Psych · General adult psychiatry — trauma and stressor-related disorders
Acute stress disorder
Also known as ASD · Acute stress reaction (related ICD construct — not identical) · Post-traumatic acute stress syndrome (descriptive) · Early post-trauma stress syndrome
Exam-exhaustive fellowship reference on acute stress disorder — DSM-5-TR Criterion A, 3-day to 1-month window, ≥9 of 14 symptoms, DSM-IV dissociation change, limited PTSD predictive utility, differentials, psychological first aid, prohibition of mandatory single-session debriefing, trauma-focused CBT evidence (Bryant trials), selective pharmacology, ICD-11 contrast, and special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Acute stress disorder (ASD) is the fellowship exam’s “first-month” trauma diagnosis: high-stakes in ED, trauma wards, sexual assault services, disaster response, and C-L, and a classic trap when candidates either pathologise every normal acute reaction or miss the difference from PTSD, adjustment disorder, and ICD-11 acute stress reaction.[1][3][9]
Overview and definition
ASD captures severe early psychological reactions after qualifying trauma. It is not a synonym for “anyone distressed after a bad day,” and it is not automatic PTSD. It exists to identify people who need clinical care in the acute window and, imperfectly, to flag elevated risk of chronic post-traumatic psychopathology — though predictive performance is limited.[1][2][11]
What ASD is not. It is not a lab diagnosis. It is not mandatory debriefing. It is not adjustment disorder after a non-traumatic stressor. It is not ICD-11 “acute stress reaction” (a transient non-disorder construct). Historical emphasis on dissociation as necessary for diagnosis was deliberately loosened in DSM-5 because the DSM-IV requirement missed many who later developed PTSD.[1][9]
Classification and diagnostic criteria
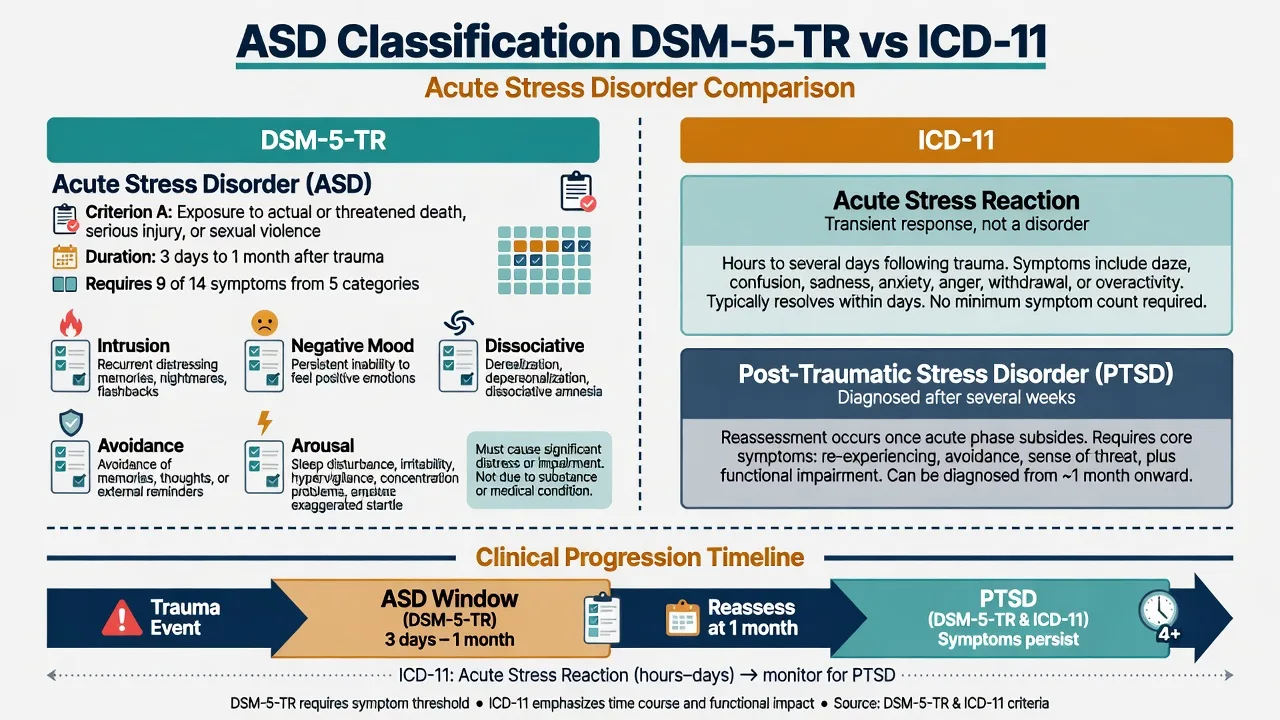
DSM-5-TR spine (reproduce in viva)
- Criterion A — trauma exposure: exposure to actual or threatened death, serious injury, or sexual violence in one (or more) of: direct experience; witnessing in person; learning that the event occurred to a close family member or close friend (violent or accidental); or experiencing repeated or extreme exposure to aversive details (for example first responders). Media-only exposure does not count unless work-related.[1][3]
- Presence of ≥9 of 14 symptoms from any of five categories, beginning or worsening after the trauma:
- Intrusion (memories, dreams, dissociative reactions/flashbacks, psychological or physiological cue distress)
