Psych · General adult psychiatry — bipolar and related disorders
Acute mania and hypomania management
Also known as Acute mania · Manic episode management · Hypomania treatment · Antimanic treatment · Manic crisis · Bipolar mania acute care · Rapid tranquillisation mania · Valproate loading mania
Exam-exhaustive fellowship reference on acute mania and hypomania management — operational mania vs hypomania criteria; medical work-up and organic mimics; risk, capacity, and legal status; de-escalation, rapid tranquillisation doses, and seclusion principles; lithium/valproate/SGA algorithms with doses and lithium-loading caveats; combination therapy and ECT; hypomania outpatient pathways; step-down to maintenance; RANZCP/NICE/CANMAT/BAP deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Acute mania is a high-stakes fellowship skill: examiners test whether you can separate mania from hypomania, clear the medical differential, contain risk without reckless restraint, prescribe doses with monitoring, explain valproate loading and lithium titration caveats, and plan maintenance before the ward round ends. A FRANZCP MEQ will demand a formulated plan with legal status; MRCPsych CASC will test explanation of diagnosis and lithium to family; ABPN items will punish antidepressant continuation and unsafe rapid tranquillisation combinations.[7][8][10]
Overview and definition
Acute mania and hypomania are elevated-energy mood poles defined operationally, not by informal "high mood." Management is pole-specific: the goal is rapid, safe antimanic control while protecting sleep, capacity, dignity, and medical safety — then preventing the next episode.[17][8]
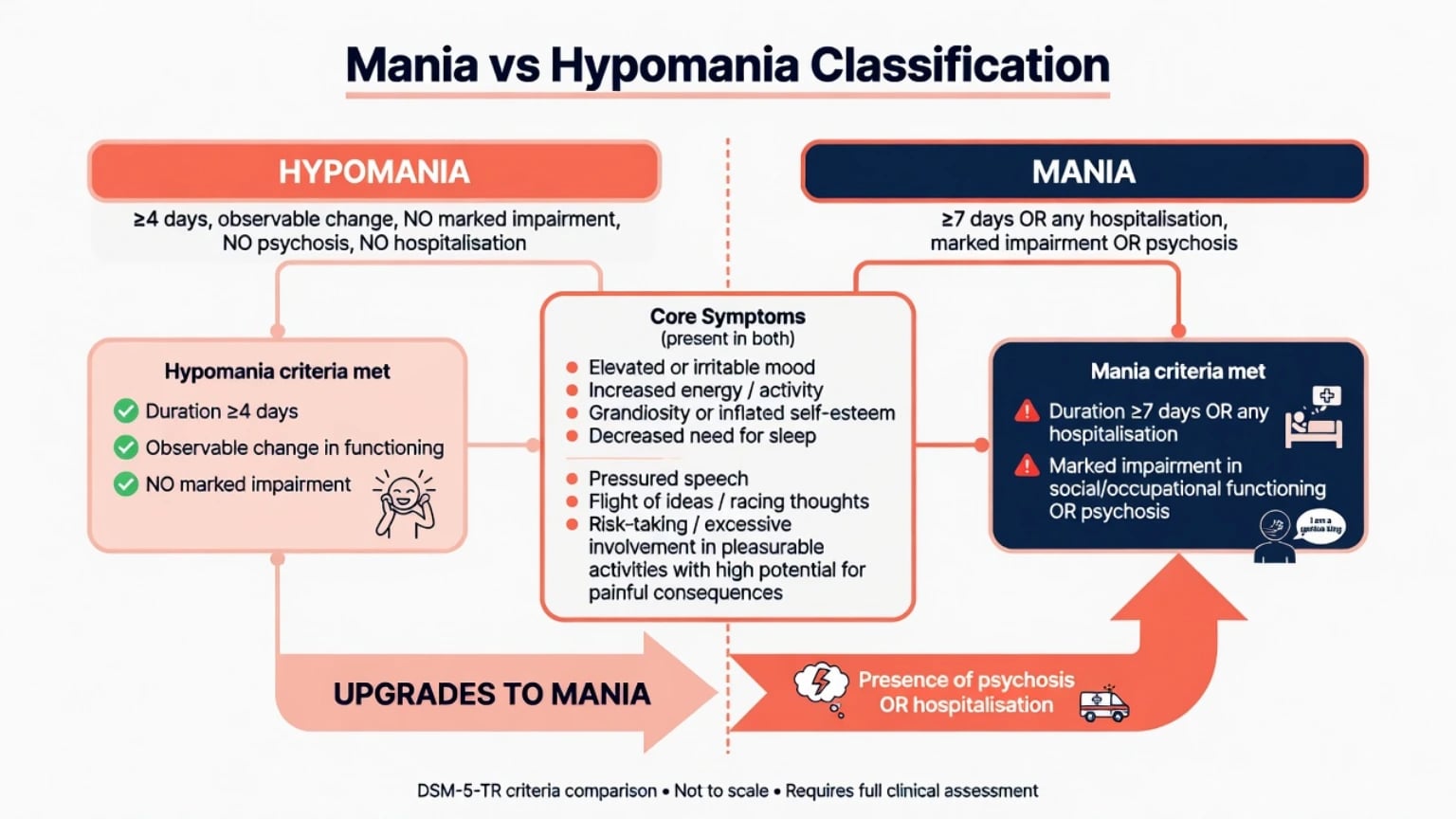
Manic episode (DSM-5-TR framing): Distinct period of abnormally elevated, expansive, or irritable mood and abnormally increased activity or energy lasting at least 7 days (or any duration if hospitalisation is required), with marked impairment, psychosis, or need for hospitalisation. Symptom cluster includes grandiosity, decreased need for sleep, pressured speech, flight of ideas, distractibility, increased goal-directed activity or agitation, and risky behaviour.[17]
