Psych · General adult psychiatry — personality disorders
Borderline personality disorder
Also known as BPD · Emotionally unstable personality disorder · Borderline pattern personality disorder · Cluster B personality disorder · Emotion dysregulation disorder
Exam-exhaustive fellowship reference on borderline personality disorder — DSM-5-TR and ICD-11 nosology; epidemiology and suicide risk; biosocial and mentalization models; differentials including bipolar, trauma, ADHD and organic change; crisis and risk formulation; DBT, MBT, schema therapy, TFP and structured clinical management; limited pharmacotherapy with Cochrane and LABILE evidence; longitudinal recovery. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
1 MCQ with explanations
Target exams
Red flags
Borderline personality disorder (BPD) is a high-yield general adult and emergency psychiatry topic across FRANZCP, MRCPsych, ABPN and MD/DNB examinations. Examiners test whether you can diagnose with operational criteria, discriminate bipolar and trauma mimics, run a risk-focused crisis interview without stigma, prescribe psychotherapy first-line with trial-level names, and resist the trap of escalating medication without a review plan.[18][19][20]
Overview and definition
BPD is a pervasive pattern of instability of interpersonal relationships, self-image and affects, with marked impulsivity, beginning by early adulthood and present across contexts. It is a clinical diagnosis based on longitudinal history, collateral and mental state — not a blood test, scan or single crisis interview. Modern fellowship framing rejects therapeutic nihilism: prospective studies show substantial symptomatic improvement over years for many people, while functional recovery and suicide risk still demand structured care.[16][17][18]
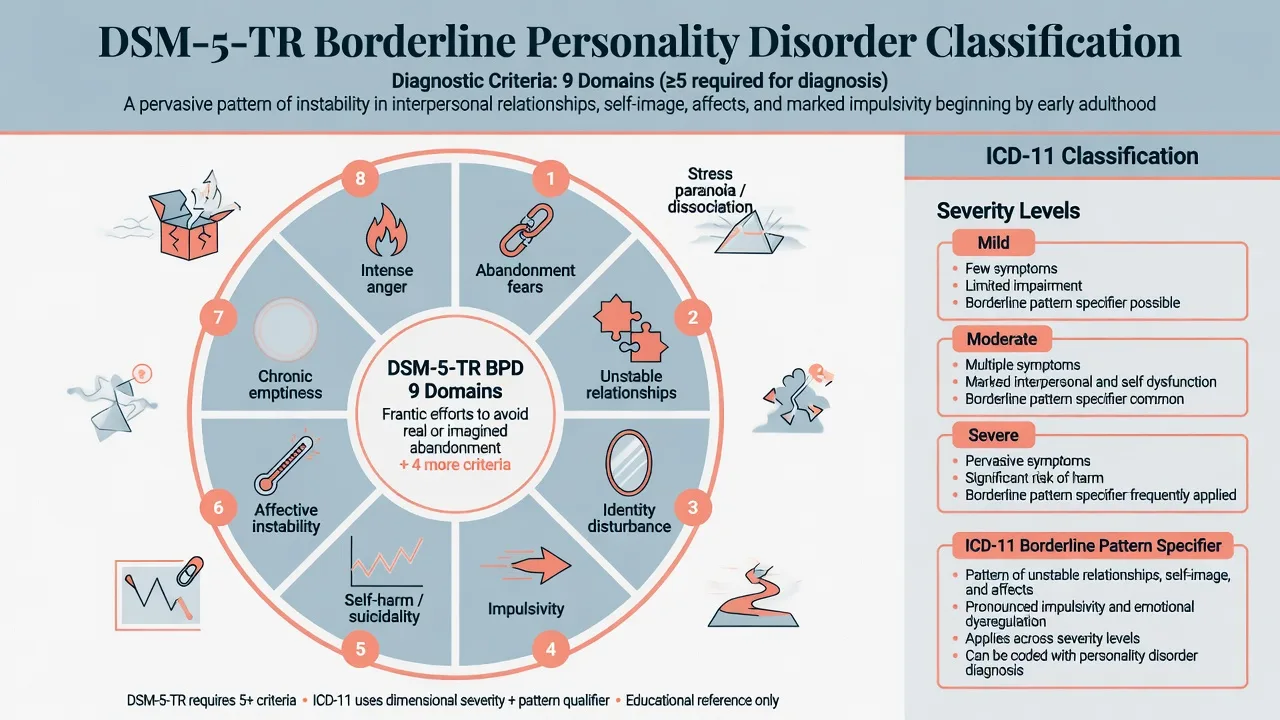
DSM-5-TR categorical threshold. After general personality disorder criteria are met, BPD requires five or more of nine Criterion features: frantic efforts to avoid real or imagined abandonment; pattern of unstable and intense interpersonal relationships (idealisation/devaluation); identity disturbance; impulsivity in at least two potentially self-damaging areas (excluding suicidal/self-mutilating behaviour, which is counted separately); recurrent suicidal behaviour, gestures, threats, or self-mutilating behaviour; affective instability due to a marked reactivity of mood; chronic feelings of emptiness; inappropriate intense anger or difficulty controlling anger; transient, stress-related paranoid ideation or severe dissociative symptoms.[18][20]
ICD-11. Personality disorder is rated by severity (mild, moderate, severe) with optional trait domain qualifiers. A borderline pattern specifier captures the familiar clinical constellation of instability in relationships, self-image and affects with impulsivity and self-harm risk. Examiners increasingly expect you to state which manual you are using and that ICD-11 is dimensional-severity plus pattern, whereas DSM still foregrounds a 5/9 categorical count for classic exam stems.[19][20]
Classification and nosology
DSM-5-TR BPD
- Categorical: ≥5 of 9 features