- Negative mood (inability to experience positive emotions)
- Dissociation (altered sense of reality; inability to remember an important aspect of the trauma not due to substances/injury)
- Avoidance (avoiding internal memories/thoughts/feelings; avoiding external reminders)
- Arousal (sleep disturbance, irritable behaviour/angry outbursts, hypervigilance, concentration problems, exaggerated startle)[1][3]
- Duration: disturbance lasts 3 days to 1 month after trauma exposure.
- Clinically significant distress or impairment.
- Not attributable to substances or another medical condition; not better explained by brief psychotic disorder.[1]
If symptoms persist beyond 1 month and meet PTSD criteria, the diagnosis becomes PTSD (with delayed expression if onset of full criteria is later).[1][3]
DSM-IV to DSM-5 change (high-yield trap)
DSM-IV required a dissociative symptom cluster for ASD. That rule improved specificity for some PTSD outcomes but missed many survivors who later developed PTSD without early dissociation. DSM-5 therefore uses a polythetic ≥9/14 rule across categories without mandatory dissociation.[1][2]
ICD-11 contrast (exam delta)
ICD-11 groups disorders specifically associated with stress (PTSD, complex PTSD, prolonged grief, adjustment disorder). Acute stress reaction is conceptualised as a normal transient reaction lasting hours to a few days, not a mental disorder equivalent to DSM ASD. PTSD in ICD-11 is diagnosed when characteristic re-experiencing, avoidance, and sense of current threat persist for several weeks. Do not invent hybrid numbers across systems — name which system you are using.[9]
DSM-5-TR ASD
- Criterion A trauma required
- 3 days–1 month duration
- ≥9 of 14 symptoms any category
- Dissociation optional (not mandatory)
PTSD (DSM)
- Beyond 1 month duration
- Cluster-based criteria
- Same trauma exposure logic
- May follow ASD or arise without prior ASD
ICD-11 acute stress reaction
- Not a mental disorder analogue
- Hours to few days
- Transient expected response
- Different purpose from DSM ASD
Adjustment disorder
- Identifiable stressor
- Need not be Criterion A trauma
- No trauma-cluster requirement
- Different first-line package emphasis
System contrasts above are anchored in DSM-5 ASD review and ICD-11 stress-disorder proposals.[1][9]
Epidemiology and risk factors
Numbers candidates should own
Rates of clinically significant acute stress symptoms vary by trauma type (sexual assault and interpersonal violence often higher than some accidental traumas), sampling frame, and criteria version. ED, trauma surgery, sexual assault services, disaster mental health, military, and ICU are high-volume recognition settings.[1][3][11]
