Psych · General adult psychiatry — OCRD
Body dysmorphic disorder
Also known as BDD · Body dysmorphia · Dysmorphophobia · Imagined ugliness · Muscle dysmorphia · BDD-YBOCS · OCRD
Exam-exhaustive fellowship reference on body dysmorphic disorder — DSM-5-TR/ICD-11 OCRD criteria; insight spectrum including delusional beliefs; differentials vs OCD and eating disorders; BDD-YBOCS; high suicide risk; CBT with ERP-style exposures; high-dose SSRI (fluoxetine RCT), clomipramine selectivity, relapse prevention; cosmetic surgery harms; muscle dysmorphia. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Body dysmorphic disorder (BDD) is a high-yield general adult OCRD topic at the FRANZCP, MRCPsych, and ABPN interface. Examiners test recognition (patients hide symptoms), discriminators from OCD and eating disorders, the insight continuum including delusional beliefs, high suicidality, high-dose SSRI logic, specialised CBT with exposure and response prevention elements, and why cosmetic surgery fails as treatment. A candidate who reads only this topic should defend diagnosis, risk, and stepped care at consultant depth.[11][12][22]
Overview and definition
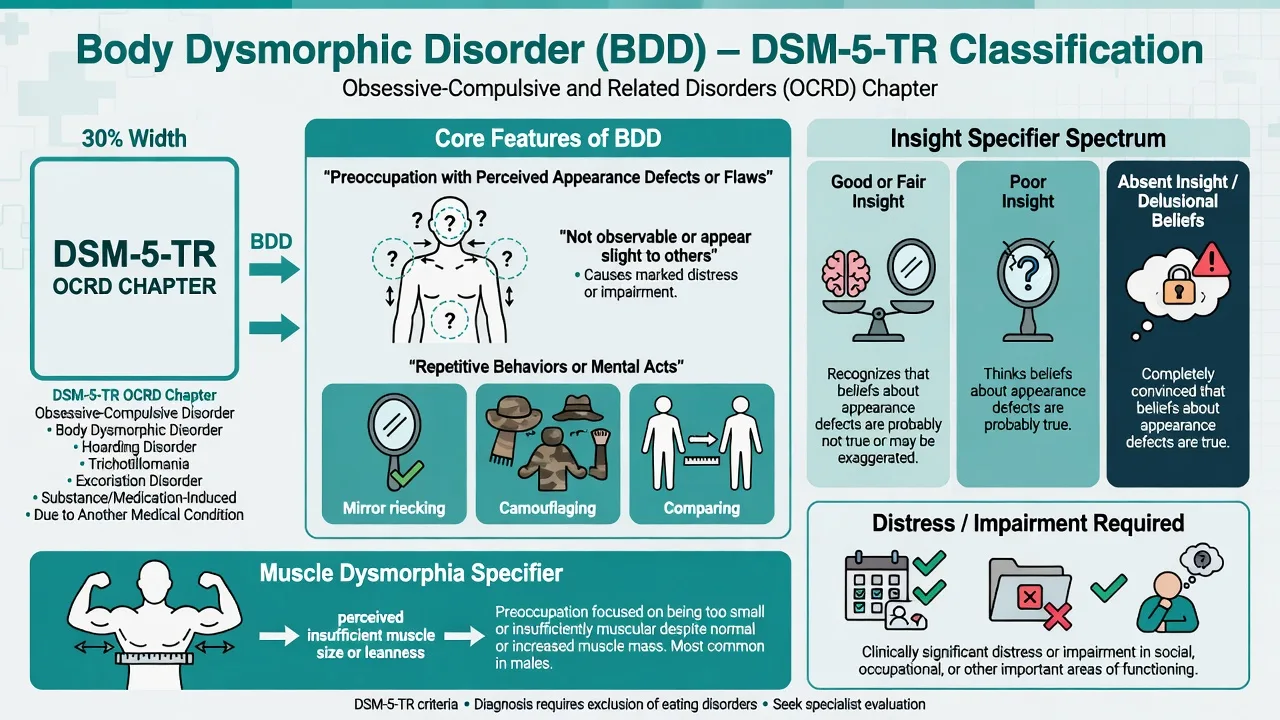
BDD is defined by preoccupation with one or more perceived defects or flaws in physical appearance that are not observable or appear slight to others, accompanied by repetitive behaviours or mental acts (mirror checking, excessive grooming, camouflaging, comparing, skin picking, seeking reassurance or cosmetic procedures) in response to the appearance concerns, with clinically significant distress or impairment, not better explained by an eating disorder or another mental disorder.[12][21][22]
Clinical essence for viva. The defect is overvalued or delusional in conviction but the core process is OCRD: intrusive appearance-focused attention, shame/anxiety, and safety behaviours that prevent disconfirmation. Patients often present with depression, social anxiety, or “OCD,” and will not volunteer BDD unless asked specifically about appearance rituals.[12][22]
DSM-5-TR placement. BDD sits in the obsessive-compulsive and related disorders (OCRD) chapter with OCD, hoarding, trichotillomania, and excoriation disorder. Insight is specified (good/fair; poor; absent insight/delusional beliefs). A muscle dysmorphia form describes preoccupation with the idea that one's body build is too small or insufficiently muscular.[12][21]
ICD-11. Body dysmorphic disorder is classified among obsessive-compulsive or related disorders with analogous core features; always state which manual you are using when insight or related-disorder boundaries are examined.[12]
Classification, insight and symptom map
Core BDD features
- Perceived defect(s) slight or invisible to others
