Psych · General adult psychiatry — bipolar and related disorders
Bipolar II disorder and cyclothymia
Also known as Bipolar II · BP-II · Hypomania · Cyclothymic disorder · Cyclothymia · Soft bipolar · Bipolar spectrum depression
Exam-exhaustive fellowship reference on bipolar II disorder and cyclothymia — hypomania versus mania thresholds, misdiagnosis as recurrent unipolar depression, antidepressant switch and cycle-acceleration risk, lamotrigine titration and depression-prevention role, quetiapine evidence in bipolar II depression (BOLDER/EMBOLDEN), STEP-BD antidepressant findings, cyclothymic disorder criteria, and RANZCP/NICE/CANMAT/BAP deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
3 MCQs with explanations
Target exams
Red flags
Bipolar II and cyclothymia are high-yield fellowship discriminators. Examiners test whether you can operationalise hypomania versus mania, catch years of misdiagnosed unipolar depression, defend lamotrigine’s maintenance role without pretending it is a rapid acute antidepressant, and refuse antidepressant monotherapy when polarity is known or highly likely. A FRANZCP MEQ will demand episode criteria, risk, and a dose-aware plan; an MRCPsych CASC will test family explanation of diagnosis and medicines; an ABPN stem will bury hypomania inside “productivity” and punish SSRI-only care.[11][12][13][14]
Overview and definition
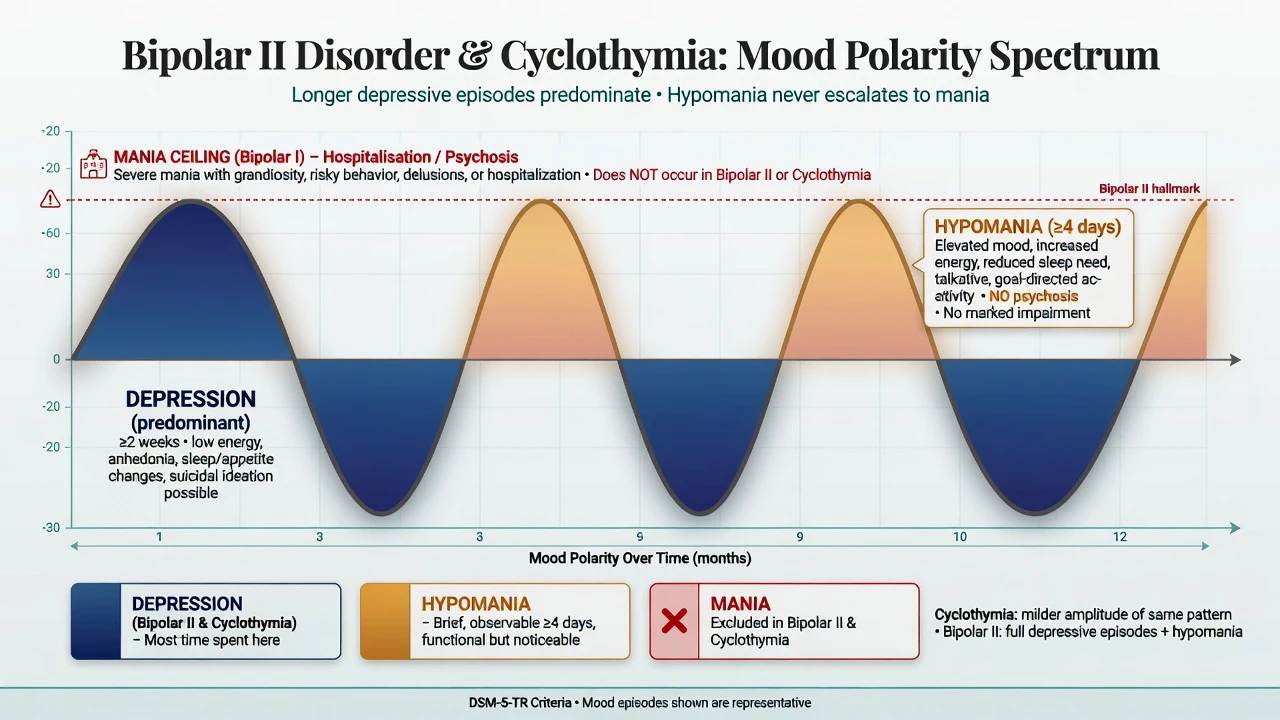
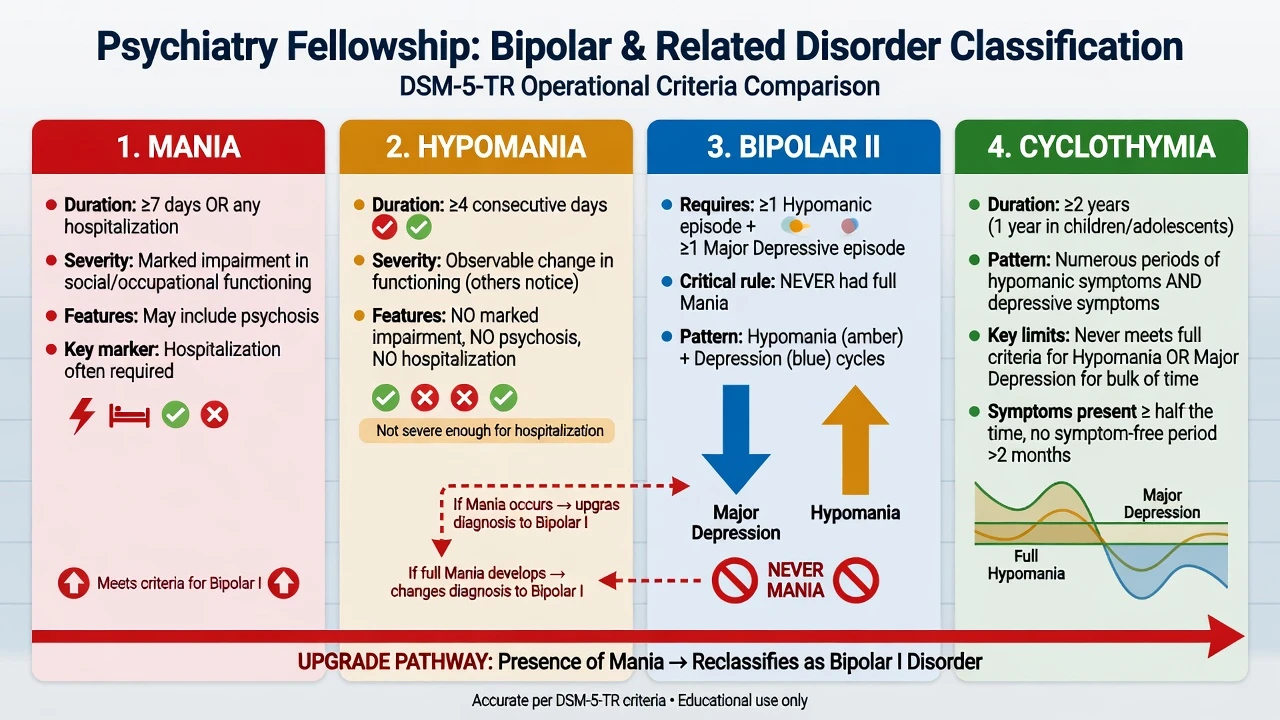
Bipolar II disorder (DSM-5-TR framing). Requires at least one hypomanic episode and at least one major depressive episode, with no lifetime manic episode. If a full manic episode ever occurs (including any elevated-pole hospitalisation, marked impairment meeting mania threshold, or psychosis), the diagnosis is bipolar I, not bipolar II. Bipolar II is not “mild bipolar” — depressive burden, residual symptoms, and suicide risk are substantial.[1][12][14]
Hypomanic episode. Distinct period of elevated, expansive, or irritable mood and increased activity or energy lasting at least 4 consecutive days, with unequivocal change in functioning that is observable by others, not severe enough for marked impairment or hospitalisation, and without psychotic features. Symptom cluster mirrors mania (grandiosity, decreased need for sleep, pressure, flight of ideas/racing thoughts, distractibility, increased goal-directed activity, risky behaviour) but intensity and consequence stay below the mania bar.[12][14]
