Psych · General adult psychiatry — personality disorders
Avoidant personality disorder
Also known as AVPD · Anxious personality disorder · Cluster C avoidant · Avoidant PD · Socially inhibited personality
Exam-exhaustive fellowship reference on avoidant personality disorder — DSM-5-TR and ICD-11 criteria, continuum with social anxiety disorder, epidemiology, cognitive-attachment mechanisms, differentials (schizoid, ASD, depression, dependent), assessment, CBT and schema therapy, SSRI treatment of comorbidity, prognosis. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Avoidant personality disorder (AVPD) is a high-yield Cluster C topic. FRANZCP MEQs demand criteria accuracy, the AVPD–social anxiety continuum debate, named psychotherapy ingredients, and a drug plan only for comorbidity. MRCPsych CASC tests plain-language explanation without stigma and why the person avoids yet still wants relationships. ABPN items test DSM thresholds, SPIN/LSAS concepts on the social-anxiety continuum, and CBT versus medication evidence from the social phobia literature. This topic is written so a candidate who has read nothing else can answer at consultant depth.[1][2][12]
Overview and definition
AVPD is an enduring, inflexible pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation that begins by early adulthood, is present across contexts, and causes distress or impairment — not better explained solely by another mental disorder, substance, or medical condition. The person typically wants social connection but anticipates humiliation, criticism, or rejection and therefore avoids occupational, intimate, and everyday interpersonal risks. That desire-with-fear pattern is the fellowship discriminator from schizoid personality disorder.[1][2][3]
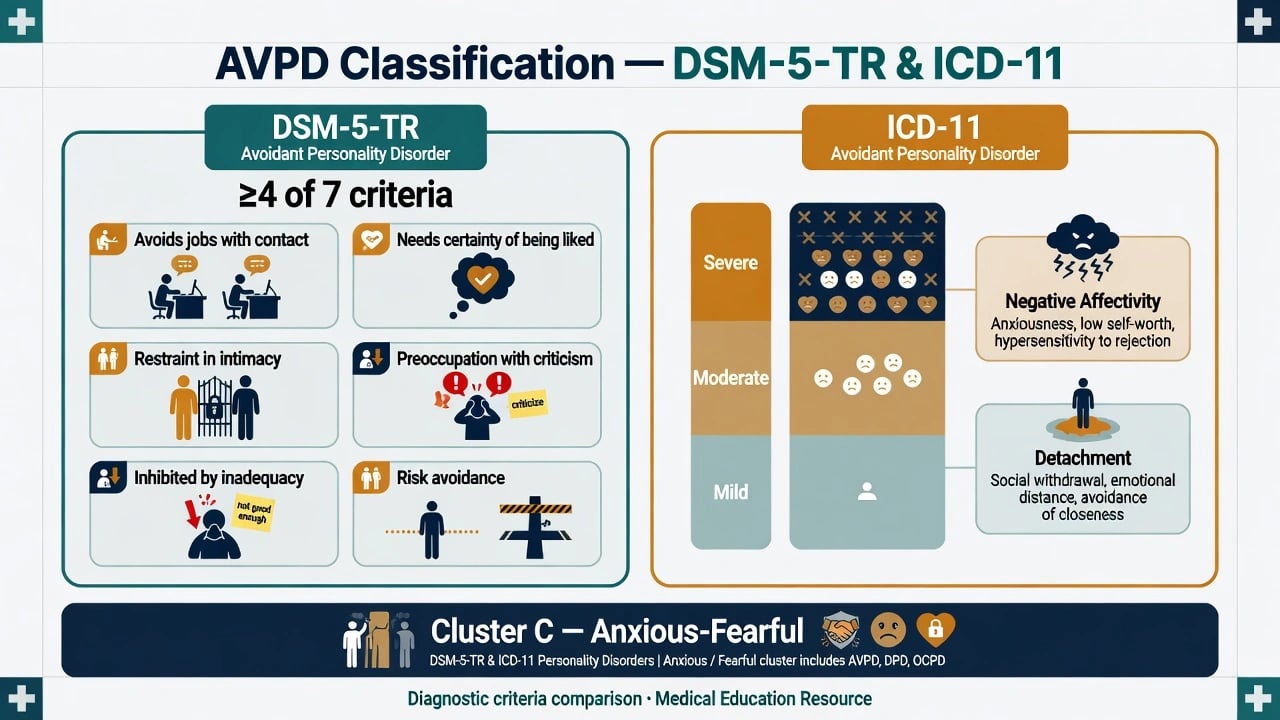
DSM-5-TR structure you must reproduce. After general personality disorder criteria are met, AVPD requires four or more of seven features: (1) avoids occupational activities that involve significant interpersonal contact because of fears of criticism, disapproval, or rejection; (2) is unwilling to get involved with people unless certain of being liked; (3) shows restraint within intimate relationships because of the fear of being shamed or ridiculed; (4) is preoccupied with being criticised or rejected in social situations; (5) is inhibited in new interpersonal situations because of feelings of inadequacy; (6) views self as socially inept, personally unappealing, or inferior to others; (7) is unusually reluctant to take personal risks or to engage in any new activities because they may prove embarrassing.[1][2]
ICD-11 framing. Personality disorder is graded by severity of self and interpersonal dysfunction (mild, moderate, severe), then qualified with trait domain descriptors. AVPD-like presentations typically map to negative affectivity (anxiousness, low self-worth) and detachment (withdrawal, intimacy avoidance) without assuming the DSM cluster label is a biological taxon. In viva answers, name which system you are applying when thresholds are examined.[1][2]