- General PD criteria must also be met
- Alternative Model (AMPD) available for trait/impairment formulation
- Exam stems often still use the 9-item checklist
ICD-11 PD + borderline pattern
- Severity first: mild / moderate / severe
- Borderline pattern specifier optional
- Trait domains describe style of dysfunction
- Better for dimensional case discussion
Related Cluster B
- Antisocial: rights violation, remorselessness, conduct history
- Narcissistic: grandiosity, entitlement, admiration need
- Histrionic: attention-seeking, dramatic affectivity
- Overlap is common — formulate primary pattern
Not the same as
- Bipolar episodes (duration and sleep need)
- PTSD alone (trauma-specific re-experiencing)
- ADHD alone (childhood neurodevelopmental pattern)
- Acute substance intoxication
The Alternative Model for Personality Disorders (AMPD) in DSM-5-TR Section III formulates Criterion A (self and interpersonal functioning impairment) plus Criterion B pathological traits (for BPD, typically high negative affectivity, disinhibition, and antagonism elements). Use AMPD language in formulation stations even when you diagnose with the classic categorical criteria.[20]
Epidemiology and risk factors
Headline numbers every candidate must own
Community surveys show BPD is not rare; clinical services see substantial enrichment because crisis, self-harm and comorbidity drive presentation. The Wave 2 NESARC analysis reported meaningful prevalence, disability and psychiatric comorbidity for DSM-IV BPD in a large US adult sample.[15][18]
Risk and aetiological factors. Childhood adversity and trauma, chronic invalidation, disrupted attachment, temperamental emotional intensity and impulsivity, and genetic contribution to personality vulnerability all feature in contemporary models. Trauma is common but neither necessary nor sufficient for diagnosis — do not collapse BPD into “complex PTSD” without criteria work, and do not miss PTSD when it is present.[18][19][20]
Suicide and self-harm epidemiology. Recurrent self-harm and suicide attempts are core to the clinical burden. Soloff and colleagues identified risk factors for suicidal behaviour in BPD; long-term follow-up continues to show elevated suicidal behaviour risk that is not static and is influenced by depression, substance use, and prior attempts.[18][19]
Pathophysiology and mechanisms
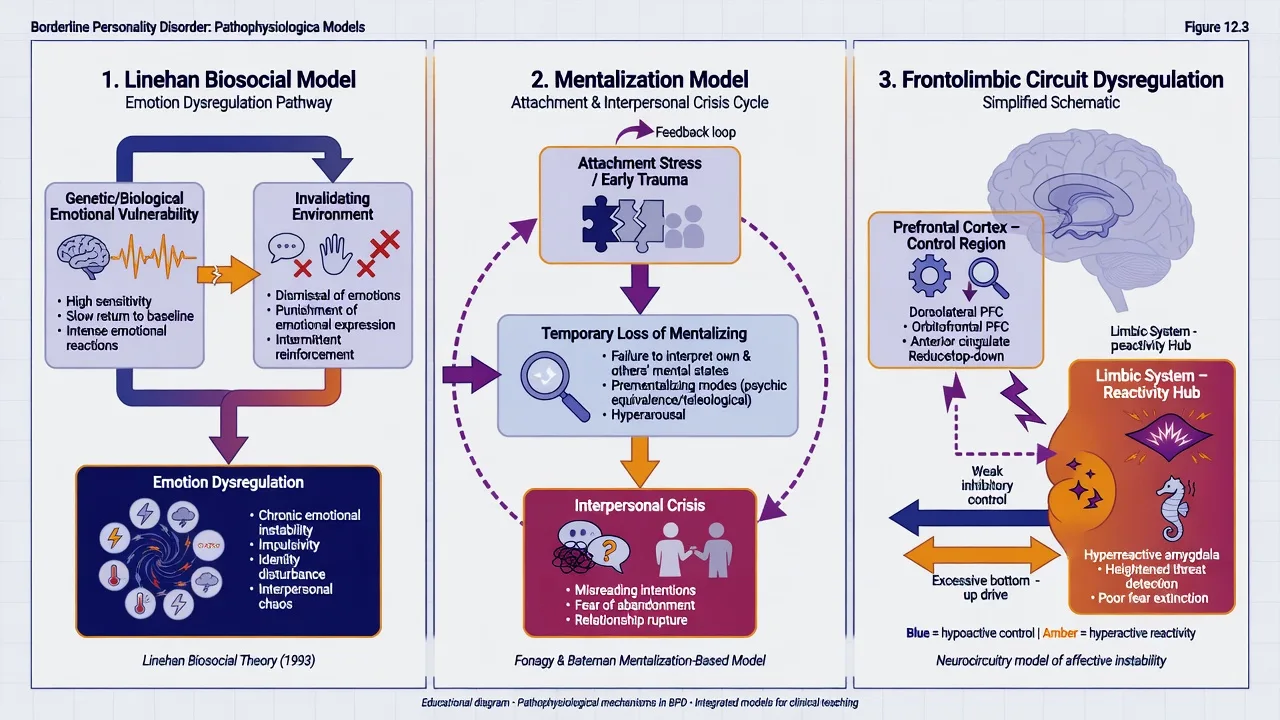
Biosocial model (Linehan). Emotionally vulnerable temperament (high sensitivity, high reactivity, slow return to baseline) interacts with an invalidating environment (dismissal, punishment of emotional expression, intermittent reinforcement of escalation) to produce chronic emotion dysregulation, identity disturbance and interpersonal chaos. This model underpins DBT’s dialectic of acceptance and change.[1][18]
Mentalization model (Bateman and Fonagy). Under attachment stress, the capacity to understand behaviour in terms of intentional mental states (one’s own and others’) becomes impaired. Premenstrual-style teaching is not the point — the viva point is that interpersonal crises reflect temporary loss of mentalizing, which MBT aims to restore in session and in relationships.[5][6]