Hypomanic episode: Same pole direction lasting at least 4 consecutive days, unequivocal change observable by others, without marked impairment, hospitalisation, or psychotic features. Psychosis or hospitalisation upgrades the episode to mania by definition.[17]
Mixed features: Opposite-pole symptoms (for example depressive cognitions during mania) raise suicide risk and change observation intensity — treat as a high-risk bipolar phenotype, not "ordinary depression with energy."[8]
Epidemiology and risk context
Bipolar spectrum illness is common enough that every acute service sees mania regularly; lifetime bipolar I is on the order of about 1%, with broader spectrum rates higher in large surveys.[18] Peak onset is typically late adolescence to early adulthood; bipolar I sex ratio is roughly equal. Mania drives hospitalisation, forensic contact, relationship and financial catastrophe, and substantial suicide mortality — especially when mixed features or prior attempts are present.[17][18]
Common precipitants examiners expect: sleep deprivation, antidepressant exposure, stimulants or corticosteroids, postpartum period, substance use, non-adherence to maintenance, and seasonal change.[8][17]
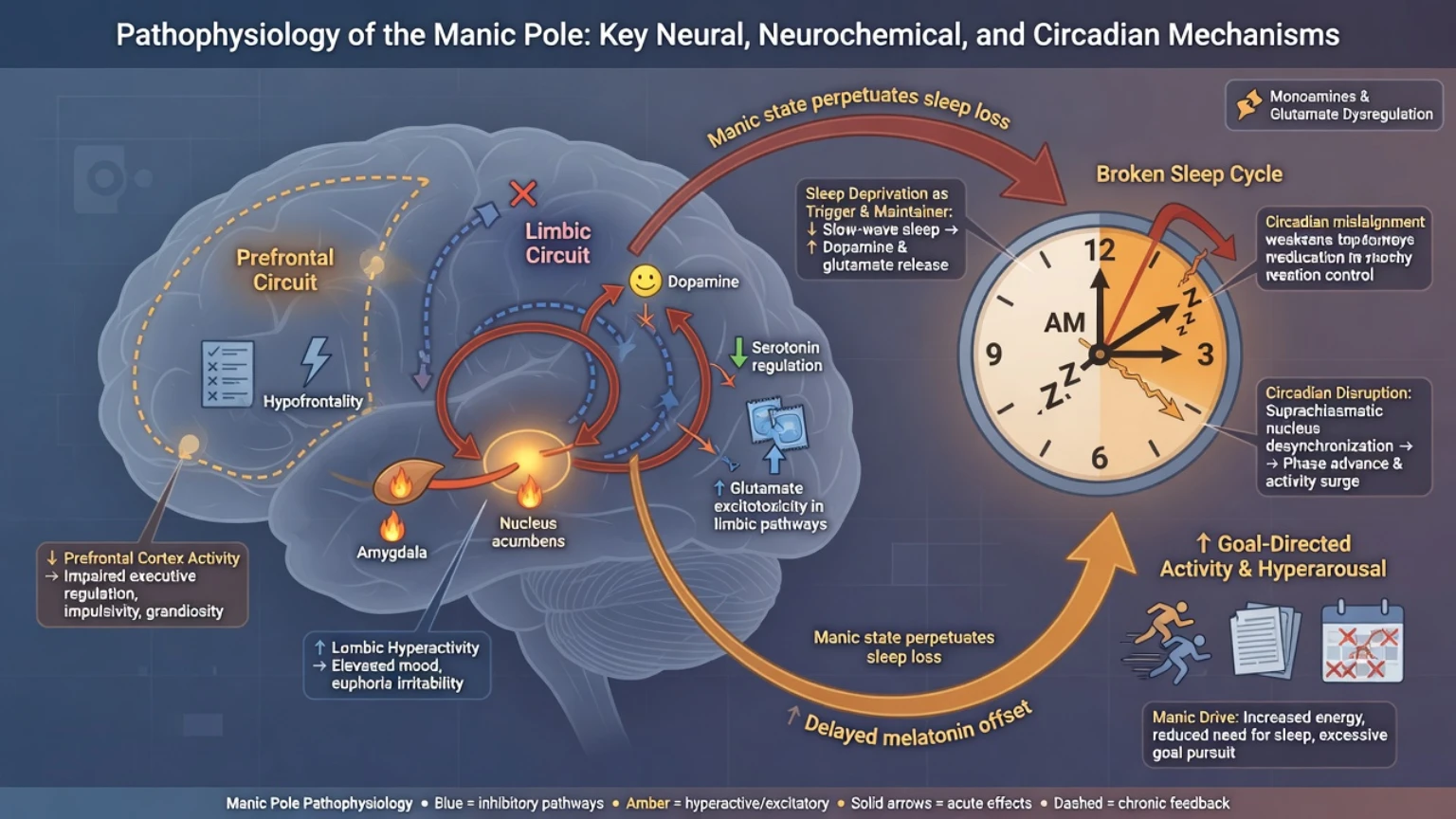
Pathophysiology (exam-level models)
Mania is not explained by a single neurotransmitter. Useful viva models include monoaminergic dysregulation, glutamatergic excess, and circadian/sleep–wake disruption — sleep loss both triggers and maintains the pole. Lithium's multi-target actions (including second-messenger and GSK-3β pathways) provide a mechanistic scaffold for antimanic and anti-suicide effects without implying a diagnostic blood test.[17][14][15]
Classification: mania versus hypomania in practice
| Feature | Hypomania | Mania |
|---|---|---|
| Duration (DSM framing) | ≥4 days | ≥7 days or any duration if hospitalised |
| Functional change | Unequivocal, observable; not markedly impairing | Marked impairment or hospitalisation |