AMPD language (exam polish). Criterion A: impairment in identity (self as inadequate), self-direction, empathy (over-reading rejection), and intimacy (avoidance despite desire). Criterion B traits often include anxiousness, withdrawal, anhedonia, and intimacy avoidance. Use this language even if the service note uses categorical DSM coding.[1]
Classification and nosology
DSM-5-TR categorical
- General PD criteria + ≥4 of 7 features
- Cluster C (anxious/fearful) teaching scaffold
- Explicit self-view as inept/inferior is high-yield
- Must begin by early adulthood and be pervasive
ICD-11 dimensional
- Severity of personality dysfunction first
- Trait domains: negative affectivity, detachment
- Optional named pattern language varies by service
- Better for stepped-care intensity decisions
AVPD–SAD continuum debate
- Severity continuum hypothesis is widely taught
- Discontinuities argued: self-concept, attachment, global constriction
- Dual diagnosis often appropriate when both met
- Treatment borrows heavily from SAD evidence
Normal shyness
- Not diagnosable without pervasive impairment
- Does not force occupational avoidance and intimacy restraint
- Cultural reserve is not AVPD
- Ask functional cost and self-schema
AVPD is not performance-only stage nerves. Performance-only social anxiety can impair public speaking without the global inadequacy schema and multi-domain life constriction that define AVPD. Conversely, many people who meet AVPD criteria also meet criteria for social anxiety disorder (SAD); examiners reward dual diagnosis when both operational thresholds are met rather than forced either/or rhetoric.[1][5][6][12]
Epidemiology and risk factors
Headline epidemiology candidates must own
Community prevalence for AVPD varies by instrument and culture, but fellowship takeaways are stable: AVPD is common enough to matter in every general adult clinic; it co-travels with SAD and depression; and it produces occupational and relational disability out of proportion to “just being shy.” Population twin work supports shared genetic liability between social phobia and AVPD while still allowing residual uniqueness; interview-based heritability estimates for avoidant PD are moderate when carefully measured.[4][5][9][10][11]
Risk and aetiology. Behavioural inhibition temperament, early parental criticism or rejection, bullying, and insecure (often fearful) attachment feed a self-view of defectiveness and predicted humiliation. Cognitive processing biases amplify threat of negative evaluation. None of these factors alone makes the diagnosis; late-onset social withdrawal is an organic and affective red flag until proven otherwise.[1][2][9]
Pathophysiology and mechanisms
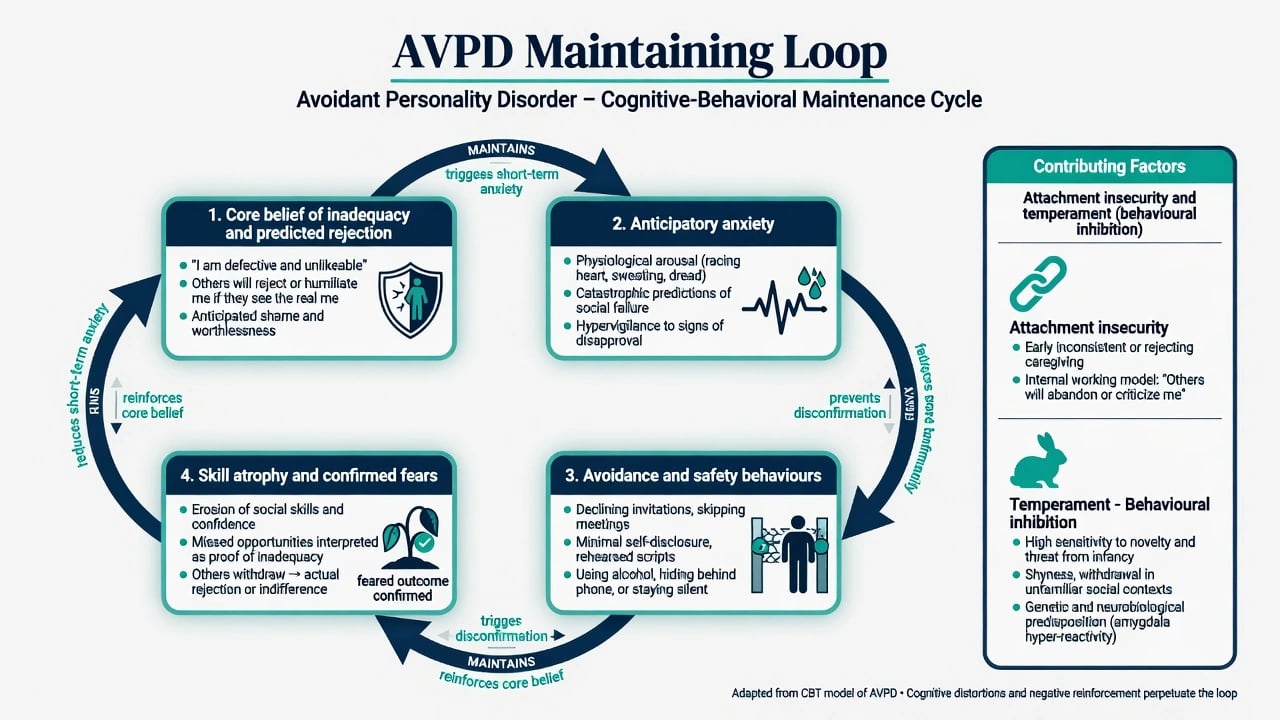
Cognitive-behavioural loop. Core beliefs (“I am inadequate / unappealing”) and conditional assumptions (“If people really know me, they will reject me”) generate anticipatory anxiety. Safety behaviours (minimal speech, gaze avoidance, rehearsing apologies, alcohol before social events) and outright avoidance reduce short-term anxiety but prevent disconfirmation and produce skill atrophy — confirming the original belief.[1][2][3]
