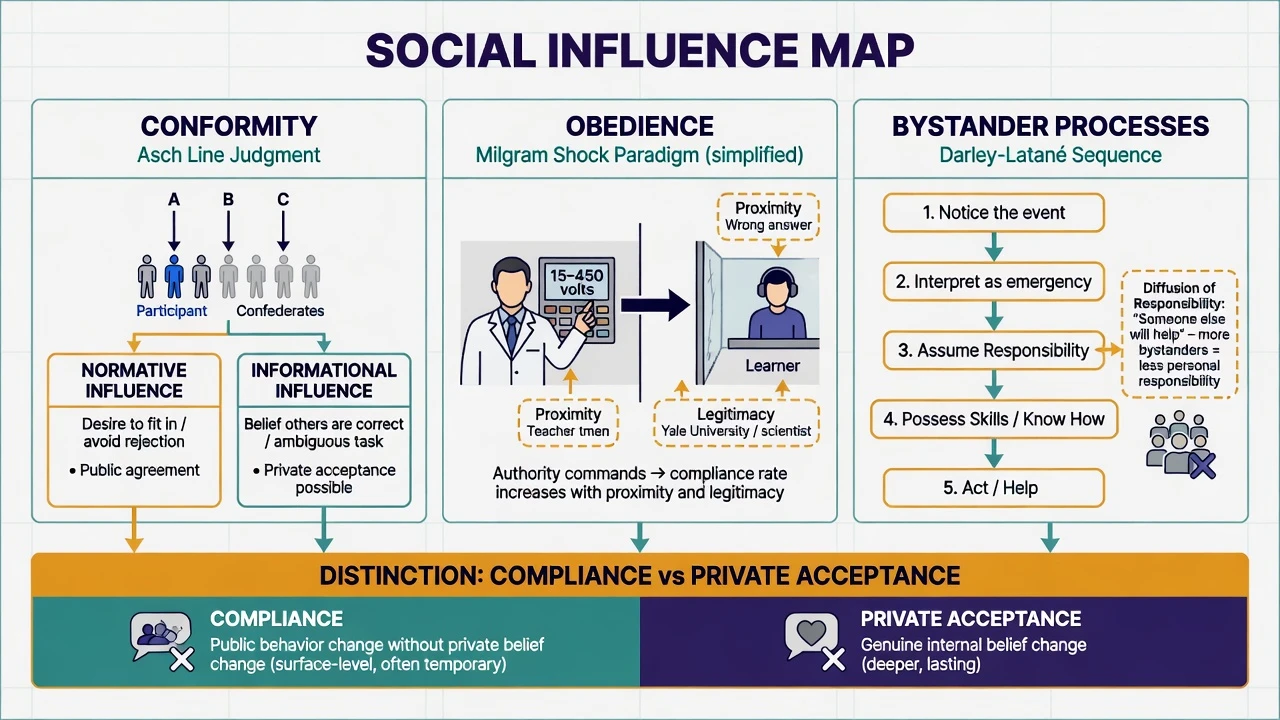
- Conformity: change toward group norms (Asch line paradigm tradition; independence also studied).
- Normative influence: fit in / avoid rejection → often public compliance without private acceptance.
- Informational influence: others as data source under uncertainty → more private acceptance.
- Compliance: request-based public change (may lack private belief change).