Risk factors for severe acute reactions and later PTSD include prior trauma or psychiatric illness, intense peritraumatic fear or dissociation, perceived life threat, low social support, ongoing secondary stressors (legal process, homelessness, pain), and female sex in some contexts — always formulate intersectionally rather than as destiny.[2][10][11]
Predictive utility pearl. Systematic review evidence shows the ASD diagnosis does not adequately identify the majority of people who eventually develop PTSD. Early Classen work showed acute stress symptoms can predict later PTSD symptoms, but diagnosis-level sensitivity remains imperfect — so monitor high-risk survivors even if they never met full ASD.[2][11][12]
Pathophysiology and maintaining mechanisms
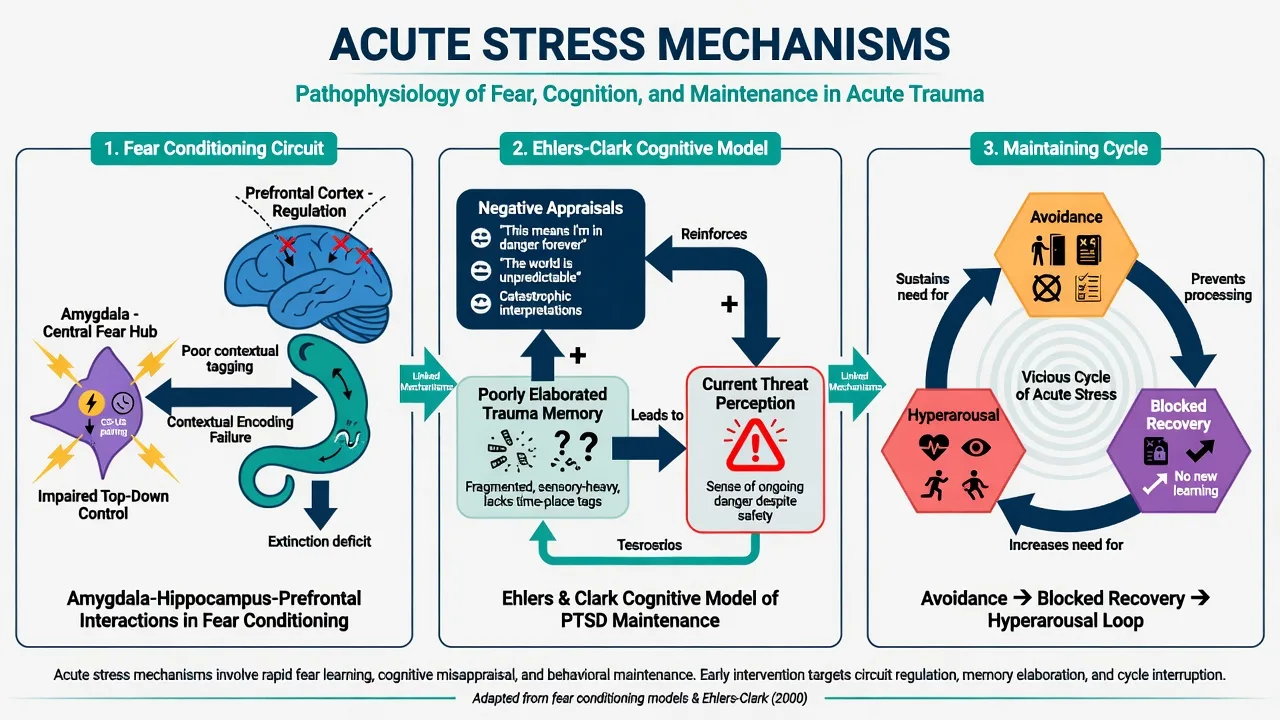
Fear conditioning and extinction. Trauma pairs cues with intense fear; hyper-reactivity of threat circuitry and incomplete extinction learning sustain intrusion and arousal in the acute window.[1][10]
Ehlers–Clark cognitive model. Persistent post-traumatic stress is maintained when trauma is processed in a way that produces a sense of serious current threat, via (1) excessively negative appraisals of the trauma and/or its sequelae, and (2) a disturbance of autobiographical memory characterised by poor elaboration and strong perceptual priming, often with data-driven (sensory) rather than conceptual processing at encoding.[10]
Dissociation. Peritraumatic dissociation may impair integrated encoding of the event and is clinically important when present, but it is not required for DSM-5 ASD.[1][12]
Maintaining behaviours. Cognitive and behavioural avoidance, safety behaviours, rumination, and substance self-medication block natural recovery and are primary therapy targets.[3][10]
Clinical presentation
Presentations track the five symptom domains. Patients may describe replaying the crash, night terrors, emotional numbing, feeling “outside my body,” refusing to drive past the intersection, jumpiness, and insomnia. In sexual assault, shame, contamination fears, and trust collapse often dominate. In first responders, repeated exposure and professional identity complicate help-seeking.[1][3]
MSE language. Quote: “I keep seeing the headlights; I can’t feel happy about anything; the ward feels unreal; I won’t talk about it; I sleep two hours and jump at doors.” Document risk, substances, head injury symptoms, and social safety (perpetrator access).[1][3]
