Psych · General adult psychiatry — personality disorders
Antisocial personality disorder
Also known as ASPD · Dissocial personality disorder · Antisocial PD · Cluster B personality disorder · Psychopathy (related construct)
Exam-exhaustive fellowship reference on antisocial personality disorder — DSM-5-TR and ICD-11 nosology; careful ASPD versus psychopathy distinction; epidemiology and substance comorbidity; developmental conduct pathway and callous-unemotional traits; differentials versus BPD and NPD; violence risk formulation; forensic interface; NICE and Cochrane treatment limits; emerging mentalization evidence. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Antisocial personality disorder (ASPD) is a high-yield general adult and forensic interface topic across FRANZCP, MRCPsych, ABPN and MD/DNB. Examiners test operational criteria (especially the conduct disorder requirement), the careful ASPD–psychopathy distinction, substance comorbidity, violence risk without fatalism, and honest treatment limits.[2][3][8]
Overview and definition
ASPD is a clinical personality disorder diagnosis describing a long-standing pattern of exploiting, harming, or disregarding the rights of others, with failure of prosocial responsibility across work, relationships and lawfulness. It is not a synonym for criminality, and it is not interchangeable with psychopathy as measured by instruments such as the PCL-R.[3][8][9]
DSM-5-TR categorical diagnosis (exam-critical). After general personality disorder criteria are met, ASPD requires a pervasive pattern of disregard for and violation of the rights of others, occurring since age 15 years, as indicated by three or more of: failure to conform to lawful norms (repeated acts that are grounds for arrest); deceitfulness (lying, aliases, conning); impulsivity or failure to plan ahead; irritability and aggressiveness (repeated fights or assaults); reckless disregard for safety of self or others; consistent irresponsibility (work or financial obligations); lack of remorse (indifference to or rationalising having hurt, mistreated, or stolen from another). The individual must be at least 18 years old, there must be evidence of conduct disorder with onset before age 15 years, and the occurrence of antisocial behaviour must not be exclusively during the course of schizophrenia or bipolar disorder.[3]