- Obedience: change ordered by authority (Milgram). Normative versus informational routes and the obedience distinction remain core exam discriminators for influence stems.[1][5]
Factors raising conformity: unanimous majority, task difficulty/ambiguity, public responding, cultural collectivism (meta-analytic cultural variation in Asch-type tasks is taught at principle level), lower status/self-efficacy.[5][6]
Obedience (Milgram)
Milgram’s laboratory paradigm showed high rates of destructive obedience under experimenter authority, with rates varying by proximity of authority and victim and perceived legitimacy of the setting.[1] Burger’s partial modern replication (stopping at first strong protest) found substantial continued obedience under updated ethics constraints — situational power of authority remains relevant, not a 1960s curiosity.[2]
Ethics teaching point: these designs would not pass modern review as originally run; the lesson is situational force and moral responsibility, not a licence to obey unethical orders in medicine — a point reinforced by ethically constrained modern partial replications that still demonstrate substantial obedience.[1][2]
Bystander processes
Darley and Latané: presence of other bystanders can reduce individual helping via diffusion of responsibility (and related processes such as pluralistic ignorance when others appear calm). Decision sequence examiners like: notice → interpret as emergency → assume personal responsibility → know how to help → act.[3]
Social identity and intergroup processes
Social identity theory: people categorise into groups, identify with in-groups, and compare to out-groups to maintain positive distinctiveness — fuelling in-group favouritism and out-group bias, with meta-analytic work on distinctiveness and differentiation.[7] Clinical bridges: stigma “us/them,” cultural identity in formulation, ward tribes (nursing vs medical), online illness communities that polarise.
Groupthink and group polarisation
Groupthink (Janis tradition, exam-list features): high cohesion + directive leadership + insulation → illusion of invulnerability, collective rationalisation, stereotyping of out-groups, self-censorship, illusion of unanimity, pressure on dissenters, mindguards. Decisions become premature consensus, not wisdom — the antithesis of Asch-informed independence that supports effective group function.[5]
Group polarisation: after discussion, group average shifts more extreme in the initially favoured direction (risky or cautious shift depending on norms) via social comparison and persuasive arguments; social identity processes can further harden in-group extremity against out-groups.[5][7]
Stigma taxonomy
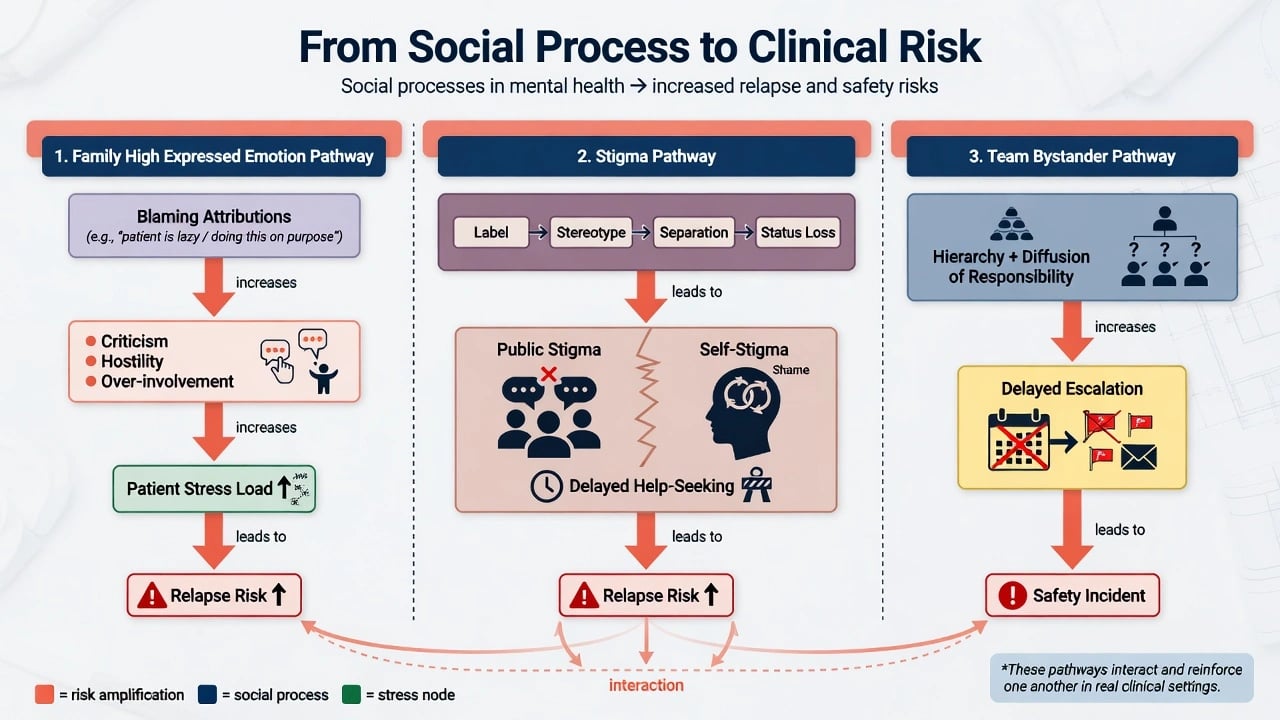
Public stigma (stereotype–prejudice–discrimination), self-stigma (aware → agree → apply → harm), structural stigma, and courtesy/associative stigma harm people with mental illness and families.[12][15] Stigma is a fundamental driver of health inequality and delays help-seeking.[14]
Epidemiology and risk (social processes as risk amplifiers)
Social mechanisms do not have “incidence rates” like a disease, but their clinical risk signatures are measurable and examinable.[9][12][14]
- Anticipated and experienced discrimination are widespread in schizophrenia and related conditions and predict social exclusion.[12]
- Stigma impedes help-seeking across quantitative and qualitative evidence syntheses.[14]
- High EE is a robust psychosocial predictor of relapse in schizophrenia and extends to other disorders.[8][9][10]
- Team diffusion of responsibility and hierarchical silence are organisational risk factors for delayed escalation (patient-safety frame), the clinical twin of classic bystander experiments.[3]