- Preoccupation that is time-consuming
- Repetitive checking, camouflage, comparing, grooming
- Distress or functional impairment required
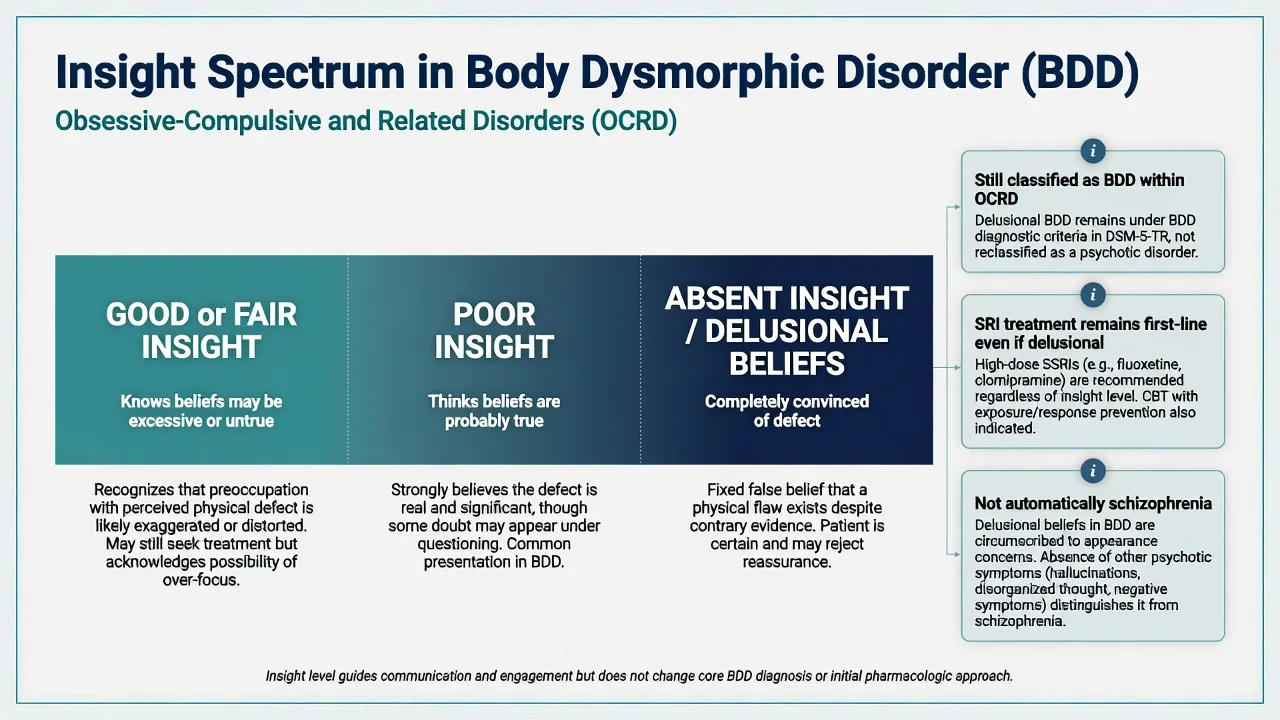
Insight specifier
- Good/fair: knows beliefs may be excessive
- Poor: thinks beliefs are probably true
- Absent/delusional: convinced of the defect
- Delusional insight still treated primarily as BDD with SRI
Common foci
- Skin, hair, nose, face symmetry
- Genitals, breasts, teeth
- Multiple body areas common
- Muscle size/definition (muscle dysmorphia)
Safety behaviours
- Mirror checking or mirror avoidance
- Camouflage (hats, makeup, posture)
- Comparing to others/photos/social media
- Cosmetic seeking and reassurance
Insight is poorer on average in BDD than in OCD — a key comparative finding that drives misdiagnosis as psychosis when the examiner is not careful.[13][14]
Epidemiology and risk factors
Headline epidemiology (exam numbers)
Population-based surveys place current BDD prevalence around 1.7–2.4% in adults, with elevated suicidal ideation and attempts relative to comparison groups.[17][18] Specialty settings (cosmetic dermatology, plastic surgery, orthodontics) show higher rates — consultation-liaison screening is examinable.[19][22]
Suicide risk is not optional content. Clinical series document very high lifetime suicidal ideation and attempts; prospective data support elevated suicidality burden. Always perform structured risk assessment at presentation and major reviews, and treat comorbid depression actively.[15][16]
Common comorbidities: major depression, social anxiety disorder, OCD, substance use disorders, eating disorders, and personality pathology. Formulate each, do not collapse everything into one label.[12][14]
Pathophysiology and maintaining model
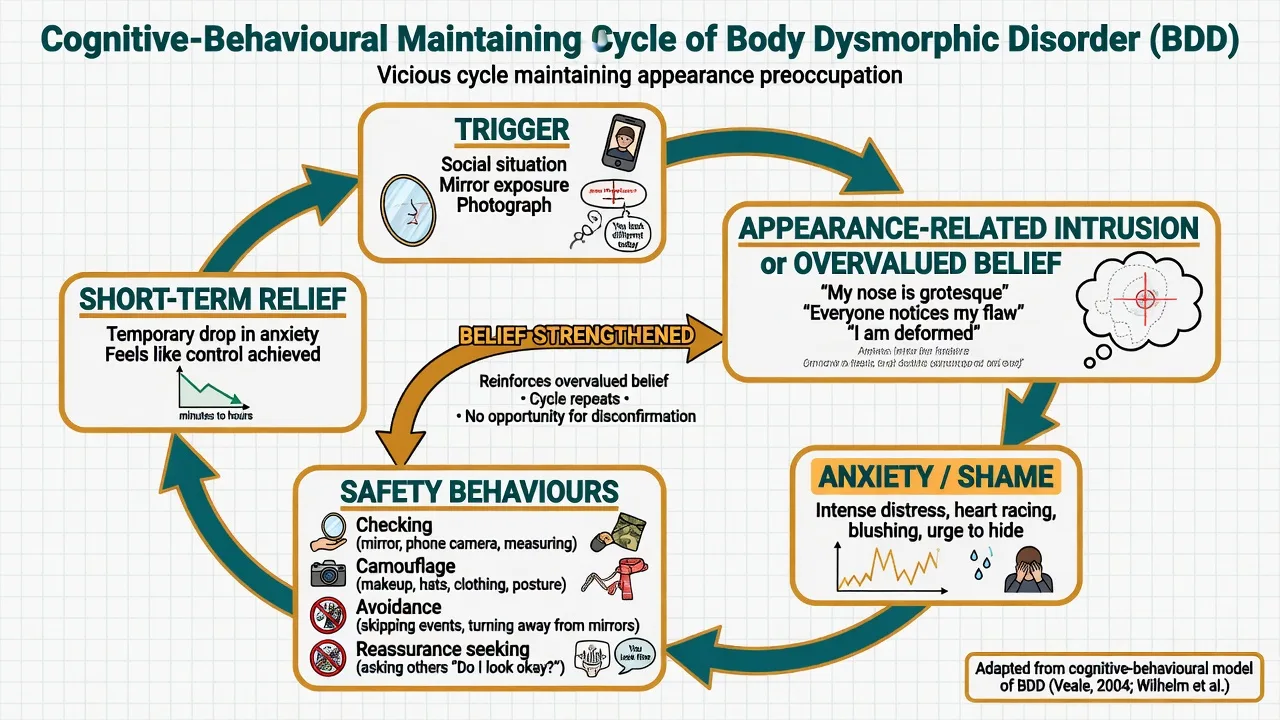
Cognitive-behavioural model (viva-ready). Selective attention to appearance, over-interpretation of minor features as catastrophic defects, and safety behaviours (checking, camouflaging, avoidance, reassurance) prevent disconfirmation and maintain shame. Social media comparing can intensify monitoring without being the sole cause.[5][12]
Serotonergic treatment model. Fluoxetine is superior to placebo for BDD symptoms on BDD-YBOCS, and clomipramine is superior to the noradrenergic TCA desipramine in a crossover design — supporting SRI pharmacology similar to OCD rather than a nonspecific “any antidepressant” story.[2][3][23] Response is often delayed and favours higher doses and longer trials than typical depression care.[11][24]
OCRD circuitry framing. Shared teaching with OCD (cortico-striato-thalamo-cortical loops) is acceptable at exam level; imaging is not diagnostic for the individual patient.[12]
Clinical presentation