Schema and object-relations models. Schema therapy targets early maladaptive schemas and modes; TFP (Kernberg tradition) targets identity diffusion, primitive defences (splitting, projective identification) and the activation of transferences in the therapeutic relationship. These are not “soft psychology” — they have randomised and multiwave comparative data.[7][8]
Neurobiology (keep humble). Group-level findings implicate frontolimbic imbalance (weaker top-down regulatory control, heightened limbic threat reactivity), impulsivity circuitry and stress-axis sensitivity. Imaging does not diagnose BPD in an individual patient.[19][20]
Clinical presentation
Core presentation combines affective instability (rapid, intense mood shifts lasting hours to a few days, often interpersonal-triggered), interpersonal hypersensitivity (abandonment fears, idealisation/devaluation), identity disturbance, impulsivity, chronic emptiness, anger dysregulation, and self-harm or suicidality, sometimes with transient stress-related paranoia or dissociation. Quote the patient’s language in the MSE (“I disappear when people leave”; “I cut to feel real”).[18][20]
Crisis presentations. Emergency departments see post-rupture crises, overdose, cutting, threats after perceived rejection, and substance-fuelled impulsivity. Distinguish acute suicidal intent from non-suicidal self-injury used for affect regulation — both require assessment; neither is dismissed as “attention-seeking.”[18][19]
Quieter outpatient presentations. Chronic emptiness, unstable work and housing, serial short therapies, mild-to-moderate self-harm without current intent, and comorbid depression or PTSD without a single dramatic crisis.[16][17]
Differential diagnosis
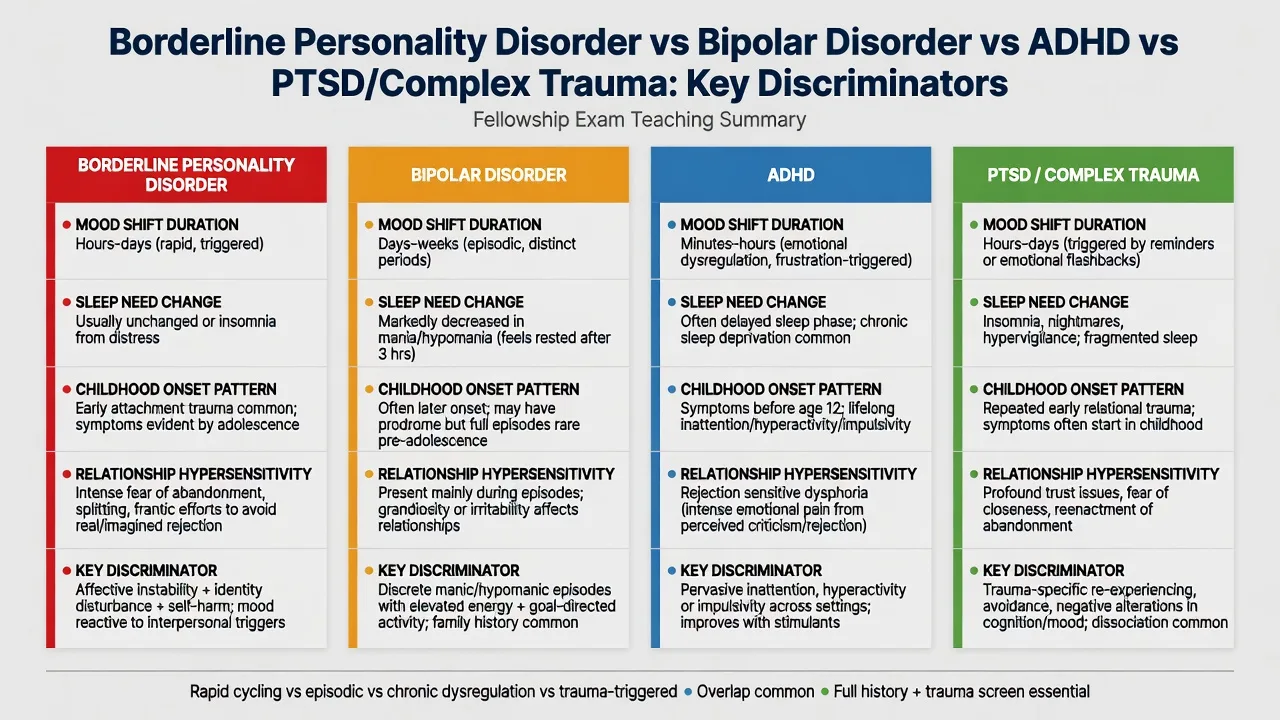
Bipolar disorder
- Episodes last days–weeks (mania ≥7 days or hospitalisation; hypomania ≥4 days)
- Reduced sleep need with preserved energy is a bipolar clue
- Grandiosity, goal-directed activity, psychosis in mania
- Family history and antidepressant switching history matter
PTSD / complex trauma
- Trauma-specific re-experiencing, avoidance, hyperarousal
- Can co-occur with BPD — dual diagnosis is allowed
- Do not force either/or when both criteria are met
- Trauma-focused therapy may be sequenced with BPD work
ADHD
- Lifelong inattention/hyperactivity from childhood across settings
- Rejection-sensitive dysphoria can mimic interpersonal storms
- Stimulant response history can be informative
- Comorbidity is common — treat both when present
Substance / organic
- Intoxication/withdrawal can look like affect dysregulation
- Late-onset personality change → medical/neurological work-up
- TBI, FTD, epilepsy, endocrine disease
- UDS, collateral timeline, imaging/EEG when indicated
Also keep major depression (which frequently coexists), other personality disorders, autism spectrum social communication differences, and psychotic disorders with affective overlays on the board. The exam skill is discriminators plus comorbidity, not exclusive single labels.[15][18][20]
Clinical and bedside assessment