Manic episode (the upgrade rule). Same pole direction lasting at least 7 days (or any duration if hospitalisation is required), with marked impairment, or psychotic features. Psychosis during an elevated pole makes the episode mania by definition. One lifetime mania reclassifies the illness to bipolar I forever for exam purposes.[12][14]
Cyclothymic disorder. For at least 2 years in adults (1 year in children/adolescents), numerous periods with hypomanic symptoms and numerous periods with depressive symptoms that do not meet full criteria for a hypomanic episode or major depressive episode for the bulk of the course; symptoms are present for at least half the time and never absent for more than 2 months at a stretch. If a full hypomanic, manic, or major depressive episode emerges and dominates the picture, reclassify (e.g. bipolar II or other specified bipolar) rather than keep forcing cyclothymia.[12][14]
ICD-11. Retains bipolar type II and cyclothymic disorder as polarity constructs. State which manual you are using; do not invent hybrid duration rules in the answer book.[14]
Classification
Mania
- ≥7 days or any hospitalisation
- Marked impairment and/or psychosis
- Defines bipolar I if ever present
- Needs acute antimanic intensity
Hypomania
- ≥4 consecutive days
- Observable change; not marked impairment
- No psychosis; no hospitalisation for the pole
- Core of bipolar II (with major depression)
Bipolar II
- ≥1 hypomania + ≥1 major depression
- Never full mania
- Depression usually dominates course
- High misdiagnosis as unipolar MDD
Cyclothymia
- ≥2 years adult subthreshold poles
- Never full hypomania or MDD bulk of time
- Symptoms ≥ half the time; gaps ≤2 months
- Reclassify if full episodes emerge
Epidemiology and risk factors
Headline numbers (exam anchors)
World Mental Health surveys reported aggregate lifetime prevalences around 0.6% bipolar I, 0.4% bipolar II, and higher rates when subthreshold bipolarity is included — the spectrum is clinically commoner than narrow BP-I alone.[1] Bipolar II is often recognised more in women and typically presents with depression first, so the elevated pole is missed until collateral history is taken years later.[1][14]