Patients may spend hours daily on appearance rituals, avoid dating/work/school, use heavy camouflage, or seek endless cosmetic opinions. Covert mental comparing and reviewing photos count as rituals. Ideas or delusions of reference (“people are staring at my nose”) are common and do not alone prove schizophrenia.[12][22]
Muscle dysmorphia. Predominantly male-leaning phenotype of BDD: preoccupation with insufficient muscularity despite normal or large muscle mass; excessive weightlifting, dietary extremes, mirror checking, and risk of anabolic-androgenic steroid (AAS) use and related medical harm.[20]
Atypical traps. Late first onset, focal neurology, or marked cognitive change — do not assume idiopathic BDD; consider organic differentials. Adolescent onset with social media intensification is common but still requires full risk and differential assessment.[12]
Differential diagnosis
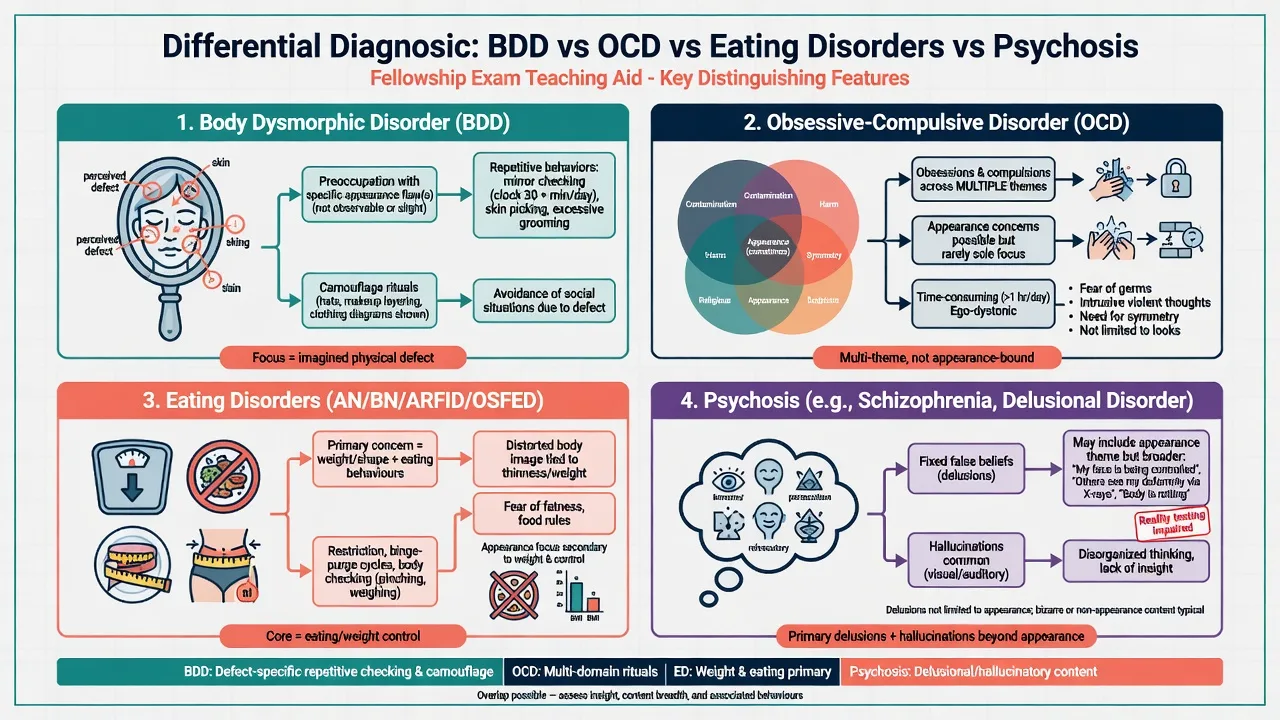
OCD
- Obsessions/compulsions across contamination, harm, symmetry, forbidden thoughts
- Not limited to appearance
- Can co-occur with BDD — treat both content streams
- Insight often better than BDD on average
Eating disorders
- Primary drive is weight, shape fatness, and eating control
- BDD defects often skin/hair/nose not solely weight
- Can co-occur — formulate both
- Do not treat AN with BDD protocol alone
Psychosis
- Primary delusions beyond appearance, hallucinations, thought disorder
- BDD with absent insight still has compulsive appearance logic
- SRI remains first-line for delusional BDD
- Antipsychotic monotherapy is not BDD first-line
Social anxiety
- Fear of negative evaluation for social performance
- BDD fear is of being seen as deformed
- Overlap common — appearance exposure differs from pure social exposure
- Camouflage and mirror rituals favour BDD
Also discriminate normal appearance concern without clinical impairment, gender dysphoria (identity incongruence vs cosmetic defect fixation — do not conflate), illness anxiety, and OCRD neighbours (excoriation, trichotillomania) that may co-exist with BDD picking/grooming.[12][14][21]
Clinical and bedside assessment
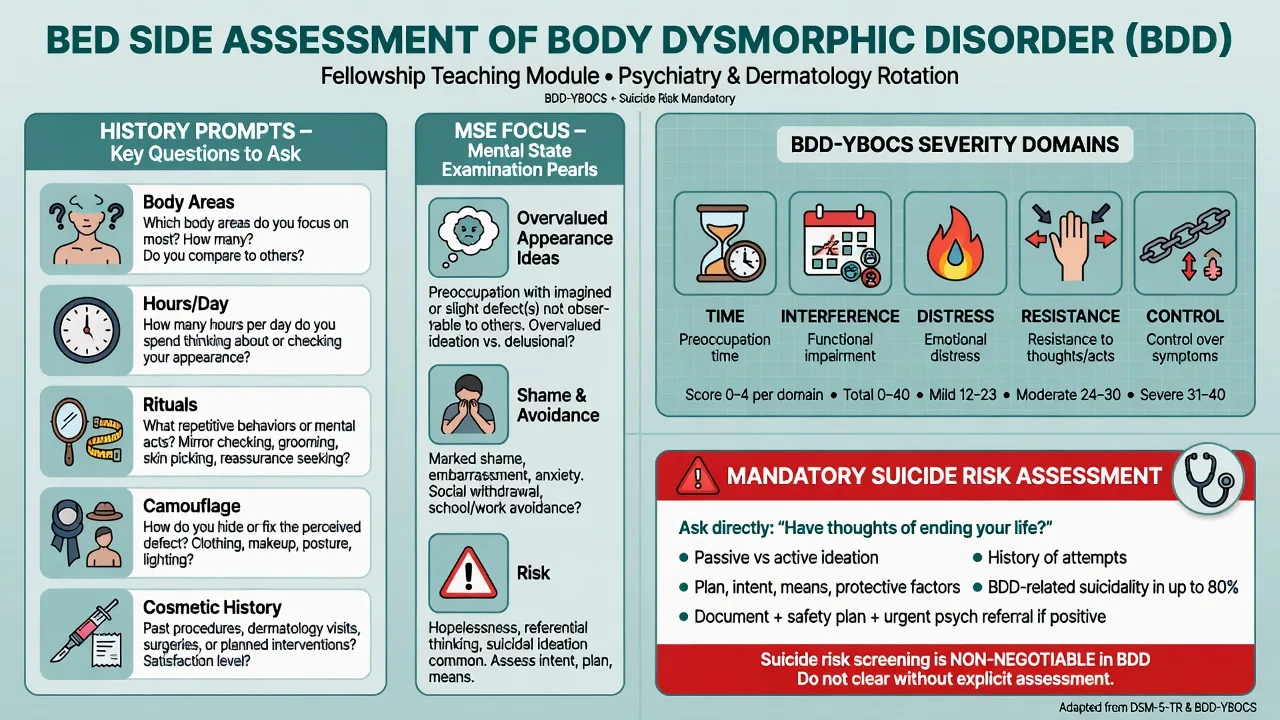
History structure. Onset and course; body areas and hierarchy of concern; hours per day; rituals (checking, camouflage, comparing, picking); avoidance; prior cosmetic procedures and outcomes; insight; substances/AAS; family accommodation and reassurance; functional impact; prior treatment adequacy (dose, duration, whether true CBT-BDD/ERP).[11][12]
MSE. Appearance-related overvalued ideas or delusional conviction; affect (shame, depression, anxiety); risk to self; absence of primary thought disorder/hallucinations when claiming delusional BDD.[13][22]
