Psych · General adult psychiatry — feeding and eating disorders
Avoidant/restrictive food intake disorder (ARFID)
Also known as ARFID · Avoidant restrictive food intake disorder · Selective eating disorder · Extreme picky eating · Feeding disorder of infancy and early childhood (legacy) · CBT-AR · PARDI · NIAS
Exam-exhaustive fellowship reference on avoidant/restrictive food intake disorder (ARFID) — DSM-5-TR/ICD-11 criteria without shape/weight overvaluation; three presentations (sensory sensitivity, fear of aversive consequences, lack of interest); medical complications of restriction; PARDI/NIAS assessment; CBT-AR and adapted FBT; autism interface; limits of pharmacotherapy. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Avoidant/restrictive food intake disorder (ARFID) is a high-yield differential and management topic at the psychiatry–paediatrics–medicine interface. FRANZCP MEQs test discrimination from anorexia nervosa, medical instability, and therapy choice. MRCPsych CASCs test explanation to families and graded exposure rationale. ABPN items test DSM criteria, presentation subtypes, and assessment tools. A candidate who reads only this topic should defend diagnosis, risk, and stepped care at consultant depth.[10][13][18]
Overview and definition
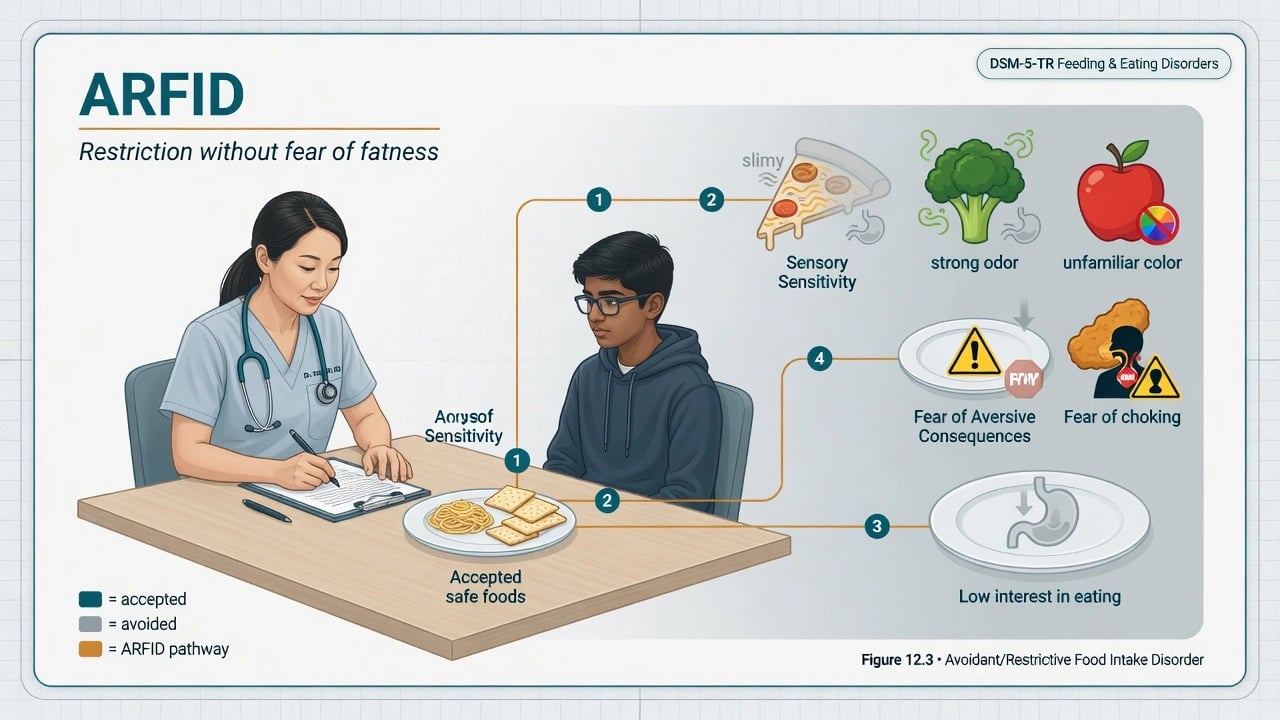
ARFID is characterised by persistent failure to meet appropriate nutritional and/or energy needs associated with one or more of: significant weight loss (or failure to achieve expected weight gain/growth in children); significant nutritional deficiency; dependence on enteral feeding or oral nutritional supplements; and/or marked interference with psychosocial functioning. The eating disturbance is not better explained by lack of available food or culturally sanctioned practice, and is not attributable solely to a concurrent medical condition or another mental disorder (or the severity exceeds what those would explain). Critically, there is no evidence of disturbance in the way body weight or shape is experienced, and the restriction is not driven by fear of gaining weight as in anorexia nervosa.[6][10][15]