ICD-11 framing. Personality disorder is graded by severity (mild, moderate, severe) with trait domain qualifiers. Features historically captured as ICD-10 dissocial personality disorder map largely onto high dissociality/antagonism (and often disinhibition) within a severity rating. Fellowship answers should name which manual is in use and that ICD-11 is dimensional-severity first, whereas classic MCQ stems still use DSM's ≥3/7 plus CD rule.[3][5]
Classification and nosology
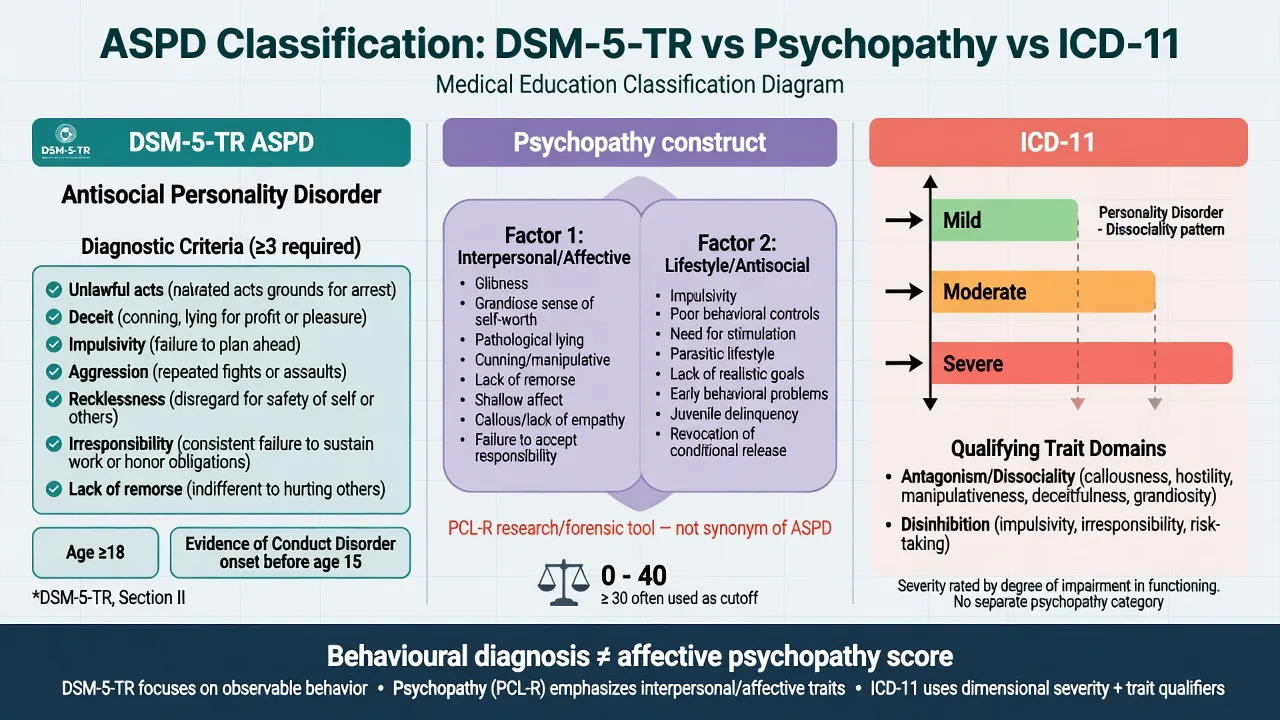
DSM-5-TR ASPD
- ≥3 of 7 behavioural criteria since age 15
- Age ≥18 required
- Conduct disorder onset before 15 is mandatory
- Exclude if antisocial acts only during schizophrenia/bipolar episodes
Psychopathy construct
- Interpersonal/affective traits (Factor 1) plus lifestyle/antisocial (Factor 2)
- PCL-R / PCL:SV are specialised tools, not routine clinic screens
- Not all ASPD meets high psychopathy thresholds
- Not all high-psychopathy people are labelled ASPD in every system
ICD-11 PD
- Severity first: mild / moderate / severe
- Trait domains (e.g. dissociality/antagonism, disinhibition)
- Legacy ICD-10 dissocial PD concept still appears in older stems
- Dimensional language helps formulation stations
AMPD (DSM Section III)
- Criterion A: self and interpersonal impairment
- Criterion B traits: typically high antagonism + disinhibition
- Useful for formulation even if categorical diagnosis used
- Avoid trait word-salad without impairment
ASPD versus psychopathy — the viva trap
Psychopathy is a clinical-research construct emphasising affective and interpersonal features (shallow affect, lack of empathy/remorse, grandiosity, pathological lying, manipulativeness) combined with impulsive-antisocial lifestyle features. Hare's PCL tradition operationalises this for research and forensic assessment; it is not a general adult "confirm ASPD" blood test equivalent.[8][9]
High-yield discriminators for exams:[2][8]
- Many people meeting DSM ASPD have prominent externalising behaviour with variable affective-interpersonal depth; a smaller subset shows classic high Factor-1 psychopathic traits.[2][8]
- Psychopathy scores associate with poorer engagement and higher reconviction risk in many forensic samples — probabilistic, never a reason to withhold medical care for comorbidity.[8][17]
