Psych · General adult psychiatry — trauma and stressor-related disorders
Adjustment disorders
Also known as Adjustment disorder · Situational depression · Reactive depression (historical misuse) · Stress response syndrome · Transient situational disturbance (historical)
Exam-exhaustive fellowship reference on adjustment disorders — DSM-5-TR and ICD-11 criteria and timing; specifiers; differential vs MDD, PTSD/ASD, normal stress and prolonged grief; suicide-risk nuance; watchful waiting and brief psychological interventions (problem-solving, brief CBT); limited role of antidepressants; occupational and C-L pathways. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Adjustment disorders sit in the trauma- and stressor-related chapter of DSM-5-TR and among disorders specifically associated with stress in ICD-11. They are high-volume in primary care, consultation-liaison, occupational health, and emergency risk assessments — and a classic trap when candidates either over-pathologise normal stress or under-treat risk because the label sounds "mild."[1][4][9][10]
Overview and definition
An adjustment disorder (AD) is a maladaptive psychological response to an identifiable psychosocial stressor (or multiple stressors). The reaction produces distress and/or functional impairment beyond what is expected for the stressor and cultural context, without meeting criteria for another more specific mental disorder that better accounts for the presentation.[1][3][5]
What AD is not. It is not a blood test diagnosis. It is not a euphemism for major depression when full episode criteria are met. It is not PTSD without trauma criteria. It is not a licence to skip suicide risk assessment. Historical terms such as "reactive depression" are imprecise and should not replace operational criteria in exam answers.[2][3][17]
Classification and diagnostic criteria
DSM-5-TR spine (reproduce in viva)
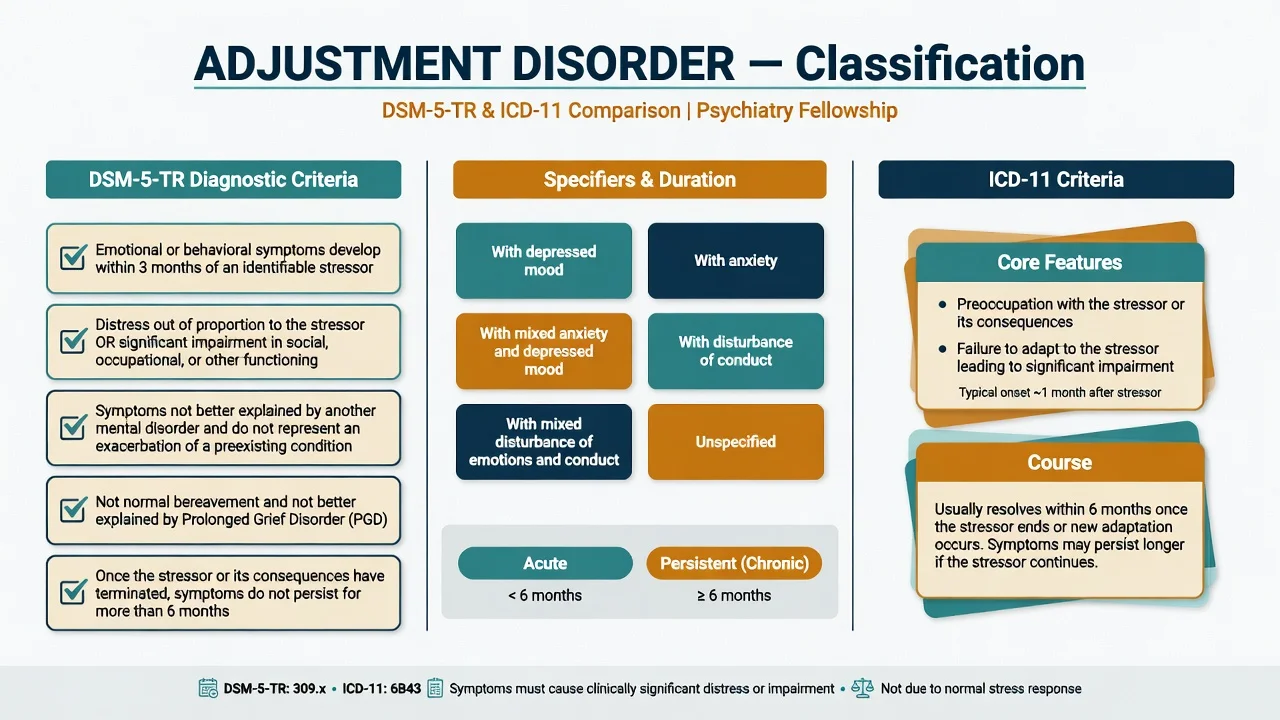
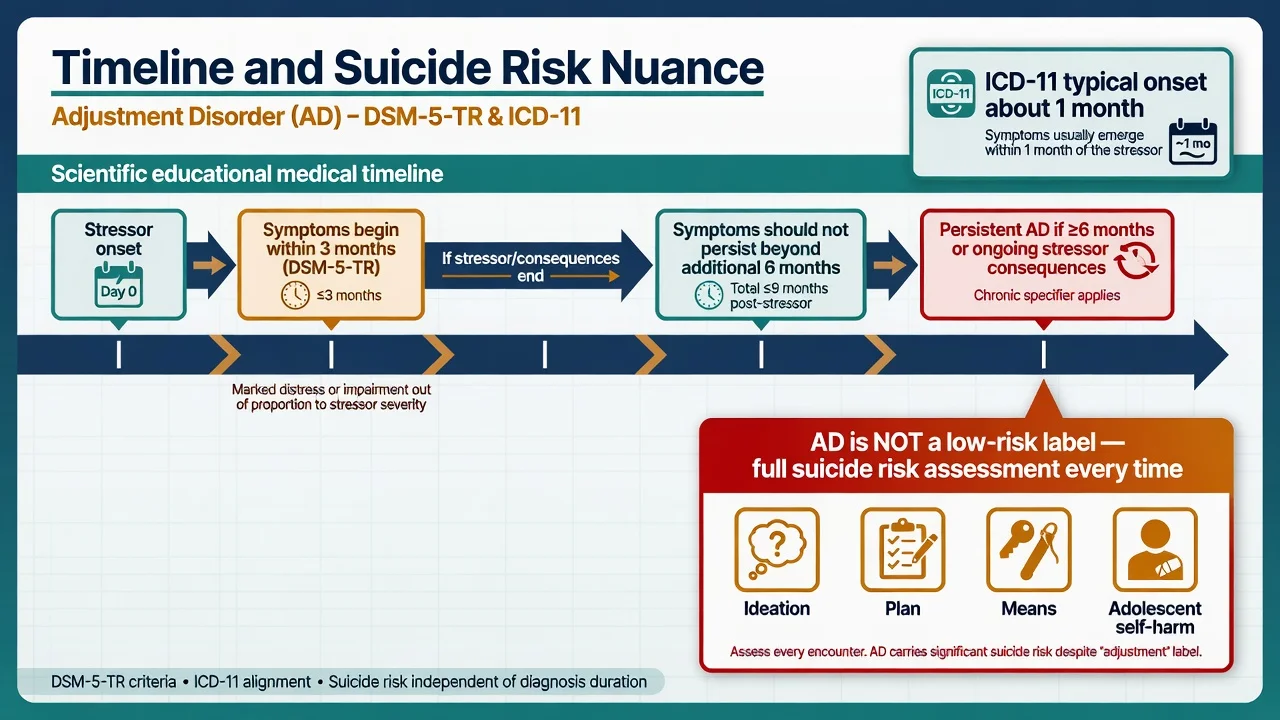
- Development of emotional or behavioural symptoms in response to an identifiable stressor(s) occurring within 3 months of the onset of the stressor(s).
- These symptoms or behaviours are clinically significant, as evidenced by one or both of:
- marked distress that is out of proportion to the severity or intensity of the stressor, taking into account the external context and the cultural factors that might influence symptom severity and presentation; and/or
- significant impairment in social, occupational, or other important areas of functioning.
- The stress-related disturbance does not meet the criteria for another mental disorder and is not merely an exacerbation of a preexisting mental disorder.
- The symptoms do not represent normal bereavement and are not better explained by prolonged grief disorder when that diagnosis applies.