Risk and precipitants. Family history of bipolar spectrum, sleep deprivation, antidepressant exposure, stimulant or cannabis use, postpartum period, and seasonal change. Incomplete inter-episode recovery and comorbid anxiety or substance use amplify morbidity.[12][14]
Pathophysiology
Think circadian instability, monoamine and glutamate models, and kindling/sensitisation language at viva depth without claiming a single diagnostic biomarker.[14] Sleep loss is both trigger and early-warning sign for elevated poles. Iatrogenic pathophysiology matters for exams: antidepressants can precipitate transition into hypomania, mania, or mixed features and may accelerate cycling in vulnerable patients — treatment-cohort data support vigilance for activation during bipolar depression care.[4][16]
Cyclothymia sits on a continuum with bipolar spectrum vulnerability: chronic subthreshold polarity rather than discrete full episodes. Do not collapse it into “personality” without checking episode thresholds and sleep-need change.[12][14]
Clinical presentation
Hypomania (patient language). “I finally got things done,” “I only need three hours sleep and I feel great,” “I was witty and spent a bit more,” “Everyone said I was intense.” Family hears pressure, irritability, impulsive purchases, sexual risk, or project binges. The patient often values the episode and under-reports it; collateral is non-negotiable.[12][14]
Bipolar II depression. Longer, recurrent major depressions dominate the life chart. Atypical features (hypersomnia, leaden paralysis, rejection sensitivity) may appear but are not required. Residual depressive symptoms between poles are common and drive functional impairment even when hypomanias look “mild.”[1][14]
Cyclothymia. Years of ups and downs that never quite become full syndromal poles. Mood charts show frequent polarity without clear multi-week major depressions or true four-day hypomanias meeting full criteria. Euthymic stretches are short.[12][14]
Atypical and high-stakes presentations. Late recognition after multiple “failed” antidepressant trials; perinatal onset with sleep collapse; cultural expressions of elevated mood that look like entrepreneurship until collateral reveals decreased sleep need and risk behaviour.[12][14]
