Psych · General adult psychiatry — bipolar and related disorders
Bipolar affective disorder
Also known as Bipolar disorder · Bipolar I · Bipolar II · Manic-depressive illness · Mania · Hypomania · Rapid cycling bipolar · Mixed features · Cyclothymia
Exam-exhaustive fellowship reference on bipolar affective disorder — DSM-5-TR and ICD-11 definitions; bipolar I/II and cyclothymia; mixed features and rapid cycling; organic and personality differentials; acute mania and bipolar depression algorithms with doses; lithium monitoring and anti-suicide evidence; BALANCE, STEP-BD, BOLDER/EMBOLDEN, lamotrigine maintenance; perinatal care; RANZCP/NICE/CANMAT/APA deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Bipolar disorder is a high-weight fellowship topic because examiners test polarity thinking, not a unipolar depression template. You must define mania versus hypomania, recognise mixed features and rapid cycling, exclude organic and substance mimics, choose acute agents with doses and monitoring, defend lithium with levels and anti-suicide evidence, and navigate perinatal decisions without casual valproate. A FRANZCP MEQ will demand a formulated plan with risk and legal status; an MRCPsych CASC will test explanation of diagnosis and lithium to a family; an ABPN item will punish antidepressant monotherapy and mis-timed lithium levels.[13][14][15]
Overview and definition
Bipolar affective disorder is a chronic, recurrent mood disorder characterised by episodes of pathologically elevated or irritable mood with increased energy (mania or hypomania), usually alternating with major depression, and often with residual inter-episode symptoms. It is diagnosed clinically with operational criteria after substance and medical causes have been reasonably excluded. It is not “moodiness,” and it is not synonymous with borderline personality disorder — though comorbidity is common and examiners love the discrimination.[20]
Core episode definitions you must reproduce. Mania, hypomania and bipolar depression are operational constructs — duration and impairment separate the poles.[20][14]
- Manic episode (DSM-5-TR framing): Distinct period of abnormally and persistently elevated, expansive, or irritable mood and abnormally increased activity or energy, lasting at least 7 days (or any duration if hospitalisation is required), with marked impairment, psychosis, or need for hospitalisation. Symptom cluster includes grandiosity, decreased need for sleep, pressured speech, flight of ideas, distractibility, increased goal-directed activity or psychomotor agitation, and risky behaviour.[20]
- Hypomanic episode: Same pole direction but milder — at least 4 consecutive days, unequivocal change in functioning observable by others, not severe enough for marked impairment or hospitalisation, and without psychotic features. If psychosis is present, the episode is mania by definition.[20]
- Major depressive episode in bipolar illness: Same syndromal depression criteria as unipolar MDD (at least 2 weeks of core mood/anhedonia with associated symptoms), but management is not the same as unipolar care.[14]
ICD-11. Uses manic and hypomanic episode constructs with similar polarity logic; duration and severity thresholds should be stated with the manual you are using. First-rank psychosis language is not the gate for bipolar diagnosis — mood polarity and course are.[20]
Classification
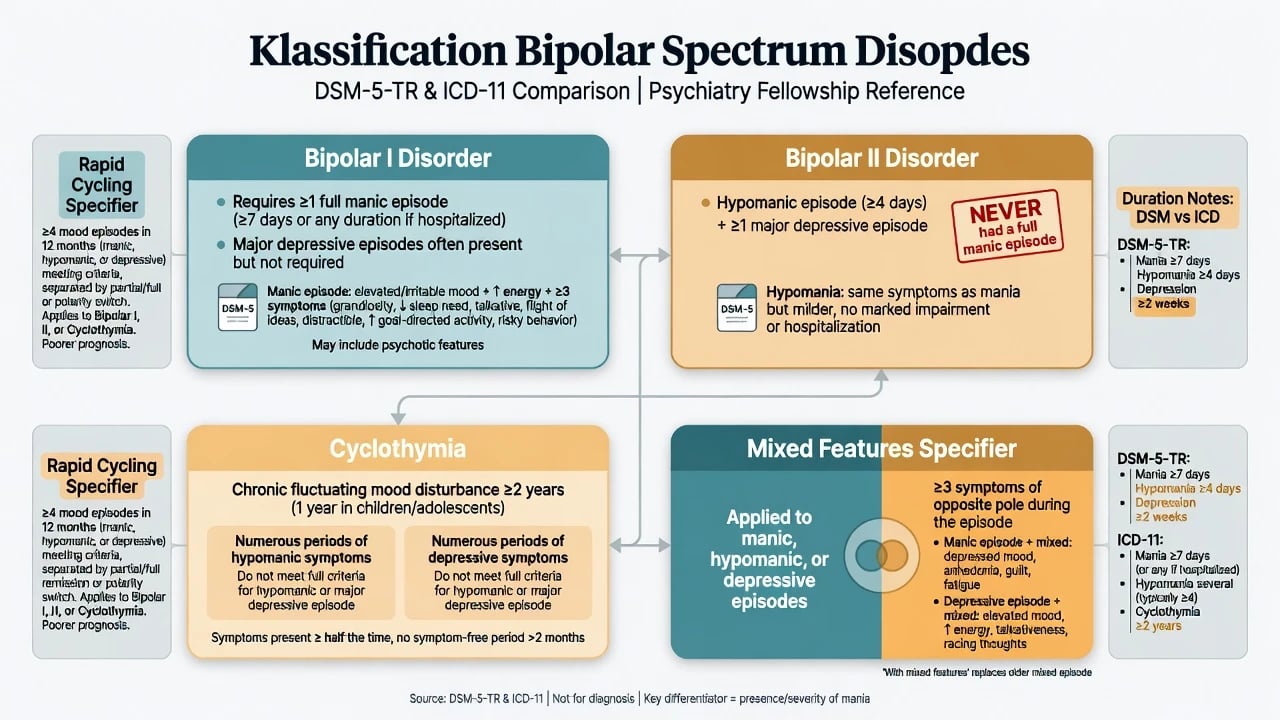
Bipolar I
- At least one manic episode required
- Major depression common but not required for diagnosis
- Psychosis may occur in mania or depression
- Highest hospitalisation and functional disruption risk
Bipolar II
- At least one hypomanic and one major depressive episode
- Never a full manic episode
- Often depression-predominant course
- Under-recognised when hypomania is pleasant or short
Cyclothymia
- Chronic fluctuating hypomanic and depressive symptoms
- Below full manic/major depressive thresholds for long periods