Clinical essence for viva. Restriction is real and can be medically dangerous, but the motivation differs from AN: sensory aversion, fear of choking/vomiting/pain, or low appetite/interest — not thinness pursuit. Missing this discriminator misroutes psychotherapy.[1][10]
DSM-5-TR placement. Feeding and eating disorders chapter (alongside pica, rumination disorder, AN, BN, binge-eating disorder). ARFID replaced and expanded the DSM-IV category of feeding disorder of infancy or early childhood and is explicitly lifespan-applicable, including adults with longstanding selective eating.[10][15]
ICD-11. Avoidant-restrictive food intake disorder is recognised with analogous core features; always declare which manual you are using when boundary cases (AN vs ARFID; ASD food selectivity) are examined.[18]
Classification and clinical presentations
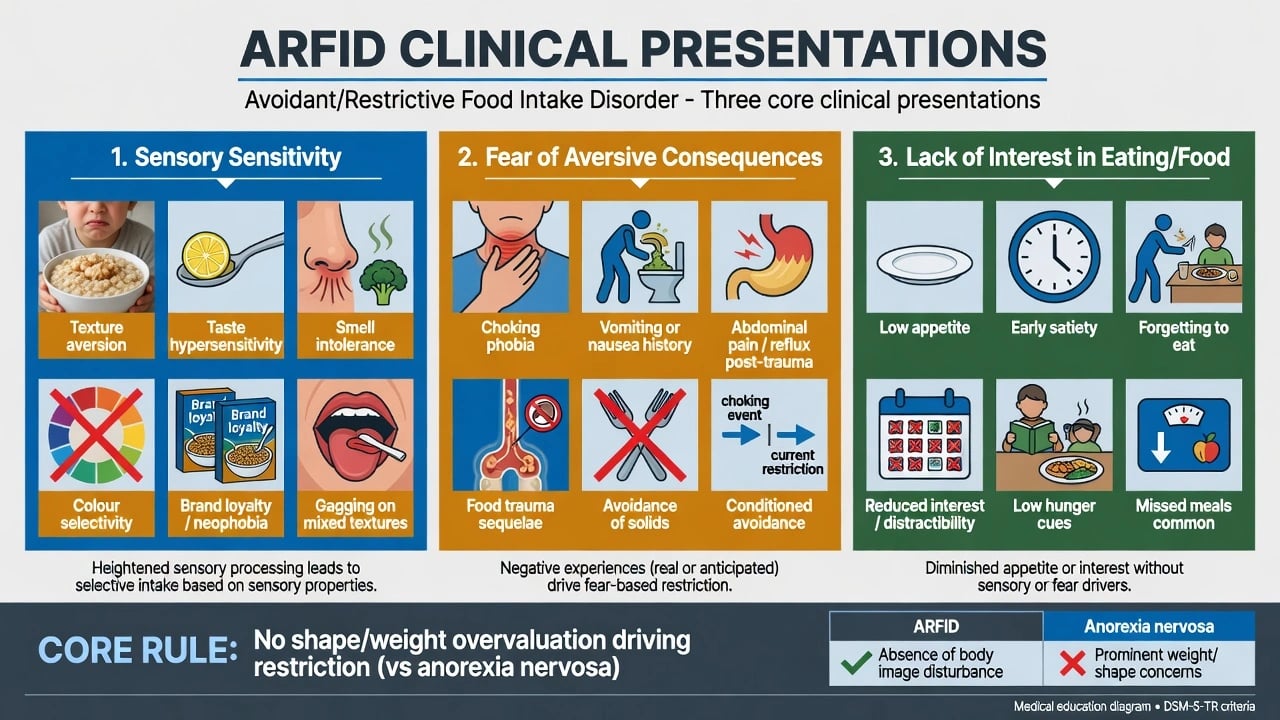
Sensory sensitivity
- Aversion to texture, taste, smell, colour, temperature, brand
- Extreme selectivity / food neophobia
- Gagging on mixed textures common
- Often lifelong picky-eating trajectory
Fear of aversive consequences
- Choking, vomiting, pain, contamination-type fear after event
- Avoidance of solids or specific textures after trauma
- High anticipatory anxiety at meals
- May look like specific phobia focused on swallowing
Lack of interest in eating/food
- Low appetite / low drive to eat
- Early satiety, forgetting meals
- Under-eating without weight phobia
- Often underweight or faltering growth
Not ARFID alone
- Fear of fatness / body-image disturbance → consider AN
- Picky eating without deficiency or impairment
- Primary medical dysphagia untreated
- Multi-theme OCD without ARFID nutritional criteria
Presentations commonly overlap. Thomas and colleagues organise a three-dimensional neurobiological framing (sensory, fear, and low-appetite pathways) that maps to formulation and treatment targets.[1][4] Severity is clinical (nutritional risk, growth, medical instability, functional impairment) rather than a simple BMI band like adult AN severity ratings.[12][16]