Differential diagnosis
Discriminators beat laundry lists.[12][14]
Discriminators for bipolar II and cyclothymia emphasise tempo, sleep need, and episode thresholds rather than single cross-sectional mood ratings. Recurrent unipolar MDD lacks lifetime hypomania after careful collateral; bipolar I is defined by any mania, psychosis, or elevated-pole hospitalisation; borderline PD shows minutes-to-hours shifts with interpersonal triggers; ADHD is a childhood-onset continuous trait; substance-induced elevation locks to the drug timeline; antidepressant activation starts after dose change without true decreased sleep need; persistent depressive disorder is chronic low mood without elevated poles; organic secondary elevation brings abnormal TFT, neurology, or mid-life first elevation.[12][14]
Organic causes of secondary elevation (hyperthyroidism, steroids, frontal lesions, autoimmune encephalitis, seizure-related mood) still need exclusion when the first elevated pole is late or atypical.[14]
Clinical and bedside assessment
Structure assessment as lifetime polarity chart + hypomania screen + suicide risk + medical exclusion + capacity.[11][12]
Assessment steps: build an episode inventory (first pole type, counts, durations, hospitalisations, psychosis, postpartum, seasonality, substance use, family history); run hypomania probes (sleep need, goal-directed bursts, spending, sexual risk, pressure, multi-day irritability, observability); take collateral from partner or family — the highest-yield manoeuvre for missed bipolar II; complete MSE with quoted content; assess suicide risk (intent, plan, means, mixed energy, alcohol, protective factors — bipolar II depression is not low-risk by default); apply capacity and least-restrictive local legal status principles without inventing foreign section numbers; and use prospective mood charts, MDQ as a screen not a diagnosis, and YMRS/MADRS conceptually when elevated or mixed features are suspected.[11][12][15]
Investigations
Before lithium, lamotrigine, valproate, or an SGA, complete a safety baseline.[12][17]
- Bloods: FBC, U&E/eGFR, calcium, TFT, LFT, fasting glucose or HbA1c, lipids.
- Weight/BMI, BP, waist circumference for metabolic baseline (especially before quetiapine).