- DSM duration typically years of chronicity
- Can later declare into bipolar I/II
Course modifiers
- Mixed features: opposite-pole symptoms during an episode
- Rapid cycling: ≥4 distinct mood episodes in 12 months
- Seasonal pattern, peripartum onset, psychotic features
- Polarity predominance guides maintenance choice
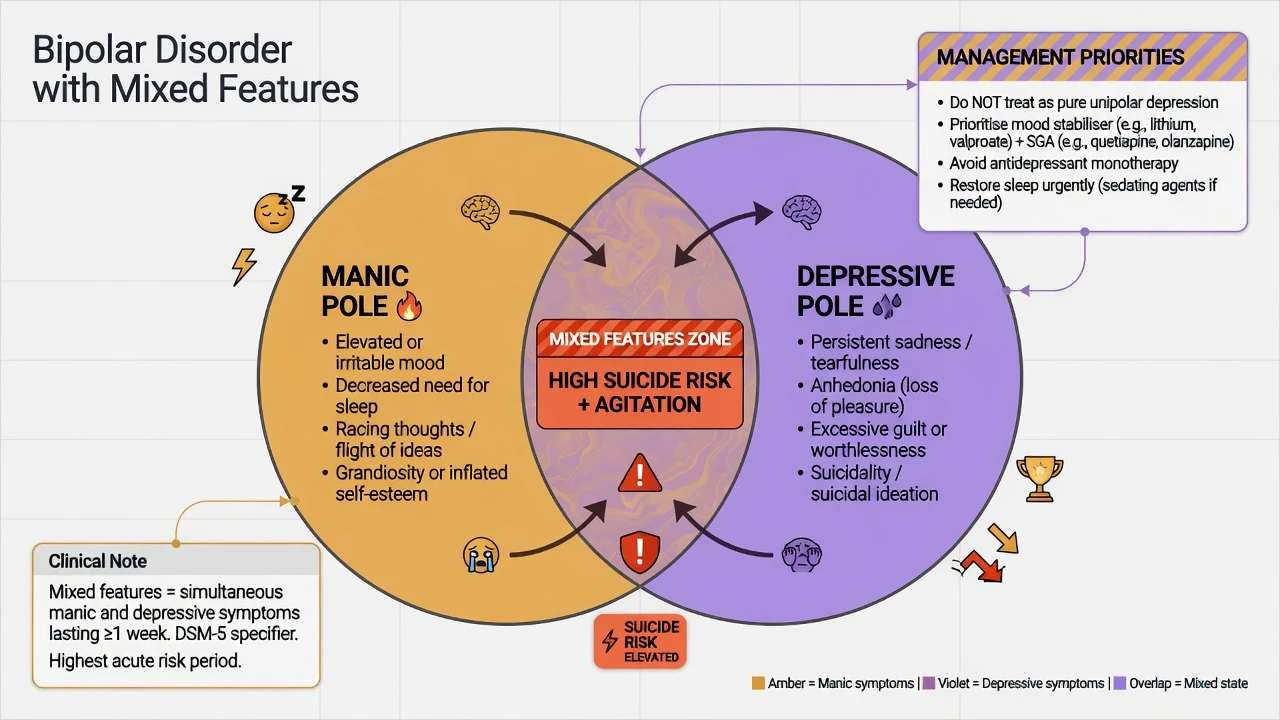
Mixed features (DSM-5-TR specifier). Replaces the older “mixed episode” construct for many exam purposes. During a manic/hypomanic episode, depressive symptoms (for example dysphoria, anhedonia, guilt, suicidality) may co-occur; during depression, manic symptoms (racing thoughts, increased energy, decreased sleep need, pressured speech) may co-occur. Mixed presentations carry high suicide risk and respond poorly to antidepressant monotherapy.[13][14]
Rapid cycling. At least four mood episodes meeting full criteria in a 12-month period, demarcated by full/partial remission or a switch in polarity. Associated with female sex in many series, antidepressant exposure, and thyroid dysfunction — treat the drivers, not only the label.[13][20]
Schizoaffective bipolar type interface. Mood episode concurrent with Criterion A psychosis plus delusions/hallucinations for a period without prominent mood symptoms, with mood symptoms present for the majority of total illness duration. Time-course documentation is the discriminator — not a single cross-sectional MSE.[20]
Epidemiology and risk factors
Headline numbers every candidate must own
World Mental Health Survey data show bipolar spectrum conditions are more prevalent than classical clinic estimates when subthreshold and bipolar II phenotypes are counted carefully.[18] Age of onset is typically adolescence or early adulthood; a first manic episode after mid-life is a classic prompt for intensified medical work-up.[20]
Risk and precipitants. Family history is the strongest non-modifiable risk. Modifiable or proximal triggers include sleep deprivation, stimulant or high-THC cannabis use, antidepressants (especially without mood-stabiliser cover), corticosteroids, postpartum hormonal/sleep upheaval, and severe psychosocial stress. None is necessary or sufficient.[20][14]
Mortality. Excess deaths relate to suicide, accidents, and cardiometabolic disease. Lithium’s association with reduced suicidal behaviour is a core evidence talking point, not a reason to ignore renal/thyroid monitoring.[3][17]
Pathophysiology
Bipolar pathophysiology is multi-level. Monoaminergic dysregulation (dopamine and noradrenaline tone in mania; serotonergic and broader network failure in depression) remains a practical pharmacology map. Circadian rhythm instability is both mechanism and clinical lever: delayed sleep phase, reduced sleep need in mania, and social-rhythm disruption predict relapse. Kindling/sensitisation language (earlier episodes more triggered, later more autonomous) is useful at viva depth if you avoid overclaiming it as proven in every patient.[20]
Lithium’s mechanisms are multi-target (second-messenger systems, GSK-3β inhibition, neurotrophic effects). Examiners reward this as explanatory pharmacology, not as a diagnostic test. Imaging and genetics provide group-level signals; they do not diagnose an individual on the ward.[20][17]
Clinical presentation
Mania — MSE viva language. Mood elevated, expansive, or irritable. Speech pressured, difficult to interrupt. Thought form accelerated with flight of ideas or clang associations. Content may be grandiose (“I am inventing a cure tonight”) or paranoid. Perception may include mood-congruent voices or no hallucinations. Cognition: distractible, poor judgement. Insight often impaired. Sleep: decreased need for sleep with preserved or increased energy — the single highest-yield early warning sign.[20]
Hypomania. The patient may feel better than well, more productive, charming, sexually activated, or irritable. Family notice spending, messages at 03:00, and unfinished projects. Because impairment is not catastrophic, bipolar II is frequently mislabelled as recurrent unipolar depression until a careful lifetime hypomania screen is done.[18][14]