| Psychosis | Absent (if present → mania) | May be present |
| Typical setting | Often outpatient if supports strong | Often inpatient when severe |
| Treatment urgency | Still polarity-safe agents and sleep; close review | Full acute algorithm; combination often |
Clinical presentation and MSE language
Classic mania. Elevated or irritable mood; grandiosity ("I am financing a new hospital"); decreased need for sleep with sustained energy; pressured speech; flight of ideas; distractibility; increased goal-directed activity; sexual disinhibition; reckless spending or driving. Psychotic mania may show mood-congruent grandiose delusions; incongruent content forces a broader differential including schizoaffective and primary psychosis pathways.[17]
Hypomania. Patients often under-report: "I finally feel myself." Families describe charm, productivity, mild spending, reduced sleep need without collapse. Your job is collateral and episode charting so hypomania is not missed until the depressive crash.[8]
Dysphoric and mixed mania. Irritability, lability, tearfulness, and suicidal ideation can coexist with decreased sleep need and pressure — high observation intensity.[8]
Differential diagnosis
Do not lock a primary bipolar label until substance and medical mimics are reasonably excluded — especially first or late-onset mania.[12][8]
- Substance/medication-induced: stimulants, cocaine, cannabis, corticosteroids, antidepressants, excess thyroxine — use timeline, collateral, and urine drug screen (limited sensitivity/specificity).[12]
- Organic mania: hyperthyroidism, Cushing syndrome, frontal lesions, MS, HIV, neurosyphilis, autoimmune encephalitis, epilepsy, B12 deficiency — red flags: fever, focal neurology, seizure, fluctuating attention, systemic signs.[12][17]
- Delirium: fluctuating attention and awareness, vital-sign derangement — medical emergency first.[12]
- Primary psychosis spectrum: chronology of mood versus psychosis; mood congruence.[17]
- ADHD trait hyperactivity vs hypomania: lifelong trait vs episodic change; sleep need; collateral.[8]