- Once the stressor or its consequences have terminated, the symptoms do not persist for more than an additional 6 months.[1][5][17]
Specifiers (must name)
DSM-5-TR mood and behaviour specifiers are: with depressed mood; with anxiety; with mixed anxiety and depressed mood; with disturbance of conduct; with mixed disturbance of emotions and conduct; and unspecified. Duration course is acute if the disturbance lasts less than 6 months and persistent (chronic) if 6 months or longer (often when the stressor or its consequences are ongoing — chronic illness, contested divorce, persistent unemployment).[1][5]
ICD-11 contrast (exam delta)
ICD-11 emphasises preoccupation with the stressor or its consequences and failure to adapt (for example reduced performance, sleep disturbance, difficulty concentrating, social withdrawal), typically arising within about 1 month of the stressor, with resolution usually within 6 months unless the stressor persists. Maercker and colleagues argued for a more "positive" operationalisation of AD among stress-associated disorders rather than a pure residual wastebasket.[5][16][17]
When an examiner asks for duration thresholds, name which system you are using. Do not invent hybrid numbers.[5][16][17]
DSM-5-TR anchors
- Onset within 3 months of stressor
- Disproportionate distress and/or impairment
- Not another mental disorder
- ≤6 months after stressor/consequences end
ICD-11 anchors
- Preoccupation with stressor/consequences
- Failure to adapt
- Typical onset ~1 month
- Usually ≤6 months unless stressor continues
Specifiers (DSM)
- Depressed / anxiety / mixed
- Conduct / mixed emotions+conduct
- Unspecified
- Acute vs persistent
Conceptual point
- Stressor-linked by definition
- Can follow traumatic or non-traumatic stressors
- Not residual once full MDD/PTSD met
- Cultural context modifies 'disproportion'
Epidemiology and risk factors
Numbers and settings candidates should own
AD is among the more frequently used psychiatric diagnoses in medical settings and occupational health, yet prevalence estimates swing widely with diagnostic thresholds and sampling frames.[3][4][9][10] Risk is higher when vulnerability (prior psychiatric illness, limited supports, high neuroticism, developmental adversity) meets high-intensity or chronic stressors and maladaptive coping.[1][5]
Suicide and self-harm. Multiple clinical series document substantial suicidal ideation and attempts among people diagnosed with AD — including adolescent outpatients and comparative work against major depression. The fellowship pearl is absolute: a mild-sounding ICD/DSM label does not equal low risk.[13][14][15]
Pathophysiology and maintaining mechanisms
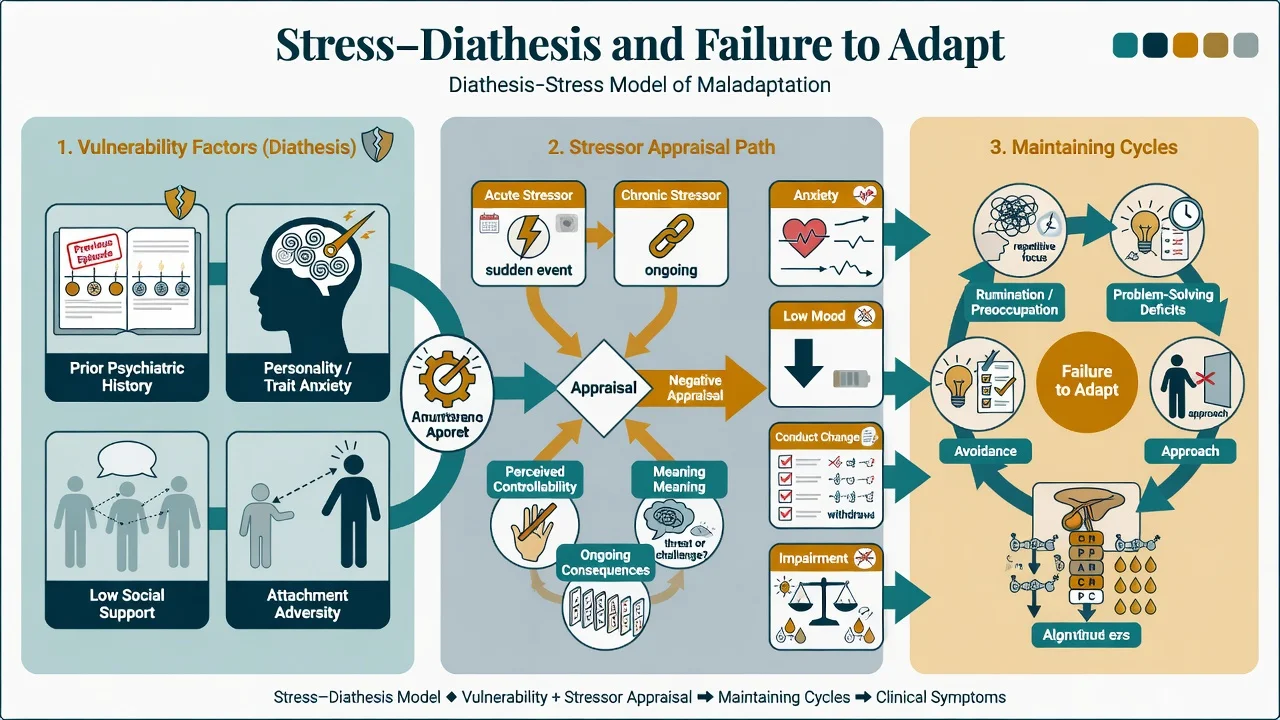