Pathophysiology and mechanisms
EE pathway
High EE is operationalised mainly as critical comments, hostility, and emotional over-involvement (warmth and positive remarks are protective counters). Classic Camberwell work linked high emotional involvement at home to worse course after discharge; meta-analysis confirms EE as a reliable relapse predictor.[8][9][10]
Attributional models: relatives who see symptoms as controllable and intentional show more criticism; this interpersonal climate elevates patient stress load and relapse vulnerability — a social pathway, not “family causation of schizophrenia.”[11]
Stigma pathway
Label → stereotype → separation (us/them) → status loss and discrimination under power imbalances. Self-stigma stages produce shame, secrecy, demoralisation, and reduced self-efficacy for recovery tasks.[12][15][6] Biogenetic “disease like any other” framing can reduce blame yet increase social distance in public attitude data — examiners love this trap.[16]
Influence and team pathway
Authority gradients produce obedience to flawed plans; cohesive teams without dissent produce groupthink; multiple staff who each assume “someone else will call the medical emergency” enact bystander diffusion.[1][3][5] Self-efficacy of the potential helper still matters for whether skills are enacted under stress.[6]
Clinical presentation (how social processes show up)
- Help-seeking delay: “I did not want people to know”; workplace discrimination fears; secrecy after first episode.[14][15]
- Family interview: critical comments about negative symptoms; hostility; intrusive over-protection that blocks autonomy (high EE pattern language).[8][10]
- MSE / history: rejection sensitivity, harsh social comparison, identity fusion with online subgroups, fear of “being the crazy one.”
- Ward/MDT: juniors agree publicly with senior plan they privately doubt; multiple staff document concern without escalating.
- Groups: scapegoating, subgrouping, polarisation into pro/anti-medication camps, contagion of methods. Each pattern is a social-process formulation target, not only a diagnosis label.[5][12]
Differential — mechanism discrimination
| Feature | Conformity | Obedience | Compliance |
|---|---|---|---|
| Source of pressure | Peer / majority norms | Authority figure | Direct request (peer or authority) |
| Classic paradigm | Asch line tradition | Milgram shocks | Foot-in-the-door / sales requests |
| Typical private belief | May be unchanged (normative) | Often conflicted guilt | Often unchanged |
| Ward example | Agreeing with team consensus silence | Following unsafe order from senior | Signing care plan under social pressure |
| Exam trap | Calling all influence 'obedience' | Calling peer pressure 'Milgram' | Ignoring public-only change |
Also contrast groupthink (premature consensus under cohesion) with group polarisation (shift more extreme after discussion) and with healthy dialectical consensus that preserves dissent.[5]
Assessment
- Help-seeking and stigma history: anticipated discrimination, disclosure fears, self-stigma language.[14][15]
- Family climate: critical comments, hostility, over-involvement; consider CFI/FMSS concepts if available; always assess carer burden and support needs.[10]
- Attribution probe: “What do you think causes the symptoms — illness, choice, stress?” maps EE risk.[11]
- Team process after incidents: who noticed, who owned the decision, authority gradient, bystander delay.[3]
- Group suitability: cohesion risks, contagion, capacity to use interpersonal feedback, self-efficacy for group homework.[6]
- Formulation: place social identity, roles, and systemic reinforcers beside biological and psychological lines.