Epidemiology and risk factors
Headline epidemiology (exam framing)
In tertiary paediatric and adolescent eating-disorder programmes, ARFID accounts for a clinically important share of presentations once DSM-5 criteria are applied, with descriptive cohorts characterising younger age and different sex ratios compared with classic AN/BN samples.[6][7][8][9] Community prevalence estimates vary by instrument and age band; for exams, state order-of-magnitude clinic enrichment and avoid quoting a fabricated single population percentage.[13]
Associated factors. Anxiety disorders, autism spectrum disorder, sensory processing differences, gastrointestinal disease history, prior choking or vomiting events, developmental delay, and family accommodation of extremely narrow diets.[10][12][13] Functional burden includes social isolation around meals, school/work impairment, and medical sequelae of malnutrition.[10][16]
Pathophysiology and maintaining model
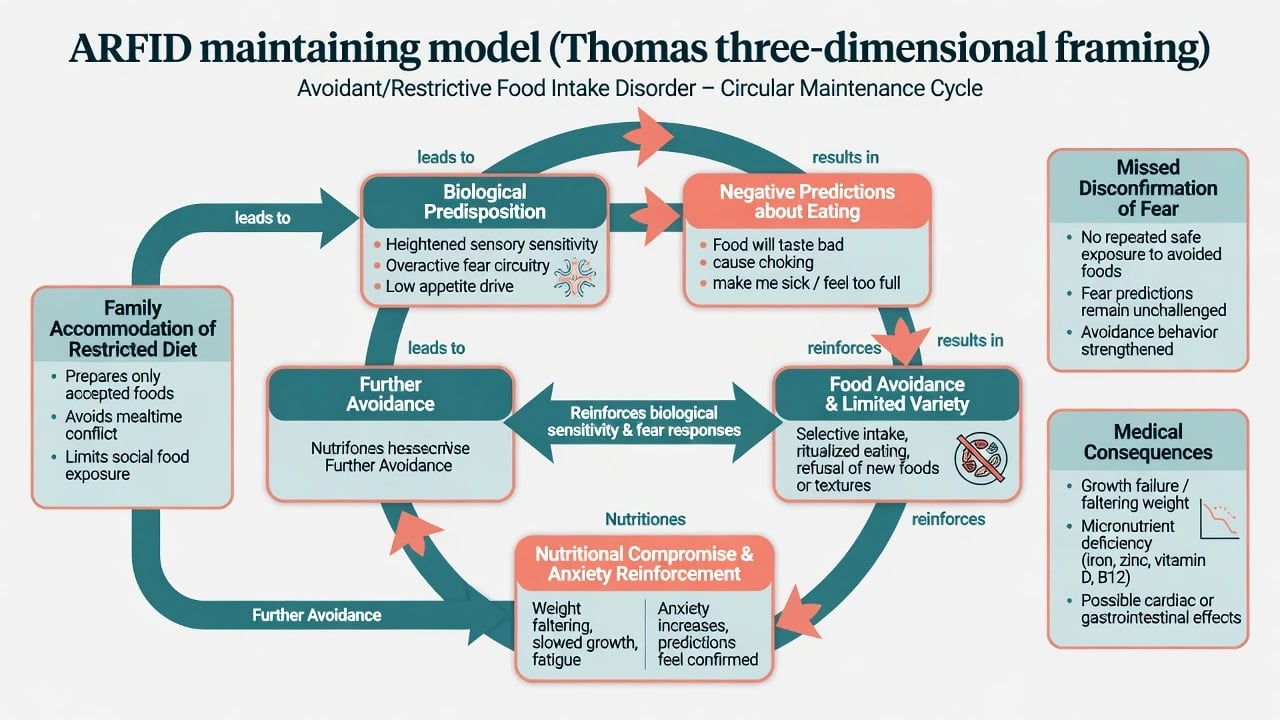
Three-dimensional model (viva-ready). Biological predispositions — heightened sensory sensitivity, overactive fear circuitry, and/or low appetite drive — generate negative predictions about eating. Avoidance and extreme selectivity prevent corrective learning, while family accommodation (preparing only accepted foods) reduces short-term conflict but maintains the repertoire. Nutritional compromise and anxiety further suppress appetite and increase aversive associations.[1][4]
Medical pathophysiology of restriction. When energy/protein intake is inadequate, multi-system effects mirror other restrictive eating disorders: bradycardia, orthostasis, bone density loss risk, endocrine disruption, gastrointestinal slowing, and micronutrient deficiency syndromes from narrow diets (iron, B12, vitamin D, vitamin C, zinc, and others depending on the accepted list).[12][16]
Imaging is not diagnostic for the individual patient.[1]
Clinical presentation