Bipolar depression. May be indistinguishable cross-sectionally from unipolar MDD. Clues: earlier onset, highly recurrent course, postpartum episodes, family bipolar history, antidepressant-induced activation/switch, hypersomnia/leadened paralysis atypical features, and brief high-energy intervals buried in the history.[14][20]
Mixed features. The dangerous middle: racing thoughts with tearfulness, agitation with guilt, decreased sleep with suicidal intent. Do not treat as “agitated unipolar depression” with antidepressant alone.[13]
Differential diagnosis
Discriminators matter more than lists.[20][14]
| Mimic | Points toward mimic | Points toward primary bipolar |
|---|---|---|
| Stimulant/substance mania | Clear intoxication timeline; resolves with abstinence | Symptoms persist weeks after abstinence; premorbid polarity history |
| Steroid-induced | High-dose glucocorticoids; dose relationship | Episodes off steroids with classic course |
| Organic secondary mania | Age more than 40 first episode, focal neurology, seizure, cognitive plunge, systemic signs | Typical early onset, strong family history, recurrent polarity |
| ADHD | Trait childhood onset, continuous inattention, sleep need usually preserved | Episodic poles, decreased sleep need, grandiosity, clear euthymic intervals |
| Borderline PD | Minutes–hours affective shifts, interpersonal triggers, identity disturbance, self-harm pattern without true decreased sleep need | Days–weeks syndromal episodes meeting duration criteria; autonomous polarity |
| Schizophrenia spectrum | Psychosis outlasts mood; negative/cognitive core | Mood drives psychosis chronology; full inter-episode recovery more common |
| Unipolar MDD | No lifetime hypo/mania after careful collateral | Any clear hypomania/mania lifetime |
Organic differentials for first or atypical mania include hyperthyroidism, Cushing syndrome, MS, frontal lesions, HIV, neurosyphilis, autoimmune encephalitis, epilepsy, and delirium. Fluctuating attention means delirium until proven otherwise.[20][14]
Borderline vs bipolar II — exam care. Borderline affective instability is reactive, short-lived, and interpersonal. Hypomania is sustained (days), energy-driven, and often includes decreased sleep need. They can co-exist. Treat each problem that is present; do not force a single label to explain all instability.[14]
Clinical and bedside assessment
Structure the interview as polarity history + risk + capacity + collateral + medical exclusion.[14][15]
- Lifetime chart: first episode type and age; number of manias/hypomanias/depressions; psychosis; hospitalisations; postpartum; seasonality; antidepressant responses/switches; suicide attempts.
- Current episode: duration, sleep hours, spending, sexual risk, aggression, driving, childcare, online behaviour.
- MSE with quoted examples, not adjectives alone.
- Risk: suicide (intent, plan, means, mixed features, alcohol), violence, sexual disinhibition, financial/forensic harm, vulnerability, absconding, child protection interface.
- Capacity and legal status: understand, retain, weigh, communicate; least-restrictive care under local statute (do not invent section numbers for other jurisdictions).
- Collateral is often diagnostic in hypomania.
- Scales conceptually: YMRS for mania severity; MADRS/HAM-D for depression; CGI for global change. Mood charting and sleep diaries beat retrospective guesswork.[14][15]
Investigations
Before lithium, valproate, or an SGA, complete a safety baseline.[14][17]
- Bloods: FBC, U&E/eGFR, calcium, TFT, LFT, fasting glucose or HbA1c, lipids.
- ECG: especially if cardiac risk, older age, or QT-prolonging agents planned.
- Weight/BMI, BP, waist as metabolic baseline.
- Pregnancy test when relevant.
- Urine drug screen (supports, does not exclude, primary bipolar).