BDD-YBOCS. The Yale–Brown Obsessive Compulsive Scale modified for BDD is a clinician-rated severity measure (parallel structure to Y-BOCS across time, interference, distress, resistance, and control domains). It tracks severity and response; it does not diagnose alone.[1]
Risk. Structured suicide assessment every major contact. Appearance-related self-harm and DIY “surgery” are psychiatric emergencies.[15][16]
Investigations and measurement-based care
No biomarker diagnoses idiopathic BDD. Obtain baseline labs and ECG as indicated before high-dose SSRI or clomipramine; pregnancy test when relevant. Medical/dermatologic liaison is appropriate when picking creates lesions or true medical disease needs exclusion — without colluding in endless cosmetic investigation.[11][23]
Serial BDD-YBOCS (or equivalent) plus depression and risk measures support measurement-based care.[1][11]
Management — acute risk and resuscitation
Manage SSRI-related activation, hyponatraemia, and serotonin syndrome risk with polypharmacy on medical pathways as indicated. Clomipramine overdose risk includes seizures and arrhythmia — cardiac monitoring and toxicology pathways apply.[23][24]
Capacity and Mental Health Act decisions are jurisdiction-specific; state principles of capacity, least restrictive care, and when compulsory treatment may apply for high-risk incapacity without inventing section numbers across countries.[11]
Management — definitive and stepwise
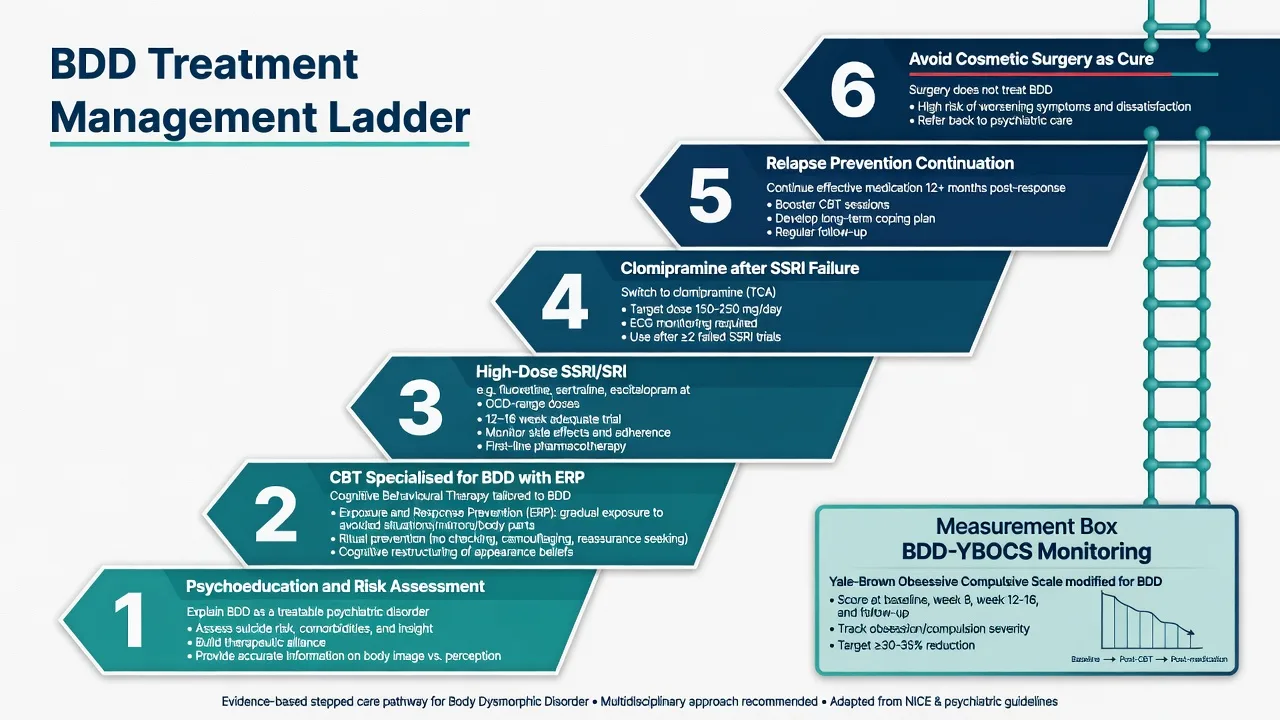
First-line psychological treatment — CBT specialised for BDD
CBT-BDD includes psychoeducation, cognitive work on appearance beliefs, perceptual retraining, and exposure with response prevention adapted to appearance triggers: graded mirror exposure, reduction of checking/camouflage/reassurance, and behavioural experiments that test feared social consequences. Family accommodation and reassurance are reduced collaboratively.[5][7][9]
Landmark evidence: modular CBT for BDD improved symptoms in randomised designs;[5] CBT outperformed anxiety management;[7] therapist-delivered CBT showed efficacy versus supportive psychotherapy with post-treatment effects;[6] meta-analysis supports CBT across RCTs;[9] therapist-guided internet CBT (BDD-NET) is superior to online supportive therapy in a single-blind RCT — useful for access when specialist face-to-face CBT is scarce.[8] Cochrane synthesis supports both pharmacotherapy and psychotherapy evidence bases, though trial numbers remain smaller than for OCD.[10]
Generic supportive counselling without exposure and ritual prevention is an exam failure mode.[6][11]
First-line pharmacotherapy — high-dose SSRI / SRI
SSRIs (and clomipramine as a potent SRI) are first-line medications. Doses are often in the OCD-range high end, and an adequate trial is longer than depression care — consensus teaching supports a 12–16 week trial including several weeks at the maximum tolerated therapeutic dose before declaring non-response, after adherence is verified.[11][23][24]