Attachment and interpersonal model. Many patients desire closeness yet fear humiliation; interpersonal distance becomes both shield and source of loneliness. Interpersonal research comparing SAD and AVPD highlights attachment and self-other representation differences that matter for therapy targets beyond simple exposure lists.[3]
Schema model. Maladaptive schemas of defectiveness/shame, social isolation, failure, and emotional inhibition organise identity and intimacy avoidance. This is why schema therapy is examinable when global self-concept, not only situation-specific anxiety, dominates the formulation.[2][7]
Continuum versus discontinuity with SAD. The prevailing teaching paradigm is a severity continuum: AVPD as a more pervasive, self-concept-laden variant of social-evaluative fear. Twin and national survey data show substantial relatedness. Distinctiveness arguments emphasise broader personality dysfunction, intimacy avoidance, and attachment features not fully captured by SAD criteria alone. Mature viva answer: name the continuum, acknowledge residual differences, and treat what is present (often both).[1][4][5][6]
Clinical presentation
Core picture. Patients avoid jobs or tasks that require meetings, presentations, or evaluation; delay dating; have few friends outside obligatory contexts; and describe chronic loneliness with intense fear of looking foolish. MSE: anxious affect, self-deprecating thought content, anticipatory worry about the interview itself, and safety behaviours (brevity, excessive apologising, poor eye contact). Insight into the cost of avoidance may be good while change remains terrifying.[1][2]
Occupational presentation. Underemployment relative to ability, refused promotions, sick leave around appraisals, and “technical excellence with invisible person” patterns. Colleagues may never know the intensity of anticipatory dread.[1]
Crisis presentation. After rejection, public embarrassment, or job loss, comorbid major depression and suicidal ideation can escalate rapidly. Alcohol may have been the only social facilitator; withdrawal and dual diagnosis then enter the acute plan.[1][12]
Differential diagnosis
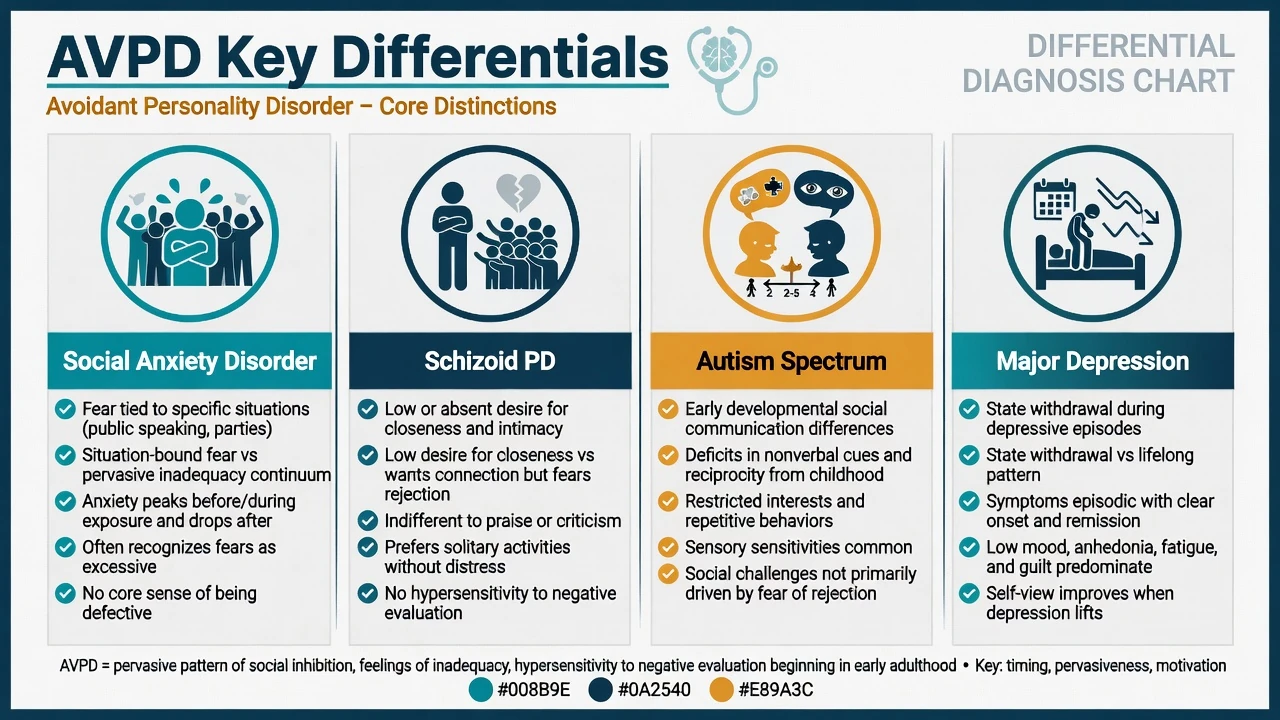
AVPD vs SAD
- Continuum is real; dual diagnosis common
- AVPD: more pervasive inadequacy schema and life constriction
- SAD: can be more situation- or performance-bound
- Both benefit from exposure-based CBT principles
AVPD vs schizoid PD
- AVPD: wants relationships, fears rejection
- Schizoid: typically low desire for close relationships
- Ask desire, not only observed solitude
- Affect is anxious vs restricted/cold
AVPD vs ASD
- ASD: early developmental social communication differences, RRB, sensory profile
- AVPD: self-conscious fear of negative evaluation dominant
- Dual formulation possible — do not force either/or
- Developmental history is mandatory
AVPD vs depression
- MDD: state withdrawal, anhedonia, often episodic
- AVPD: lifelong pattern from early adulthood
- Depression can amplify avoidance — treat both
- Suicide risk rises when they co-occur