- Do not tell an examiner that "ASPD means psychopath" or that every prisoner has ASPD.[8]
Epidemiology and risk factors
Headline epidemiology candidates must own
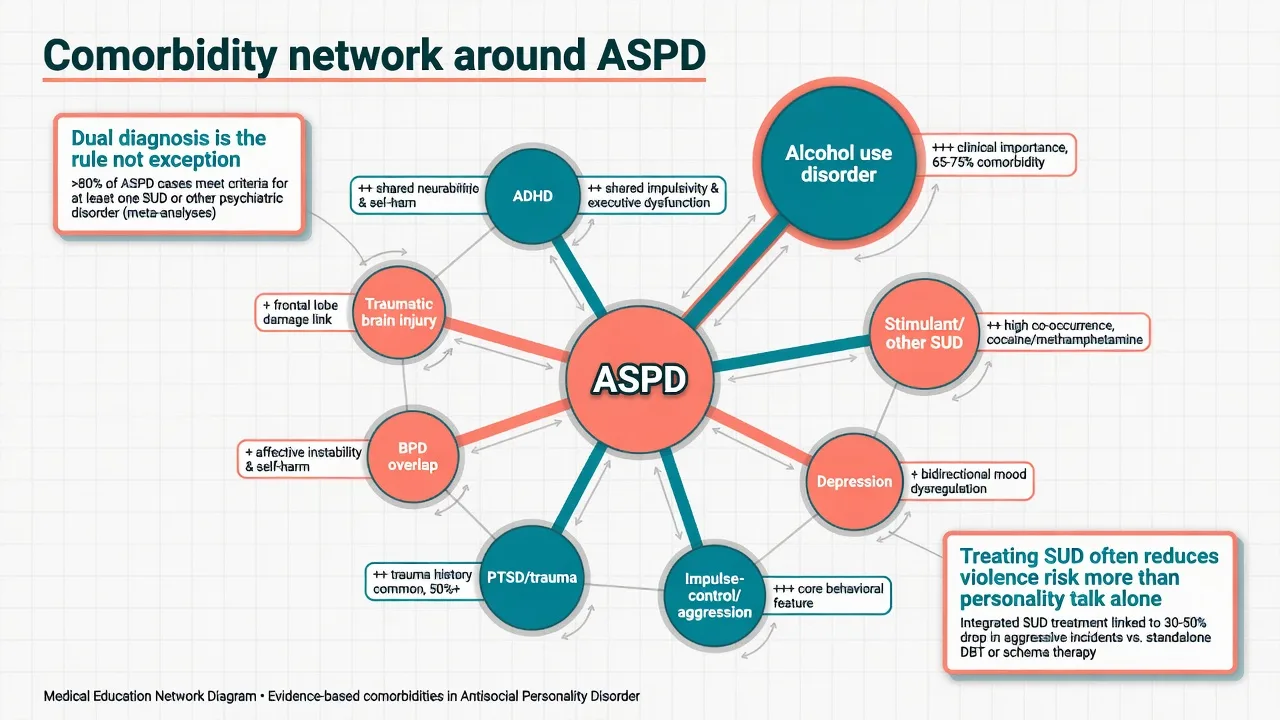
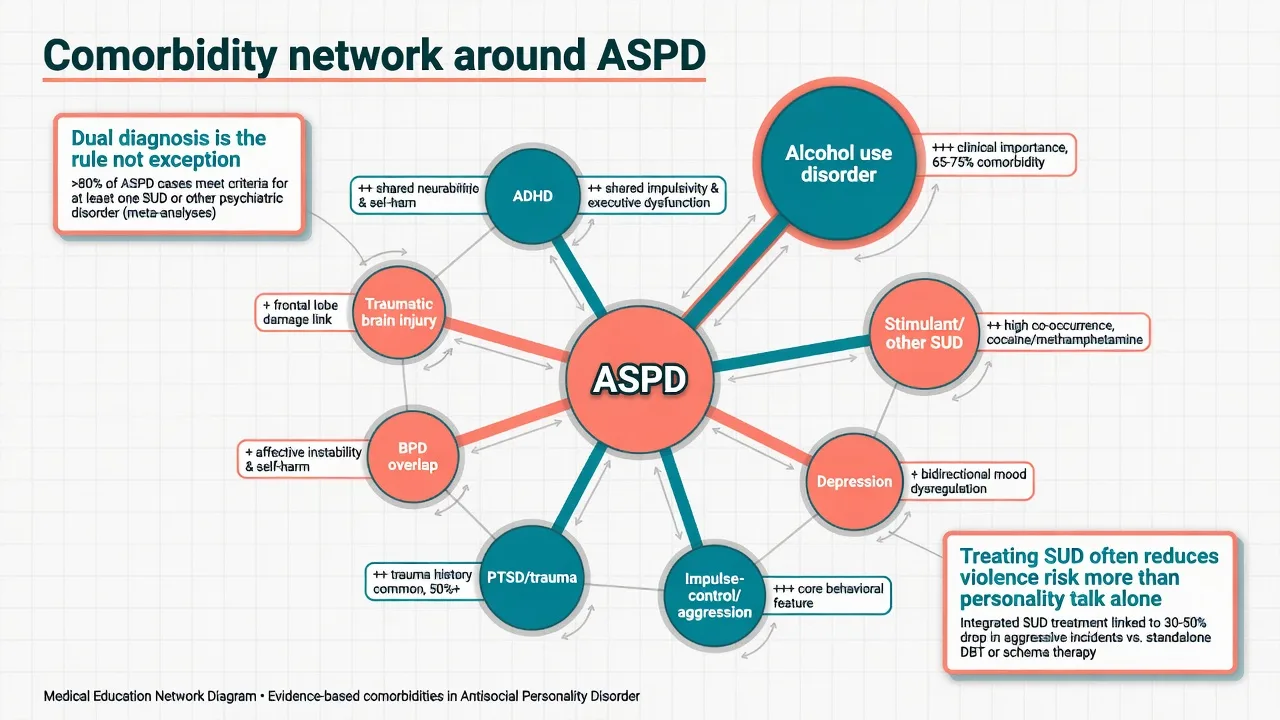
Large epidemiologic work, including NESARC-III analyses of antisocial behavioural syndromes, documents substantial population burden, strong male predominance for many antisocial syndromes, and dense comorbidity with substance use and other externalising problems.[1][2] British household survey work likewise shows personality disorder is common enough to matter for public mental health planning, with antisocial patterns concentrated among younger men and linked to service and justice contact.[15]
Aetiological and risk factors. Childhood conduct disorder is the developmental gateway for DSM ASPD.[10][20] Additional risk includes callous-unemotional / limited prosocial emotion traits, childhood maltreatment and adversity, parental antisocial behaviour, peer delinquency, socioeconomic disadvantage, and early substance use.[2][10] Twin data show substantial genetic contribution to personality disorder risk structure, with ASPD-relevant externalising liability shared across related traits — environment still shapes expression.[14]
Pathophysiology and mechanisms
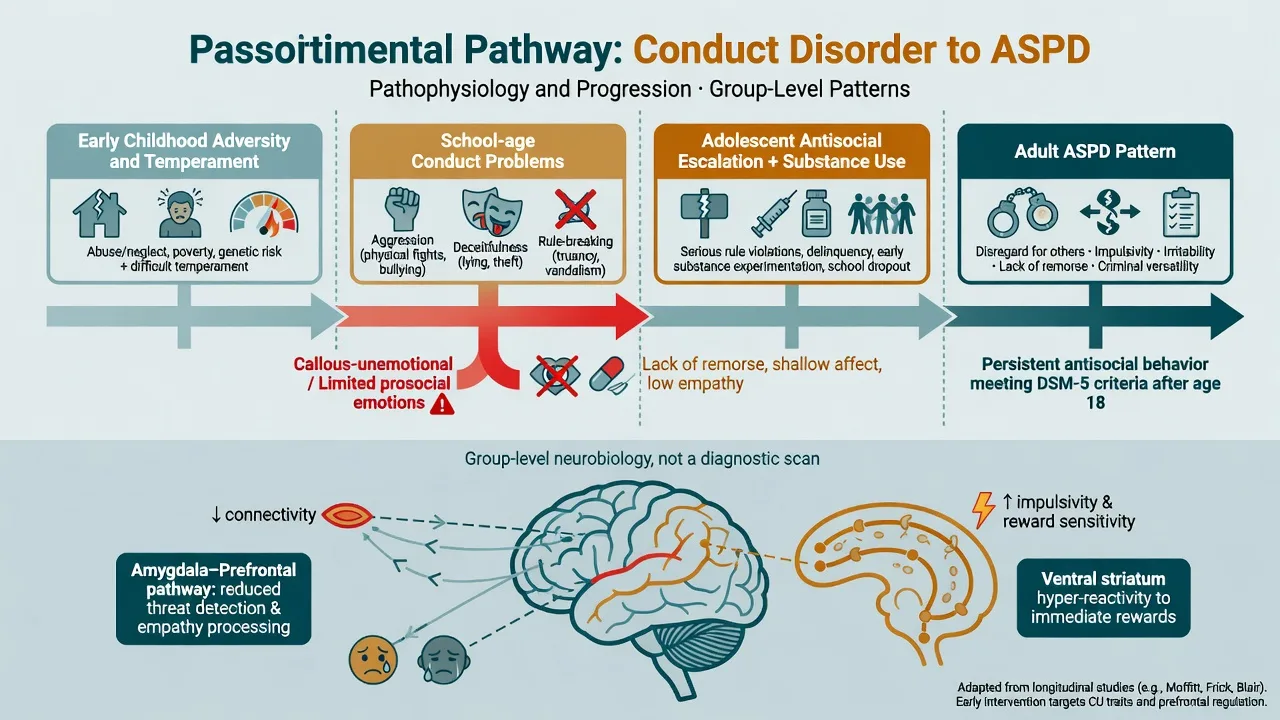
Developmental model. Classic longitudinal teaching (Robins and subsequent developmental psychopathology) is that many antisocial adults were antisocial children; not all conduct-disordered youth become ASPD adults, but adult ASPD without earlier conduct problems fails the DSM rule and should make you rethink the label.[4][20] A clinically important subgroup shows callous-unemotional traits (limited prosocial emotions specifier language in youth nosology): reduced empathy and guilt, shallow affect, and more instrumental aggression trajectories.[10][11]
Neurobiology (keep humble). Reviews implicate atypical processing in circuits supporting empathy, threat conditioning, decision-making and reward/impulsivity (amygdala–prefrontal networks and related systems) at the group level in youth with psychopathic traits and in adult antisocial populations.[11][19] Imaging and biomarkers do not diagnose ASPD in an individual patient and must never replace history, collateral and risk formulation.[8][19]