Investigations
No serum test for conformity. Use structured social measures and systems review as the “investigations” of this domain.[10][12]
- Structured EE measures in research/specialist family programmes when available.[10]
- Validated stigma scales when evaluating programmes (exam awareness, not mandatory bedside).[12][15]
- Organisational incident tools that capture hierarchy, communication, and role clarity after harm events (anti-bystander design).[3]
- Medical work-up remains indicated for the underlying psychiatric presentation; social science is additive, not a substitute for organic exclusion when clinically needed.[10]
Acute / emergency management
Do not invoke Milgram to justify following an illegal or unethical order; professional ethics and jurisdiction-specific law outrank hierarchical obedience.[1][2]
Definitive management (application)
Family EE and psychoeducation
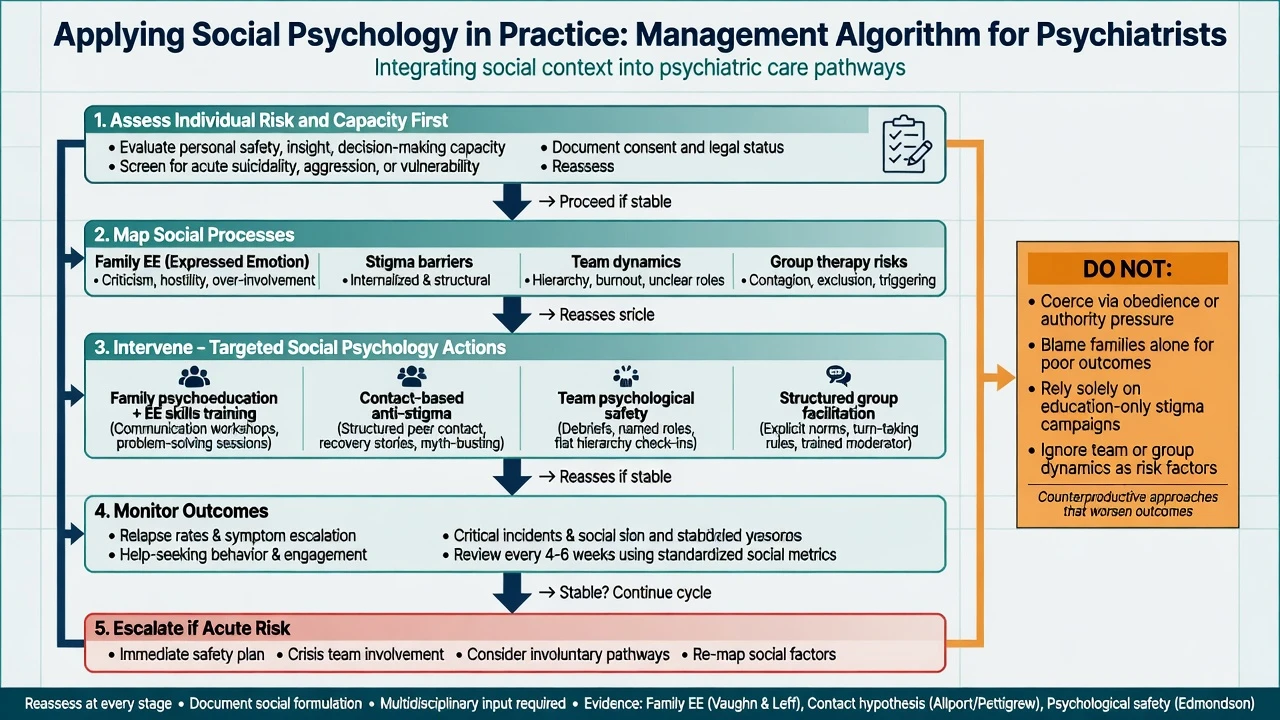
Psychoeducation, communication training, and problem-solving reduce the toxicity of high-EE climates and support carers. Evidence linking EE to relapse justifies family intervention as relapse prevention, not as optional “soft” care.[8][9][10] Address attributions explicitly: symptoms as illness-related and stress-sensitive rather than wilful.[11]
Anti-stigma practice
Evidence syntheses favour social contact interventions (structured, recovery-oriented contact) over education-only approaches for attitude and discrimination outcomes; multi-level strategies also target structural stigma.[13] Self-stigma work includes disclosure decision counselling, peer support, and cognitive approaches to internalised stereotypes.[15] Avoid sole reliance on biogenetic slogans that may widen social distance.[16]
Team psychological safety
Train speak-up behaviours, dual dissent (“two challenge rule” style), and role-named escalation to counter conformity and bystander effects. Debrief incidents for process as well as clinical content.[3][5]
Group therapy facilitation
Set norms, model independence of judgment, interrupt scapegoating, monitor contagion, and process polarisation. Leader authority should invite dissent (anti-groupthink), not demand obedience. Build member self-efficacy for interpersonal experiments.[5][6]
Combining with individual care
Social interventions sit with pharmacotherapy and psychological therapy — shared decision-making rather than forced public compliance without private acceptance where capacity allows. Dissonance theory predicts that heavy coercion without engagement may yield only temporary surface compliance.[4]
Guidelines (regional deltas)