Fluoxetine has the strongest placebo-controlled monotherapy RCT signal in BDD and is preferred as the initial SSRI in NICE guidance for adults with BDD because of that evidence base.[2][11]
| Agent (class) | Typical adult start (oral) | Common BDD therapeutic range (exam teaching) | Key notes |
|---|---|---|---|
| Fluoxetine (SSRI) | 20 mg daily | 40–80 mg daily (some specialist practice higher under monitoring) | Best BDD-specific RCT evidence |
| Sertraline (SSRI) | 50 mg daily | 150–200 mg daily (sometimes higher specialist) | Often used; titrate; sexual/GI effects |
| Escitalopram (SSRI) | 10 mg daily | 20–30+ mg specialist range in BDD series | Relapse-prevention evidence after response |
| Fluvoxamine (SSRI) | 50 mg daily | 200–300 mg daily order | CYP interactions |
| Paroxetine (SSRI) | 20 mg daily | 40–60 mg daily | Discontinuation symptoms |
| Clomipramine (TCA/SRI) | 25 mg daily | 100–250 mg daily (individualise) | After SSRI failure; ECG, anticholinergic, seizure risk |
| Typical adult oral ranges for exam use; individualise for age, hepatic/renal function, interactions, pregnancy; check local product information. High-dose practice is specialist territory with monitoring.[2][11][23][24] |
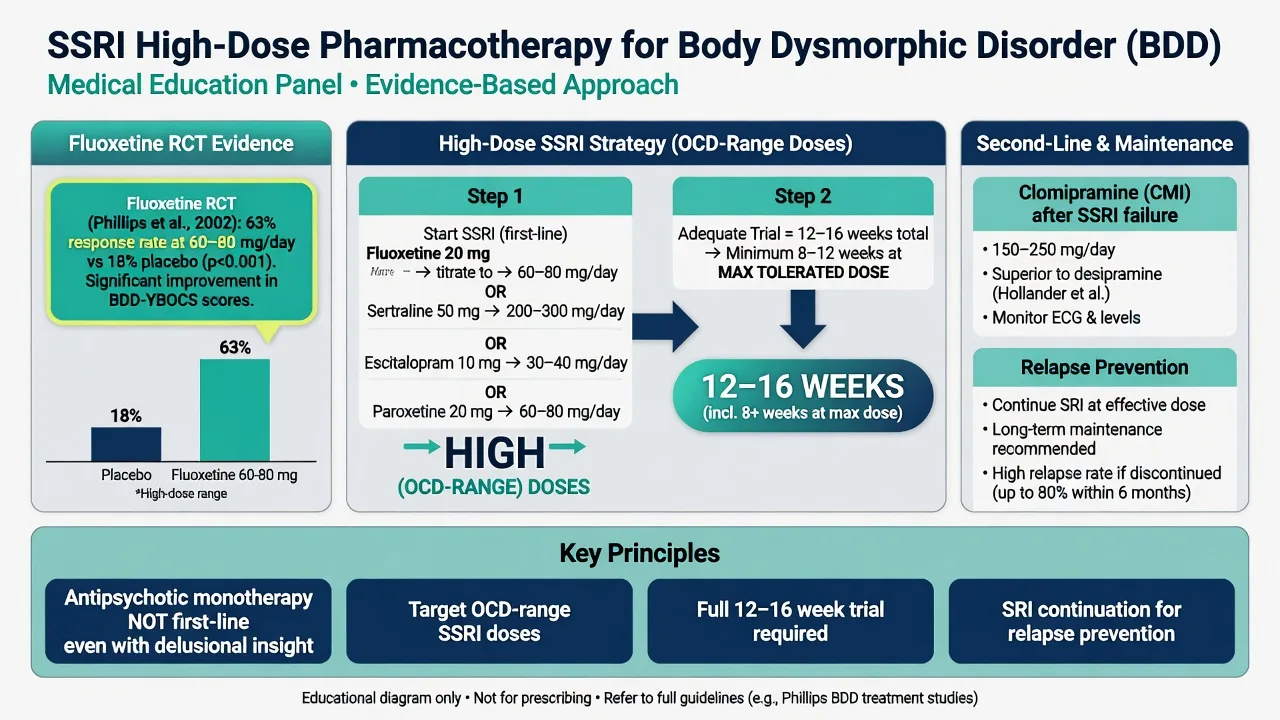
Delusional insight. Fluoxetine improved BDD including among participants with delusional beliefs in the placebo-controlled trial — do not withhold SRI because insight is absent, and do not treat pure delusional BDD as schizophrenia with antipsychotic monotherapy as first-line.[2][12][23]
Monitoring. Early activation; sexual dysfunction (adherence driver); GI effects; hyponatraemia in older adults; QTc context for some agents; suicide risk with comorbid depression. Educate that benefit may lag weeks.[23][24]
Clomipramine
Clomipramine was superior to desipramine in a double-blind crossover trial, supporting serotonergic selectivity for BDD over a noradrenergic TCA control.[3] Use after SSRI non-response or intolerance, with baseline ECG, anticholinergic counselling, seizure risk awareness, and careful titration. Avoid casual serotonergic polypharmacy.[3][23]
Relapse prevention and maintenance
After response to escitalopram, double-blind discontinuation to placebo increased relapse risk versus continuation — continue effective SRI after response rather than stopping early.[4] Combine with booster CBT for residual rituals. Withdraw medication slowly with a plan if eventually stopping.[4][11]
Cosmetic surgery and procedures — do not collude
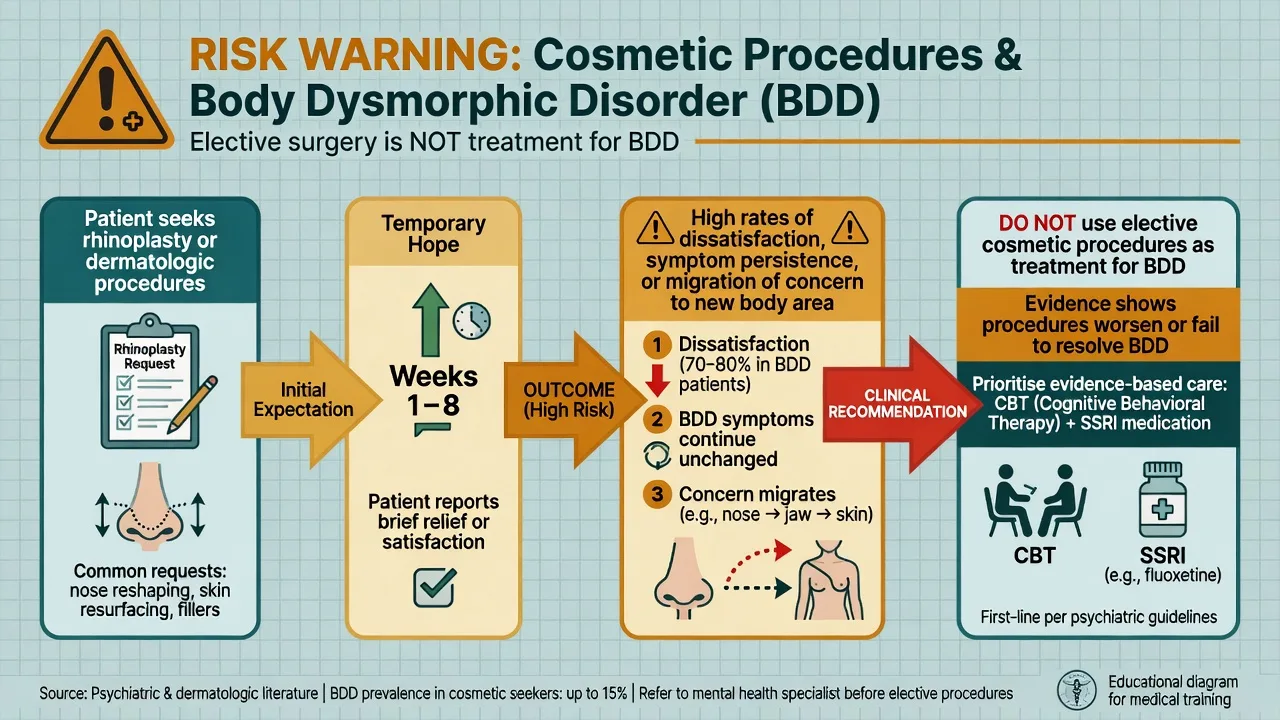