- ECG if cardiac risk, older age, or QT-relevant polypharmacy.
- Pregnancy test when relevant.
- Urine drug screen supports formulation; does not exclude primary bipolar spectrum.
- Imaging/EEG/autoimmune work-up for first atypical elevated pole after mid-life, focal neurology, seizure, or encephalitis features.[12][14]
Lithium 12-hour troughs (if used): maintenance commonly about 0.6–0.8 mmol/L, individualised; check 5–7 days after initiation or dose change. Own renal, thyroid, and calcium monitoring long term.[15][17]
Lamotrigine has no therapeutic serum target for mood efficacy in routine practice — safety is titration discipline and rash protocol, not a level chase.[11][12]
Management — acute / emergency
Priority order for acute bipolar II crises. Safety first (suicide, violence, sexual disinhibition, financial harm, child protection), then medical exclusion and baselines, stop or carefully taper antidepressant monotherapy when it is driving activation or when bipolar spectrum is clear, restore sleep (short-term benzodiazepine per local protocol while cover starts), start polarity-safe pharmacotherapy, assess legal status if incapacitous with high risk, and engage family with a written early-warning plan before discharge.[11][12]
Management — definitive and stepwise
Acute bipolar II depression
Do not apply a unipolar antidepressant ladder as first logic.[4][11][12]
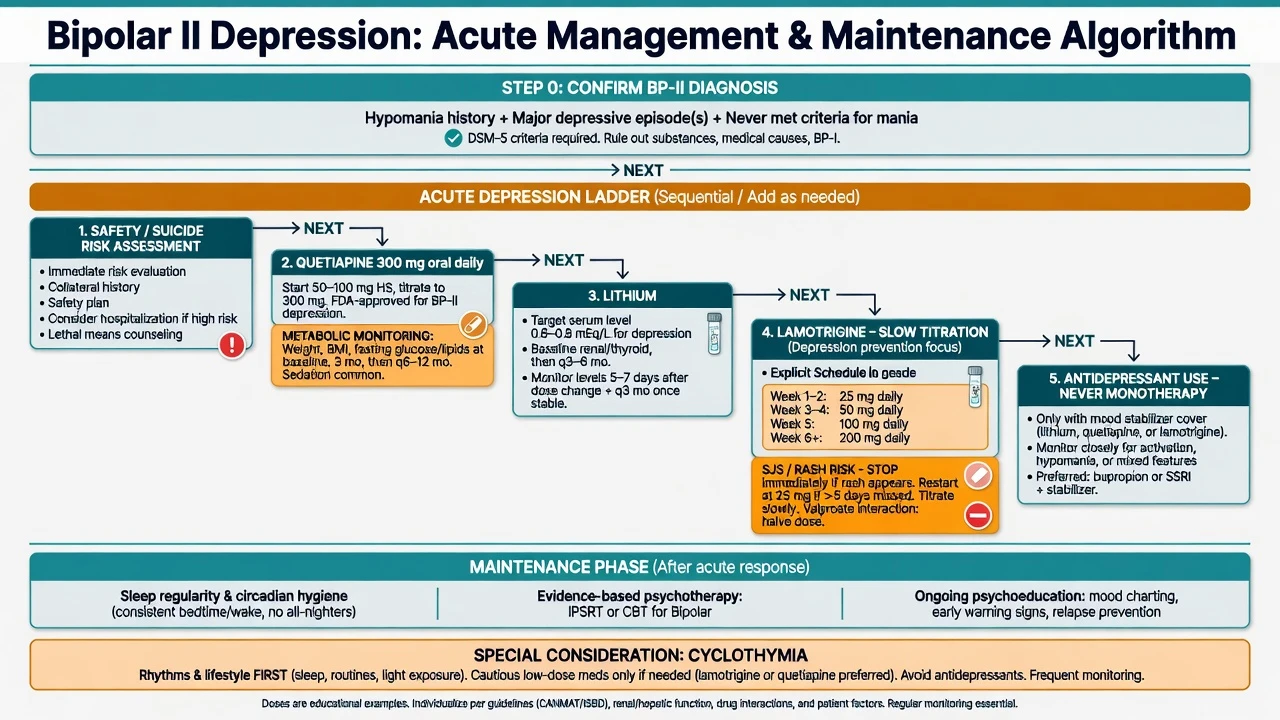
For acute bipolar II depression, polarity-safe frameworks include quetiapine commonly titrated toward 300 mg oral at night (trials also studied 600 mg) with metabolic monitoring; lithium often started at 450–900 mg/day with 12-hour trough individualisation; and lamotrigine slow titration (classic adult pattern 25 mg daily weeks 1–2, 50 mg weeks 3–4, then stepwise toward 100–200 mg/day maintenance targets, adjusted for valproate or enzyme inducers), with rash counselling and low restart after interruption more than about 5 days. Other SGAs (for example lurasidone where available) follow product information. Avoid antidepressant monotherapy; if an antidepressant is used at all, require mood-stabiliser or SGA cover, short duration, and daily early activation checks. Individualise to age, comorbidity, pregnancy potential, and local product information.[2][3][10][11][12]