Stress–diathesis framing. Predisposing factors (prior depression/anxiety, personality style, insecure attachment, social isolation) interact with stressor characteristics (severity, controllability, chronicity, interpersonal meaning) and cognitive appraisal. ICD-11’s dual emphasis on preoccupation and failure to adapt maps cleanly onto rumination about the event and blocked problem-solving/behavioural engagement.[1][5][16]
Psychobiology (viva depth, not diagnostic tests). Stress physiology and allostatic load concepts (HPA-axis, sleep disruption, autonomic arousal) provide a bridge to liaison psychiatry presentations after medical illness, but no biomarker diagnoses AD.[10]
Contrast with PTSD models. Fear conditioning, trauma memory fragmentation, and extinction failure dominate PTSD formulation. AD after ordinary (non-Criterion-A) stressors is more about coping failure, loss, role transition, and problem-solving deficits — so first-line packages differ (brief problem-solving/CBT versus trauma-focused therapy).[5][6]
Clinical presentation
Presentations track the specifier. Depressed mood AD: tearfulness, demoralisation, anhedonia that is reactive to the stressor narrative, without full MDD symptom count or autonomy from the stressor. Anxious AD: worry, tension, insomnia focused on the stressor and its consequences rather than free-floating multi-domain GAD worry for six months. Conduct presentations (especially youth): truancy, fighting, rule-breaking temporally linked to the stressor. Mixed pictures are common in primary care.[1][3][9]
MSE language. Quote the link: “Since the redundancy I can’t stop replaying the meeting; I don’t sleep; I cancelled social plans.” Affect often brightens when practical solutions appear. Document risk explicitly. Note substances used to self-medicate stress.[1][9]
Setting variants. C-L: new cancer or cardiac diagnosis with acute demoralisation. Occupational: sickness absence after workplace conflict. Emergency: relationship breakdown with impulsive self-harm. Cultural: somatic complaints after migration or family shame events — formulate culture before forcing Western affect labels.[9][10]
Differential diagnosis
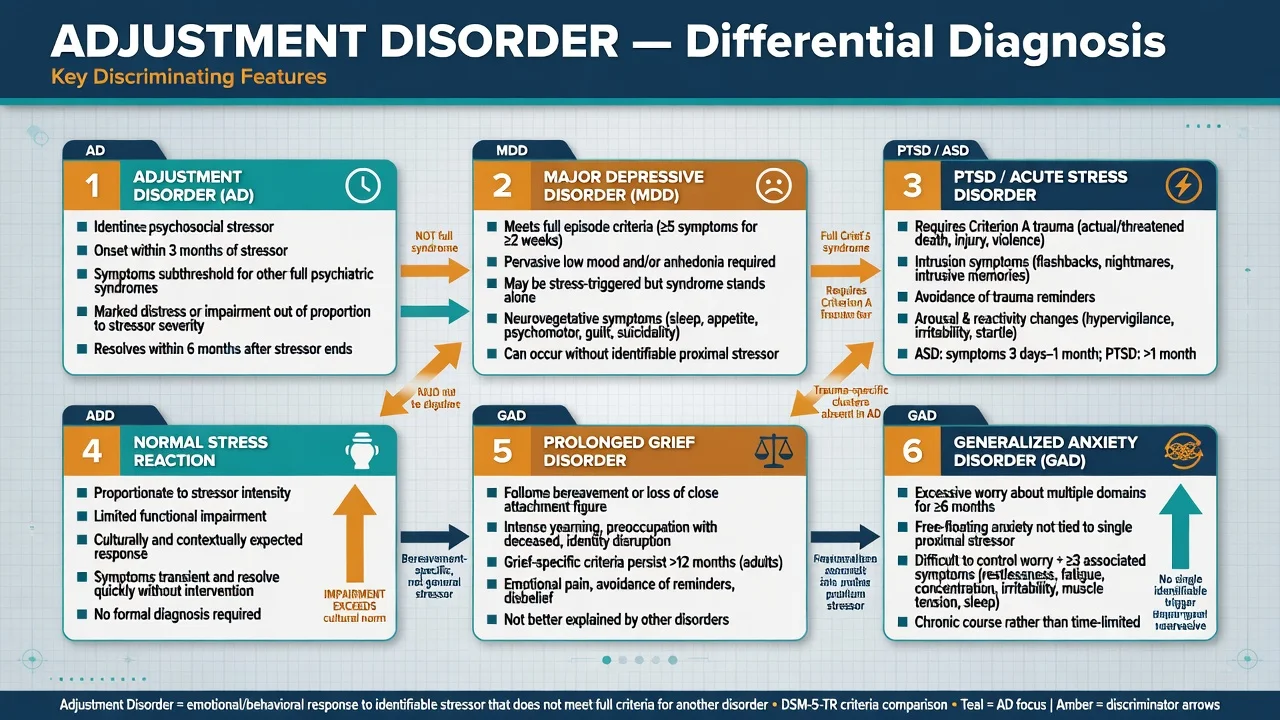
Key discriminators: MDD needs full episode count/severity and pervasiveness (AD keeps subthreshold stressor-linked symptoms); PTSD/ASD need Criterion A trauma plus trauma clusters (AD does not); normal stress is proportionate with limited impairment; prolonged grief disorder is bereavement-specific beyond its duration rules; GAD is free-floating multi-domain worry for at least 6 months; personality disorder crisis is an enduring cross-context pattern; substance/medical causes must be excluded when they explain the picture.[1][2][5][17]
Do not dual-code AD when criteria for MDD or PTSD are fully met — that is an exam fail.[1][5][17]
Clinical and bedside assessment
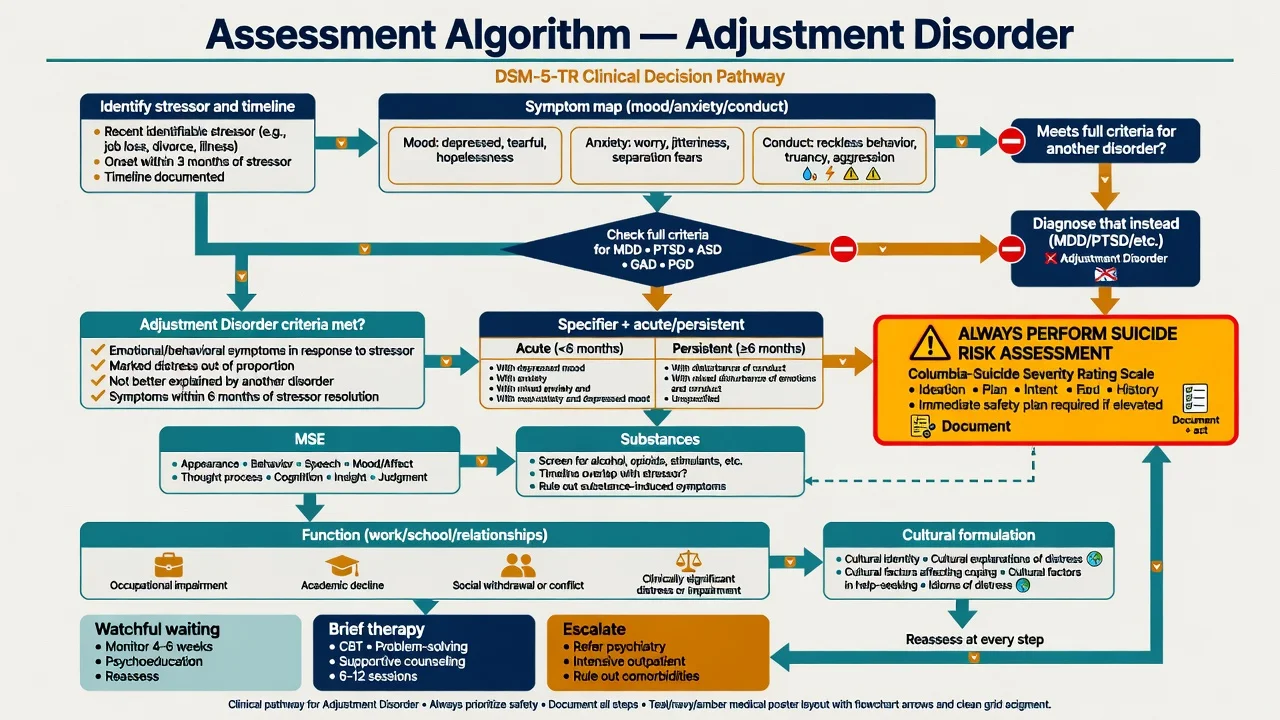