Differential diagnosis
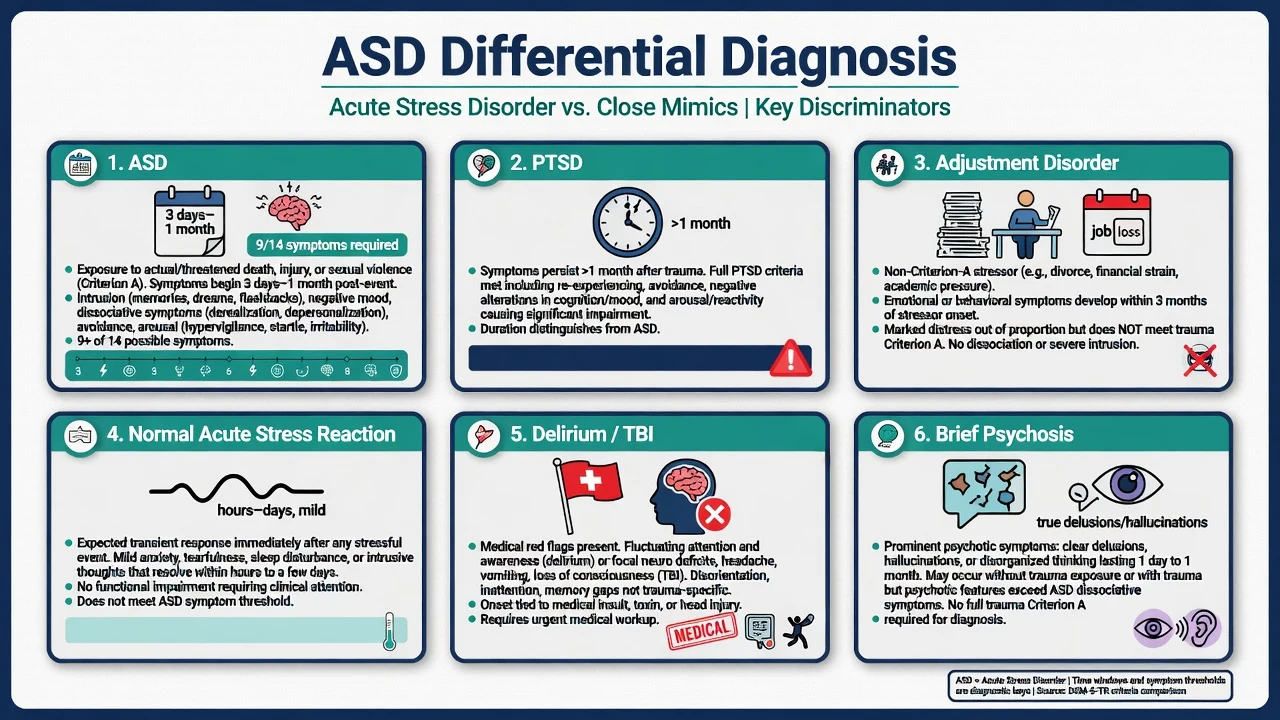
Key discriminators for fellowship answers are as follows.[1][3][9]
- PTSD: same trauma logic but duration greater than 1 month with PTSD cluster criteria.[1][3]
- Normal acute stress reaction: proportionate, time-limited distress without the severity/impairment and symptom count of ASD; still offer support.[9]
- Adjustment disorder: stressor may be non-Criterion-A; lacks the trauma-cluster framework of ASD.[1][9]
- Delirium / TBI / substance effects: fluctuating attention, neurological signs, toxidromes — medical work-up first when indicated.[1]
- Brief psychotic disorder: true delusions/hallucinations not limited to trauma-related flashback phenomena.[1]
- MDD / panic disorder: may co-occur; do not miss independent episode criteria after trauma.[3][11]
Clinical and bedside assessment
Structure: (1) ensure medical stability; (2) map Criterion A carefully; (3) timeline from trauma hour-zero; (4) inventory the 14 symptoms and functional impact; (5) full risk assessment (suicide, homicide, ongoing violence, child protection); (6) substances and prior trauma/psychiatric history; (7) social supports and cultural meaning; (8) practical needs (housing, legal, sexual assault pathway).[1][3]
Avoid coercive detailed retelling in the first hours. Gathering enough history for safety and diagnosis is not the same as forced abreaction.[3][8]
Scales. Research and clinical tools for acute stress symptoms exist; PCL-family measures become more relevant as the PTSD window opens. PHQ-9 tracks comorbid depression. Scales support monitoring; they do not replace Criterion A and clinical judgement.[2][3]
Legal status uses local mental health law when risk requires compulsory care — least restrictive, statute-bound; do not invent jurisdiction-specific section numbers.[3]
Investigations
There is no confirmatory biomarker for ASD. Investigate for differentials and trauma complications: neuroimaging for red-flag head injury, toxicology when substance contribution is plausible, pregnancy test when relevant, and metabolic panels as indicated before medication. Do not order scans to “prove” psychological trauma.[1][3]
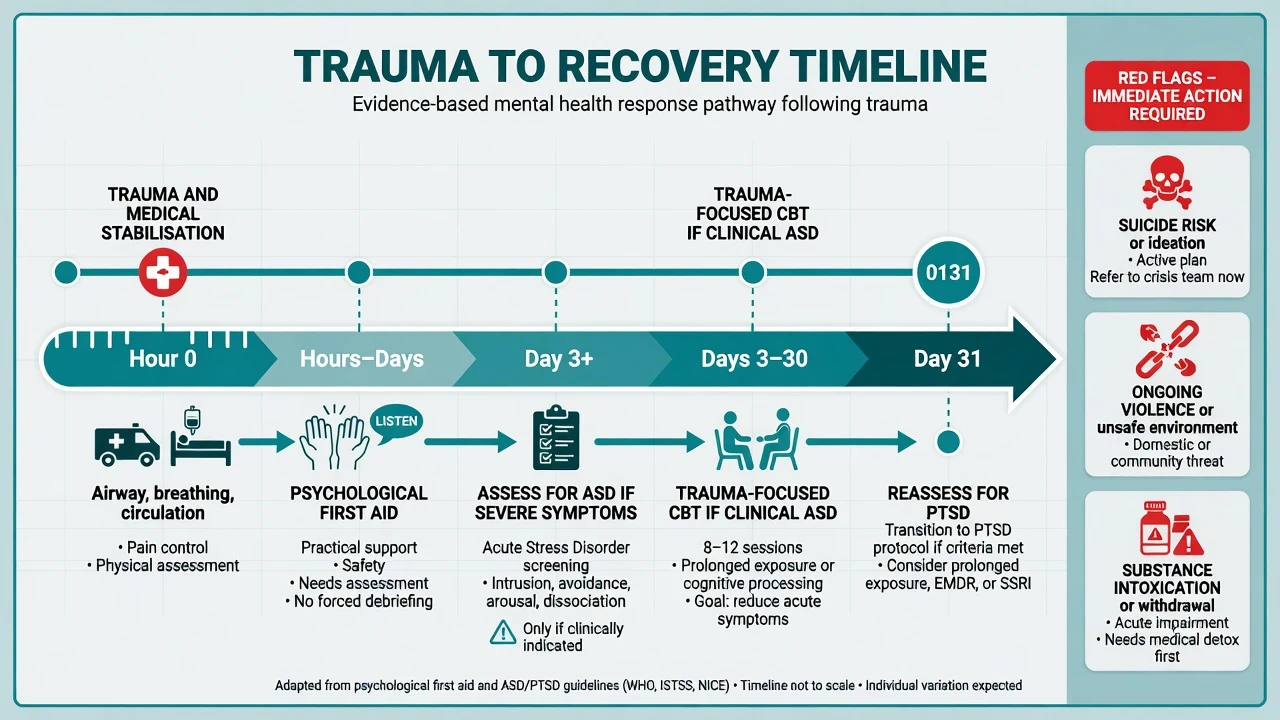
Management — acute safety and early response
Psychological first aid (PFA) principles examiners expect: promote safety, calm, connectedness, self-efficacy, and hope; practical assistance; family contact; accurate information; minimise secondary trauma. PFA is not a multi-hour forced narrative of the event.[3][8]