- CT/MRI, EEG, autoimmune panel when first/atypical mania, focal signs, seizure, or encephalitis features.[14][17]
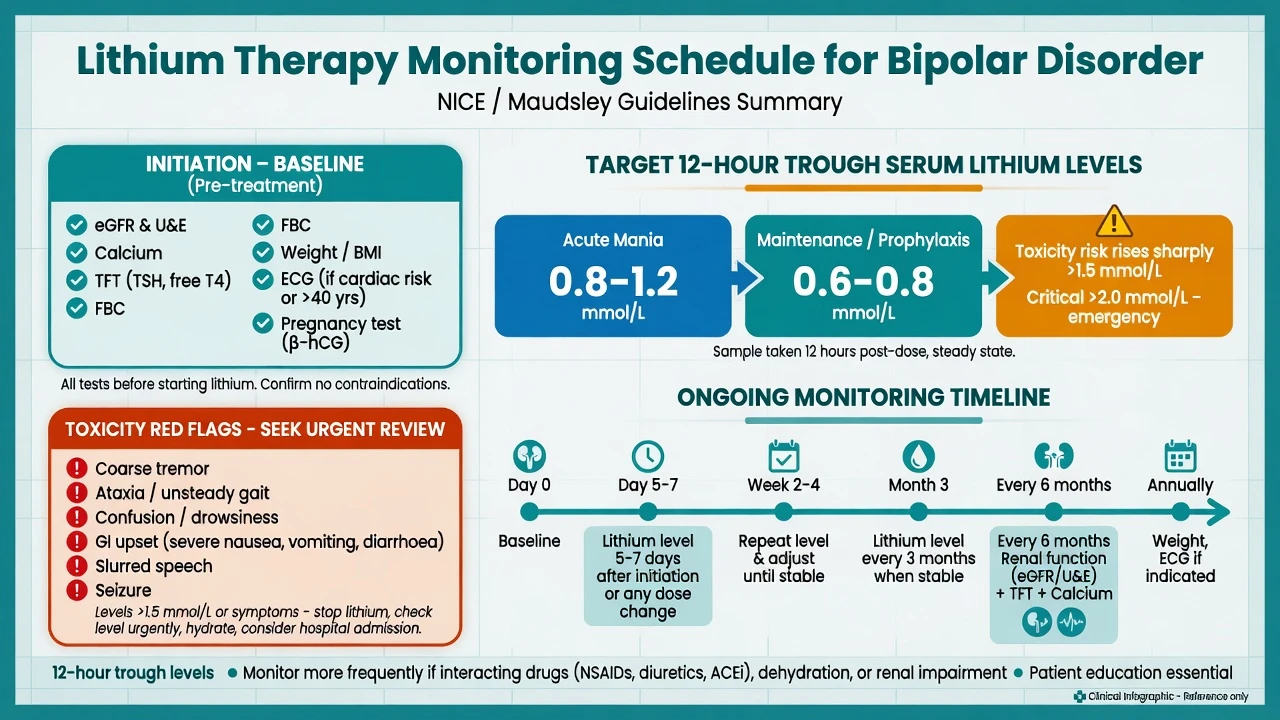
Lithium levels are 12-hour troughs after a steady evening dose. Acute mania targets are often in the 0.8–1.2 mmol/L region; maintenance commonly 0.6–0.8 mmol/L, individualised to response and tolerability. Toxicity risk rises substantially as levels climb above about 1.5 mmol/L; severe toxicity may present above 2.0 mmol/L. Check level 5–7 days after initiation or dose change, then periodically when stable, and after interacting drugs, dehydration, or renal change.[17][15]
Management — acute / emergency
Agitation ladder. De-escalate first. Offer oral medication before IM when safe. Short-term benzodiazepines (for example lorazepam) for arousal and sleep. Antipsychotic IM options per local protocol; avoid hazardous combinations (notably parenteral olanzapine with parenteral benzodiazepines in many safety frameworks). Document capacity and least-restrictive legal pathway.[14]
Lithium toxicity emergency. Stop lithium, check urgent level and renal function, IV fluids as indicated, cardiac monitoring, and higher-level care for severe neurotoxicity — dialysis pathway for life-threatening toxicity per medical toxicology. Common precipitants: NSAIDs, ACE inhibitors/ARBs, thiazides, dehydration, intercurrent illness.[17]
Management — definitive and stepwise
Acute mania algorithm
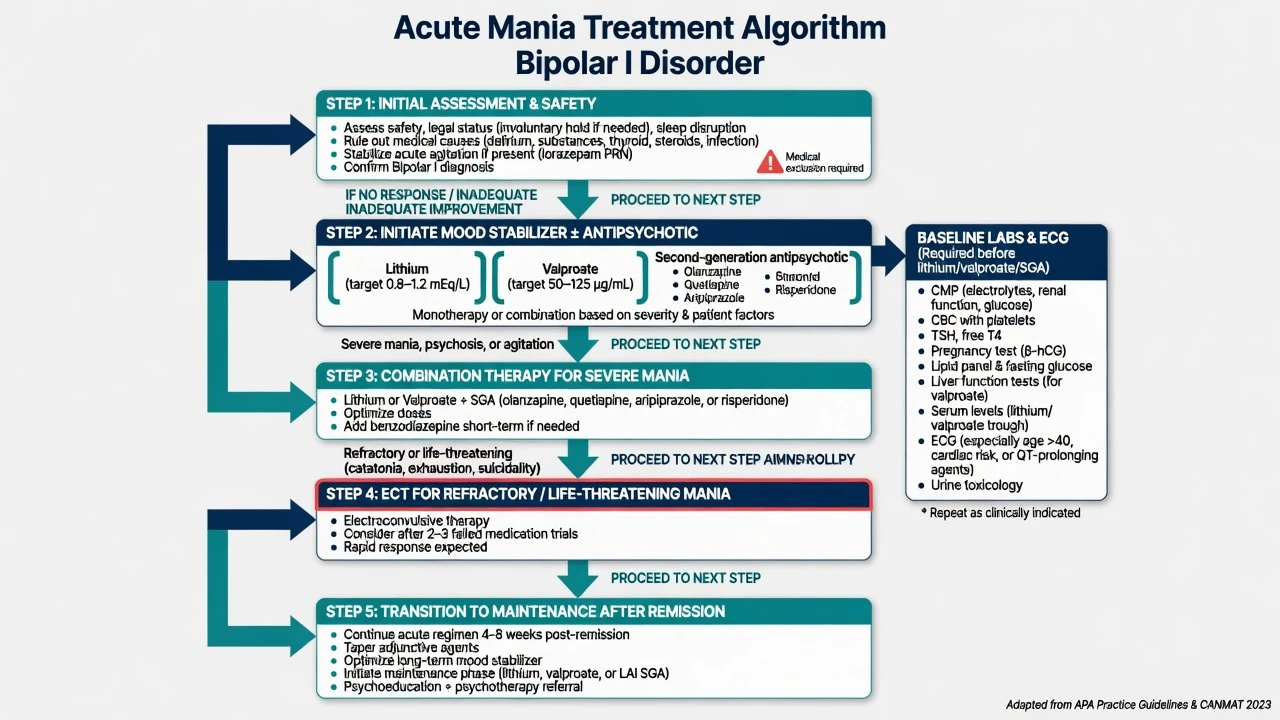
Network meta-analysis evidence supports multiple antimanic agents; ranking varies by efficacy and acceptability, with several SGAs, lithium, and valproate in the effective set.[4] Landmark divalproex versus lithium versus placebo mania data established anticonvulsant antimanic efficacy alongside lithium.[19] Aripiprazole has placebo-controlled acute mania evidence.[4]
Practical first-line options (adult, illustrative doses — always localise to product information and comorbidity). Antimanic agents with trial and guideline support include lithium, valproate and several SGAs.[4][13][19]
| Agent | Typical acute approach | Monitoring / notes |
|---|---|---|
| Lithium carbonate | Start often 400–800 mg/day in divided or night dosing; titrate to 12-hour trough | eGFR, TFT, calcium, level, ECG as indicated |
| Sodium valproate / divalproex | Loading strategies in mania where appropriate (e.g. about 20–30 mg/kg/day in divided doses in selected acute protocols) or standard titration to clinical response; many target levels roughly 50–100 mg/L (lab-specific) | LFT, FBC, pregnancy prevention absolute priority |
| Olanzapine | Often 10–20 mg oral daily (IM per protocol for agitation) | Metabolic panel, weight, sedation |