Quetiapine evidence. BOLDER I demonstrated quetiapine efficacy in bipolar I or II depression at 300 and 600 mg/day versus placebo; BOLDER II replicated monotherapy benefit; EMBOLDEN programmes further support quetiapine in acute bipolar depression; pooled bipolar II analyses reinforce efficacy in the BP-II depressive pole.[2][3][10][18]
Lamotrigine role (exam precision). Strongest story is prevention of depressive relapse after stabilisation and slow titration, with classic maintenance trials and pooled lithium–lamotrigine analyses in bipolar I informing the class effect used clinically across bipolar spectrum depression-predominance; acute monotherapy results across five placebo-controlled trials were largely disappointing, so do not sell lamotrigine as a rapid acute antidepressant.[5][6][7][9] The rapid-cycling prophylaxis study is frequently cited for lamotrigine’s depression-pole signal, including bipolar II participants in that programme.[8]
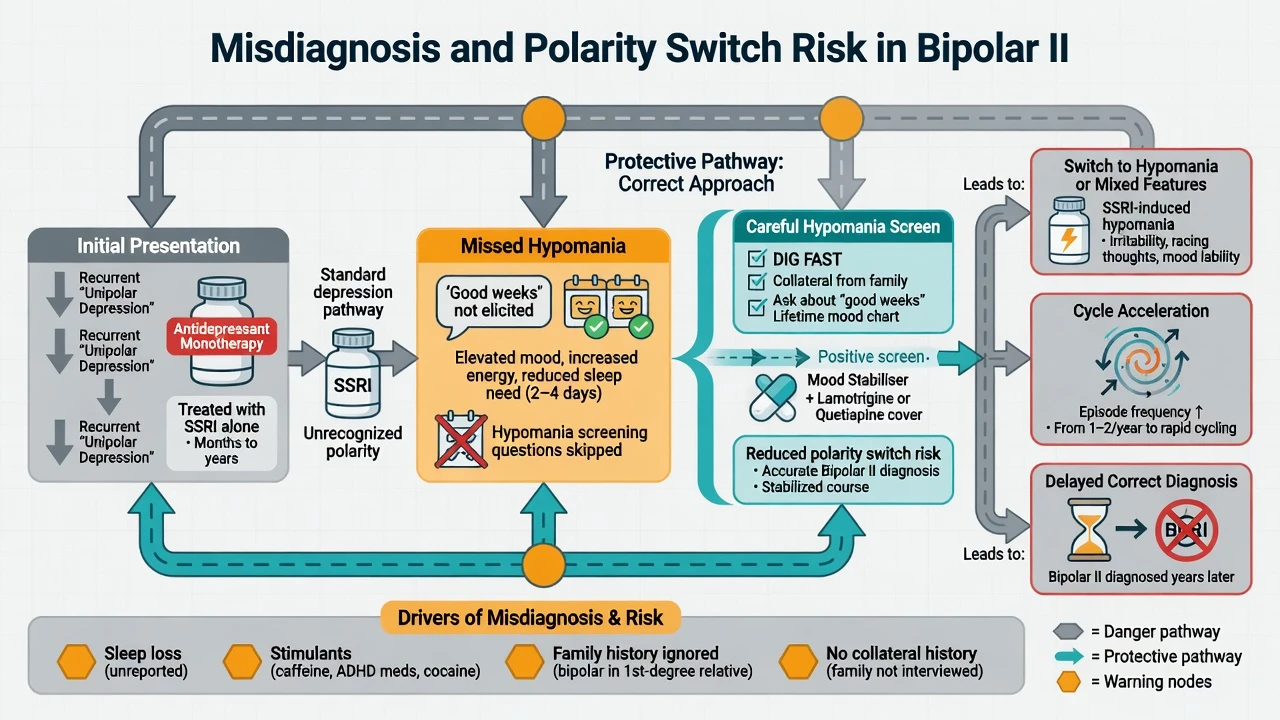
Antidepressant risk. STEP-BD found adjunctive antidepressants (paroxetine or bupropion) added to mood stabilisers did not outperform mood stabiliser plus placebo for durable recovery — foundational evidence against casual antidepressant use.[4] Transition-to-mania analyses during bipolar depression treatment reinforce monitoring for polarity switch.[16] If an antidepressant is used in highly selected bipolar II cases, cover with a mood stabiliser or SGA, keep duration short, and stop promptly if sleep need falls or activation appears.[4][11][12][16]
Maintenance and psychosocial care
- Continue the regimen that secured recovery into early maintenance, then simplify toward the best-tolerated preventive agent (often lamotrigine for depression-predominance, lithium when suicide risk or classic polarity warrants it and monitoring is feasible).[5][11][12][15]
- Lithium’s anti-suicide signal in mood disorders is highly relevant even when the current label is bipolar II.[15]
- Psychoeducation, IPSRT (interpersonal and social rhythm therapy), CBT for bipolar, and family-focused work — sleep regularity is a treatment, not a lifestyle aside.[11][12][13]
- Written early-warning signs with a named support person; crisis contacts; substance review.