Structure the interview: developmental history; attachment and trauma (with pacing and safety); relationship patterns; self-harm and suicide chronology (methods, intent, lethality, functions of self-injury); substance use; prior therapies and medications with adherence and benefit; current crisis triggers; collateral; safeguarding (children, intimate partner violence); capacity.[18][19]
Mental State Examination. Affect (range, reactivity, congruence), thought content (abandonment themes, paranoia under stress), perceptual phenomena and dissociation, cognition, insight and judgement, alliance quality, and risk. Document both chronic baseline risk and today’s acute risk change.[19]
Risk assessment in BPD is specialised. Chronic elevated risk does not mean every presentation needs admission; acute escalation after abandonment, intoxication, new plan/means, or comorbid depression does change the plan. Assess ideation, intent, plan, means, protective factors, impulsivity, substance use, and prior near-lethal attempts. Capacity is decision-specific. Involuntary care uses local Mental Health Act principles — least restrictive, statute-bound; do not invent section numbers for the wrong jurisdiction.[18][19]
Investigations
BPD has no laboratory gold standard. Investigate to exclude mimics and prepare for medication when used: TSH, FBC, U&E, LFT, glucose/lipids and BMI if antipsychotics considered, pregnancy test when relevant, urine drug screen when substances may explain behaviour, ECG when cardiac risk or QTc-risk drugs are planned. Neuroimaging or EEG when late-onset change, focal neurology, seizures or cognitive decline fire. Screen systematically for bipolar spectrum, PTSD, ADHD, eating disorders and substance use disorders because they change the treatment map.[12][19][20]
Management — acute crisis and resuscitation
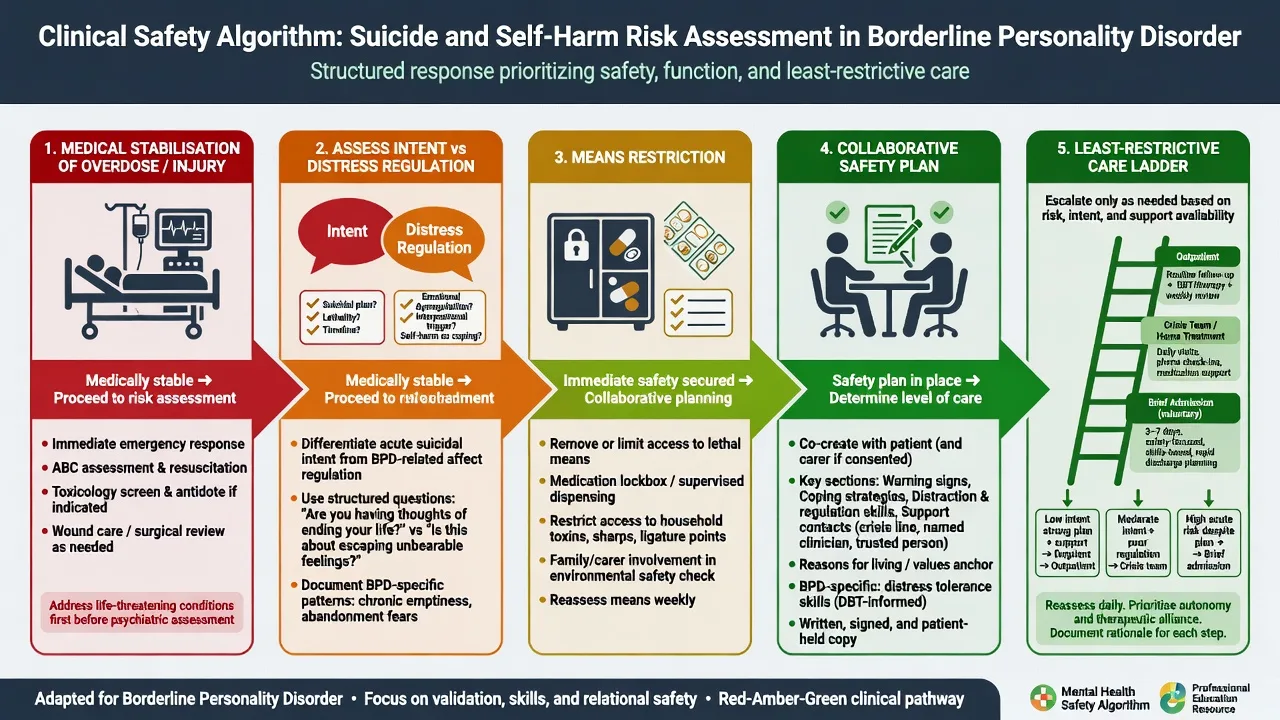
Crisis principles that score marks. Validate emotion without validating unsafe behaviour. Clarify the problem of the day. Co-create a time-limited plan. Restrict means. Avoid both punitive discharge and indefinite open-ended admission that reinforces crisis as the only care pathway. Link early to a named outpatient clinician. Use de-escalation before pharmacological restraint; if acute agitation threatens safety, use local emergency rapid-tranquillisation protocols with monitoring rather than inventing a long-term “BPD sedative regimen.” Legal status is jurisdiction-specific.[4][19]
Collaborative safety planning. Warning signs; internal coping skills; social contacts; professional crisis contacts; means restriction; reasons for living. Reassess after relationship rupture, substance relapse, therapy drop-out, or discharge.[19]
Management — definitive and stepwise
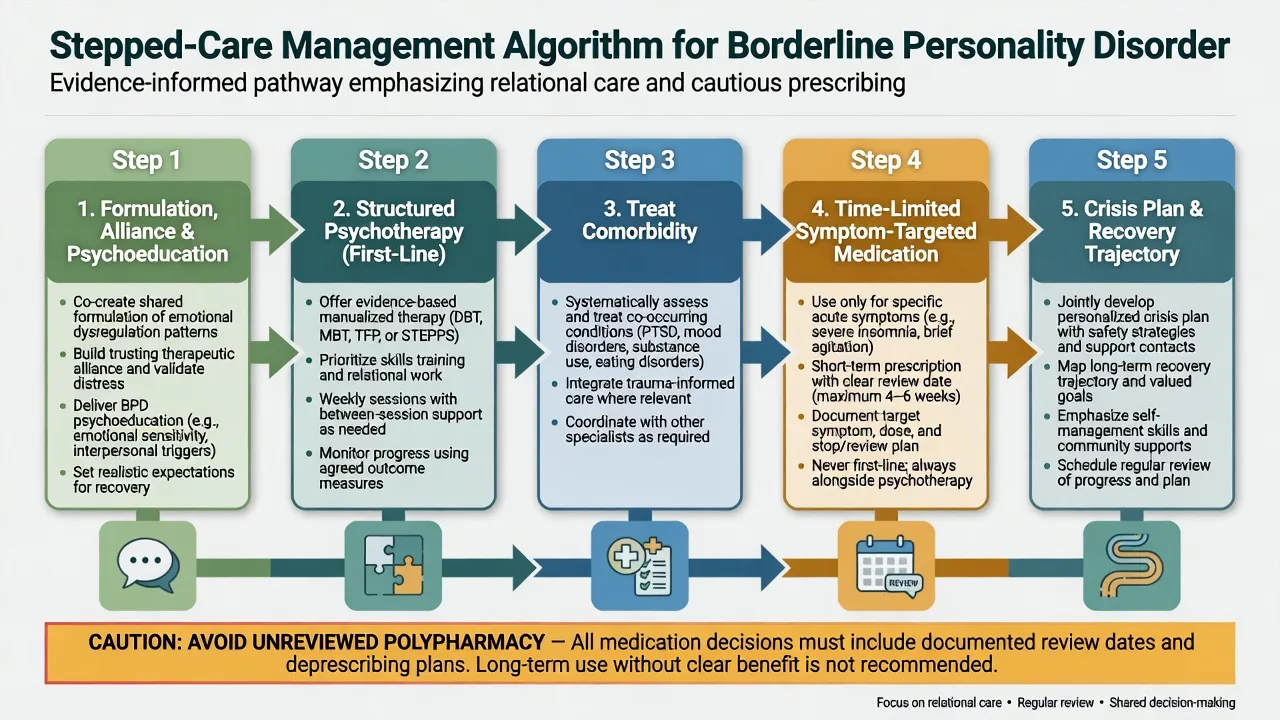
First-line: structured psychotherapy
Meta-analysis and Cochrane synthesis support specialised psychotherapies for BPD relative to control conditions, with clinically important reductions in BPD severity and self-harm for several manualised approaches. Choice is guided by availability, patient preference, comorbidity and therapist training — not by brand loyalty alone.[9][10]
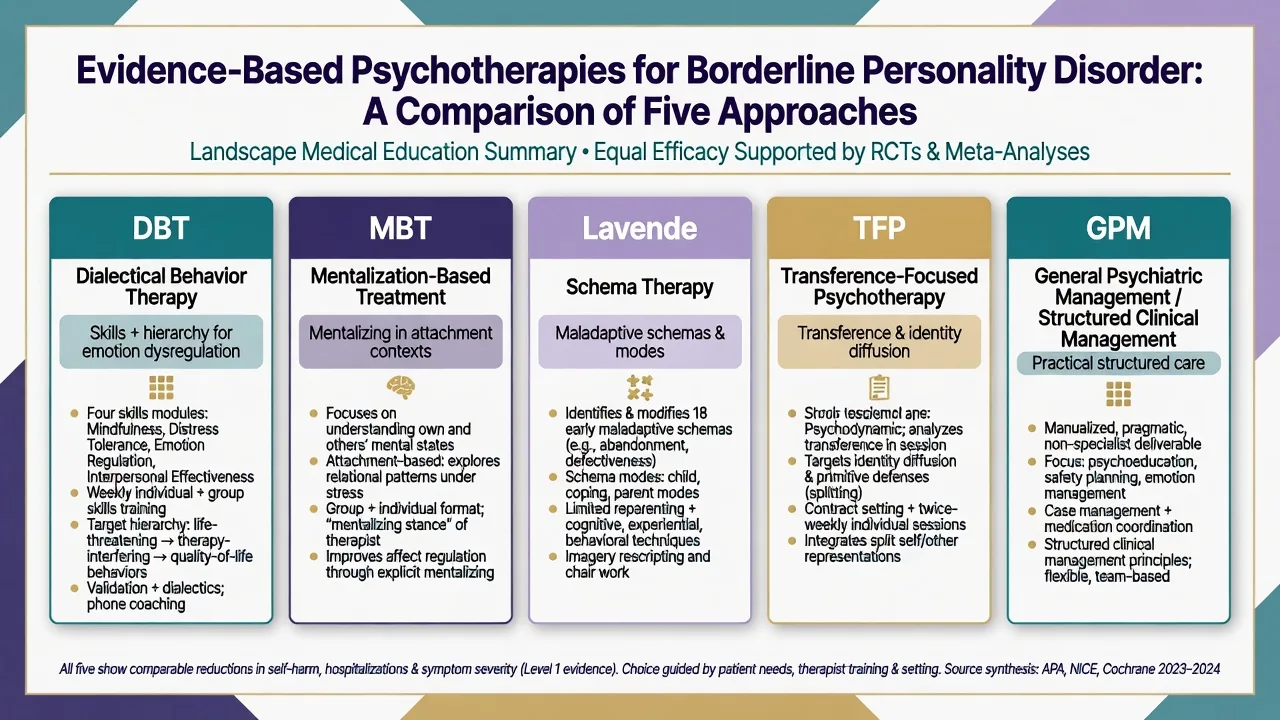