- Borderline affective instability: interpersonal tempo, identity, short-lived shifts without sustained decreased need for sleep.[8]
Assessment: risk, capacity, collateral
Structure the encounter as safety first, then diagnosis, then treatment.[8]
- Risk domains: suicide (especially mixed), violence, sexual disinhibition, financial/forensic harm, vulnerability/exploitation, driving, child-protection interface, absconding.[8]
- MSE with quoted speech; sleep hours last week; insight and capacity for treatment decisions.[8]
- Collateral on baseline personality, previous effective agents and levels, adherence, substances, early-warning signs.[8]
- Legal status: least-restrictive pathway under local statute if incapacitous with serious risk — do not invent foreign section numbers in exams.[8][10]
- Scales: YMRS and CGI conceptual use; ward behavioural and sleep charts matter more than a single score.[7]
Investigations and medical work-up
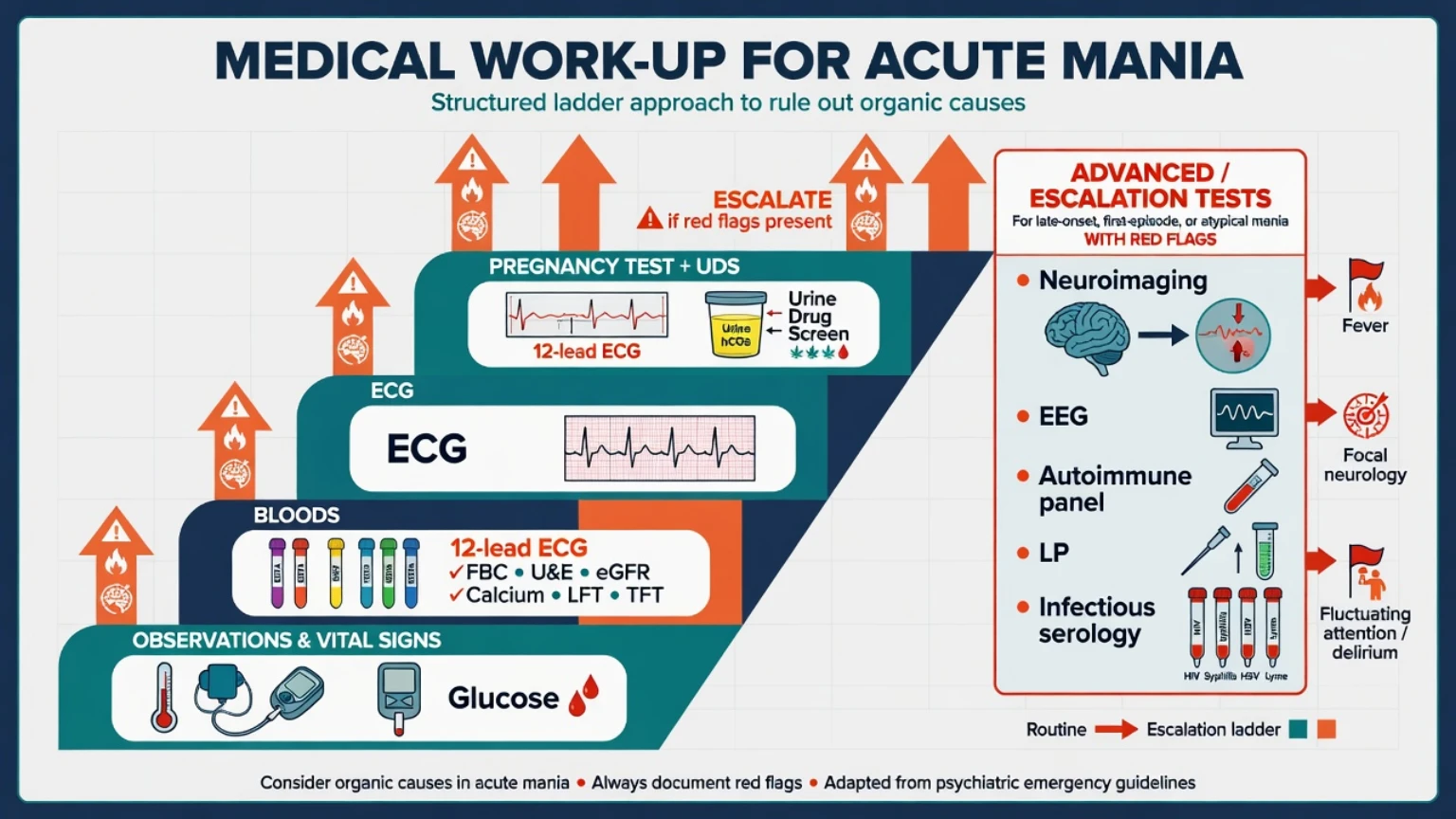
Baseline before antimanic drugs (typical adult set): observations including glucose; FBC; U&E and eGFR; calcium; LFT; TFT; ECG; weight/BMI, BP, lipids and glucose/HbA1c before SGA; pregnancy test if relevant; urine drug screen.[7][8][12]
Escalate imaging/EEG/autoimmune/infectious work-up when first mania is late (classically after about age 40 in exam teaching), atypical, with fever, seizure, fluctuating consciousness, focal signs, or incomplete response that raises secondary mania concern.[12][8]
Drug monitoring essentials:
- Lithium: 12-hour trough; acute mania targets often about 0.8–1.2 mmol/L (individualise); toxicity risk rises substantially above about 1.5 mmol/L. Check level about 5–7 days after initiation or dose change, and after interacting drugs, dehydration, or renal change.[14][9]
- Valproate: many labs target roughly 50–100 mg/L (assay-specific); monitor LFT, FBC; ammonia if encephalopathic. Pregnancy prevention is non-negotiable when relevant.[7][8]
- SGAs: metabolic panel and, when indicated, ECG/QTc — especially with other QT-risk drugs.[7][10]