Psychological debriefing. Cochrane review evidence does not support single-session individual psychological debriefing as a useful treatment to prevent PTSD after traumatic incidents; routine mandatory CISD-style interventions for all exposed people are not indicated and may be unhelpful or harmful in some analyses.[8]
Acute behavioural emergency. Use local rapid tranquillisation pathways only when needed for safety. Short-term sleep support is occasional: for example lorazepam 0.5–1 mg orally as needed for severe acute insomnia/agitation in a medically suitable adult, days not weeks, with an exit plan — not indefinite benzodiazepines for trauma.[3]
Management — definitive care for clinical ASD
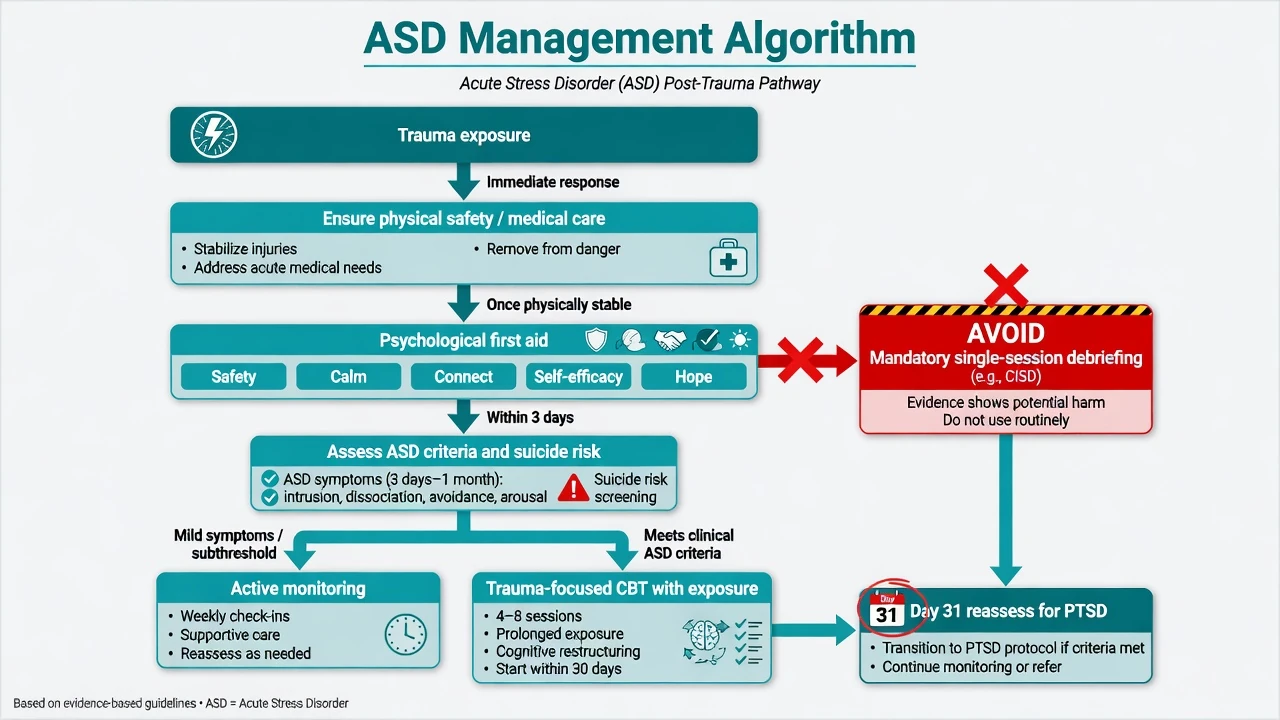
Step 0 — Medical and safeguarding priorities
Treat injuries, pain, infection risk, and intoxication. Activate sexual assault, domestic violence, child protection, and forensic pathways as indicated.[3]
Step 1 — Support, monitoring, and psychoeducation
For mild, improving symptoms with good supports: education about normal recovery trajectories, sleep and substance advice, scheduled review, crisis contacts, and social reconnection. Active monitoring is legitimate; silent discharge is not.[3]
Step 2 — Trauma-focused CBT (first-line for clinical ASD)
Current evidence indicates that trauma-focused cognitive behaviour therapy is the treatment of choice for ASD and reduces risk of chronic PTSD relative to supportive approaches.[3][4][6]
Classic Bryant programme ingredients (name in MEQs): psychoeducation; anxiety management/breathing; cognitive restructuring of maladaptive trauma appraisals; imaginal exposure to the trauma memory; in vivo exposure to avoided safe reminders; relapse prevention — typically brief (about 5–6 sessions) in trial protocols.[4][5][6]
Key trial findings candidates should own are summarised from the Bryant ASD treatment series.[4][5][6][7]
- CBT superior to supportive counselling for ASD and for preventing chronic PTSD.[4][6]
- Exposure-based therapy produced greater reduction in subsequent PTSD symptoms than cognitive restructuring alone in an ASD RCT.[5]
- Benefits of early CBT for ASD can be durable at four-year follow-up.[7]
Stabilise psychosis, severe substance withdrawal, or uncontrolled suicidality before exposure work; individualise pace after sexual assault and in complex trauma histories.[3][5]
Step 3 — Pharmacotherapy (selective)