Other essential discriminators. Dependent PD: excessive need to be cared for and submissive clinging, not primarily fear of evaluation. Paranoid PD: distrust and perceived malevolence rather than self as inferior. Body dysmorphic disorder: appearance-focused shame driving avoidance. Substance-induced social fear. Late-onset organic personality change (TBI, frontotemporal, endocrine). Always place mood, trauma, and neurodevelopmental conditions on the board.[1][3][18]
Clinical and bedside assessment
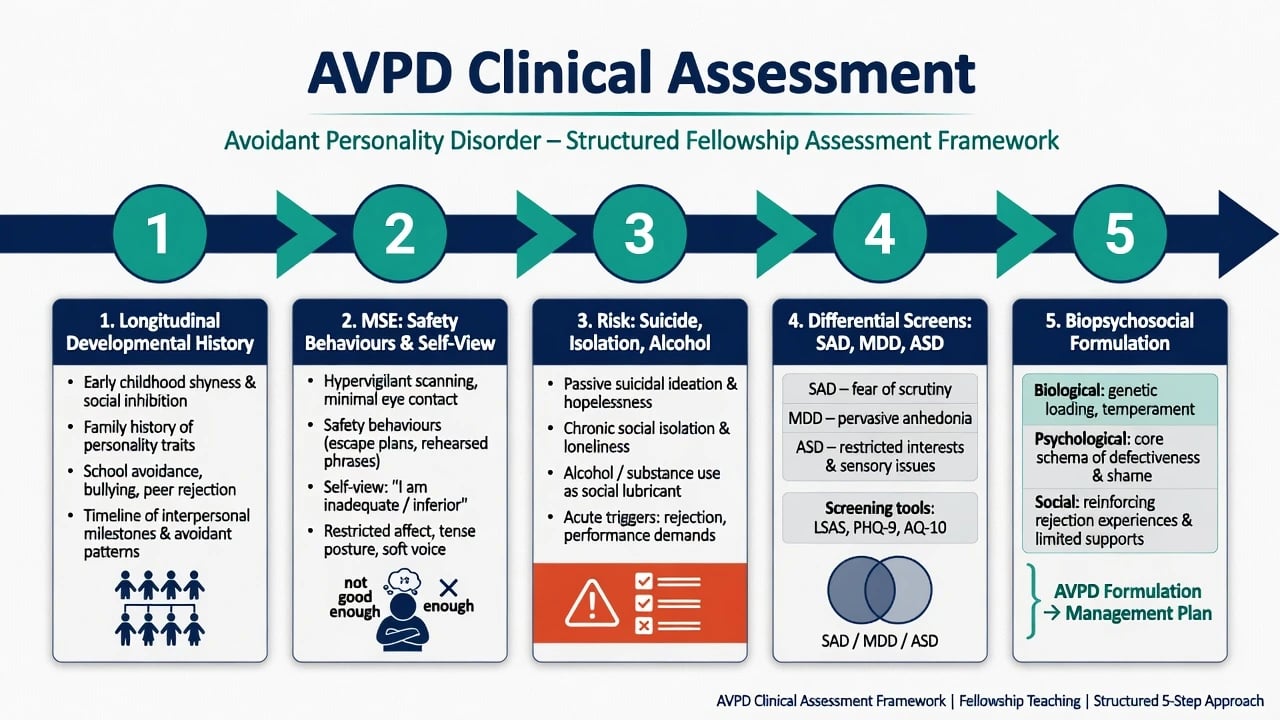
History structure. Developmental shyness and behavioural inhibition; school bullying or humiliation events; friendship and romantic chronology; occupational avoidance under evaluation; alcohol or substances as social lubricants; prior therapy and medication trials; what the patient wants help with today (often depression or work, not “personality”). Obtain collateral when isolation and minimisation limit the history.[1][2]
MSE focus. Rapport (anxious, apologetic), affect anxiety, thought content (anticipated humiliation), insight, judgement about risks of total avoidance, and alliance quality. Document safety behaviours in the room — they are formulation gold.[1]
Risk. Suicide and self-harm risk rise with comorbid depression and after rejection. Assess isolation, self-neglect, access to means, and alcohol. Capacity is decision-specific. Safeguarding matters if the person is exploited because of isolation and low self-worth.[1]
Tools (conceptual). SCID-5-PD / IPDE for categorical PD diagnosis; SPIN and related social anxiety scales for severity on the continuum; depression rating scales; ASD screens when developmental clues fire. Tools support — they do not replace — clinical diagnosis.[19]
Investigations
AVPD has no laboratory gold standard. Investigate to exclude mimics and prepare for medication when used: TSH, FBC, U&E, LFT, glucose/lipids, pregnancy test when relevant, urine drug screen when substances may explain behaviour, ECG when cardiac risk or QTc-risk drugs are planned. Neuroimaging or EEG only when late-onset change, focal neurology, seizures, or cognitive decline fire. Screen systematically for SAD, major depression, ASD, substance use, and other PD traits because they change the map more than the AVPD label alone.[1][12][18]
Management — acute / emergency
Acute principles. Validate the fear of rejection without colluding with total avoidance forever. Do not force intensive group exposure in the first crisis hour. Assess alcohol dependence if drinking was the only social strategy. Use jurisdiction-specific Mental Health Act principles when statutory criteria are met; do not invent section numbers.[1][12]
Management — definitive and stepwise
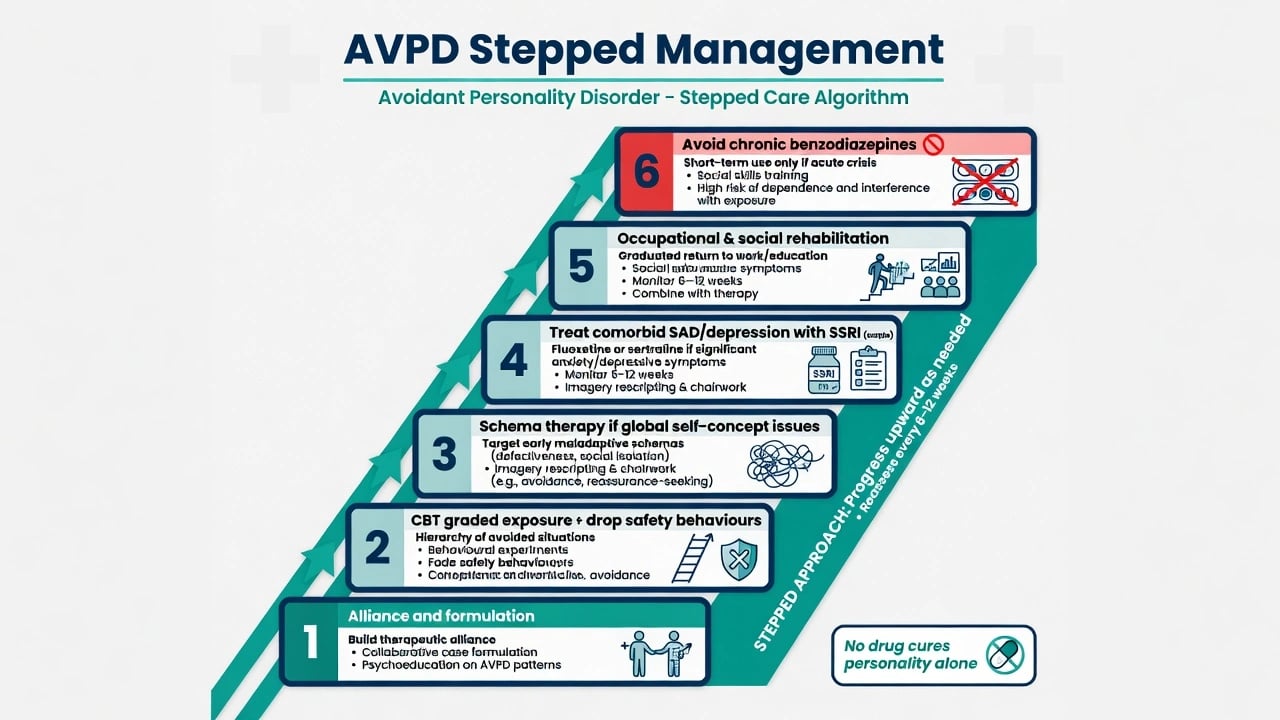
Psychotherapy first-line
Structured psychological treatment is the core of definitive care. Reviews of AVPD emphasise CBT and schema-focused approaches as the most promising evidence base, while noting the disorder remains under-researched relative to its disability.[1][2]