Persons with BDD frequently seek surgical and minimally invasive cosmetic procedures; outcomes are typically poor for the psychiatric disorder itself, with dissatisfaction, persistence, or migration of concern to another body area.[19][22] Exam answer: screen for BDD in cosmetic pathways; advise against elective cosmetic treatment as a BDD cure; offer psychiatric care with CBT-BDD and SRI.[11][19]
Insight spectrum in treatment
Specific subtypes and scenarios
Muscle dysmorphia. Screen AAS, overtraining injuries, body composition extremes, and medical complications; use CBT-BDD adapted to muscle beliefs plus SRI as indicated; do not label healthy fitness culture as BDD without impairment and preoccupation criteria.[20]
Adolescent BDD. Family engagement, school avoidance, social media comparing, and higher relative weight of specialised CBT; SSRI when indicated with activation/suicidality discussion.[11][12]
Comorbid OCD + BDD. Dual-content ERP hierarchies; do not assume treating one extinguishes the other.[12][14]
Consultation-liaison (plastics/dermatology). Brief screen: Do you spend a lot of time worrying about a defect others say is minor? Do you check mirrors, camouflage, or seek procedures repeatedly? If yes, refer for full assessment rather than proceeding with elective surgery.[19][22]
Complications and pitfalls
- Missing suicide risk while focusing only on rituals.[15][16]
- Misdiagnosing delusional BDD as schizophrenia and withholding SRI/CBT-BDD.[2][13]
- Colluding with endless cosmetic procedures.[19]
- Under-dosing SSRI or declaring failure after a brief low-dose trial.[11][24]
- Offering non-specific therapy without exposure and ritual prevention components.[6][9]
- Collapsing BDD into “just depression” or “just OCD” without appearance-focused treatment targets.[12][14]
Prognosis and disposition
Without treatment, course is often chronic. With specialised CBT and/or adequate SRI, many achieve clinically meaningful symptom reduction, though residual symptoms and relapse risk with early stop are common.[4][9][11]
Poorer markers: longer untreated duration, poor insight, severe depression/suicidality, ongoing cosmetic chasing, incomplete CBT fidelity. Disposition: outpatient specialist CBT + meds; intensive day or inpatient care for high risk or housebound cases; CL psychiatry for surgical clinics.[11][12]
Special populations
Children and adolescents. Developmentally adapted CBT-BDD; family reduction of accommodation and reassurance; careful SSRI discussion when severity warrants medication.[11]
Pregnancy and lactation. Untreated severe BDD impairs function and may elevate risk; shared decision-making on sertraline/fluoxetine versus prioritising CBT access; involve perinatal psychiatry when available.[23]
Older adults. Hyponatraemia, falls, polypharmacy; late-onset organic screen; start lower, titrate slower; ECG before clomipramine.[23]