Dialectical behaviour therapy (DBT). Multimodal: individual therapy, skills training group (mindfulness, distress tolerance, emotion regulation, interpersonal effectiveness), between-session coaching where available, and a therapist consultation team. Target hierarchy prioritises life-threatening behaviours, then therapy-interfering behaviours, then quality-of-life targets. Foundational RCT evidence includes Linehan’s early parasuicide trial, multi-year comparisons with community treatment by experts, and component analyses in high suicide-risk samples.[1][2][3]
Mentalization-based treatment (MBT). Individual and group formats aiming to restore mentalizing under attachment arousal. Outpatient MBT improved outcomes versus structured clinical management in RCT evidence; longer-term follow-up of earlier MBT cohorts showed sustained advantages over treatment as usual on clinically important outcomes including suicidality and service use in published 8-year data.[5][6]
Schema-focused therapy and TFP. Outpatient RCT evidence found schema-focused therapy superior to TFP on several recovery indicators in one landmark Dutch trial, while Clarkin’s multiwave study evaluated TFP, DBT and supportive treatment with differential effects across outcome domains — examiners want the names and the principle that specialised structured therapies outperform unstructured TAU.[7][8]
General psychiatric management (GPM) / structured clinical management. McMain and colleagues showed DBT and GPM both produced substantial improvement in a large RCT — a critical exam pearl: good structured psychiatric care is not “nothing,” and scarcity of DBT does not justify nihilism if structured clinical management is delivered well.[4]
Pharmacotherapy — limited, targeted, time-limited
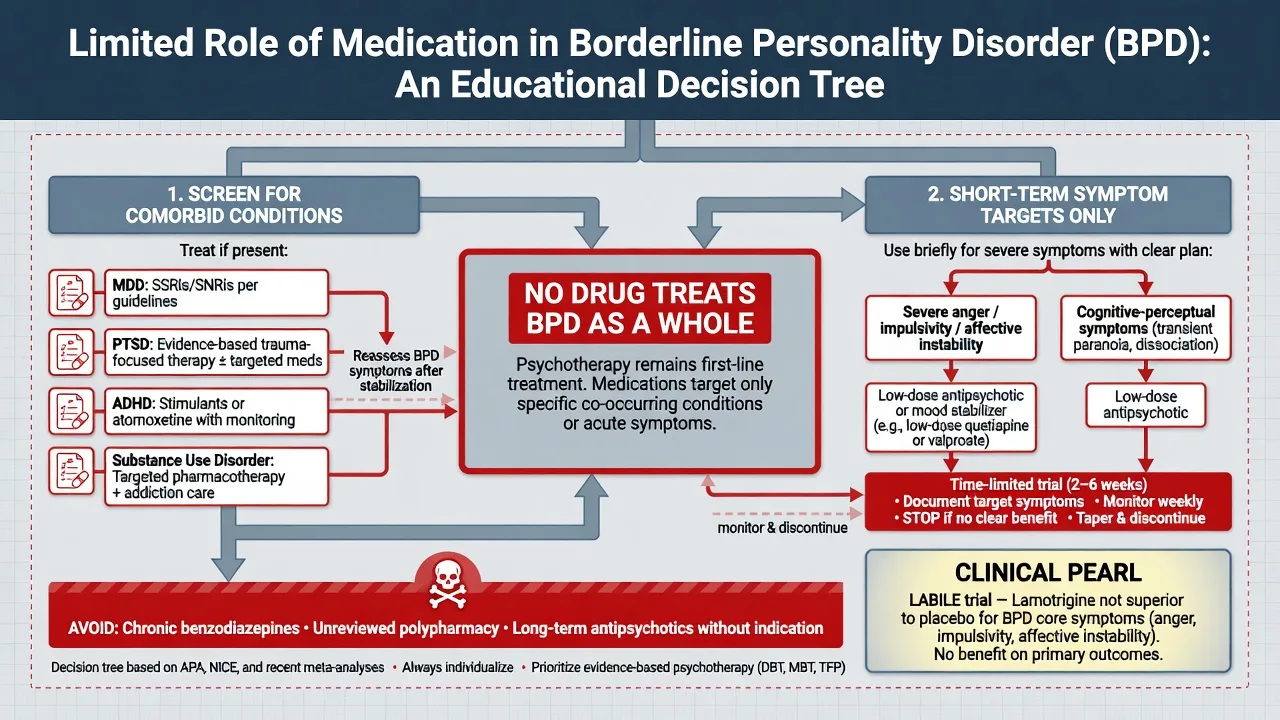
What you may still prescribe (with a stop date). Treat comorbid major depression, PTSD, ADHD, anxiety disorders and substance use with the same evidence standards as outside BPD. For severe cognitive-perceptual symptoms or marked anger/impulsivity, time-limited low-dose antipsychotic trials are sometimes used in specialist practice — always document the target symptom, baseline metabolic/ECG risk as indicated, expected review (commonly within weeks), and plan to stop if no benefit. Avoid chronic benzodiazepines for emotion regulation. Avoid stacking multiple psychotropics without a formulation.[11][12][13]
LABILE trial pearl. In a large randomised placebo-controlled trial, lamotrigine was not superior to placebo for BPD core symptoms and was not cost-effective — do not add lamotrigine as default “mood stabilisation for BPD.”[14]
Example adult prescribing language when an examiner forces a named plan (individualise; check local product information). For comorbid major depression without bipolarity, a common first-line example is sertraline 50 mg orally daily, review in 1–2 weeks for activation and suicidality, titrate toward 50–150 mg as tolerated with a clear measurement plan — this treats depression, not BPD identity. If a specialist trial of a low-dose antipsychotic is used for severe transient stress-related paranoia or marked aggression after non-drug strategies fail, exam-level examples discussed in literature syntheses include low-dose second-generation agents with metabolic monitoring; treat any such trial as time-limited with a written stop/review date rather than indefinite continuation.[12][13][19]