CBT ingredients examiners expect by name. Collaborative formulation of the fear-of-negative-evaluation loop; hierarchy of avoided situations; graded exposure and behavioural experiments; explicit identification and dropping of safety behaviours; cognitive restructuring of inadequacy and mind-reading of rejection; social skills practice when true skill deficits exist (not assumed). Because of continuum with SAD, the adult social anxiety evidence base — including network meta-analysis favouring individual CBT among psychological options — is legitimate support for exposure-based work on this pathway.[2][12][13][17]
Schema therapy. When global defectiveness schemas, intimacy avoidance, and lifelong self-concept dominate, schema therapy targets modes and early maladaptive schemas. A multicentre RCT of schema therapy for personality disorders (Bamelis and colleagues) demonstrated clinical effectiveness versus clarification-oriented psychotherapy and treatment as usual in a mixed PD sample that included substantial Cluster C pathology — the named trial beyond BPD-only evidence that fellowship answers should own. Economic evaluation supported its value in that programme of research.[7][8]
Alliance stance. Predictability, warmth without smothering, and paced exposure beat early forced groups that confirm the fear of humiliation. Dropout is often formulation, not “laziness.” Rupture repair is part of the treatment.[1][2]
Pharmacotherapy — comorbidity and social-evaluative anxiety
No medication treats AVPD as a whole. Drugs are for comorbid SAD, depression, or other Axis I targets, with measurement and review dates. Evidence-based pharmacotherapy of social anxiety disorder supports SSRIs (and some SNRIs) as first-line medication options; phenelzine has historical efficacy but practical and safety limits; benzodiazepines are not a long-term personality solution.[13][14][20]
Named adult example when an examiner forces a plan (individualise; check local product information). For comorbid generalised social anxiety or major depression without bipolarity: sertraline 50 mg orally once daily, review in 1–2 weeks for activation, anxiety increase and suicidality (especially under age 25), titrate toward a therapeutic range commonly 50–150 mg daily as tolerated, with a response review at 6–12 weeks at an adequate dose and limited early supply if overdose risk is elevated. Sertraline has placebo-controlled evidence in generalised social phobia; paroxetine also has classic RCT support — choose one agent, counsel sexual side effects and discontinuation syndrome, and pair with CBT rather than using pills as permanent avoidance of exposure.[15][16][20]
Historical exam pearl. Cognitive behavioural group therapy versus phenelzine trials in social phobia established that both can work acutely, with different long-term and tolerability profiles — useful for ABPN-style history of treatment questions, not a mandate to start MAOIs in every AVPD patient.[17]
Avoid. Chronic benzodiazepines for social performance; alcohol as prescribed “courage”; polypharmacy stacking without targets; treating “personality” with antipsychotics in the absence of psychotic phenomena or another indication.[14][20]
Care system and disposition