Cultural beauty ideals. Culture shapes content of concern but does not erase clinical BDD when preoccupation, rituals, and impairment meet criteria.[12]
Evidence, guidelines and regional differences
Landmark pillars: BDD-YBOCS development;[1] Phillips fluoxetine RCT;[2] Hollander clomipramine vs desipramine;[3] escitalopram relapse prevention;[4] Wilhelm modular CBT;[5] Wilhelm CBT vs supportive psychotherapy;[6] Veale CBT vs anxiety management;[7] Enander internet CBT;[8] Harrison CBT meta-analysis;[9] Ipser Cochrane review;[10] Castle ICOCS treatment synthesis;[11] Phillips clinical overview;[12] insight and comparative OCD studies;[13][14] suicidality series;[15][16] prevalence surveys;[17][18] cosmetic procedure outcomes;[19] muscle dysmorphia clinical features.[20]
In Australian and New Zealand practice, access to therapists trained in CBT-BDD is often rate-limiting. Use secondary services, private psychologists with OCRD competence, and evidence-supported remote protocols where fidelity is acceptable. Prescribing follows TGA product information; high-dose SSRI and clomipramine require monitoring and shared decision-making. Mental Health Act frameworks are state/territory-specific. Cosmetic industry access makes screening and non-collusion ethically important.[11]
Exam pearls
BDD exam anchors
References
- [1]Phillips KA, Hollander E, Rasmussen SA, et al. A severity rating scale for body dysmorphic disorder: development, reliability, and validity of a modified version of the Yale-Brown Obsessive Compulsive Scale Psychopharmacol Bull, 1997.PMID 9133747
- [2]Phillips KA, Albertini RS, Rasmussen SA A randomized placebo-controlled trial of fluoxetine in body dysmorphic disorder Arch Gen Psychiatry, 2002.PMID 11926939
- [3]Hollander E, Allen A, Kwon J, et al. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: selective efficacy of a serotonin reuptake inhibitor in imagined ugliness Arch Gen Psychiatry, 1999.PMID 10565503
- [4]Phillips KA, Keshaviah A, Dougherty DD, et al. Pharmacotherapy Relapse Prevention in Body Dysmorphic Disorder: A Double-Blind, Placebo-Controlled Trial Am J Psychiatry, 2016.PMID 27056606
- [5]Wilhelm S, Phillips KA, Didie E, et al. Modular cognitive-behavioral therapy for body dysmorphic disorder: a randomized controlled trial Behav Ther, 2014.PMID 24680228
- [6]Wilhelm S, Phillips KA, Greenberg JL, et al. Efficacy and Posttreatment Effects of Therapist-Delivered Cognitive Behavioral Therapy vs Supportive Psychotherapy for Adults With Body Dysmorphic Disorder: A Randomized Clinical Trial JAMA Psychiatry, 2019.PMID 30785624
- [7]Veale D, Anson M, Miles S, et al. Efficacy of cognitive behaviour therapy versus anxiety management for body dysmorphic disorder: a randomised controlled trial Psychother Psychosom, 2014.PMID 25323062