Cyclothymia management
Prioritise psychoeducation, sleep–wake regularity, substance reduction, and mood charting. Pharmacotherapy is more cautious and individualised than for full bipolar II; avoid cascading antidepressant monotherapy for every dip. If full major depression or hypomania emerges, reclassify and treat to the new diagnosis.[11][12]
Regional deltas
ANZ / FRANZCP. RANZCP 2020 mood disorder guidance anchors polarity-safe care, careful diagnosis of bipolar spectrum depression, and structured long-term planning; lithium and evidence-based SGAs remain central tools.[12] UK / MRCPsych. BAP bipolar guidance and NICE-aligned pathways emphasise structured assessment, caution with antidepressants, and specialist bipolar pathways; document shared decisions on lamotrigine titration and monitoring.[13] US / ABPN. APA-framed practice punishes antidepressant monotherapy and rewards operational hypomania criteria, metabolic monitoring for quetiapine, and lamotrigine rash safety.[11] India / MD-DNB / NEET-SS. Expect DSM/ICD criteria, mania versus hypomania thresholds, lamotrigine titration numbers, and STEP-BD framing of antidepressant limits at viva.[4][11][12]
Specific subtypes and scenarios
First recognition after three failed antidepressants. Stop the unipolar template. Take collateral hypomania history. Start polarity-safe cover (e.g. quetiapine or lithium ± planned lamotrigine titration). Educate that “feeling better for a few high-energy days” may have been hypomania.[4][12]
Depression-predominant bipolar II long-term care. Lamotrigine maintenance logic, lithium if high suicide risk or classic polarity, quetiapine when residual depression or insomnia/agitation features dominate, relentless sleep regularity.[5][10][15]
Antidepressant-associated hypomania. Stop or taper the antidepressant, restore sleep, cover with mood stabiliser/SGA, and update diagnosis if full hypomanic criteria are met independently of ongoing intoxication.[4][16]
Cyclothymia with borderline traits. Use tempo, sleep need, and episode duration discriminators; formulate both if comorbid rather than forced choice.[12][14]
Pregnancy planning. Preconception counselling; valproate hierarchy of avoidance in people who can become pregnant; lithium decisions require specialist shared care and cardiac-risk counselling context; protect postpartum sleep.[12]
Older adults. Secondary causes of elevation, renally cautious lithium, lower SGA starts, fall and metabolic risk.[12][17]
Complications and pitfalls
- Years of misdiagnosed unipolar depression with antidepressant stacking.[1][4][12]
- Calling bipolar II “mild” and under-treating suicide risk.[1][15]
- Overcalling every good day hypomania — or undercalling clear four-day episodes with decreased sleep need.[12][14]
- Confusing borderline affective storms with bipolar II poles.[12]
- Lamotrigine rapid titration or full-dose restart after a gap — serious rash risk.[11][12]
- Chronic high-dose quetiapine without metabolic monitoring.[2][10]
- Lithium under-monitoring and interaction-precipitated toxicity (NSAIDs, ACEI/ARB, thiazides, dehydration).[17]
Prognosis and disposition
Bipolar II often follows a chronic, depression-dominant course with incomplete inter-episode recovery. Functional recovery lags syndromal recovery. Good prognostic factors include early correct diagnosis, adherence, sleep regularity, and low substance use; poor factors include delayed diagnosis, antidepressant-driven cycling, and heavy comorbidity.[1][12][14]
Disposition. Admit for high suicide risk, severe functional collapse, or escalating hypomania with inadequate supports. Intensive community follow-up after medication changes. Recovery goals include work, relationships, polarity charting, and a living crisis plan — not only a PHQ-9 score.[11][12]
Special populations
Youth. Irritability alone is not hypomania. Require duration, sleep-need change, and collateral. Family psychoeducation is essential; avoid premature lifelong labels without operational criteria, but do not ignore clear polarity.[12][14]
Perinatal. Depression and hypomania risk rise with sleep loss; protect sleep aggressively; medication choices need specialist perinatal psychiatry input.[12]
Older adults. Organic differential, drug interactions, lower starting doses, renal lithium caution.[12][17]
Intellectual disability and autism. Diagnostic overshadowing of polarity; use behavioural baselines and caregiver charts.[12]