Care system and disposition
Match intensity to risk and function: specialist psychotherapy pathway; community mental health team coordination; day programs; brief crisis admission for acute uncontainable risk; longer inpatient stays only when necessary and with a discharge plan from day one. Consistency of team response and a written crisis plan reduce iatrogenic chaos.[4][19]
Australian and New Zealand services increasingly frame BPD within stepped mental health and personality disorder pathways emphasising early intervention, trauma-informed care, cultural safety, and access to structured therapies where available. Local Mental Health Act provisions govern involuntary care — name principles, not invented section numbers from other countries.[19][20]
Specific subtypes and scenarios
Chronic non-suicidal self-injury versus high-lethality attempts. Function of self-injury (affect regulation, self-punishment, communication) must be assessed separately from desire to die. Prior high-lethality attempts and current intent drive higher care intensity.[18]
BPD with bipolar or major depression. Dual formulation is allowed. Treat mood episodes with bipolar-safe or depression-appropriate algorithms; do not assume every mood swing is BPD or every crisis is mania.[15][20]
BPD with substance use. Substances amplify impulsivity and suicide risk; integrated dual treatment outperforms sequential siloed care rhetoric.[15][19]
Adolescents and early intervention. Diagnosis can be made in adolescence when criteria are met; early structured intervention is preferred to “wait until 18.” Developmental formulation and family work matter.[19][20]
Forensic interface. Impulsivity and aggression require structured risk formulation (static/dynamic factors, substance use, context) without diagnostic fatalism or pejorative labelling as the risk tool.[19]
Complications and pitfalls
Classic pitfalls: stigma and diagnostic overshadowing of medical illness; missed bipolarity, PTSD, ADHD or autism; declaring “untreatable” because DBT waitlists exist while omitting structured clinical management; confusing chronic risk with acute unmanageable risk; under-treating true major depression or psychosis; therapist isolation without supervision.[9][19][20]
Prognosis and disposition
Longitudinal studies (MSAD, CLPS) show that many people with BPD experience substantial reductions in symptomatic criteria over years; functional recovery (work, relationships) often lags symptomatic improvement. Suicide risk remains a lifelong consideration for some, with highest relative concern earlier in the course and during depressive or substance-use exacerbations. Engagement in treatment, reduced substance use, and supportive relationships predict better trajectories.[16][17][19]
Special populations
Pregnancy and parenting. Collaborative risk–benefit decisions; minimise teratogenic polypharmacy; support attachment and safeguarding; coordinate perinatal mental health when available.[19]