Most patients are managed in outpatient psychotherapy and general adult pathways. Step up for acute suicide risk, severe depression, or self-neglect. Step down when exposure generalises and occupational function improves. Occupational rehabilitation and graded return-to-work plans are part of recovery, not optional extras.[1][7]
Australian and New Zealand practice emphasises stepped mental health care, access to psychological therapies where available, trauma-informed engagement, and culturally safe practice. Local Mental Health Act provisions govern involuntary care — name least-restrictive principles, not invented foreign section numbers. Coordinate with primary care for SSRI prescribing and monitoring when specialist waitlists are long.[1][14]
Specific subtypes and scenarios
AVPD + generalised SAD. Dual diagnosis; combine structured CBT with SSRI when severity or non-response to therapy alone warrants medication.[5][13]
AVPD + major depression after rejection. Treat depression aggressively; do not dismiss suicidality as “personality.” Sequence risk containment, antidepressant when indicated, and resume exposure when affective load allows.[1][12]
Performance-only social anxiety without AVPD. Narrower fear; beta-blocker discussion may appear in pure performance contexts in some services — do not over-expand to lifelong AVPD without criteria.[12]
Alcohol as safety behaviour. Dual-diagnosis pathway; motivational work; do not simply ban alcohol without replacement skills and support.[12]
AVPD dual-formulated with ASD. Developmental history, sensory profile, and quality of social motivation prevent false dichotomies; adapt CBT language and pace.[18]
Severe isolation with care refusal. Outreach, treat depression, capacity assessment for specific decisions, least-restrictive support — hospitalisation is for risk or severe illness, not the PD label alone.[1]
Complications and pitfalls
Classic pitfalls: calling AVPD “just shy” and excluding from services; missing depression, ASD, or BDD; forcing early intensive group without alliance; chronic benzodiazepines or alcohol replacing exposure; polypharmacy without targets; therapist frustration misread as patient “unmotivation”; confusing schizoid low desire with avoidant fear; diagnosing PD from a single interview.[1][2][18]
Prognosis and disposition
Without treatment, symptoms are relatively stable and disabling. With structured CBT or schema-focused work and treatment of comorbidity, meaningful improvement is expected — AVPD is not a life sentence of solitude. Functional recovery (intimacy, career) may lag symptom reduction and needs explicit rehabilitation goals. Disposition is usually outpatient; reassess after rejection crises and after major life transitions (new job, university, relationship attempts).[1][2][7]
Special populations
Youth. Distinguish emerging avoidant patterns from normal developmental shyness. Early treatment of social anxiety may prevent entrenchment of inadequacy schemas. Do not casually assign permanent PD labels without longitudinal evidence.[1][12]
Older adults. Lifelong AVPD may decompensate after retirement, bereavement, or loss of a protective partner. New late-life social withdrawal is organic/mood until proven otherwise.[1]