RANZCP / NICE / APA-aligned practice supports family intervention in psychosis, recovery-oriented and rights-based care, and anti-stigma principles. Exact programme names, commissioning routes, and mental health statutes are jurisdiction-specific — quote local pathways in viva; do not invent section numbers. Shared mechanism language (EE, stigma, team communication) travels across boards.[10][13]
Subtypes and scenarios
| Scenario | Dominant social levers |
|---|---|
| First-episode psychosis discharge | Family EE, stigma, identity threat |
| MDT disagreement | Conformity, authority, groupthink |
| Community overdose | Bystander diffusion, pluralistic ignorance |
| Adolescent peer group | Conformity, social identity, contagion |
| Secure/forensic unit | Roles, deindividuation risks, obedience |
| Online forums | Polarisation, informational cascades |
| Perinatal mental illness | Shame, structural stigma, delayed care |
| Cultural minority patient | Intergroup bias, collectivist norms, mistrust |
| Across scenarios, map influence source (peers, authority, family, public) before choosing the intervention lever.[3][7][10][14] |
Complications and pitfalls
- Weaponising EE: shaming families without support increases alliance rupture and secrecy.[10]
- Obedience excuse: “I was just following the consultant” is not an ethical defence.[1]
- Token anti-stigma: posters without contact, power sharing, or structural change.[13]
- Unmoderated groups: method sharing, polarisation against evidence-based care.
- WEIRD over-generalisation: classic samples were often Western students; cultural variation in conformity and family norms matters in formulation.[5][7] Each pitfall either amplifies blame, silences dissent, or fails to convert mechanism knowledge into safer systems.[3][12]
Prognosis and disposition
Lowering high EE and supporting families improves course for many with serious mental illness; stigma reduction improves help-seeking pathways when contact-based and multi-level.[9][13][14] Disposition planning should include family climate, social support density, discrimination risks at work/school, and team handovers that name responsibility (anti-bystander).
Special populations
- Children/adolescents: peer conformity, social media comparison, self-harm contagion — moderate groups carefully.[5]
- Older adults: role loss, loneliness, ageism as structural stigma.
- Indigenous and minoritised communities: intersectional stigma, historical mistrust of institutions; cultural safety over majority-norm conformity pressure.[7][12]
- Intellectual disability: courtesy stigma for carers; exclusion from group programmes.
- Perinatal: shame and anticipated child-protection stigma delaying care for postpartum illness.[14] Developmental and cultural context changes which norms bind, not whether social influence operates.