Structure the interview as follows — stressor map (what happened, when, ongoing consequences, controllability, meaning); timeline (symptom onset relative to stressor, DSM within 3 months); symptom inventory (mood, anxiety, conduct, sleep, concentration, substances); full syndrome screen (MDD, bipolar, PTSD/ASD, panic, GAD, psychosis, PGD if bereaved); risk (ideation, intent, plan, means, prior attempts, impulsivity, intoxication, protective factors, safety plan); function (work/school, relationships, self-care); supports and culture; prior episodes and treatment adequacy.[5][9][13]
Scales. PHQ-9 and GAD-7 monitor symptom burden but do not diagnose AD. Research tools such as ADNM-style self-reports exist for stress-response symptoms; know they exist without overselling clinical routine use in every ANZ clinic.[5][9]
Legal status: use local Mental Health Act principles when risk is high — least restrictive care, statute-bound; do not invent section numbers for the wrong jurisdiction.[9]
Investigations
There is no confirmatory lab or scan for AD. Investigate to exclude differentials and to baseline care before medication: TSH when indicated, FBC/U&E/LFT as relevant, pregnancy test, urine drug screen when substance contribution is plausible, ECG if starting an antidepressant in cardiac risk. Neuroimaging only for neurological red flags.[9][10]
Management — acute risk and crisis
Crisis priorities. Ensure physical safety; treat intoxication/withdrawal; address immediate social dangers (violence, homelessness); decide setting (home with plan vs crisis team vs inpatient). Short-term benzodiazepines for severe acute agitation or insomnia are occasional bridges only — name agent, low dose, days not months, and an exit plan (for example lorazepam 0.5–1 mg orally as needed with strict limits in a medically suitable adult). Do not convert life stress into long-term sedative dependence.[3][9]
Management — definitive stepped care
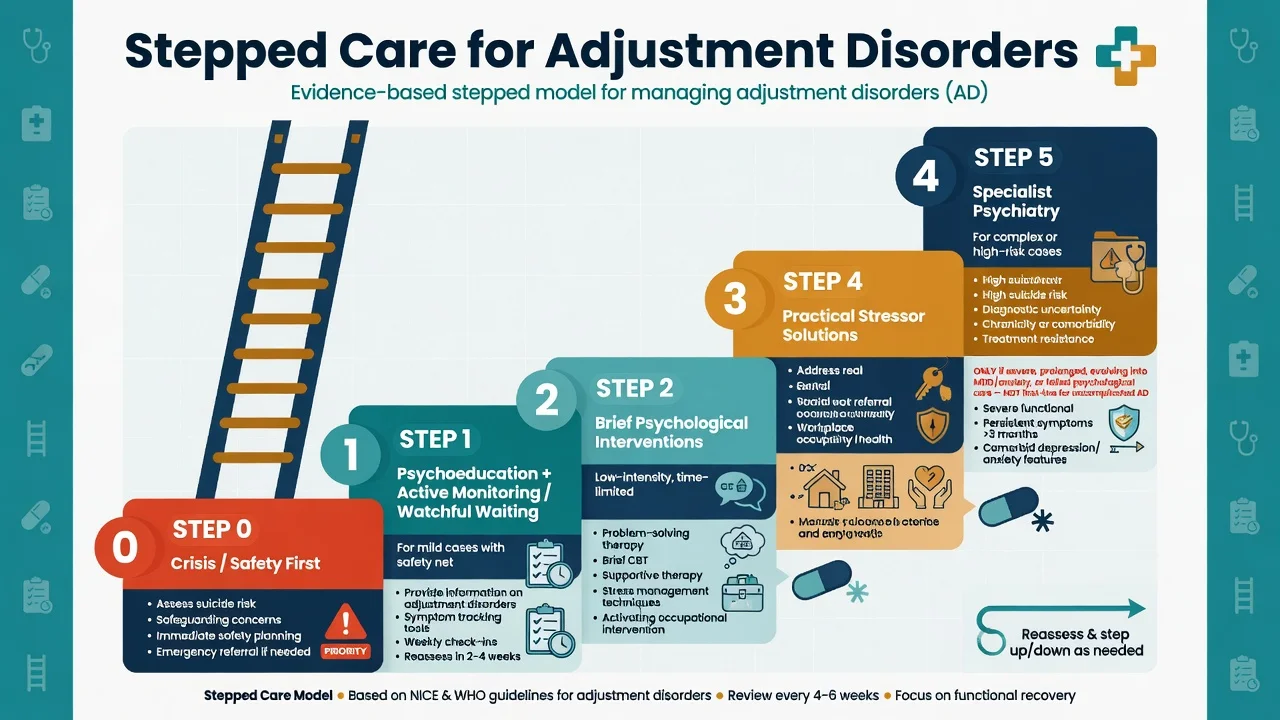
Step 0 — Safety and practical needs
Risk management and safeguarding first. Address housing, domestic violence, child protection, and medical emergencies before pure "talking therapy" scheduling.[9]
Step 1 — Psychoeducation and watchful waiting / active monitoring
For mild presentations with good supports, limited impairment, and low risk, active monitoring is legitimate: explain the stress-response model, normalise without minimising, schedule review (for example 2–4 weeks), provide sleep and substance advice, and give clear crisis contacts. "Watchful waiting" means planned follow-up, not neglect.[3][9][12]
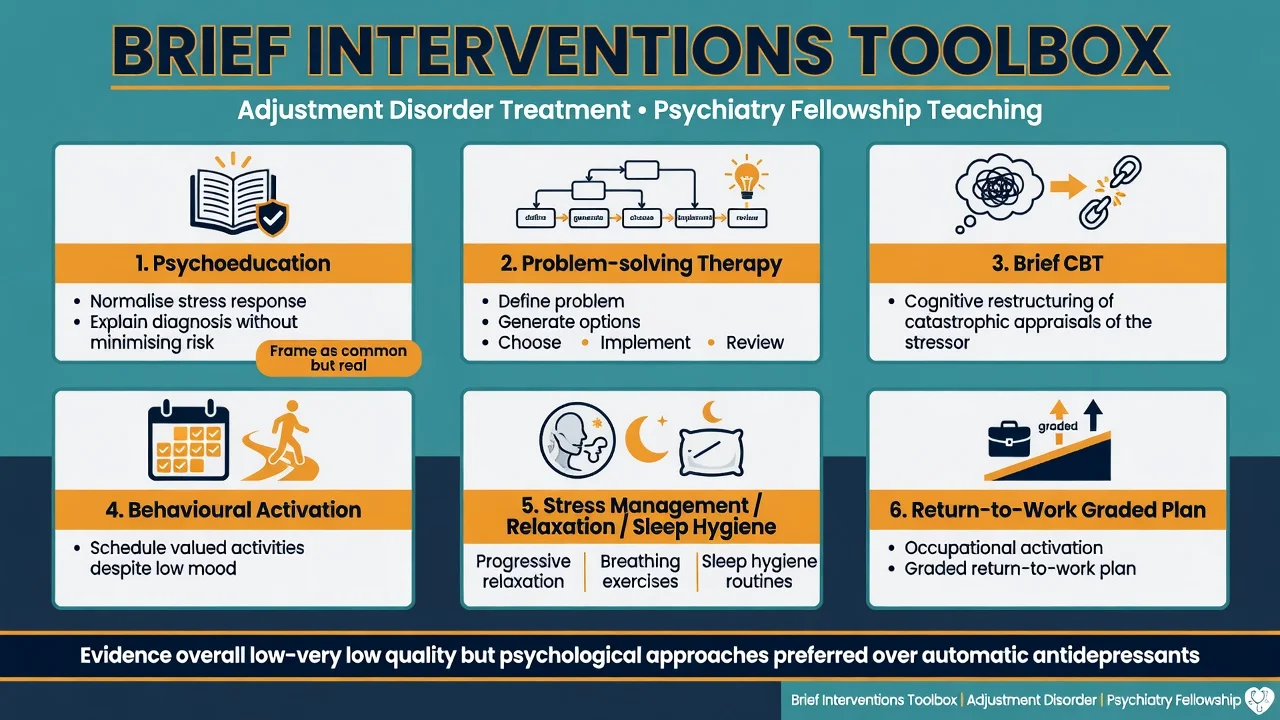
Step 2 — Brief psychological interventions (first-line active treatment)
Evidence quality for AD-specific trials is often low to very low, but synthesised reviews support psychological approaches as the preferred active treatment domain.[6][7]