| Quetiapine | Mania doses commonly titrated toward 400–800 mg/day | Sedation, metabolic, BP |
| Aripiprazole | Often 15–30 mg oral daily in mania trials | Akathisia |
| Risperidone | Often 2–6 mg/day | Prolactin, EPS |
| Dose ranges are illustrative adult starting frameworks from guideline and trial practice — individualise and check local product information.[4][13][14][19] |
Severe mania frequently needs combination mood stabiliser + SGA. ECT remains highly effective for refractory, exhausted, catatonic, or life-threatening mania.[13][14][4]
Bipolar depression algorithm
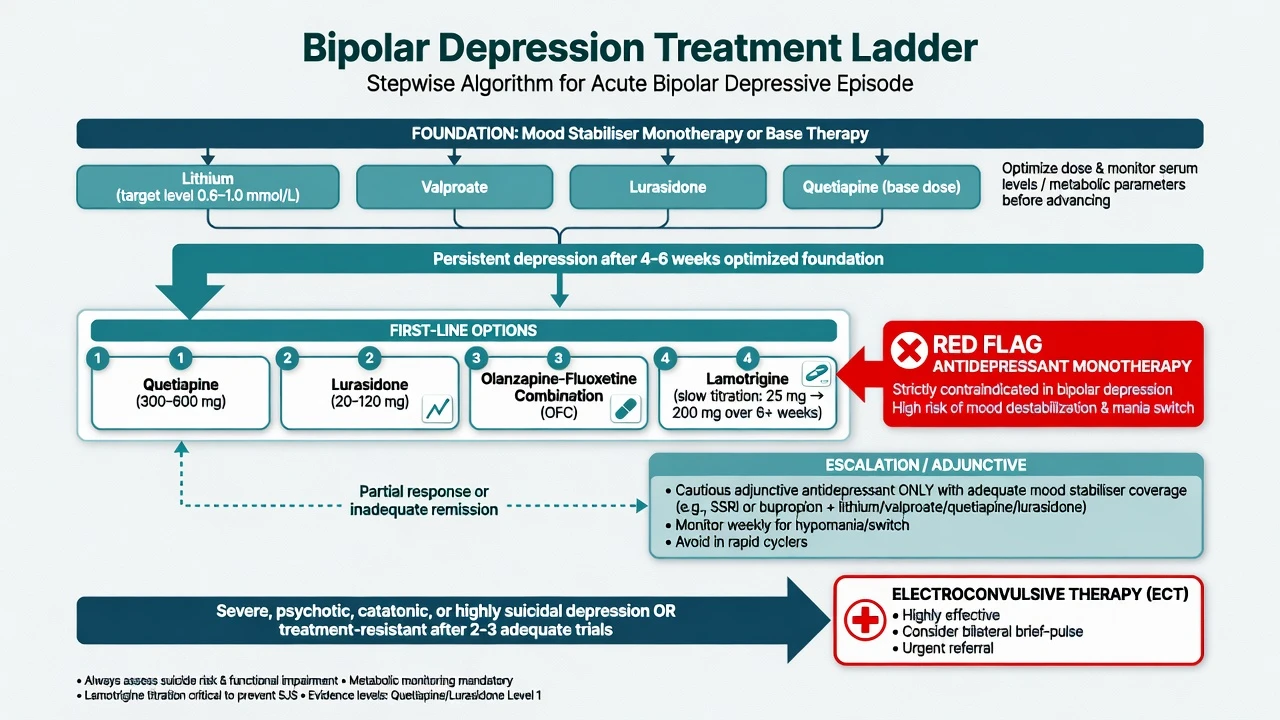
Evidence-backed options include the following polarity-safe pathways.[13][14]
- Quetiapine monotherapy: BOLDER and related trials support efficacy in bipolar I/II depression; common effective range 300–600 mg at night (titrate; metabolic burden).[6][7][8]
- Lurasidone monotherapy: 20–120 mg daily with food in bipolar I depression trials.[12]
- Olanzapine–fluoxetine combination (OFC): positive bipolar I depression data versus placebo; metabolic cost of olanzapine requires active monitoring.[9]
- Lamotrigine: stronger for maintenance depression prevention than as a fast acute antidepressant; acute effects are slower. Titrate carefully (classic adult schedule often 25 mg daily for 2 weeks, 50 mg for 2 weeks, then upward toward 200 mg/day as tolerated; slower with valproate, faster adjustments may apply with enzyme inducers — follow product guidance). Stop and urgent review for rash concerning for SJS/TEN.[10][11]
- Lithium: antisuicide and maintenance value; modest acute antidepressant effect in some data (EMBOLDEN compared quetiapine and lithium).[8][3]
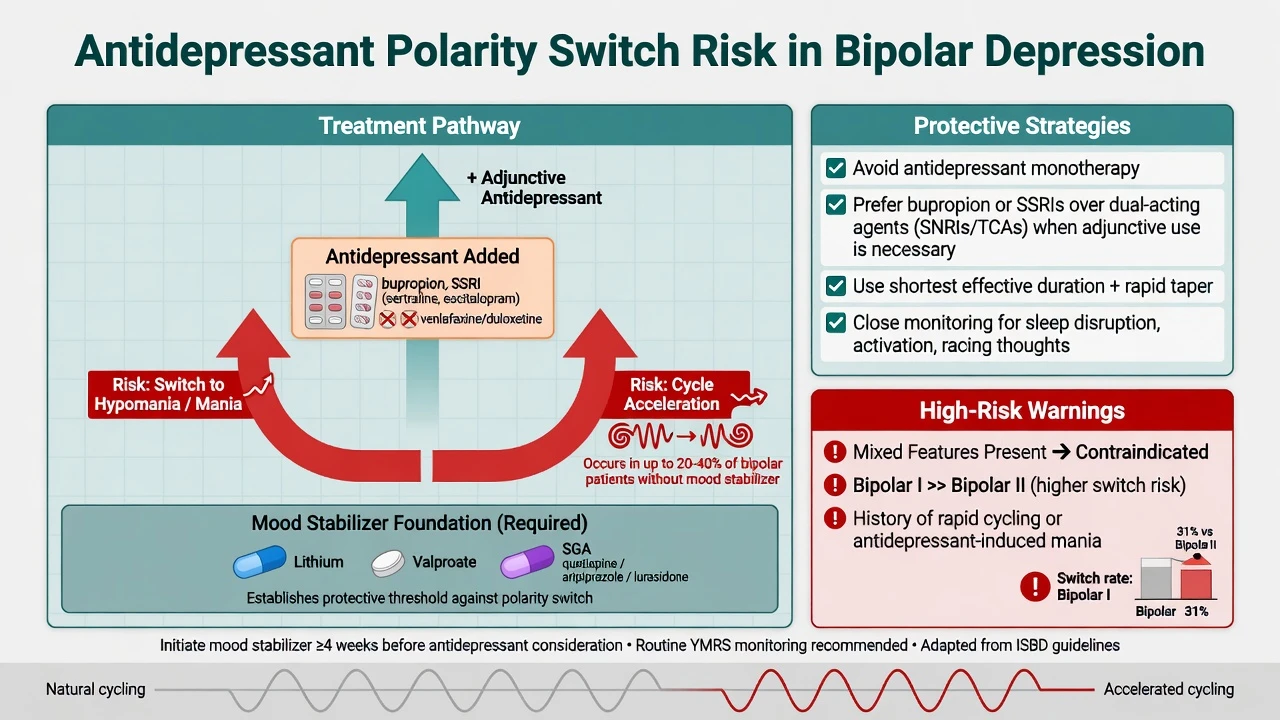
Antidepressants. STEP-BD found adjunctive antidepressants (paroxetine or bupropion) added to mood stabilisers did not outperform mood stabiliser plus placebo for durable recovery, a foundational challenge to casual antidepressant use.[2] Switch risk is higher with dual-acting agents in several analyses; if an antidepressant is used, cover with a mood stabiliser, avoid monotherapy in bipolar I, keep duration short, and monitor sleep/activation closely.[2][13]
Maintenance and relapse prevention
BALANCE (bipolar I relapse prevention) showed lithium monotherapy superior to valproate monotherapy, with combination lithium–valproate also effective; lithium remains a cornerstone when tolerated.[1] Network meta-analysis of maintenance treatments supports lithium among the most robust long-term options, with several SGAs and anticonvulsants in the comparative set depending on index pole and tolerability.[5] Lamotrigine’s maintenance signal is relatively stronger for delaying depressive recurrence; lithium covers both poles more evenly in classic data.[10][11]