Older adults. Trait intensity may attenuate, but depression, loneliness and self-harm can persist. New-onset “borderline” behaviour in late life is a red flag for organic or mood disease.[16]
Cultural formulation. Idioms of distress, family structures and discrimination shape presentation and help-seeking. In ANZ practice, cultural safety and Indigenous health frameworks are part of competent care, not optional courtesy.[19][20]
Evidence, guidelines and controversies
Landmark psychotherapy evidence includes Linehan’s DBT programme (1991 onward), McMain DBT versus GPM, Bateman MBT trials and long-term follow-up, Giesen-Bloo schema versus TFP, Clarkin multiwave comparison, Cristea meta-analysis and Storebø Cochrane psychological therapies review.[1][2][3][4][5][6][7][8][9][10]
Pharmacotherapy evidence is sobering: Lieb and colleagues’ Cochrane-linked synthesis, the 2022 Cochrane pharmacological update, NICE-aligned commentary, and the negative LABILE lamotrigine RCT should end reflexive mood-stabiliser stacking for core BPD.[11][12][13][14]
Epidemiology and course rest on NESARC, MSAD, CLPS and major Lancet/Nature Reviews primers.[15][16][17][18][19][20]
Controversy you can discuss maturely. Whether “borderline” should be renamed; how fully ICD-11 severity replaces categorical BPD; sequencing trauma-focused therapy with BPD treatments; and how health systems resource specialised therapies equitably.[19][20]
Exam pearls
BORDERLINE — viva checklist
BORDERLINE
Biosocial + mentalization formulation (not pejorative label)
Operational criteria (DSM 5/9 or ICD-11 severity + pattern)
Risk: acute vs chronic; intent vs affect regulation; means
Differentials: bipolar, PTSD, ADHD, substances, organic
Evidence-based psychotherapy first-line (name one fully)
Review dates on any medication; LABILE kills routine lamotrigine
Least-restrictive crisis care with written safety plan
Integrated treatment of comorbidity
No nihilism — longitudinal recovery is real for many
Everyone on one team plan (anti-splitting structure)
60-second oral summary
BPD is diagnosed with DSM ≥5/9 or ICD-11 severity plus borderline pattern after excluding or co-diagnosing bipolar, trauma, ADHD, substances and organic change. Risk is dynamic: stabilise medically, separate intent from affect regulation, restrict means, safety-plan, use least-restrictive care. First-line treatment is structured psychotherapy (DBT/MBT/schema/TFP/GPM). Medications treat comorbidity or short-term targets with review dates — LABILE argues against routine lamotrigine; Cochrane/NICE argue against polypharmacy-as-cure. Longitudinal data support realistic hope with structured care.[4][9][12][14][19]
References
- [1]Linehan MM, Armstrong HE, Suarez A, Allmon D, et al. Cognitive-behavioral treatment of chronically parasuicidal borderline patients Arch Gen Psychiatry, 1991.PMID 1845222
- [2]Linehan MM, Comtois KA, Murray AM, Brown MZ, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder Arch Gen Psychiatry, 2006.PMID 16818865
- [3]Linehan MM, Korslund KE, Harned MS, Gallop RJ, et al. Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: a randomized clinical trial and component analysis JAMA Psychiatry, 2015.PMID 25806661