Problem-solving therapy (PST) ingredients examiners expect: define the problem concretely; brainstorm options; evaluate pros/cons; choose and implement; review outcome; repeat. Fits occupational and primary-care AD particularly well.[6][11][12]
Brief CBT: identify catastrophic appraisals of the stressor and future; cognitive restructuring; behavioural activation; graded re-engagement; sleep routine; reduce avoidance and reassurance traps.[6][7]
Supportive psychotherapy and stress management: validation, containment, skills for arousal reduction — useful when full CBT protocols are inaccessible, but still goal-oriented and time-limited.[3][6]
Occupational activating interventions. Dutch practice guidelines and cluster-RCT work on activating interventions in AD show reduced long-term sickness absence compared with care as usual — know the principle: early activation, graded return, problem-solving focused on work barriers, not indefinite medicalisation of demoralisation.[11][12]
Technology-supported guided self-help and internet interventions are an emerging access option with preliminary meta-analytic support — useful when face-to-face waitlists are long, with the same risk safety-nets.[18]
Step 3 — Practical stressor solutions
Social work, financial counselling, workplace mediation, occupational health, legal advocacy, family meetings. Treating only cognitions while ignoring an ongoing controllable stressor is incomplete care.[9][12]
Step 4 — Pharmacotherapy (selective, not default)
Antidepressants are not first-line for uncomplicated, mild, time-limited AD.[3][6][7][9]
Consider an SSRI/SNRI when symptoms are severe with major functional collapse; course is prolonging toward a full depressive or anxiety syndrome; full MDD or anxiety disorder criteria emerge (then treat that disorder fully); psychological care is inaccessible or insufficient and distress remains high; or sleep/anxiety severity blocks engagement with therapy (still plan psychological care in parallel).[3][6][9]
Exam-level named regimen example (adult): sertraline 25–50 mg orally each morning, early review in 1–2 weeks for activation, akathisia and suicidality (especially under 25 years), titrate toward 50–100 mg if tolerated and still symptomatic, plan several weeks at a therapeutic dose with serial PHQ-9/GAD-7 and risk review. Individualise for age, pregnancy, interactions and local product information. Do not claim a unique AD-licensed dose separate from depression/anxiety practice.[3][9]
Avoid routine long-term benzodiazepines. Avoid antipsychotics for ordinary stress reactions.[3][9]
Step 5 — Specialist escalation
Refer or escalate for high suicide risk, diagnostic uncertainty (possible bipolar, PTSD, personality crisis, organic disease), failed adequate brief interventions, heavy substance comorbidity, or complex C-L/occupational situations.[8][9]