Lithium practicalities. Educate on hydration, sodium balance, and interacting drugs. McKnight’s systematic review quantifies long-term renal, thyroid, and parathyroid risks — monitor rather than mythologise.[17] Cipriani meta-analysis supports lithium for suicide prevention in mood disorders — one of the few pharmacotherapies with this signal.[3]
Psychological and social care. Psychoeducation, interpersonal and social rhythm therapy (IPSRT), CBT adapted for bipolar disorder, and family-focused approaches reduce relapse risk as adjuncts to medication. Sleep regularity is a treatment, not lifestyle trivia. Address alcohol and stimulants aggressively.[13][14][15]
Specific subtypes and scenarios
First manic episode. Medical exclusion, risk, start antimanic therapy, decide legal status, begin psychoeducation, and plan at least 6–12 months of maintenance after a single mania in many guideline frameworks — longer if high risk, residual symptoms, or recurrent family pattern.[14][13]
Bipolar II depression-predominant. Screen carefully for hypomania. Quetiapine has bipolar II depression evidence; lamotrigine often used for recurrent depression prevention; still avoid reckless antidepressant monotherapy.[6][7][13]
Rapid cycling. Remove cycle accelerators (antidepressants, substances), correct thyroid disease, optimise lithium/valproate/SGA, consider lamotrigine for depression burden, and use mood charting. Evidence for any single “rapid-cycling drug” is weaker than for classic bipolar I maintenance — be honest at viva.[13][20]
Mixed features. Treat as bipolar spectrum high-risk state: SGA ± lithium/valproate, restore sleep, hold antidepressants, lower admission threshold.[13][14]
Complications and pitfalls
- Antidepressant monotherapy and unrecognised switch.
- Missing hypomania → years of failed “treatment-resistant depression” care.
- BPD/bipolar conflation in either direction.
- Lithium prescribed without interaction counselling (NSAIDs, ACEI/ARB, thiazides).
- Valproate exposure in pregnancy-capable patients without prevention programme.
- Metabolic syndrome from olanzapine/quetiapine ignored.
- Akathisia mislabelled as worsening mania or anxiety.
- Secondary mania missed in older adults.[14][17][2]
Prognosis and disposition
Most people have recurrent episodes; inter-episode recovery is possible but residual depressive symptoms and cognitive/functional gaps are common. Good prognostic factors include treatment adherence, absence of substance use, good premorbid function, and fewer mixed/rapid-cycling features. Disposition: admit for dangerous mania/mixed states, severe suicidality, psychosis with impaired judgement, or failed community containment. Step down with early-warning-sign plans, sleep targets, lithium/level logistics, and rapid re-access pathways.[20][5][3]