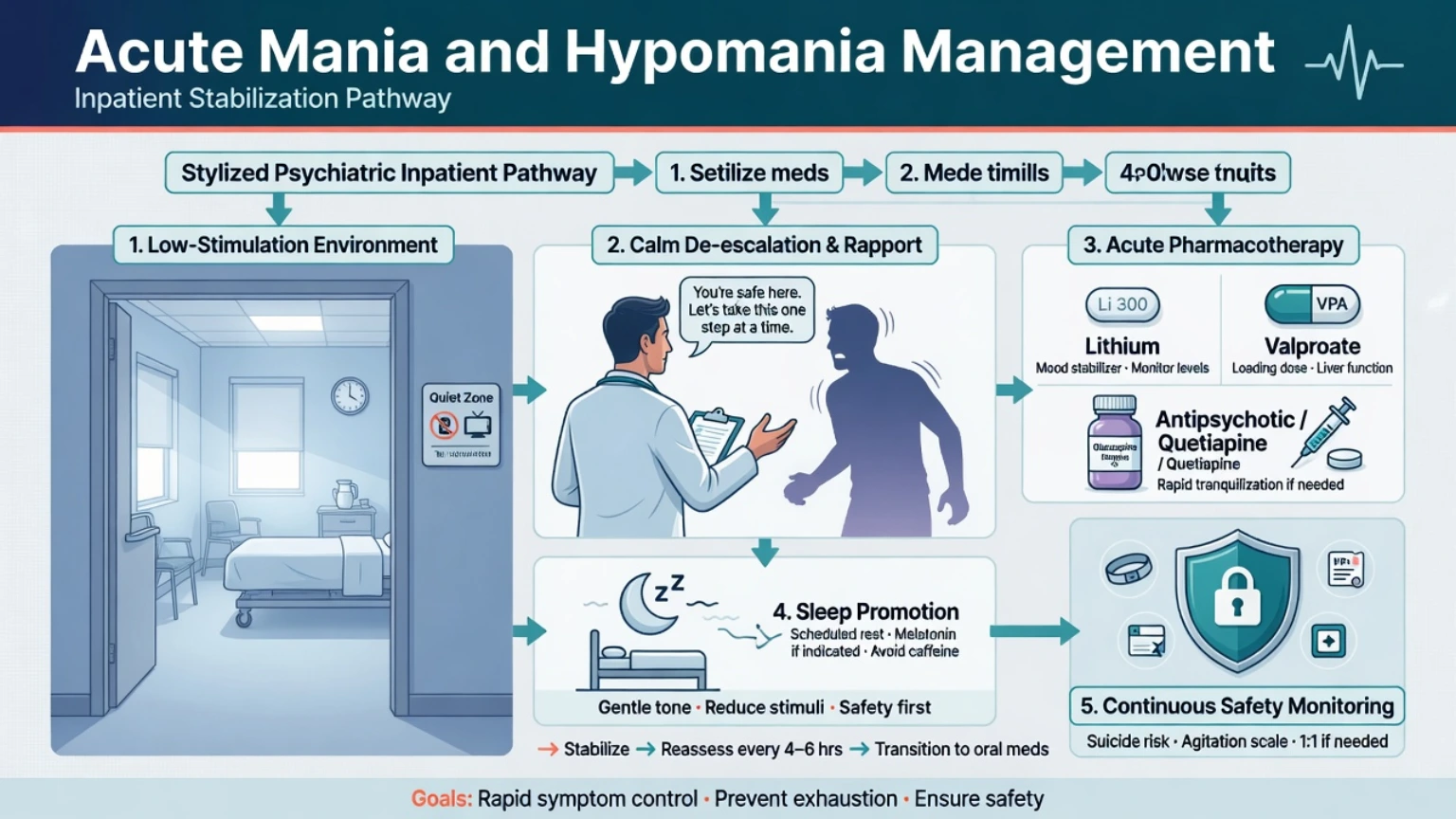
Acute behavioural emergency: de-escalation, RT, seclusion
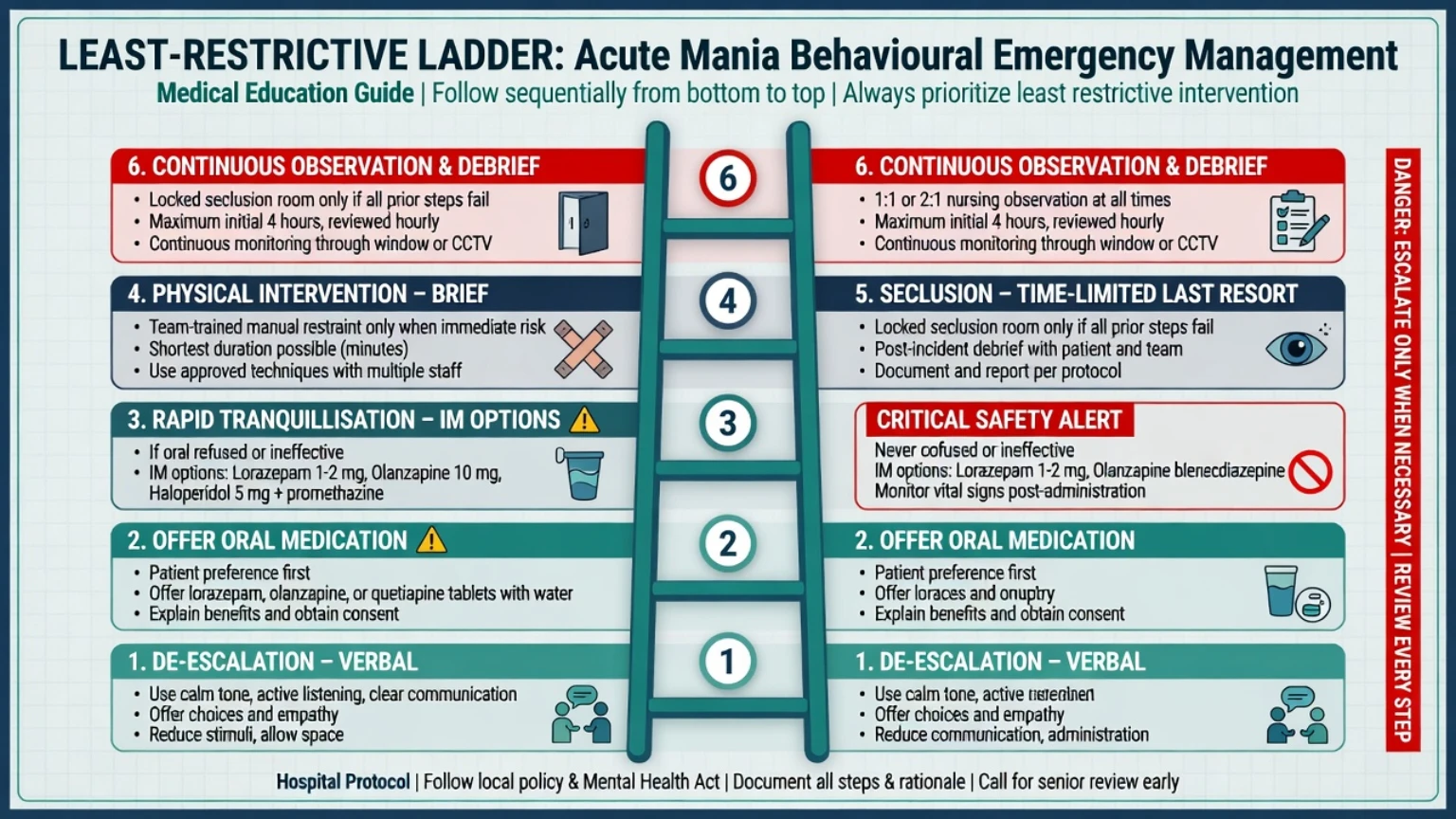
Project BETA and BAP/NAPICU principles agree: verbal de-escalation first, medical causes of agitation considered early, oral medication preferred when safe, parenteral rapid tranquillisation (RT) when necessary for safety, and restrictive practices as last resort.[10][11][12]
Environment. Low stimulation, one spokesperson, offer food/drink/phone contact if safe, protect sleep, remove weapons and access to high-risk means, increase observation level as needed.[11][10]
Rapid tranquillisation — named options (adult protocol principles)
Local protocols govern exact choices; fellowship answers must still name agents and monitoring. Illustrative adult ranges commonly cited in consensus frameworks (always check local formulary and age/hepatic/renal adjustments):[10]
| Step | Example options | Monitoring notes |
|---|---|---|
| Oral first | Lorazepam 1–2 mg oral; promethazine 25–50 mg oral; olanzapine 5–10 mg oral; risperidone 1–2 mg oral | Prefer oral if accepted |
| IM RT | Lorazepam 1–2 mg IM; promethazine 25–50 mg IM; haloperidol 5 mg IM (often with anticholinergic cover available); olanzapine 5–10 mg IM | Continuous observation; SpO2, RR, BP, conscious level |
| ED contexts | Droperidol per ED protocol where used | ECG/QTc awareness |
| Source | BAP/NAPICU illustrative ranges — always use local protocol | [10] |
Post-RT care. Unrousable or desaturating patients are airway emergencies, not "settled." Document indication, capacity/legal basis, dose, response, and physical observations. Offer oral fluids and discussion when settled; plan antimanic cover so RT is not the only treatment.[10]
Seclusion and restraint principles
Seclusion and physical restraint are last-resort, time-limited safety interventions, not treatments of mania. Requirements examiners expect:[10][11]
- Least restrictive option after de-escalation and medication offers fail or are unsafe to wait for.