Learning and social mechanisms. Coercive family processes, modelling of aggression, reinforcement of deceit, and criminogenic peer networks maintain antisocial repertoires alongside temperament.[2][3]
Clinical presentation
Core adult presentation combines recurrent unlawful or exploitative behaviour, deceit, impulsivity, irritability/aggression, recklessness, irresponsibility, and remorseless rationalisation. On MSE, listen for minimisation, externalisation of blame, charm that collapses under confrontation, restricted affective response to others' distress, and secondary agendas (bail, benefits, access to drugs).[3][4]
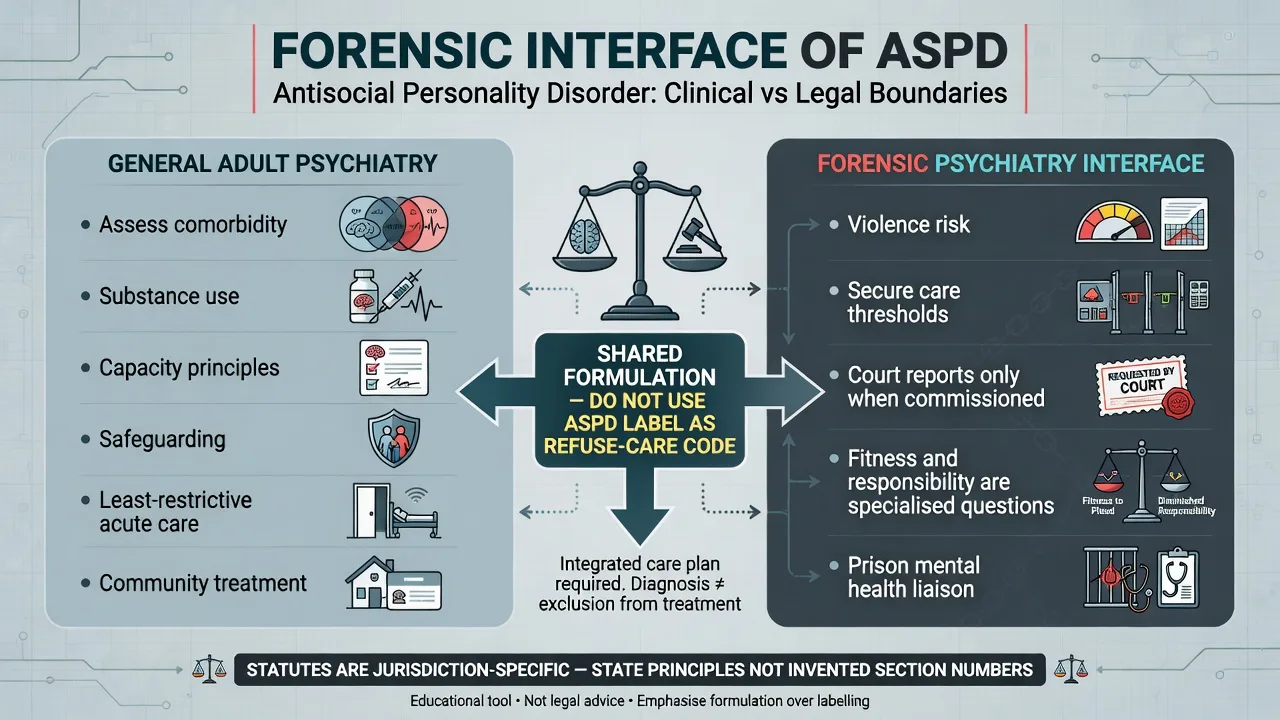
Settings examiners use. Emergency and trauma services see assault injuries, intoxication, threats and partner violence; community psychiatry sees dual-diagnosis referrals, ADHD reassessment requests and crises driven by legal pressure; forensic and prison settings show high co-occurrence of mental illness, substance use and ASPD — dual and triple comorbidity is expected, not exotic.[3][17]
"Successful" antisociality. White-collar exploitation, serial relationship harm and workplace predation can meet criteria without street crime; diagnosis rests on pattern and history, not socioeconomic stereotype.[3]
Differential diagnosis
vs BPD
- BPD: abandonment fear, identity disturbance, emptiness
- Self-harm often for affect regulation
- Idealisation/devaluation cycles
- ASPD: rights violation, conduct history, remorseless exploitation
vs NPD
- NPD: grandiosity, admiration need, envy
- May lack early CD and repeated illegal acts
- Entitlement overlaps with ASPD antagonism
- Formulate which pattern drives impairment
vs SUD alone
- Antisocial acts confined to intoxication/acquisition periods argue against standalone ASPD
- Dual diagnosis is extremely common
- Collateral timeline is decisive
- Treat SUD regardless of PD label
vs organic / other
- Late-onset change → TBI, FTD, epilepsy, endocrine
- Mania: episodic elevated mood/energy/sleep need
- Psychosis: delusions drive acts
- IED: discrete aggressive outbursts without full PD pattern