Sensory-selective. Extremely short accepted food lists (often beige/crunchy/specific brands), refusal of mixed textures, gagging, brand loyalty, and meltdowns or shutdowns when novel foods are presented. Weight may be normal if accepted foods are calorically dense — do not use normal BMI as reassurance against deficiency or impairment.[6][10]
Fear-based. Onset after choking, vomiting, or painful swallowing; progressive avoidance of solids; fear of dying or choking at meals; safety behaviours (tiny bites, purees only, prolonged chewing). Anxiety can be catastrophic despite medical clearance of the oropharynx.[1][12]
Low interest. Little spontaneous eating, early fullness, “I forget to eat,” underweight without body checking or fat phobia. Adults may present with longstanding low BMI and social avoidance of food-centred events.[1][3]
MSE language. Restricted intake history; anxiety or sensory distress around food; absence of shape/weight overvaluation on direct enquiry; insight into consequences may be partial in adolescents. Always screen suicide risk when depression/anxiety co-exist, and always screen for AN psychopathology so you do not miss dual or misclassified presentations.[10][15]
Differential diagnosis
Anorexia nervosa
- Fear of weight gain / interfering behaviours
- Body image disturbance or denial of seriousness
- Restriction serves thinness/control of shape
- May have sensory features secondary — still AN if core present
Medical GI/ENT disease
- Dysphagia, odynophagia, blood, nocturnal symptoms
- IBD, coeliac, EoE, stricture, malignancy
- Investigate red flags — do not assume pure ARFID
- ARFID can follow aversive medical events
Autism food selectivity
- Sensory eating common in ASD
- ARFID requires nutritional/psychosocial threshold
- Can fully co-occur — dual formulation
- ASD supports do not replace ARFID treatment
OCD / specific phobia
- Multi-theme OCD rituals beyond food
- Contamination OCD may overlap fear ARFID
- Choking phobia may meet ARFID if criteria met
- Treat content streams explicitly