Medication is not first-line for preventing PTSD in uncomplicated ASD.[3] Treat comorbid major depression or severe anxiety when criteria are met using standard agents — for example sertraline 25–50 mg orally daily, early review in 1–2 weeks for activation and suicidality (especially under 25 years), titrate as tolerated with risk monitoring. Do not claim a unique ASD-licensed preventive dose separate from depression/anxiety practice. Avoid antipsychotics for ordinary acute stress. Avoid long-term benzodiazepines as the primary trauma plan.[3]
Step 4 — Systems and follow-up
Coordinate primary care, psychology, trauma service, occupational health, and legal supports. Explicitly reassess at or after 1 month for PTSD and for depression/substance use disorders.[2][3][11]
ANZ practice emphasises trauma-informed care, cultural safety for Māori and Aboriginal and Torres Strait Islander peoples, sexual assault service pathways, and stepped access to trauma-focused therapy via public and primary mental health programmes. Apply local mental health legislation for compulsory care when risk requires it. Prescribe within PBS/PHARMAC constraints.[3]
Specific subtypes and scenarios
Motor vehicle / industrial accident. Combine medical rehab with graded driving/ situative exposure once safe; screen mTBI.[4][6]
Sexual assault. Immediate medical-forensic care, emergency contraception/STI pathways as indicated, advocacy, paced trauma therapy, and meticulous safety planning regarding the perpetrator.[3]
Domestic violence. Safety planning and multi-agency safeguarding outrank outpatient CBT scheduling if home is unsafe.[3]
Disaster / mass casualty. Population PFA, triage to stepped care, avoid one-size mandatory debriefing of all exposed people.[8]
ICU / medical trauma. Delirium exclusion, family support, meaning-making; ASD can follow awareness experiences or catastrophic illness.[1][11]
ASD with prominent dissociation. Still use TF-CBT framework; ground skills first; do not assume dissociation alone equals poor prognosis or different mandatory medication.[1][5]
ASD after mild TBI. Overlapping cognitive symptoms require joint neurological and psychiatric formulation; do not attribute everything to “stress” or everything to concussion without assessment.[1]
Complications and pitfalls
Classic pitfalls: mandatory CISD; missing TBI/delirium; soft-labelling Criterion A trauma as “adjustment”; starting chronic benzodiazepines; forcing exposure without stabilisation when risk is high; ignoring secondary stressors; media-only Criterion A errors; assuming absence of dissociation excludes ASD (DSM-5).[1][8][9]
Prognosis and disposition