Also keep ADHD (childhood neurodevelopmental pattern; comorbidity common), autism spectrum social-rule differences without callous exploitation, and intermittent explosive disorder on the board. The exam skill is discriminators plus comorbidity, not exclusive single labels.[2][3][10]
Clinical and bedside assessment
Structure the interview: developmental and school history; conduct symptoms before 15; legal chronology; violence typology (reactive versus instrumental); intimate partner and child safeguarding; substance use (amount, route, withdrawal); employment and relationships; trauma; prior treatments; current motivation (intrinsic versus legal leverage); collateral from family, probation, records.[3][17]
Mental State Examination. Affective range and response to others' distress; thought content (grievances, entitlement, threats); insight; judgement; deceit signals; alliance motives. Document capacity as decision-specific. Assess staff safety and interview environment.[3][8]
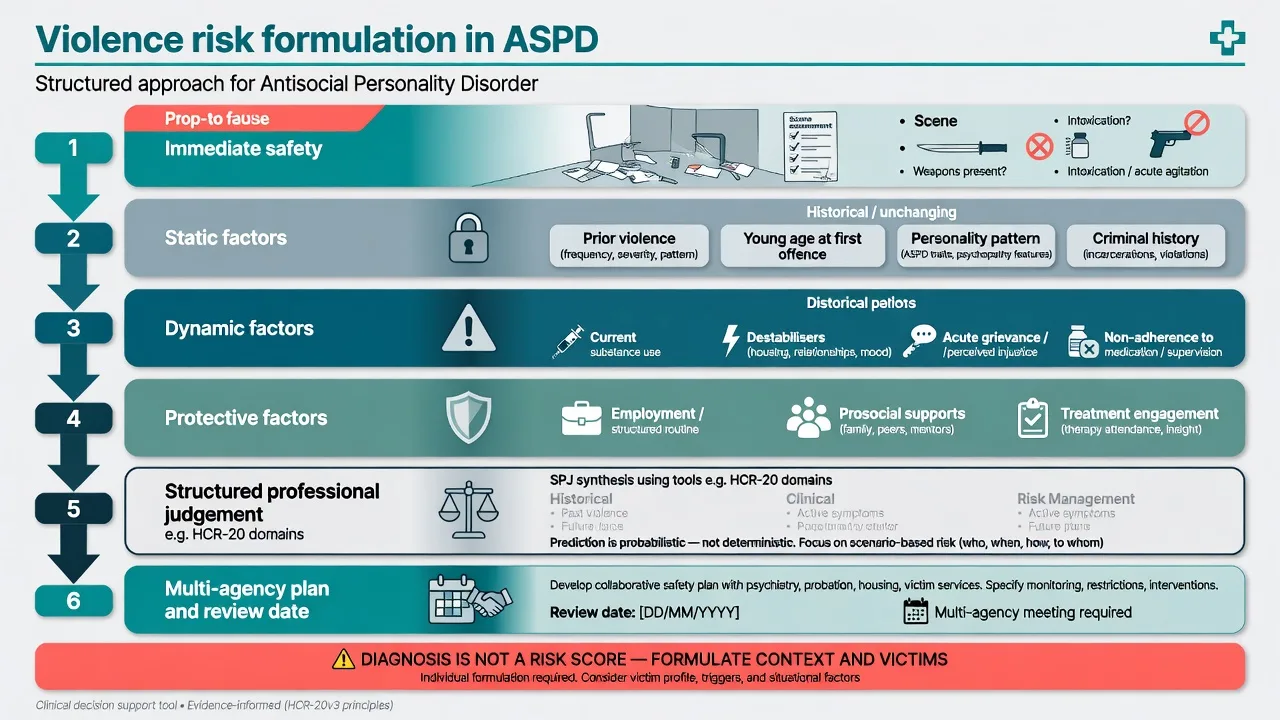
Violence risk is formulation, not a label. Integrate static factors (prior violence, age at first violence, criminal history, personality pattern) with dynamic factors (current substance use, weapon access, destabilisers, acute grievance, treatment non-adherence, victim access) and protective factors (employment, prosocial supports, engagement). Structured professional judgement tools (for example HCR-20 domains in forensic settings) and psychopathy measures may inform specialist assessment; meta-analytic evidence shows risk instruments have modest predictive accuracy at group level and do not replace clinical judgement or multi-agency planning.[16]
Investigations
ASPD has no laboratory gold standard. Investigate to manage substances, exclude mimics, and prepare for any medication: urine drug screen when relevant; FBC, U&E, LFT, glucose/lipids as baseline; pregnancy test when applicable; cognitive screen and neuroimaging or EEG when late-onset change, focal neurology, seizures or significant TBI history fire. Screen systematically for mood disorders, psychosis, ADHD, PTSD and substance use disorders because they change treatment and risk more than the personality label alone.[3][7][17]
Management — acute crisis and resuscitation