Also discriminate ordinary developmental picky eating without deficiency or marked impairment; major depression with appetite loss (mood primary); substance use; and, in young children, safeguarding concerns including neglect or fabricated/induced illness when history is inconsistent.[10][13][15]
Clinical and bedside assessment
History structure. Onset and trajectory; exhaustive accepted/refused food list; sensory descriptors; aversive food events; volume and timing of intake; supplements or tube feeds; weight/growth chart; menses if relevant; gastrointestinal symptoms; autism/ADHD/anxiety history; family meal patterns and accommodation; prior treatments; explicit body-image and fear-of-fatness screen.[5][12]
Physical exam. BMI or BMI centile/growth velocity; heart rate, blood pressure (sitting/standing), temperature; signs of malnutrition; dental/ENT if indicated; abdominal exam.[16]
Structured tools. The PARDI (Pica, ARFID and Rumination Disorder Interview) is a multi-informant semi-structured diagnostic interview developed for feeding disorders including ARFID across the lifespan (pilot validation in youth).[5] The Nine-Item ARFID Screen (NIAS) provides dimensional subscales that help distinguish sensory, fear, and low-appetite presentations and support screening.[14] Neither replaces clinical diagnosis or medical risk assessment.
Risk. Medical instability, suicide if comorbid mood disorder, safeguarding, and capacity for nutrition decisions when refusal is life-threatening — decision-specific and jurisdiction-specific.[15][16]
Investigations
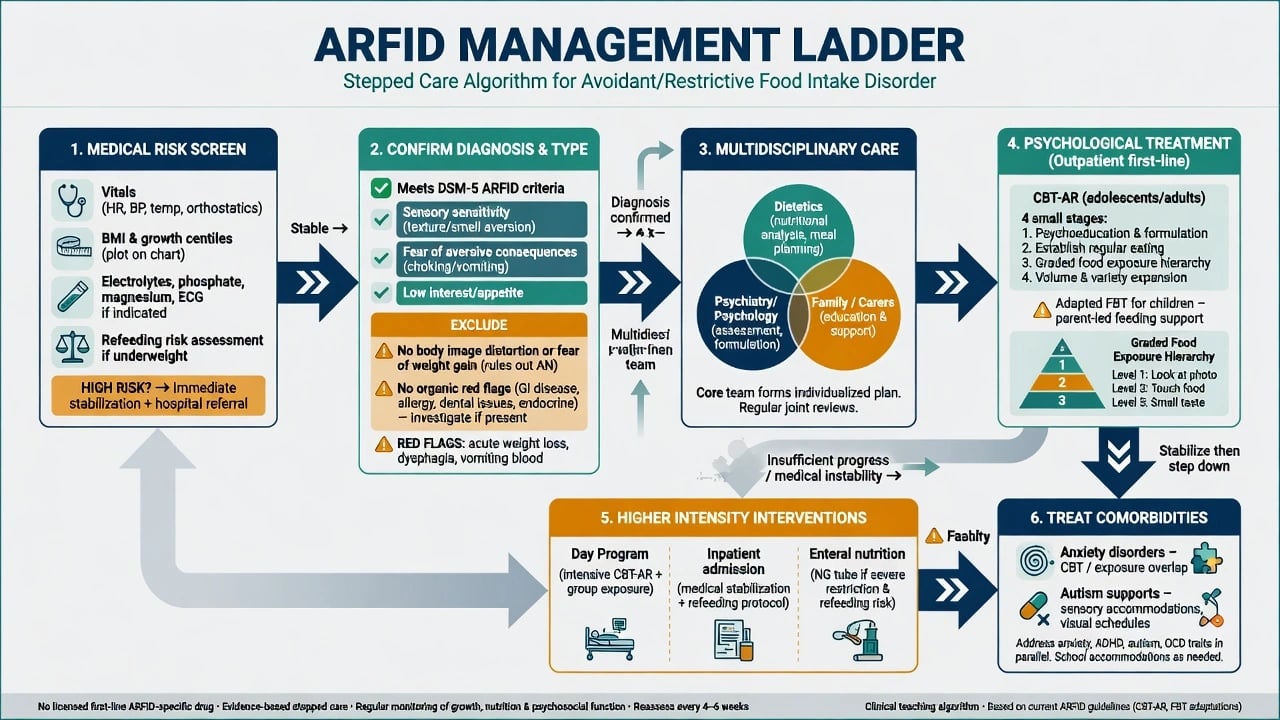
No biomarker diagnoses ARFID. Baseline bloods guided by restriction pattern: FBC, U&E, phosphate, magnesium, calcium, LFT, glucose, and micronutrients as indicated (iron studies, B12, folate, vitamin D; others by clinical suspicion). ECG when underweight, rapid loss, or cardiovascular symptoms. Targeted GI/ENT investigation for organic red flags. DEXA when prolonged malnutrition or other bone-risk features. During refeeding of depleted patients, serial phosphate/K/Mg as for other restrictive eating disorders.[12][16]
Management — acute risk and resuscitation