ANZ practice maps onto stepped common-mental-health logic: GP shared care, primary psychology (for example Better Access / local public primary mental health), occupational rehabilitation pathways, and secondary mental health for risk or complexity. Apply cultural safety frameworks for Māori, Aboriginal and Torres Strait Islander peoples rather than stereotype checklists. Prescribe within PBS/PHARMAC constraints and local formulary.[9][12]
Specific subtypes and scenarios
AD with depressed mood after job loss or relationship breakdown. PST plus behavioural activation; monitor for conversion to MDD; work or housing practical plan.[3][11]
AD with anxiety before exams, procedures, or migration. Stress inoculation, brief CBT for threat appraisal, sleep; short-term anxiolytic only with strict limits if severe.[3][6]
Conduct-specifier youth. Family work, school liaison, impulsivity and substance assessment, self-harm risk (Pelkonen-type clinical caution).[13]
C-L after medical diagnosis. Strain’s liaison framing: demoralisation versus MDD, communication with medical teams, meaning-making, avoid both nihilism and forced cheerfulness.[10]
Persistent AD with ongoing stressor consequences. Chronic illness, contested legal cases, prolonged unemployment — treat maintaining factors; do not endlessly relabel without a rehabilitation plan.[5][8]
Military/refugee transitions without full PTSD. Screen carefully for trauma syndromes; if AD, focus on role transition, supports, and problem-solving rather than default PE/EMDR packages designed for PTSD.[5]
Complications and pitfalls
Classic pitfalls: residual wastebasket use of AD; missing PTSD; over-pathologising culturally expected grief; chronic benzodiazepines; ignoring DV/workplace bullying; failing to re-diagnose when symptoms intensify into MDD; indefinite sick leave without activation plan.[1][8][11][17]
Prognosis and disposition
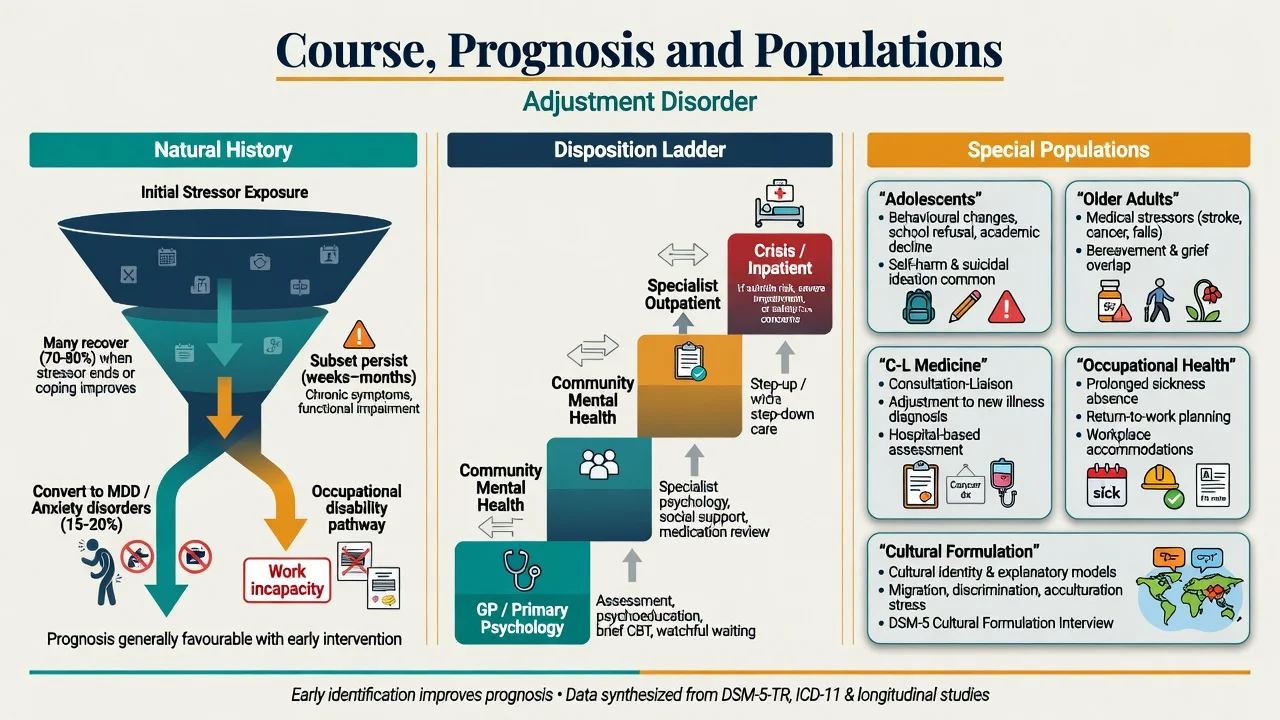
Systematic review data show heterogeneous outcomes: many adults improve, but a clinically important minority have persistent symptoms, recurrent stress reactions, or progression toward other disorders and disability — prognosis is not uniformly benign.[8] Occupational outcomes improve with activating, guideline-based approaches versus passive care.[11][12]
Disposition ladder: GP and primary psychology → secondary community mental health for complexity/risk → crisis/inpatient care when safety requires it. Functional recovery (work, school, relationships) is a co-primary outcome with symptom scores.[8][9]
Special populations
Children and adolescents. Irritability, school refusal, and behavioural change may dominate; family and school are part of the treatment system; self-harm risk can be high even when the formal diagnosis is AD.[13]