Many acute stress symptoms remit with support and time; a clinically important minority progress to PTSD, depression, anxiety disorders, or substance use problems.[2][11] Early TF-CBT for clinical ASD improves symptom trajectories and reduces later PTSD relative to supportive care in trial populations.[4][5][7]
Disposition ladder: primary care and low-intensity support → specialist trauma-focused psychology/psychiatry for clinical ASD or complexity → crisis/inpatient care when safety requires it. Functional recovery (sleep, work, relationships, legal navigation) is a co-primary outcome with symptom scores.[3]
Special populations
Children and adolescents. Developmental presentations include repetitive play re-enactment, behavioural dysregulation, and school refusal; involve caregivers; adapt exposure carefully.[1][3]
Older adults. Medical comorbidity, bereavement, and cognitive vulnerability complicate assessment; start any medication low and slow.[3]
Perinatal. Birth trauma and assault in pregnancy require obstetric liaison and careful prescribing discussion if medication is considered.[3]
First responders. Repeated Criterion A exposure, organisational culture, and peer support programmes; still avoid mandatory ineffective debriefing models.[8]
Cultural and Indigenous care. FRANZCP cultural safety: interpreters, community supports, avoid pathologising culturally expected mourning after collective trauma while still treating impairing ASD when present.[3][9]
Evidence, guidelines and controversies
Nosology. Bryant and colleagues’ DSM-5 review is the high-yield anchor for criteria evolution and the dissociation debate.[1] Maercker and colleagues frame ICD-11 stress-associated disorders and the non-disorder status of acute stress reaction.[9]
Prediction. Bryant’s systematic review and multi-site work show limited capacity of ASD diagnosis to capture most future PTSD cases; Classen’s earlier work supports the broader principle that acute stress symptoms relate to later PTSD symptoms.[2][11][12]
Treatment. Bryant CBT vs supportive counselling trials (1998–1999), the 2008 exposure vs cognitive restructuring RCT, the four-year follow-up, and the 2018 evidence update form the core exam set: trauma-focused CBT with exposure elements is preferred for clinical ASD.[3][4][5][6][7]
Debriefing. Rose Cochrane review underpins the “no routine single-session debriefing” teaching point.[8]
Mechanism. Ehlers and Clark’s cognitive model supplies formulation language for MEQs and therapy planning.[10]
Controversies: how early to start imaginal exposure; pharmacologic prevention of PTSD (evidence insufficient for routine prophylaxis); residual role of ASD if prediction is imperfect; alignment of ICD and DSM acute constructs.[1][2][3][9]