- Authorisation and documentation under local policy and mental health law.
- Continuous observation; regular nursing and medical reviews; attention to hydration, toileting, temperature, injuries.
- Avoid prolonged prone restraint (positional asphyxia and sudden death risk).
- Post-event debrief for patient, family where appropriate, and staff; review whether antimanic regimen is adequate.[10][11]
Definitive antimanic pharmacotherapy
Network meta-analysis supports multiple effective antimanic drugs, including several SGAs, lithium, and valproate, with trade-offs in acceptability.[1] Landmark RCT evidence established divalproex antimanic efficacy alongside lithium versus placebo.[2] Olanzapine and aripiprazole have classic placebo-controlled acute mania trials.[3][4] Hierarchical guidelines (CANMAT/ISBD, RANZCP, BAP) organise first-line choices and combinations for severe illness.[7][8][9]
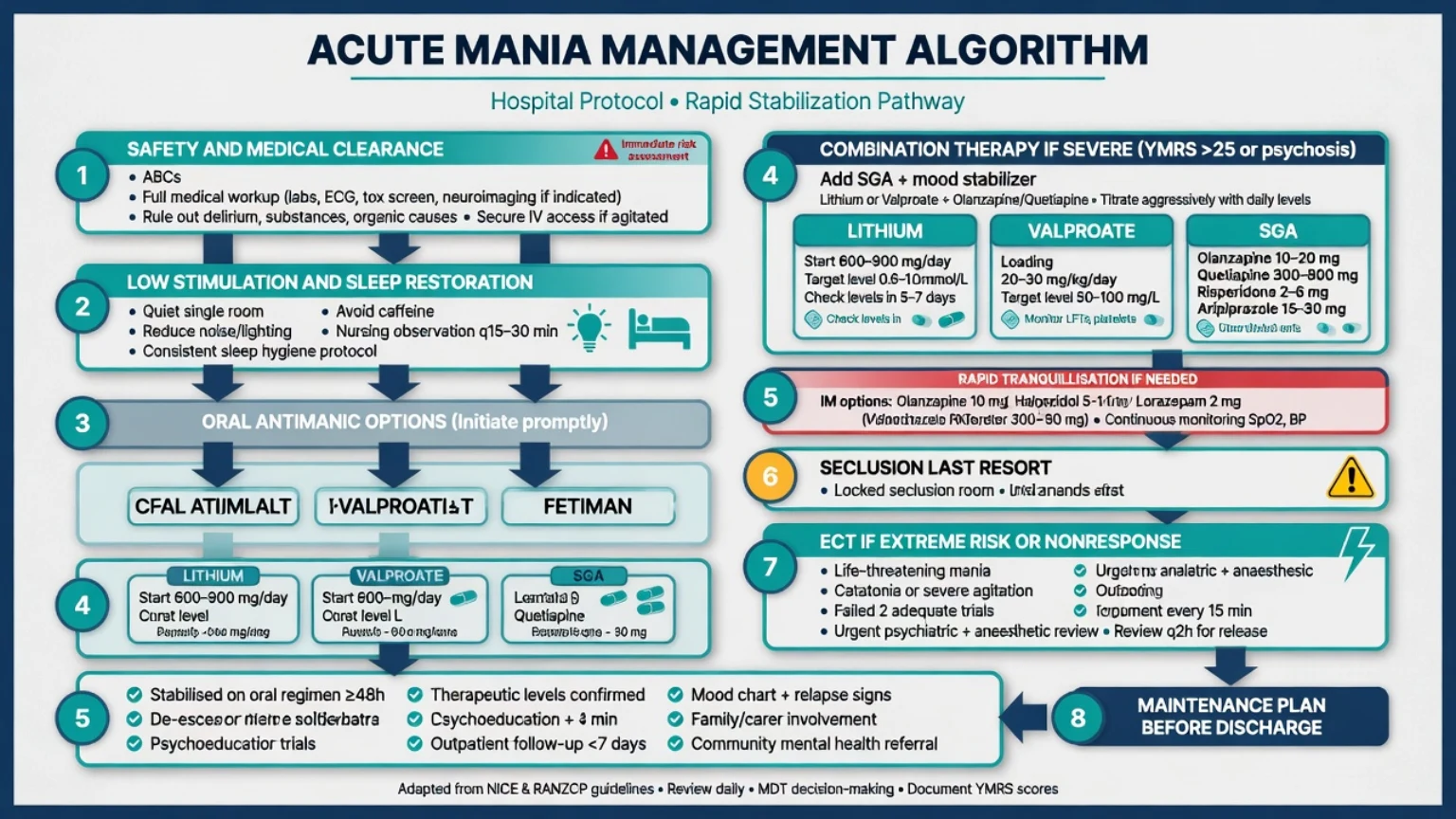
Core acute mania algorithm
- Safety, legal status, medical clearance, sleep.
- Stop antidepressants (and review stimulants/steroids with medical teams).[16][8]
- Start polarity-safe cover — lithium and/or valproate and/or SGA.