Refeeding syndrome prevention when restarting nutrition in depleted patients: protocolised intake, thiamine and multivitamins per local protocol, frequent phosphate/potassium/magnesium monitoring and proactive replacement, fluid balance, multidisciplinary ownership (medicine, dietetics, psychiatry).[16] Enteral nutrition (including nasogastric feeding) may be required when oral rehabilitation is unsafe or inadequate; use least-restrictive lawful means and decision-specific capacity assessment.[15][16]
Management — definitive and stepwise
Nutritional rehabilitation and dietetics
Core goals are adequate energy/protein, correction of deficiencies, and expansion of variety appropriate to the presentation. Dietitians skilled in eating disorders/feeding disorders co-lead plans. Weight restoration is prioritised when underweight before aggressive variety work if medical risk is high — paralleling restrictive-ED sequencing principles.[12][16][17]
CBT for ARFID (CBT-AR)
CBT-AR (Thomas/Eddy lineage) is a structured outpatient approach typically spanning roughly 20–30 sessions (more when significant underweight needs weight restoration first). Stages emphasise psychoeducation and formulation by presentation type, establishment of regular eating, graded exposure to novel foods, and relapse prevention. Youth proof-of-concept data support feasibility, acceptability, and clinical improvement including food variety and ARFID severity measures; adult proof-of-concept work similarly shows reductions in ARFID severity and increases in novel foods, with underweight subgroups showing BMI gains in early series.[2][3][4] These are proof-of-concept / open-series foundations — examiners reward naming CBT-AR and its logic while acknowledging the thinner RCT base versus AN/BN therapies.[4][13]
Presentation-specific tactics:
- Sensory: food chaining, texture hierarchies, repeated non-contingent exposure without forced flooding.
- Fear: graded hierarchy for solids/textures, behavioural experiments testing choking predictions after medical clearance, anxiety management skills.