- [4]McMain SF, Links PS, Gnam WH, Guimond T, et al. A randomized trial of dialectical behavior therapy versus general psychiatric management for borderline personality disorder Am J Psychiatry, 2009.PMID 19755574
- [5]Bateman A, Fonagy P Randomized controlled trial of outpatient mentalization-based treatment versus structured clinical management for borderline personality disorder Am J Psychiatry, 2009.PMID 19833787
- [6]Bateman A, Fonagy P 8-year follow-up of patients treated for borderline personality disorder: mentalization-based treatment versus treatment as usual Am J Psychiatry, 2008.PMID 18347003
- [7]Giesen-Bloo J, van Dyck R, Spinhoven P, van Tilburg W, et al. Outpatient psychotherapy for borderline personality disorder: randomized trial of schema-focused therapy vs transference-focused psychotherapy Arch Gen Psychiatry, 2006.PMID 16754838
- [8]Clarkin JF, Levy KN, Lenzenweger MF, Kernberg OF Evaluating three treatments for borderline personality disorder: a multiwave study Am J Psychiatry, 2007.PMID 17541052
- [9]Cristea IA, Gentili C, Cotet CD, Palomba D, et al. Efficacy of Psychotherapies for Borderline Personality Disorder: A Systematic Review and Meta-analysis JAMA Psychiatry, 2017.PMID 28249086
- [10]Storebø OJ, Stoffers-Winterling JM, Völlm BA, Kongerslev MT, et al. Psychological therapies for people with borderline personality disorder Cochrane Database Syst Rev, 2020.PMID 32368793
- [11]Lieb K, Völlm B, Rücker G, Timmer A, et al. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials Br J Psychiatry, 2010.PMID 20044651
- [12]Stoffers-Winterling JM, Storebø OJ, Pereira Ribeiro J, Kongerslev MT, et al. Pharmacological interventions for people with borderline personality disorder Cochrane Database Syst Rev, 2022.PMID 36375174
- [13]Kendall T, Burbeck R, Bateman A Pharmacotherapy for borderline personality disorder: NICE guideline Br J Psychiatry, 2010.PMID 20118465
- [14]Crawford MJ, Sanatinia R, Barrett B, Cunningham G, et al. The Clinical Effectiveness and Cost-Effectiveness of Lamotrigine in Borderline Personality Disorder: A Randomized Placebo-Controlled Trial Am J Psychiatry, 2018.PMID 29621901
- [15]Grant BF, Chou SP, Goldstein RB, Huang B, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions J Clin Psychiatry, 2008.PMID 18426259
- [16]Gunderson JG, Stout RL, McGlashan TH, Shea MT, et al. Ten-year course of borderline personality disorder: psychopathology and function from the Collaborative Longitudinal Personality Disorders study Arch Gen Psychiatry, 2011.PMID 21464343
- [17]Zanarini MC, Frankenburg FR, Hennen J, Reich DB, et al. The McLean Study of Adult Development (MSAD): overview and implications of the first six years of prospective follow-up J Pers Disord, 2005.PMID 16274279
- [18]Lieb K, Zanarini MC, Schmahl C, Linehan MM, et al. Borderline personality disorder Lancet, 2004.PMID 15288745
- [19]Bohus M, Stoffers-Winterling J, Sharp C, Krause-Utz A, et al. Borderline personality disorder Lancet, 2021.PMID 34688371
- [20]Gunderson JG, Herpertz SC, Skodol AE, Torgersen S, et al. Borderline personality disorder Nat Rev Dis Primers, 2018.PMID 29795363