Immediate priorities. Scene safety, weapons, medical stabilisation of intoxication, withdrawal, head injury or overdose. De-escalate; use environmental controls; pharmacological rapid tranquillisation only when needed for imminent harm per local emergency protocols with monitoring — not as long-term "ASPD sedation."[5]
Crisis psychiatry stance. Validate nothing that excuses harm; still treat medical and psychiatric comorbidity with the same standard of care as any other patient. Avoid collusive minimisation and avoid pejorative exclusion ("personality — no admission") when acute risk or treatable illness is present.[5][17]
Management — definitive and stepwise
What the evidence actually supports
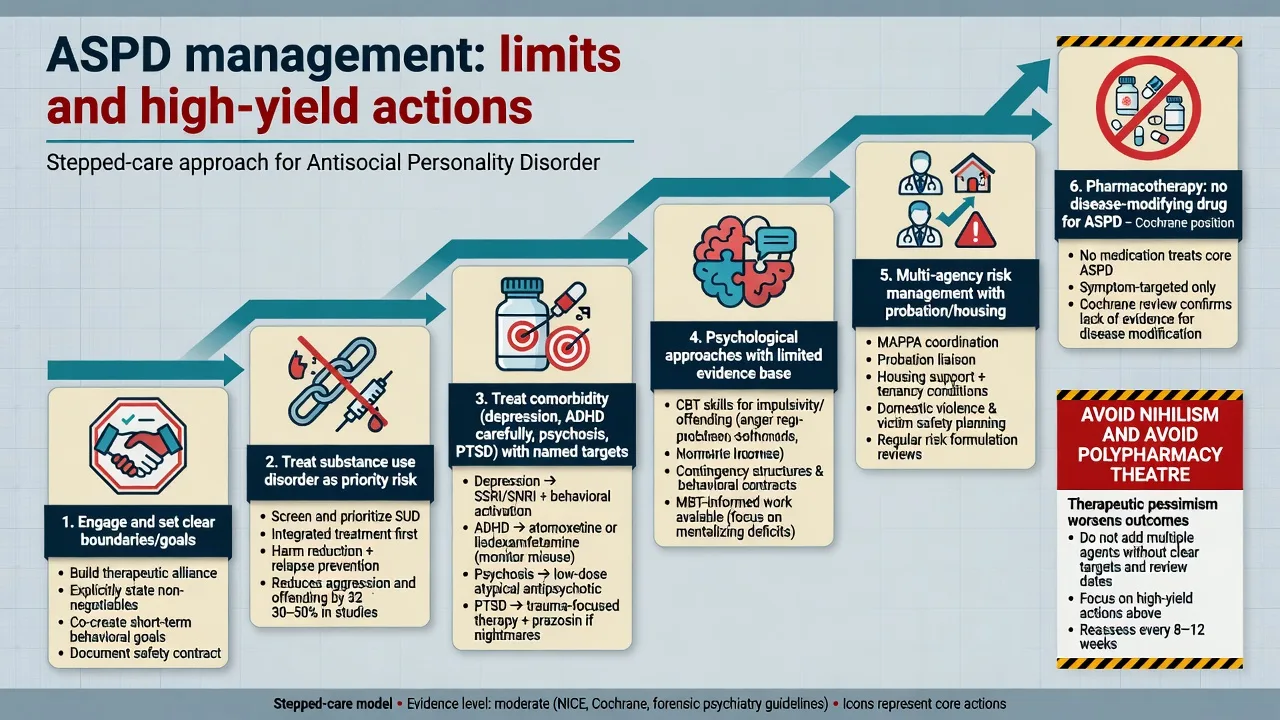
NICE-aligned summaries for antisocial personality disorder emphasise recognition, assessment of risk and needs, multi-agency working, and psychological approaches where engagement is possible, while remaining honest about evidence limits.[5] Cochrane reviews of psychological interventions for ASPD find the evidence base limited and heterogeneous; no single therapy has a robust, replicated disease-modifying effect across populations.[6] Cochrane reviews of pharmacological interventions likewise do not support any medication as treatment of ASPD itself.[7]
Psychological and psychosocial approaches
In practice (and in exam answers), name a coherent package rather than a miracle brand: clear goals and firm team boundaries with transparency about confidentiality limits when risk escalates; cognitive-behavioural work on impulsivity, problem-solving, offence-related thinking and anger where engagement is possible; contingency structures reinforcing prosocial behaviour in forensic and residential programmes; and mentalization-based approaches for ASPD where available — RCT evidence in comorbid BPD+ASPD populations supported MBT over structured clinical management on some outcomes, and a multicentre probation RCT (MOAM line / Fonagy and colleagues) evaluates MBT for men with ASPD on community sentences. Cite these as emerging structured evidence, not a universal cure.[5][6][12][13]
Pharmacotherapy — only for targets you can name
No medication treats the personality disorder as a whole.[7] Treat:
- Substance use disorders with standard evidence-based pathways (this is often the highest-yield risk lever).[1][17]
- Major depression, anxiety, psychosis with usual algorithms and means-safety awareness.