Pregnancy and parenting. Treat depression and anxiety carefully; minimise unnecessary polypharmacy; support attachment and social support networks that reduce isolation.[14]
Cultural formulation. Collectivist reserve, respect hierarchies, or distrust of systems after discrimination is not automatically AVPD. In ANZ practice, Indigenous cultural safety and family-inclusive care are competencies.[1]
Evidence, guidelines and controversies
Phenomenology and treatment reviews: Lampe and Malhi 2018; Weinbrecht and colleagues 2016; Frandsen interpersonal SAD–AVPD work.[1][2][3]
Epidemiology and relatedness: NESARC and NCS-R personality disorder prevalence; Cox national survey relationship of generalised social phobia and AVPD; Ralevski distinctiveness debate; Reichborn-Kjennerud twin study; Gjerde heritability of avoidant PD.[4][5][6][9][10][11]
Treatment anchors: Bamelis schema therapy RCT and economic evaluation; Mayo-Wilson network meta-analysis of psychological and pharmacological interventions for adult SAD; Canadian anxiety guidelines; SSRI RCTs (paroxetine, sertraline); Heimberg CBGT versus phenelzine lineage; Blanco pharmacotherapy synthesis.[7][8][13][14][15][16][17][20]
Mature controversies. Whether AVPD should be collapsed into severe SAD; how far ICD-11 severity should replace categorical Cluster C labels; how early to introduce group exposure; and how to resource schema therapy outside specialist clinics.[1][5][6]
Exam pearls
AVOIDANT — viva checklist
AVOIDANT
≥4 of 7 DSM features after general PD criteria
Views self as inept/inferior — core self-schema
Overlap with SAD is large; dual diagnosis OK
Intimate restraint from fear of shame, not low desire
Differentiate schizoid (desire), ASD, depression
Alliance-first CBT: exposure + drop safety behaviours
No drug cures PD; SSRI for comorbid SAD/depression
Therapy evidence includes schema (Bamelis) and SAD CBT NMA
60-second oral summary
AVPD is DSM ≥4/7 social inhibition, inadequacy, and rejection sensitivity with general PD criteria — the person wants connection but fears humiliation. Related to but not identical with social anxiety disorder; dual diagnosis is common. Discriminate schizoid (desire), ASD (developmental), and depression (state). Treat with alliance-first CBT: graded exposure, drop safety behaviours, restructure inadequacy beliefs; use schema therapy when global self-concept dominates (Bamelis RCT). Medicate comorbid SAD/depression with a named SSRI (e.g. sertraline 50 mg titrated) plus review — not polypharmacy as personality cure. Risk rises after rejection; hope and structure beat stigma.[1][2][7][13][16]
References
- [1]Lampe L, Malhi GS Avoidant personality disorder: current insights Psychol Res Behav Manag, 2018.PMID 29563846
- [2]Weinbrecht A, Schulze L, Boettcher J, Renneberg B Avoidant Personality Disorder: a Current Review Curr Psychiatry Rep, 2016.PMID 26830887
- [3]Frandsen FW, Simonsen S, Poulsen S, Sørensen P, et al. Social anxiety disorder and avoidant personality disorder from an interpersonal perspective Psychol Psychother, 2020.PMID 30656823