Special populations
Youth. Diagnostic caution for non-episodic chronic irritability (not automatically bipolar). Lithium has paediatric maintenance evidence in carefully selected bipolar I populations; specialist oversight required.[20]
Older adults. Higher rates of secondary mania; reduce lithium dose for renal clearance; watch delirium, falls, and polypharmacy interactions.[17]
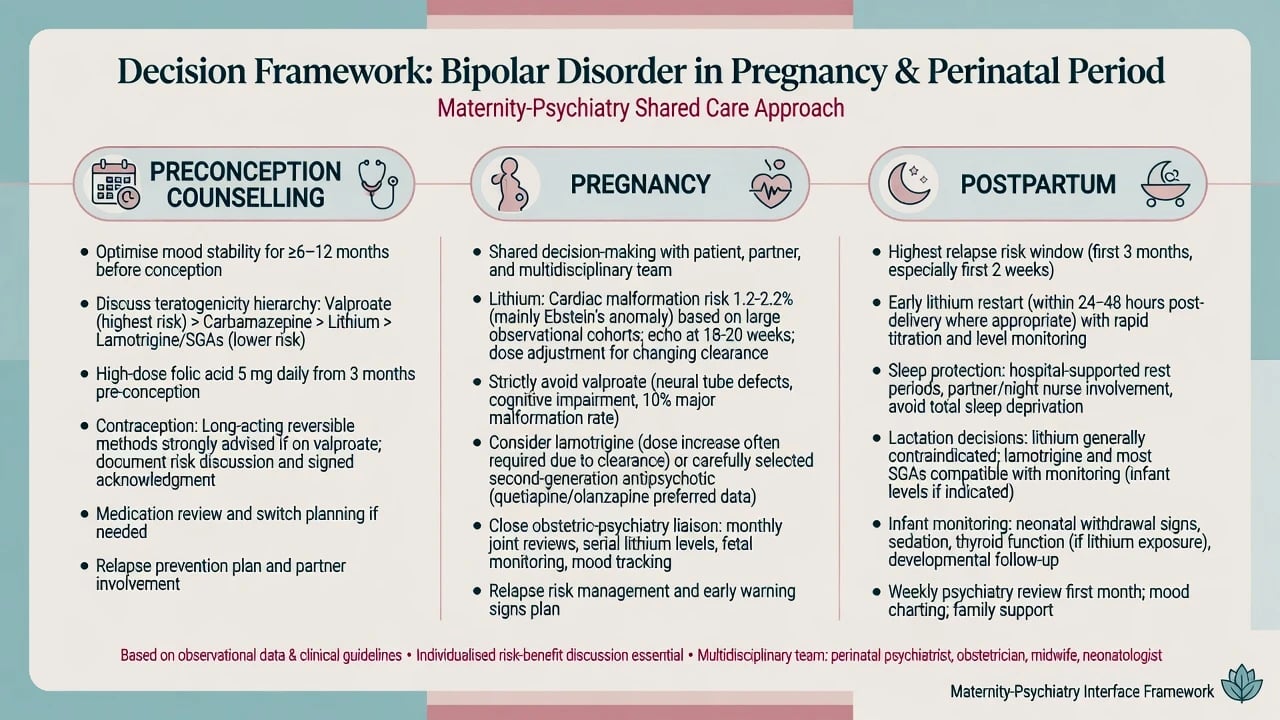
Pregnancy and postpartum. Preconception counselling is mandatory. Valproate sits at the top of the teratogenicity concern hierarchy (neural tube defects, neurodevelopmental harm) and is generally avoided. Lithium has a measurable increase in cardiac malformation risk in large observational data, but absolute risks are lower than older dogma implied — Patorno et al. inform a nuanced shared decision rather than automatic cessation in every stable patient.[16] Lamotrigine and selected SGAs are often considered. Postpartum is a peak relapse window: protect sleep, plan prophylaxis restart, and coordinate maternity–psychiatry care.[16][14][13]
Lactation. Lithium often avoided or used only with intensive infant monitoring in specialist settings; many prefer alternatives. Individualise with paediatric liaison.[14]
Evidence, guidelines and regional differences
RANZCP 2020 mood disorder guidance is the local fellowship anchor: formulation-based care, careful bipolar/depression differentiation, lithium retained as a core maintenance option, strong cautions on antidepressants and valproate in pregnancy-capable patients, and integrated psychological care.[14]
Landmark trials to name in the exam room. BALANCE (Li vs VPA vs combination); STEP-BD adjunctive antidepressants; BOLDER/EMBOLDEN quetiapine; OFC; lamotrigine maintenance twins/pooled analyses; Cipriani antimanic NMA; Miura maintenance NMA; Cipriani lithium–suicide meta-analysis; Patorno lithium–pregnancy cardiac malformations.[1][2][4][5][6][9][10][3][16]
Exam pearls
POLARITY — bipolar viva checklist
References
- [1]BALANCE investigators and collaborators, Geddes JR, Goodwin GM, et al. Lithium plus valproate combination therapy versus monotherapy for relapse prevention in bipolar I disorder (BALANCE): a randomised open-label trial Lancet, 2010.PMID 20092882
- [2]Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression N Engl J Med, 2007.PMID 17392295
- [3]Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104
- [4]Cipriani A, Barbui C, Salanti G, et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis Lancet, 2011.PMID 21851976