Exam pearls
ACUTE
Self-test: high-yield traps
- DSM duration? 3 days to 1 month after trauma.
- Symptom rule? ≥9 of 14 from any of five categories.
- Dissociation mandatory? No in DSM-5-TR (was emphasised in DSM-IV).
- If symptoms last past 1 month? Reassess for PTSD.
- Does ASD catch most future PTSD? No — limited sensitivity/PPV.
- Routine single-session debriefing? Not recommended for PTSD prevention.
- First-line for clinical ASD? Trauma-focused CBT with exposure elements.
- ICD-11 acute stress reaction? Transient non-disorder construct — not identical to DSM ASD.[1][2][3][5][8][9]
References
- [1]Bryant RA, Friedman MJ, Spiegel D, Ursano R, Strain J A review of acute stress disorder in DSM-5 Depress Anxiety, 2011.PMID 21910186
- [2]Bryant RA Acute stress disorder as a predictor of posttraumatic stress disorder: a systematic review J Clin Psychiatry, 2011.PMID 21208593
- [3]Bryant RA The Current Evidence for Acute Stress Disorder Curr Psychiatry Rep, 2018.PMID 30315408
- [4]Bryant RA, Sackville T, Dang ST, Moulds M, Guthrie R Treating acute stress disorder: an evaluation of cognitive behavior therapy and supportive counseling techniques Am J Psychiatry, 1999.PMID 10553743
- [5]Bryant RA, Mastrodomenico J, Felmingham KL, Hopwood S, et al. Treatment of acute stress disorder: a randomized controlled trial Arch Gen Psychiatry, 2008.PMID 18519824
- [6]Bryant RA, Harvey AG, Dang ST, Sackville T, Basten C Treatment of acute stress disorder: a comparison of cognitive-behavioral therapy and supportive counseling J Consult Clin Psychol, 1998.PMID 9803707
- [7]Bryant RA, Moulds ML, Nixon RV Cognitive behaviour therapy of acute stress disorder: a four-year follow-up Behav Res Ther, 2003.PMID 12643970
- [8]Rose S, Bisson J, Churchill R, Wessely S Psychological debriefing for preventing post traumatic stress disorder (PTSD) Cochrane Database Syst Rev, 2002.PMID 12076399
- [9]Maercker A, Brewin CR, Bryant RA, Cloitre M, et al. Diagnosis and classification of disorders specifically associated with stress: proposals for ICD-11 World Psychiatry, 2013.PMID 24096776
- [10]Ehlers A, Clark DM A cognitive model of posttraumatic stress disorder Behav Res Ther, 2000.PMID 10761279
- [11]Bryant RA, Creamer M, O'Donnell M, Silove D, McFarlane AC The capacity of acute stress disorder to predict posttraumatic psychiatric disorders J Psychiatr Res, 2012.PMID 22088925
- [12]Classen C, Koopman C, Hales R, Spiegel D Acute stress disorder as a predictor of posttraumatic stress symptoms Am J Psychiatry, 1998.PMID 9585712