- Low interest: scheduled meals/snacks, volume goals, reduce grazing that suppresses hunger cues.[1][4][12]
Adapted family-based treatment (youth)
Family-based treatment adaptations apply parental empowerment for renourishment and variety expansion across sensory, fear, and low-interest presentations — Lock and colleagues describe clinical application of FBT principles to ARFID presentations.[11] First-line for many medically suitable children/adolescents when family can lead meals, with individual CBT-AR when FBT is unsuitable or for older adolescents/adults.[2][11][12]
Pharmacotherapy
There is no licensed first-line ARFID-specific medication. Do not default to olanzapine as an ARFID “cure.” Treat comorbid anxiety, depression, OCD, or ADHD with standard evidence-based agents and monitoring when indicated. Any appetite-stimulating or off-label strategies belong in specialist contexts with clear goals, monitoring, and concurrent behavioural treatment — not as monotherapy while medical risk is ignored.[12][15][17]
Stepped care intensity
Outpatient CBT-AR/adapted FBT and dietetics → day programmes with supervised meals and exposure → inpatient medical/psychiatric care for instability or failed lower intensity → planned step-down with relapse prevention. Autism supports (sensory planning, visual schedules, communication adaptations) run in parallel, not instead of ARFID treatment.[12][15]
Specific subtypes and scenarios
Enteral-dependent ARFID. Multidisciplinary tube-weaning programmes after medical stability; graded oral exposure; avoid abrupt tube removal without oral competence.[12][16]
Adult ARFID. Lifelong selective eating may present via infertility work-ups, workplace impairment, pregnancy nutrition risk, or GI clinics; CBT-AR adult series supports a treatment pathway.[3]
Autism + ARFID. Dual formulation; sensory accommodations enable rather than replace exposure; meta-analytic and clinical literature highlight meaningful co-occurrence — neither diagnosis is automatic from the other.[13]
Post-choking fear presentation. ENT/medical clearance, then CBT-style graded exposure; avoid permanent puree diets without rehabilitation goals.[1][12]
Complications and pitfalls
- Missing micronutrient deficiency at normal BMI.[10][16]
- Treating as AN with pure weight-phobia CBT-E targets when body-image drive is absent.[4][15]
- Forced oral challenges without hierarchy or medical safety — trauma and drop-out.[4][12]
- Ignoring organic disease red flags or autism needs.[13]
- Colluding indefinitely with a five-food diet because “they grow on it.”[10]
- Declaring “no treatment evidence” and offering only generic counselling — name CBT-AR/FBT adaptations and medical pathways.[2][11]
Prognosis and disposition
Without specialised help, selective and fear-based patterns often persist into adulthood. Emerging specialised psychological treatments show meaningful improvement in severity, variety, and weight where relevant, but the evidence base is earlier-stage than for AN/BN.[2][3][13] Poorer markers include long untreated duration, severe autism complexity without adapted supports, extreme medical compromise, and unaddressed family accommodation. Disposition: shared care with GP/paediatrics, dietetics follow-up, booster exposures, and clear medical safety-netting for weight loss, food refusal escalation, and cardiorespiratory symptoms.[12][16]
Special populations
Infants and young children. Growth charts, parent–child feeding dynamics, developmental feeding disorders interface, safeguarding when intake is severely limited.[10][16]
Adolescents. School meals, peer stigma, FBT adaptations, transition planning.[11][12]
Pregnancy. Fetal nutritional risk from extreme selectivity — obstetric–dietetic–psychiatric collaboration.[15]
Intellectual disability. Adapted communication, behavioural supports, capacity and best-interests frameworks for nutrition decisions.[13]
Cultural context. Distinguish culturally sanctioned diets from pathological restriction meeting ARFID criteria of deficiency/impairment.[15]
Evidence, guidelines and regional differences