Older adults. Medical illness and grief are common stressors; exclude delirium and depression; start any medication low and slow; prioritise social supports.[8][9]
Perinatal. Role transition and birth-related stress are common; still apply full perinatal mood/anxiety criteria when met — do not hide postpartum depression behind an AD label.[1][9]
Cultural and Indigenous care. FRANZCP cultural safety expectations: interpreter, family inclusion as appropriate, avoid pathologising culturally expected mourning or spiritual practices.[9]
Intellectual disability. Environmental change (carer loss, move) can present as behavioural decompensation — formulate stressor link carefully and simplify interventions.[9]
Evidence, guidelines and controversies
Core synthesis papers. Bachem and Casey argue AD’s time has come as a legitimate stress-response diagnosis rather than a pure residual category.[1] Casey’s epidemiology/treatment and later updates, Carta’s overview, and O’Donnell’s developments paper are high-yield orientation sources.[2][3][4][5] Casey and Doherty’s British Journal of Psychiatry piece frames ICD-11/DSM implications examiners still probe.[17]
Treatment evidence. Domhardt and Baumeister review psychotherapy state of play; Cowansage and colleagues’ systematic review/meta-analysis of RCTs updates effect estimates — expect the examiner phrase “limited but directionally supportive evidence for psychological treatments.”[6][7] Fernández-Buendía and colleagues summarise technology-supported treatments.[18]
Occupational landmark. van der Klink activating intervention cluster RCT and Dutch practice guidelines remain classic named sources for work-focused AD care.[11][12]
Risk literature. Pelkonen (adolescent outpatients), Kryzhanovskaya, and Polyakova (attempt characteristics versus major depression) support the suicide-risk teaching point.[13][14][15]
Nosology. Maercker ICD-11 stress-disorder proposals operationalise preoccupation and failure to adapt.[16] Controversies continue: residual versus positive diagnosis; antidepressant utility in pure AD; how aggressively to intervene early versus monitor; boundary with demoralisation in medical illness.[1][7][10][17]
Exam pearls
ADJUST
Self-test: high-yield traps
- DSM onset window? Within 3 months of stressor.
- Post-stressor duration rule? Symptoms do not persist more than 6 additional months after stressor/consequences end.
- ICD-11 cores? Preoccupation + failure to adapt.
- If full MDD criteria met? Diagnose MDD, not AD.
- First-line active treatment? Brief psychological interventions (PST/brief CBT), not automatic SSRI.
- Watchful waiting for? Mild, low-risk, well-supported cases with planned review.
- Suicide pearl? AD samples show substantial suicidality — assess fully.
- Occupational pearl? Activating interventions reduce long-term sickness absence.[5][6][11][13][16]