- ADHD only after careful longitudinal diagnosis; stimulants require risk–benefit analysis for diversion and misuse — non-stimulant options may be considered in high-diversion-risk contexts (individualise; check local product information).
- Aggression/impulsivity symptom targets sometimes prompt specialist off-label trials in forensic settings; any such trial needs a written target, baseline investigations as indicated, metabolic/ECG monitoring when using antipsychotics, and a stop/review date. Do not stack benzodiazepines for chronic personality control.[7]
Example adult prescribing language when an examiner forces a named comorbid plan (individualise). For co-occurring major depressive disorder without bipolarity, a common first-line example is sertraline 50 mg orally daily, early review for activation and adherence, titrate toward 50–150 mg as tolerated with limited dispensing if overdose/diversion risk is high — this treats depression, not ASPD identity.[7] For alcohol use disorder with dependence features, combine psychosocial treatment with evidence-based relapse-prevention pharmacotherapy when appropriate (for example naltrexone 50 mg orally daily if no opioid use and LFTs acceptable, or acamprosate per product information) — again treating SUD, not "curing ASPD."[1][7]
Care system and multi-agency work
Match intensity to risk: community dual-diagnosis and CMHT pathways; probation/parole partnership; housing and employment support; residential or forensic pathways when community risk is uncontainable. Write a risk management plan with review dates. Consistency beats charismatic one-off confrontations.[5][17]
Australian and New Zealand practice emphasises multi-agency risk management, cultural safety, and integration with alcohol and other drug services. Forensic mental health services manage higher-risk and justice-involved cohorts where ASPD and substance comorbidity are common. Mental Health Act and justice statutes are state/territory-specific — name principles, not invented sections.[17]
Specific subtypes and scenarios
High psychopathic traits versus impulsive-aggressive externalising. Factor-1-heavy presentations show more instrumental harm and shallow affect; impulsive-aggressive presentations show more reactive violence and affective instability — management still centres on substances, boundaries and structured risk work.[8][9]
ASPD with severe SUD. Expect higher violence, overdose and chaos; integrated dual treatment outperforms siloed care rhetoric.[1][17]
ASPD with BPD. Comorbidity is examinable; mentalization-based work has trial data in this dual group.[13]
Intimate partner violence. Risk formulation must name the partner/children, separation spikes, stalking, and substance use — ASPD label neither explains away nor excuses harm.[16]
Youth pathway. Recognition and management of conduct disorder and antisocial behaviour in children and young people (including parenting programmes and multimodal interventions summarised in NICE/SCIE guidance) is the prevention conversation examiners expect when asked about "stopping ASPD before it starts."[10][18]
Complications and pitfalls
Classic pitfalls: equating ASPD with psychopathy; missing late-onset organic change; collusion and boundary violations; writing court opinions outside expertise; polypharmacy for "aggression" without review; ignoring victim safety; staff-splitting when multiple agencies disagree.[3][8][16]
Prognosis and disposition
Natural history work suggests many individuals show some reduction in overt criminality with age, while interpersonal, occupational and substance problems often persist; a minority remain highly antisocial into later life.[4] Better trajectories associate with substance remission, stable relationships/employment and sustained engagement with structured supports.[4][5] Disposition follows risk and needs: community multi-agency plans when containable; escalation to more secure or residential settings when not. Reassess dynamically after relationship rupture, substance relapse, release from custody, or new weapon access.[4][16]
Special populations
Women. ASPD is under-recognised relative to men; higher rates of co-occurring BPD and trauma-related presentations appear in many clinical samples — apply the same operational criteria without sex stereotype.[2][15]
Adolescents and transition. Diagnose conduct disorder with care; intervene early (family-based and multimodal approaches). Do not casually label a 14-year-old with ASPD — age and CD rules matter.[10][18]
Older adults. New-onset antisocial behaviour is an organic/mood red flag until proven otherwise.[4]
Cultural and structural context. Over-representation of some groups in justice systems reflects structural factors as well as individual risk. Cultural formulation and Indigenous cultural safety in ANZ practice are part of competent care; structural context never erases individual accountability for harm.[15][17]
Evidence, guidelines and controversies
Core evidence pillars for fellowship answers include epidemiology and comorbidity (NESARC-III antisocial behavioural syndromes; British PD prevalence; ASPD/psychopathy reviews), construct clarity (psychopathy primers and Hare/Neumann), developmental pathways (conduct disorder and callous-unemotional traits; Robins tradition; natural history), treatment limits (NICE summaries; Cochrane psychological and pharmacological reviews), emerging MBT signals in comorbid and probation ASPD populations, risk-tool humility (Fazel meta-analysis), and neurobiology updates in youth psychopathic traits and adult ASPD.[1][2][4][5][6][7][8][9][10][11][12][13][15][16][19][20]