Landmark pillars: Thomas three-dimensional model;[1] CBT-AR youth and adult proof-of-concept;[2][3] CBT-AR treatment overview;[4] PARDI development;[5] Fisher/Norris/Nicely/Ornstein descriptive cohorts;[6][7][8][9] Zimmerman clinical review;[10] Lock FBT adaptations;[11] Brigham adolescent evaluation/treatment;[12] Bourne scoping review;[13] NIAS subscale validation;[14] APA eating disorders practice guideline;[15] SAHM medical management of restrictive eating disorders;[16] RANZCP eating disorder guidelines;[17] Treasure Lancet overview.[18]
In Australian and New Zealand practice, use RANZCP eating disorder guidance principles for multidisciplinary specialist care, with paediatric and adult pathways depending on age and medical risk. Access to clinicians trained specifically in CBT-AR may be limited — adapt evidence-based CBT and FBT principles with dietetic partnership rather than offering non-specific counselling alone. Medical instability follows local MEED-informed / specialist ED medical protocols. Mental Health Act and guardianship frameworks for compulsory nutrition are jurisdiction-specific; assess capacity decision-specifically.[15][16][17]
Exam pearls
ARFID exam anchors
References
- [1]Thomas JJ, Lawson EA, Micali N, et al. Avoidant/Restrictive Food Intake Disorder: a Three-Dimensional Model of Neurobiology with Implications for Etiology and Treatment Curr Psychiatry Rep, 2017.PMID 28714048
- [2]Thomas JJ, Becker KR, Kuhnle MC, et al. Cognitive-behavioral therapy for avoidant/restrictive food intake disorder: Feasibility, acceptability, and proof-of-concept for children and adolescents Int J Eat Disord, 2020.PMID 32776570
- [3]Thomas JJ, Becker KR, Breithaupt L, et al. Cognitive-behavioral therapy for adults with avoidant/restrictive food intake disorder J Behav Cogn Ther, 2021.PMID 34423319
- [4]Thomas JJ, Wons OB, Eddy KT Cognitive-behavioral treatment of avoidant/restrictive food intake disorder Curr Opin Psychiatry, 2018.PMID 30102641
- [5]Bryant-Waugh R, Micali N, Cooke L, et al. Development of the Pica, ARFID, and Rumination Disorder Interview, a multi-informant, semi-structured interview of feeding disorders across the lifespan: A pilot study for ages 10-22 Int J Eat Disord, 2019.PMID 30312485
- [6]Fisher MM, Rosen DS, Ornstein RM, et al. Characteristics of avoidant/restrictive food intake disorder in children and adolescents: a "new disorder" in DSM-5 J Adolesc Health, 2014.PMID 24506978
- [7]Norris ML, Robinson A, Obeid N, et al. Exploring avoidant/restrictive food intake disorder in eating disordered patients: a descriptive study Int J Eat Disord, 2014.PMID 24343807
- [8]Nicely TA, Lane-Loney S, Masciulli E, et al. Prevalence and characteristics of avoidant/restrictive food intake disorder in a cohort of young patients in day treatment for eating disorders J Eat Disord, 2014.PMID 25165558
- [9]Ornstein RM, Rosen DS, Mammel KA, et al. Distribution of eating disorders in children and adolescents using the proposed DSM-5 criteria for feeding and eating disorders J Adolesc Health, 2013.PMID 23684215
- [10]Zimmerman J, Fisher M Avoidant/Restrictive Food Intake Disorder (ARFID) Curr Probl Pediatr Adolesc Health Care, 2017.PMID 28532967
- [11]Lock J, Robinson A, Sadeh-Sharvit S, et al. Applying family-based treatment (FBT) to three clinical presentations of avoidant/restrictive food intake disorder Int J Eat Disord, 2019.PMID 30578635
- [12]Brigham KS, Manzo LD, Eddy KT, Thomas JJ Evaluation and Treatment of Avoidant/Restrictive Food Intake Disorder (ARFID) in Adolescents Curr Pediatr Rep, 2018.PMID 31134139
- [13]Bourne L, Bryant-Waugh R, Cook J, Mandy W Avoidant/restrictive food intake disorder: A systematic scoping review of the current literature Psychiatry Res, 2020.PMID 32283448
- [14]Burton Murray H, Dreier MJ, Zickgraf HF, et al. Validation of the nine item ARFID screen (NIAS) subscales for distinguishing ARFID presentations and screening for ARFID Int J Eat Disord, 2021.PMID 33884646
- [15]Crone C, Fochtmann LJ, Attia E, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Eating Disorders Am J Psychiatry, 2023.PMID 36722117
- [16]Society for Adolescent Health and Medicine Medical Management of Restrictive Eating Disorders in Adolescents and Young Adults J Adolesc Health, 2022.PMID 36058805
- [17]Hay P, Chinn D, Forbes D, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of eating disorders Aust N Z J Psychiatry, 2014.PMID 25351912
- [18]Treasure J, Duarte TA, Schmidt U Eating disorders Lancet, 2020.PMID 32171414