References
- [1]Bachem R, Casey P Adjustment disorder: A diagnosis whose time has come J Affect Disord, 2018.PMID 29107817
- [2]Casey P Adjustment disorder: new developments Curr Psychiatry Rep, 2014.PMID 24748555
- [3]Casey P Adjustment disorder: epidemiology, diagnosis and treatment CNS Drugs, 2009.PMID 19845414
- [4]Carta MG, Balestrieri M, Murru A, Hardoy MC Adjustment Disorder: epidemiology, diagnosis and treatment Clin Pract Epidemiol Ment Health, 2009.PMID 19558652
- [5]O'Donnell ML, Agathos JA, Metcalf O, Gibson K, et al. Adjustment Disorder: Current Developments and Future Directions Int J Environ Res Public Health, 2019.PMID 31315203
- [6]Domhardt M, Baumeister H Psychotherapy of adjustment disorders: Current state and future directions World J Biol Psychiatry, 2018.PMID 30204563
- [7]Cowansage KP, Milligan T, Morgan MA, et al. Treatments for adjustment disorder: A systematic review and meta-analysis of randomized controlled trials Psychiatry Res, 2025.PMID 41005147
- [8]Morgan MA, Kelber MS, Bellanti DM, et al. Outcomes and prognosis of adjustment disorder in adults: A systematic review J Psychiatr Res, 2022.PMID 36347110
- [9]Geer K Adjustment Disorder: Diagnosis and Treatment in Primary Care Prim Care, 2023.PMID 36822730
- [10]Strain JJ The Adjustment Disorder Diagnosis, Its Importance to Liaison Psychiatry, and its Psychobiology Int J Environ Res Public Health, 2019.PMID 31766628
- [11]van der Klink JJ, Blonk RW, Schene AH, van Dijk FJ Reducing long term sickness absence by an activating intervention in adjustment disorders: a cluster randomised controlled design Occup Environ Med, 2003.PMID 12771395
- [12]van der Klink JJ, van Dijk FJ Dutch practice guidelines for managing adjustment disorders in occupational and primary health care Scand J Work Environ Health, 2003.PMID 14712856
- [13]Pelkonen M, Marttunen M, Henriksson M, Lönnqvist J Suicidality in adjustment disorder--clinical characteristics of adolescent outpatients Eur Child Adolesc Psychiatry, 2005.PMID 15959663
- [14]Kryzhanovskaya L, Canterbury R Suicidal behavior in patients with adjustment disorders Crisis, 2001.PMID 11831599
- [15]Polyakova I, Knobler HY, Ambrumova A, Lerner V Characteristics of suicidal attempts in major depression versus adjustment reactions J Affect Disord, 1998.PMID 9476756
- [16]Maercker A, Brewin CR, Bryant RA, Cloitre M, et al. Diagnosis and classification of disorders specifically associated with stress: proposals for ICD-11 World Psychiatry, 2013.PMID 24096776
- [17]Casey P, Doherty A Adjustment disorder: implications for ICD-11 and DSM-5 Br J Psychiatry, 2012.PMID 22859575
- [18]Fernández-Buendía S, Miguel C, Dumarkaite A, Kazlauskas E, et al. Technology-supported treatments for adjustment disorder: A systematic review and preliminary meta-analysis J Affect Disord, 2024.PMID 37992766