- Combine mood stabiliser + SGA when mania is severe, psychotic, or high-risk.
- Adjunctive short-term benzodiazepine for sleep/arousal (e.g. lorazepam 1–2 mg oral/IM as needed within RT rules); taper as pole settles.[10][8]
- ECT for extreme risk, catatonic features, pregnancy scenarios where appropriate, or non-response to adequate pharmacotherapy.[7][8]
- Maintenance plan before discharge — lithium-first prevention when suitable (BALANCE; suicide meta-analysis).[13][15][20]
Agent table — doses, routes, monitoring (adult)
| Agent | Typical acute approach | Monitoring and caveats |
|---|---|---|
| Lithium | Start commonly 450–900 mg/day in divided doses (or local equivalent), titrate to clinical response; 12-hour trough often 0.8–1.2 mmol/L in acute mania | eGFR, U&E, calcium, TFT, level 5–7 days after change; toxicity education; interactions (NSAIDs, ACEI/ARB, thiazides); dehydration |
| Sodium valproate / divalproex | Standard titration or oral loading strategies about 20–30 mg/kg/day in divided doses in selected acute protocols to reach therapeutic levels faster | Pregnancy test and prevention hierarchy; LFT, FBC, levels; avoid casual use in people who can become pregnant |
| Olanzapine | Often 10–20 mg/day oral (start 5–10 mg if elderly/sensitive); IM 5–10 mg for RT only with RT rules | Sedation, metabolic syndrome; never IM + parenteral BDZ |
| Quetiapine | Immediate-release often titrated toward 400–800 mg/day for mania (faster inpatient titration when monitored) | Sedation, orthostasis, metabolic effects |
| Aripiprazole | Often 15–30 mg/day oral for acute mania | Akathisia may mimic agitation — do not blindly escalate antipsychotic |
| Risperidone | Often 2–6 mg/day oral | EPS, prolactin; useful combination partner |
| Asenapine | Sublingual dosing per product (commonly 5–10 mg twice daily where available) | Oral hypoesthesia; adherence to sublingual technique |
| Evidence base | Cipriani NMA; Bowden; SGA mania RCTs; loading and guideline syntheses | [1][2][3][4][5][7][8][14] |
Lithium loading caveats (exam favourite)
"Lithium loading" is not a license for reckless bolus dosing. Fellowship-safe framing:[14][9]
- Lithium has a narrow therapeutic index. Acute mania may justify faster titration toward the higher end of the therapeutic window (often about 0.8–1.2 mmol/L trough) under inpatient observation — not unsupervised mega-doses.[14][9]
- Always obtain baselines (renal function, electrolytes, calcium, TFT, pregnancy test if relevant, ECG as indicated) before aggressive titration.[14][8]
- Schedule 12-hour troughs after steady dosing; recheck after dose changes, intercurrent illness, dehydration, or new interacting drugs.[14]
- Toxicity red flags: coarse tremor, ataxia, dysarthria, vomiting, confusion, myoclonus, seizures — stop lithium, check level and renal function, hydrate, escalate (dialysis thresholds are clinical + level).[14]
- Contrast with valproate oral loading, which has dedicated safety/efficacy literature for more rapid attainment of antimanic serum levels in selected patients.[5][6]
Valproate oral loading
Oral-loaded divalproex (commonly discussed as about 20–30 mg/kg/day in divided doses in research protocols) can achieve therapeutic serum concentrations faster than standard titration and has been studied against standard titration and other antimanics.[5][6] Before loading: exclude pregnancy when relevant, check LFT/FBC, and counsel on sedation, GI effects, tremor, and rare serious hepatic/haematologic reactions. Do not choose valproate as a casual first-line in people who can become pregnant — teratogenicity hierarchy applies even in acute mania; prefer alternatives or documented exceptional multidisciplinary decisions with contraception planning.[8][7]
Hypomania management (not "mild enough to ignore")
Hypomania can often be managed outpatient if risk is low, supports are reliable, and daily or near-daily review is possible. Still:[8][7]
- Use polarity-safe agents (often restart/optimise lithium or SGA; consider valproate only with pregnancy-safe framing).
- Enforce sleep regularity; short-term benzodiazepine if needed.
- Stop antidepressants.