Cultural care. Elevated mood may be framed as productivity or spiritual gift; still apply operational criteria with respectful formulation and access-aware care.[12]
Evidence and guidelines
Landmark anchors for exams: Merikangas WMH prevalence; BOLDER/EMBOLDEN quetiapine in bipolar depression including BP-II; STEP-BD adjunctive antidepressant null durable recovery finding; lamotrigine maintenance and acute-trial programme results; Calabrese rapid-cycling lamotrigine study; Cipriani lithium suicide meta-analysis; McKnight lithium long-term toxicity profile; CANMAT/ISBD 2018 hierarchies; RANZCP 2020 mood guidelines; BAP bipolar recommendations.[1][2][3][4][5][6][8][9][10][11][12][13][15][17][18]
Where evidence is thinner: large dedicated bipolar II maintenance head-to-heads, precise antidepressant choice when covered, and pharmacotherapy algorithms for pure cyclothymia — say so honestly in viva rather than inventing trials.[11][12]
Exam pearls
- Screen every recurrent depression for hypomania before the third antidepressant trial.[12]
- Patients call hypomania “the good weeks” — ask collateral about sleep need and spending.[12][14]
- Lamotrigine: slow titration; counsel rash; restart low after gap more than about 5 days; think prevention more than acute rescue.[5][9][11]
- Quetiapine 300 mg night pathway is a classic bipolar depression exam anchor (metabolic cost acknowledged).[2][3][10]
- Cyclothymia is years of subthreshold poles — not four full episodes in 12 months (that is rapid cycling).[12][14]
- Bipolar II is not mild: depression time and suicide risk dominate morbidity.[1][15]
Related topics
Cross-link bipolar II reading with the bipolar hub, mixed-features and rapid-cycling leaf, unipolar depression, treatment-resistant depression, borderline personality discriminators, and suicide-risk pathways as needed for exam depth.[12][14]
References
- [1]Merikangas KR, Jin R, He JP, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative Arch Gen Psychiatry, 2011.PMID 21383262
- [2]Calabrese JR, Keck PE Jr, Macfadden W, et al. A randomized, double-blind, placebo-controlled trial of quetiapine in the treatment of bipolar I or II depression Am J Psychiatry, 2005.PMID 15994719
- [3]Thase ME, Macfadden W, Weisler RH, et al. Efficacy of quetiapine monotherapy in bipolar I and II depression: a double-blind, placebo-controlled study (the BOLDER II study) J Clin Psychopharmacol, 2006.PMID 17110817
- [4]Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression N Engl J Med, 2007.PMID 17392295
- [5]Goodwin GM, Bowden CL, Calabrese JR, et al. A pooled analysis of 2 placebo-controlled 18-month trials of lamotrigine and lithium maintenance in bipolar I disorder J Clin Psychiatry, 2004.PMID 15096085
- [6]Calabrese JR, Bowden CL, Sachs G, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently depressed patients with bipolar I disorder J Clin Psychiatry, 2003.PMID 14628976
- [7]Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression J Clin Psychiatry, 1999.PMID 10084633
- [8]Calabrese JR, Suppes T, Bowden CL, et al. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder J Clin Psychiatry, 2000.PMID 11105737
- [9]Calabrese JR, Huffman RF, White RL, et al. Lamotrigine in the acute treatment of bipolar depression: results of five double-blind, placebo-controlled clinical trials Bipolar Disord, 2008.PMID 18271912
- [10]Young AH, Calabrese JR, Gustafsson U, et al. Quetiapine monotherapy in bipolar II depression: combined data from four large, randomized studies. Int J Bipolar Disord, 2013.PMID 25505677
- [11]Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder Bipolar Disord, 2018.PMID 29536616
- [12]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [13]Goodwin GM, Haddad PM, Ferrier IN, et al. Evidence-based guidelines for treating bipolar disorder: Revised third edition recommendations from the British Association for Psychopharmacology J Psychopharmacol, 2016.PMID 26979387
- [14]Grande I, Berk M, Birmaher B, et al. Bipolar disorder Lancet, 2016.PMID 26388529
- [15]Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104
- [16]Perlis RH, Ostacher MJ, Goldberg JF, et al. Transition to mania during treatment of bipolar depression Neuropsychopharmacology, 2010.PMID 20827274
- [17]McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis Lancet, 2012.PMID 22265699
- [18]Young AH, McElroy SL, Bauer M, et al. A double-blind, placebo-controlled study of quetiapine and lithium monotherapy in adults in the acute phase of bipolar depression (EMBOLDEN I) J Clin Psychiatry, 2010.PMID 20122369