- [5]Miura T, Noma H, Furukawa TA, et al. Comparative efficacy and tolerability of pharmacological treatments in the maintenance treatment of bipolar disorder: a systematic review and network meta-analysis Lancet Psychiatry, 2014.PMID 26360999
- [6]Calabrese JR, Keck PE Jr, Macfadden W, et al. A randomized, double-blind, placebo-controlled trial of quetiapine in the treatment of bipolar I or II depression Am J Psychiatry, 2005.PMID 15994719
- [7]Thase ME, Macfadden W, Weisler RH, et al. Efficacy of quetiapine monotherapy in bipolar I and II depression: a double-blind, placebo-controlled study (the BOLDER II study) J Clin Psychopharmacol, 2006.PMID 17110817
- [8]Young AH, McElroy SL, Bauer M, et al. A double-blind, placebo-controlled study of quetiapine and lithium monotherapy in adults in the acute phase of bipolar depression (EMBOLDEN I) J Clin Psychiatry, 2010.PMID 20122369
- [9]Tohen M, Vieta E, Calabrese J, et al. Efficacy of olanzapine and olanzapine-fluoxetine combination in the treatment of bipolar I depression Arch Gen Psychiatry, 2003.PMID 14609883
- [10]Goodwin GM, Bowden CL, Calabrese JR, et al. A pooled analysis of 2 placebo-controlled 18-month trials of lamotrigine and lithium maintenance in bipolar I disorder J Clin Psychiatry, 2004.PMID 15096085
- [11]Calabrese JR, Bowden CL, Sachs G, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently depressed patients with bipolar I disorder J Clin Psychiatry, 2003.PMID 14628976
- [12]Loebel A, Cucchiaro J, Silva R, et al. Lurasidone monotherapy in the treatment of bipolar I depression: a randomized, double-blind, placebo-controlled study Am J Psychiatry, 2014.PMID 24170180
- [13]Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder Bipolar Disord, 2018.PMID 29536616
- [14]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [15]Goodwin GM, Haddad PM, Ferrier IN, et al. Evidence-based guidelines for treating bipolar disorder: Revised third edition recommendations from the British Association for Psychopharmacology J Psychopharmacol, 2016.PMID 26979387
- [16]Patorno E, Huybrechts KF, Hernandez-Diaz S Lithium Use in Pregnancy and the Risk of Cardiac Malformations N Engl J Med, 2017.PMID 28854098
- [17]McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis Lancet, 2012.PMID 22265699
- [18]Merikangas KR, Jin R, He JP, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative Arch Gen Psychiatry, 2011.PMID 21383262
- [19]Bowden CL, Brugger AM, Swann AC, et al. Efficacy of divalproex vs lithium and placebo in the treatment of mania. The Depakote Mania Study Group JAMA, 1994.PMID 8120960
- [20]Grande I, Berk M, Birmaher B, et al. Bipolar disorder Lancet, 2016.PMID 26388529