- Written early-warning plan with family; lower threshold to admit if escalation, mixed features, or poor insight.[8][7]
Combination therapy and ECT
Severe, psychotic, or highly agitated mania commonly needs mood stabiliser + SGA. Combination is guideline-supported when monotherapy is insufficient or illness is severe at presentation.[7][1] ECT remains a definitive option for life-threatening risk, catatonia, pregnancy in selected cases, or refractory mania — discuss early rather than after week-long chaotic polypharmacy.[8][7]
Antidepressants and polarity safety
STEP-BD showed adjunctive antidepressants did not improve durable recovery versus mood stabiliser plus placebo in bipolar depression; monotherapy antidepressants in bipolar I are polarity-unsafe and can switch or accelerate cycling. In acute mania/hypomania or mixed features, stop the antidepressant under antimanic cover rather than "treating the tears" with another SSRI.[16][8]
Psychosocial acute package
Even on day one: reduce stimulation, structured ward routine, protect sleep, limit visitors who escalate arousal, involve family for collateral and psychoeducation, and begin a simple explanation of diagnosis and medicines. After stabilisation, offer evidence-based psychosocial prevention (psychoeducation, IPSRT, CBT for bipolar, family-focused approaches) as part of the discharge plan — not as a substitute for acute pharmacotherapy.[8][7]
Special populations
Older adults. Intensify secondary mania work-up; reduce starting doses; lithium renal clearance falls with age; watch delirium, falls, QTc, and drug interactions.[8][14]
Pregnancy and postpartum. Valproate sits at the top of teratogen avoidance hierarchies. Lithium has a small absolute increase in cardiac malformation risk in large data (Patorno) — preconception counselling and specialist perinatal psychiatry input are required; do not improvise in exams.[19][8] Protect sleep aggressively postpartum; link to postpartum psychosis pathways when psychotic mania appears in the first weeks after birth.[8]
Youth. Diagnostic caution, family engagement, careful dosing, and attention to school/forensic risk; avoid adult-style polypharmacy without indication.[8]
Intellectual disability / autism. Diagnostic overshadowing; behavioural phenocopies; careful capacity assessment; environmental interventions carry extra weight.[8]
Prognosis and disposition
Most manic episodes improve over days to a few weeks with adequate antimanic cover and sleep restoration, but functional recovery lags syndromal recovery. Poor prognostic drivers include substance use, non-adherence, mixed features, rapid cycling, and untreated sleep loss.[17][8]
Admit when risk is high, psychosis is present, supports fail, medical work-up needs inpatient setting, or RT/seclusion capacity is required. Community care for hypomania needs reliable review, adherence, and a written escalation plan. Before discharge: confirmed maintenance regimen, level/metabolic plan, sleep schedule, early-warning signs with carers, crisis contacts, and outpatient appointment timing.[8][13]
Guidelines and regional deltas
RANZCP 2020 mood guidelines emphasise formulation, polarity-safe acute care, lithium's central preventive role, and practical monitoring — primary ANZ fellowship anchor.[8]
CANMAT/ISBD 2018 provides hierarchical first-/second-line lists for acute mania with levels of evidence — useful for structured ABPN/Canadian-style answers.[7]
BAP bipolar guidelines and NICE-aligned UK practice stress evidence-based antimanic choices and careful antidepressant use; BAP/NAPICU 2018 is the key acute disturbance/RT consensus for UK-style RT answers.[9][10]
APA/US exam framing often tests FDA-labelled agents, combination therapy for severe mania, and Project BETA medical/de-escalation principles for ED agitation.[11][12]
Exam pearls
Summary
Acute mania and hypomania management is a sequenced craft: define the pole, exclude mimics, contain risk with least-restrictive means, prescribe antimanic drugs with doses and monitoring, respect lithium and valproate loading caveats, avoid antidepressant polarity errors, use ECT when risk or refractoriness demands it, and convert every admission into a maintenance and sleep plan. That sequence is what fellowship examiners are scoring.[1][7][8][10]
References
- [1]Cipriani A, Barbui C, Salanti G, et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis Lancet, 2011.PMID 21851976
- [2]Bowden CL, Brugger AM, Swann AC, et al. Efficacy of divalproex vs lithium and placebo in the treatment of mania. The Depakote Mania Study Group JAMA, 1994.PMID 8120960
- [3]Tohen M, Sanger TM, McElroy SL, et al. Olanzapine versus placebo in the treatment of acute mania Am J Psychiatry, 1999.PMID 10327902
- [4]Keck PE Jr, Marcus R, Tourkodimitris S, et al. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania Am J Psychiatry, 2003.PMID 12944341
- [5]Hirschfeld RM, Baker JD, Wozniak P, et al. The safety and early efficacy of oral-loaded divalproex versus standard-titration divalproex, lithium, olanzapine, and placebo in the treatment of acute mania associated with bipolar disorder J Clin Psychiatry, 2003.PMID 12934987
- [6]Hirschfeld RM, Allen MH, McEvoy JP, et al. Safety and tolerability of oral loading divalproex sodium in acutely manic bipolar patients J Clin Psychiatry, 1999.PMID 10665626
- [7]Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder Bipolar Disord, 2018.PMID 29536616
- [8]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [9]Goodwin GM, Haddad PM, Ferrier IN, et al. Evidence-based guidelines for treating bipolar disorder: Revised third edition recommendations from the British Association for Psychopharmacology J Psychopharmacol, 2016.PMID 26979387
- [10]Patel MX, Sethi FN, Barnes TR, et al. Joint BAP NAPICU evidence-based consensus guidelines for the clinical management of acute disturbance: De-escalation and rapid tranquillisation J Psychopharmacol, 2018.PMID 29882463
- [11]Richmond JS, Berlin JS, Fishkind AB, et al. Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup West J Emerg Med, 2012.PMID 22461917
- [12]Nordstrom K, Zun LS, Wilson MP, et al. Medical evaluation and triage of the agitated patient: consensus statement of the American Association for Emergency Psychiatry Project BETA medical evaluation workgroup West J Emerg Med, 2012.PMID 22461915
- [13]BALANCE investigators and collaborators, Geddes JR, Goodwin GM, et al. Lithium plus valproate combination therapy versus monotherapy for relapse prevention in bipolar I disorder (BALANCE): a randomised open-label trial Lancet, 2010.PMID 20092882
- [14]McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis Lancet, 2012.PMID 22265699
- [15]Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104
- [16]Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression N Engl J Med, 2007.PMID 17392295
- [17]Grande I, Berk M, Birmaher B, et al. Bipolar disorder Lancet, 2016.PMID 26388529
- [18]Merikangas KR, Jin R, He JP, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative Arch Gen Psychiatry, 2011.PMID 21383262
- [19]Patorno E, Huybrechts KF, Hernandez-Diaz S Lithium Use in Pregnancy and the Risk of Cardiac Malformations N Engl J Med, 2017.PMID 28854098
- [20]Miura T, Noma H, Furukawa TA, et al. Comparative efficacy and tolerability of pharmacological treatments in the maintenance treatment of bipolar disorder: a systematic review and network meta-analysis Lancet Psychiatry, 2014.PMID 26360999