Evidence pearls (named)
- Milgram 1963 — destructive obedience under authority; situational modifiers.[1]
- Burger 2009 — partial modern replication with ethics constraints; obedience persists.[2]
- Darley and Latané 1968 — bystander diffusion of responsibility.[3]
- Festinger and Carlsmith 1959 — forced compliance and insufficient justification.[4]
- Asch legacy (Levine 1999) — conformity, independence, and group research influence.[5]
- Bandura 1977 — self-efficacy as behaviour-change mediator.[6]
- Jetten et al. 2004 — social identity distinctiveness and differentiation meta-integration.[7]
- Brown et al. 1972; Butzlaff and Hooley 1998; Hooley 2007 — EE and relapse line.[8][9][10]
- Barrowclough and Hooley 2003 — attributions and EE.[11]
- Corrigan; Thornicroft; Clement; Pescosolido lines — stigma impact, discrimination, help-seeking, messaging traps.[12][13][14][15][16]
Exam pearls
SOCIAL — viva checklist
- Small external justification → more dissonance-driven attitude change than large payoff.[4]
- Biogenetic-only anti-stigma can increase social distance.[16]
- Legal frameworks for coercion remain jurisdiction-specific — social psychology never replaces capacity and least-restrictive statutes. These lines convert classic experiments into safe clinical reasoning under exam pressure.[1][10][13]
Summary
Master attribution, dissonance, influence types, bystander dynamics, social identity, group decision failures, stigma, and EE. Apply them to family intervention, team safety, group facilitation, and anti-stigma strategy. That combination — mechanism precision plus ethical clinical use — is what fellowship examiners reward.[3][9][13]
References
- [1]Milgram S Behavioral study of obedience J Abnorm Psychol, 1963.PMID 14049516
- [2]Burger JM Replicating milgram: would people still obey today? Am Psychol, 2009.PMID 19209958
- [3]Darley JM, Latané B Bystander intervention in emergencies: diffusion of responsibility J Pers Soc Psychol, 1968.PMID 5645600
- [4]Festinger L, Carlsmith JM Cognitive consequences of forced compliance J Abnorm Psychol, 1959.PMID 13640824
- [5]Levine JM Solomon Asch's legacy for group research Pers Soc Psychol Rev, 1999.PMID 15661682
- [6]Bandura A Self-efficacy: toward a unifying theory of behavioral change Psychol Rev, 1977.PMID 847061
- [7]Jetten J, Spears R, Postmes T Intergroup distinctiveness and differentiation: a meta-analytic integration J Pers Soc Psychol, 2004.PMID 15149260
- [8]Brown GW, Birley JL, Wing JK Influence of family life on the course of schizophrenic disorders: a replication Br J Psychiatry, 1972.PMID 5073778
- [9]Butzlaff RL, Hooley JM Expressed emotion and psychiatric relapse: a meta-analysis Arch Gen Psychiatry, 1998.PMID 9633674
- [10]Hooley JM Expressed emotion and relapse of psychopathology Annu Rev Clin Psychol, 2007.PMID 17716059
- [11]Barrowclough C, Hooley JM Attributions and expressed emotion: a review Clin Psychol Rev, 2003.PMID 14529701
- [12]Corrigan PW, Watson AC Understanding the impact of stigma on people with mental illness World Psychiatry, 2002.PMID 16946807
- [13]Thornicroft G, Mehta N, Clement S, et al. Evidence for effective interventions to reduce mental-health-related stigma and discrimination Lancet, 2016.PMID 26410341
- [14]Clement S, Schauman O, Graham T, et al. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies Psychol Med, 2015.PMID 24569086
- [15]Corrigan PW, Rao D On the self-stigma of mental illness: stages, disclosure, and strategies for change Can J Psychiatry, 2012.PMID 22854028
- [16]Pescosolido BA, Martin JK, Long JS, et al. "A disease like any other"? A decade of change in public reactions to schizophrenia, depression, and alcohol dependence Am J Psychiatry, 2010.PMID 20843872