- [8]Enander J, Andersson E, Mataix-Cols D, et al. Therapist guided internet based cognitive behavioural therapy for body dysmorphic disorder: single blind randomised controlled trial BMJ, 2016.PMID 26837684
- [9]Harrison A, Fernández de la Cruz L, Enander J, et al. Cognitive-behavioral therapy for body dysmorphic disorder: A systematic review and meta-analysis of randomized controlled trials Clin Psychol Rev, 2016.PMID 27393916
- [10]Ipser JC, Sander C, Stein DJ Pharmacotherapy and psychotherapy for body dysmorphic disorder Cochrane Database Syst Rev, 2009.PMID 19160252
- [11]Castle D, Beilharz F, Phillips KA, et al. Body dysmorphic disorder: a treatment synthesis and consensus on behalf of the International College of Obsessive-Compulsive Spectrum Disorders Int Clin Psychopharmacol, 2021.PMID 33230025
- [12]Phillips KA, Kelly MM Body Dysmorphic Disorder: Clinical Overview and Relationship to Obsessive-Compulsive Disorder Focus (Am Psychiatr Publ), 2021.PMID 35747292
- [13]Phillips KA, Pinto A, Hart AS, et al. A comparison of insight in body dysmorphic disorder and obsessive-compulsive disorder J Psychiatr Res, 2012.PMID 22819678
- [14]Phillips KA, Gunderson CG, Mallya G, et al. A comparison study of body dysmorphic disorder and obsessive-compulsive disorder J Clin Psychiatry, 1998.PMID 9862601
- [15]Phillips KA, Menard W Suicidality in body dysmorphic disorder: a prospective study Am J Psychiatry, 2006.PMID 16816236
- [16]Phillips KA, Coles ME, Menard W, et al. Suicidal ideation and suicide attempts in body dysmorphic disorder J Clin Psychiatry, 2005.PMID 15960564
- [17]Koran LM, Abujaoude E, Large MD, et al. The prevalence of body dysmorphic disorder in the United States adult population CNS Spectr, 2008.PMID 18408651
- [18]Buhlmann U, Glaesmer H, Mewes R, et al. Updates on the prevalence of body dysmorphic disorder: a population-based survey Psychiatry Res, 2010.PMID 20452057
- [19]Crerand CE, Menard W, Phillips KA Surgical and minimally invasive cosmetic procedures among persons with body dysmorphic disorder Ann Plast Surg, 2010.PMID 20467296
- [20]Pope CG, Pope HG, Menard W, et al. Clinical features of muscle dysmorphia among males with body dysmorphic disorder Body Image, 2005.PMID 17075613
- [21]Phillips KA, Wilhelm S, Koran LM, et al. Body dysmorphic disorder: some key issues for DSM-V Depress Anxiety, 2010.PMID 20533368
- [22]Phillips KA Body dysmorphic disorder: recognizing and treating imagined ugliness World Psychiatry, 2004.PMID 16633443
- [23]Hong K, Nezgovorova V, Uzunova G, et al. Pharmacological Treatment of Body Dysmorphic Disorder Curr Neuropharmacol, 2019.PMID 29701157
- [24]Phillips KA Pharmacotherapy for Body Dysmorphic Disorder Psychiatr Ann, 2010.PMID 27761054