Mature controversies. Whether dimensional ICD-11 should replace categorical ASPD in clinical notes; how far psychopathy measurement should enter general adult practice; resource ethics for specialist therapies with limited effect sizes; and balancing public protection with non-discriminatory health care.[5][8]
Exam pearls
ANTISOCIAL — viva checklist
ANTISOCIAL
Age ≥18 + CD onset before 15 (DSM rule)
Not synonymous with psychopathy (Factor 1/2 construct)
Treat substances and other comorbidity first-yield
Instrumental vs reactive violence in risk formulation
Safeguarding partners/children; multi-agency plans
Organic exclusion for late-onset change
Cochrane/NICE: no disease-modifying drug; limited psych evidence
ICD-11 severity + dissociality/antagonism language
Assessment needs collateral — self-report minimises
Limits: boundaries, realistic goals, no nihilism
60-second oral summary
ASPD is DSM ≥3/7 behavioural features since 15, age ≥18, with conduct disorder before 15 — not the same as psychopathy. Expect substance comorbidity and elevated but non-deterministic violence risk; formulate static/dynamic factors and protect victims. Differentials: BPD, NPD, SUD alone, mania, psychosis, late-onset organic change. Treatment: multi-agency risk plans, treat SUD and other illness aggressively, offer structured psychological engagement with honest evidence limits (NICE/Cochrane), consider MBT-informed work where available, and never use polypharmacy as personality cure or nihilism as clinical policy.[3][5][6][7][8][12]
References
- [1]Goldstein RB, Chou SP, Saha TD, Smith SM, et al. The Epidemiology of Antisocial Behavioral Syndromes in Adulthood: Results From the National Epidemiologic Survey on Alcohol and Related Conditions-III J Clin Psychiatry, 2017.PMID 27035627
- [2]Werner KB, Few LR, Bucholz KK Epidemiology, Comorbidity, and Behavioral Genetics of Antisocial Personality Disorder and Psychopathy Psychiatr Ann, 2015.PMID 26594067
- [3]Glenn AL, Johnson AK, Raine A Antisocial personality disorder: a current review Curr Psychiatry Rep, 2013.PMID 24249521
- [4]Black DW The Natural History of Antisocial Personality Disorder Can J Psychiatry, 2015.PMID 26175389
- [5]Kendall T, Pilling S, Tyrer P, Duggan C, et al. Borderline and antisocial personality disorders: summary of NICE guidance BMJ, 2009.PMID 19176682
- [6]Gibbon S, Khalifa NR, Cheung NH, Völlm BA, et al. Psychological interventions for antisocial personality disorder Cochrane Database Syst Rev, 2020.PMID 32880104
- [7]Khalifa NR, Gibbon S, Völlm BA, Cheung NH, et al. Pharmacological interventions for antisocial personality disorder Cochrane Database Syst Rev, 2020.PMID 32880105
- [8]De Brito SA, Forth AE, Baskin-Sommers AR, Brazil IA, et al. Psychopathy Nat Rev Dis Primers, 2021.PMID 34238935
- [9]Hare RD, Neumann CS Psychopathy as a clinical and empirical construct Annu Rev Clin Psychol, 2008.PMID 18370617
- [10]Blair RJ, Leibenluft E, Pine DS Conduct disorder and callous-unemotional traits in youth N Engl J Med, 2014.PMID 25470696
- [11]Blair RJ The neurobiology of psychopathic traits in youths Nat Rev Neurosci, 2013.PMID 24105343
- [12]Fonagy P, Simes E, Yirmiya K, Wason J, et al. Mentalisation-based treatment for antisocial personality disorder in males convicted of an offence on community probation in England and Wales (Mentalization for Offending Adult Males): a multicentre, assessor-blinded, randomised controlled trial Lancet Psychiatry, 2025.PMID 39978982
- [13]Bateman A, O'Connell J, Lorenzini N, Gardner T, et al. A randomised controlled trial of mentalization-based treatment versus structured clinical management for patients with comorbid borderline personality disorder and antisocial personality disorder BMC Psychiatry, 2016.PMID 27577562
- [14]Kendler KS, Aggen SH, Czajkowski N, Røysamb E, et al. The structure of genetic and environmental risk factors for DSM-IV personality disorders: a multivariate twin study Arch Gen Psychiatry, 2008.PMID 19047531
- [15]Coid J, Yang M, Tyrer P, Roberts A, et al. Prevalence and correlates of personality disorder in Great Britain Br J Psychiatry, 2006.PMID 16648528
- [16]Fazel S, Singh JP, Doll H, Grann M Use of risk assessment instruments to predict violence and antisocial behaviour in 73 samples involving 24 827 people: systematic review and meta-analysis BMJ, 2012.PMID 22833604
- [17]Ogloff JR, Talevski D, Lemphers A, Wood M, et al. Co-occurring mental illness, substance use disorders, and antisocial personality disorder among clients of forensic mental health services Psychiatr Rehabil J, 2015.PMID 25799303
- [18]Pilling S, Gould N, Whittington C, Taylor C, et al. Recognition, intervention, and management of antisocial behaviour and conduct disorders in children and young people: summary of NICE-SCIE guidance BMJ, 2013.PMID 23535256
- [19]Choy O, Raine A The neurobiology of antisocial personality disorder Neuropharmacology, 2024.PMID 39244014
- [20]Robins LN Deviant children grown up Eur Child Adolesc Psychiatry, 1996.PMID 9010663