- [4]Reichborn-Kjennerud T, Czajkowski N, Torgersen S, et al. The relationship between avoidant personality disorder and social phobia: a population-based twin study Am J Psychiatry, 2007.PMID 17974938
- [5]Cox BJ, Pagura J, Stein MB, Sareen J The relationship between generalized social phobia and avoidant personality disorder in a national mental health survey Depress Anxiety, 2009.PMID 19031488
- [6]Ralevski E, Sanislow CA, Grilo CM, et al. Avoidant personality disorder and social phobia: distinct enough to be separate disorders? Acta Psychiatr Scand, 2005.PMID 16095476
- [7]Bamelis LL, Evers SM, Spinhoven P, Arntz A Results of a multicenter randomized controlled trial of the clinical effectiveness of schema therapy for personality disorders Am J Psychiatry, 2014.PMID 24322378
- [8]Bamelis LL, Arntz A, Wetzelaer P, Verdoorn R, et al. Economic evaluation of schema therapy and clarification-oriented psychotherapy for personality disorders: a multicenter, randomized controlled trial J Clin Psychiatry, 2015.PMID 26579561
- [9]Gjerde LC, Czajkowski N, Røysamb E, Orstavik RE, et al. The heritability of avoidant and dependent personality disorder assessed by personal interview and questionnaire Acta Psychiatr Scand, 2012.PMID 22486635
- [10]Lenzenweger MF, Lane MC, Loranger AW, Kessler RC DSM-IV personality disorders in the National Comorbidity Survey Replication Biol Psychiatry, 2007.PMID 17217923
- [11]Grant BF, Hasin DS, Stinson FS, Dawson DA, et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions J Clin Psychiatry, 2004.PMID 15291684
- [12]Stein MB, Stein DJ Social anxiety disorder Lancet, 2008.PMID 18374843
- [13]Mayo-Wilson E, Dias S, Mavranezouli I, Kew K, Clark DM, et al. Psychological and pharmacological interventions for social anxiety disorder in adults: a systematic review and network meta-analysis Lancet Psychiatry, 2014.PMID 26361000
- [14]Katzman MA, Bleau P, Blier P, Chokka P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders BMC Psychiatry, 2014.PMID 25081580
- [15]Stein MB, Liebowitz MR, Lydiard RB, Pitts CD, et al. Paroxetine treatment of generalized social phobia (social anxiety disorder): a randomized controlled trial JAMA, 1998.PMID 9728642
- [16]Van Ameringen MA, Lane RM, Walker JR, Bowen RC, et al. Sertraline treatment of generalized social phobia: a 20-week, double-blind, placebo-controlled study Am J Psychiatry, 2001.PMID 11156811
- [17]Heimberg RG, Liebowitz MR, Hope DA, Schneier FR, et al. Cognitive behavioral group therapy vs phenelzine therapy for social phobia: 12-week outcome Arch Gen Psychiatry, 1998.PMID 9862558
- [18]Lugnegård T, Hallerbäck MU, Gillberg C Personality disorders and autism spectrum disorders: what are the connections? Compr Psychiatry, 2012.PMID 21821235
- [19]Connor KM, Davidson JR, Churchill LE, Sherwood A, et al. Psychometric properties of the Social Phobia Inventory (SPIN). New self-rating scale Br J Psychiatry, 2000.PMID 10827888
- [20]Blanco C, Bragdon LB, Schneier FR, Liebowitz MR The evidence-based pharmacotherapy of social anxiety disorder Int J Neuropsychopharmacol, 2013.PMID 22436306