Psych · General adult psychiatry
Catatonia
Also known as Catatonic syndrome · Retarded catatonia · Excited catatonia · Malignant catatonia · Bush-Francis catatonia · Lorazepam challenge
Exam-exhaustive fellowship topic on catatonia — DSM-5-TR and ICD-11 nosology, Bush-Francis screening and severity scales, retarded versus excited phenotypes, malignant catatonia, medical and autoimmune causes, lorazepam challenge and high-dose benzodiazepine therapy, ECT, NMS overlap, and special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
4 MCQs with explanations
Target exams
Red flags
Catatonia is not a historical curiosity and is not synonymous with schizophrenia. Fellowship examiners test whether you can name the DSM-5-TR sign set, use a structured exam (Bush-Francis), run a lorazepam challenge, separate malignant catatonia from NMS, and get ECT before the patient dies of PE, aspiration, or multi-organ failure.[3][4][8][22]
Overview and definition
Catatonia is a psychomotor syndrome of abnormal motor activity, speech, and responsiveness — ranging from stuporous immobility to purposeless excitement — that occurs with mood disorders, schizophrenia-spectrum illness, autism/intellectual disability, medical and neurological disease, substances, and idiopathic presentations.[3][5][21][23]
The modern teaching line, after Fink and Taylor, is that catatonia was forgotten but not gone: under-recognised when clinicians only look for full-blown "classic" posturing in schizophrenia, yet highly responsive to benzodiazepines and ECT when identified.[3][4][9]
Classification and diagnostic criteria
DSM-5-TR — twelve signs, three contexts
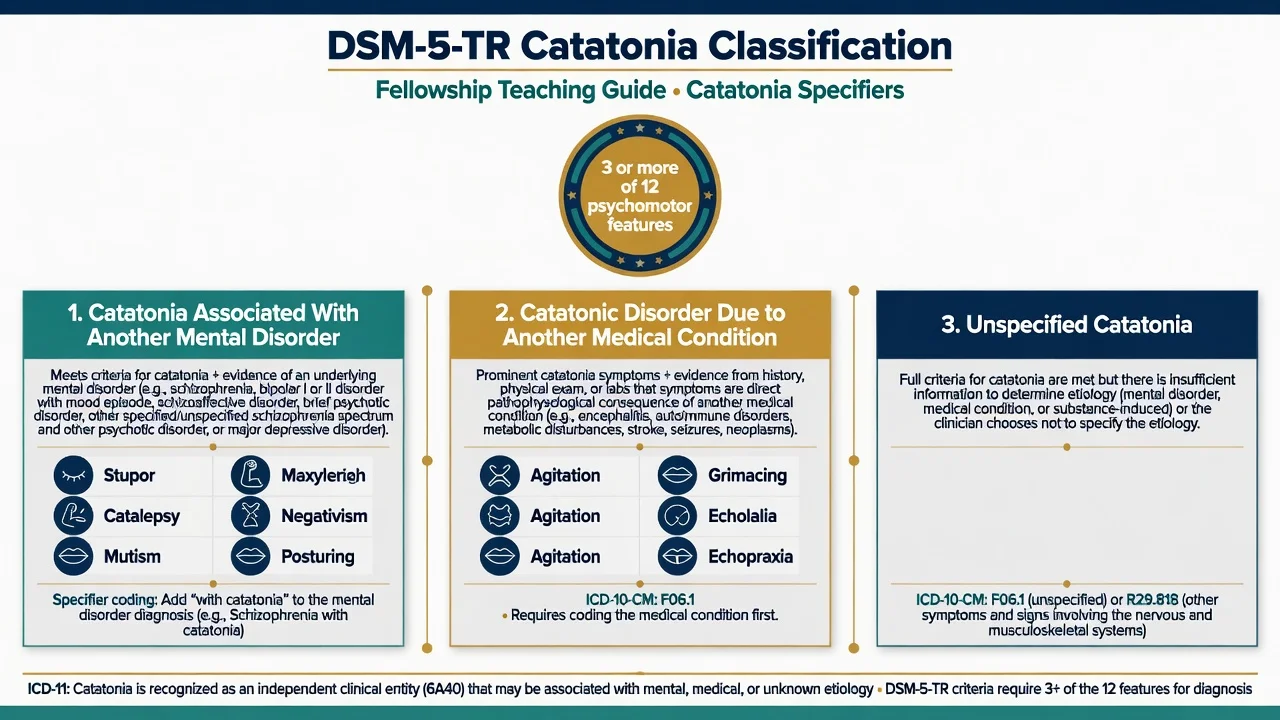
Diagnosis requires three or more of the following twelve psychomotor features:[5][6][22]
| # | Feature | Bedside meaning |
|---|---|---|
| 1 | Stupor | No psychomotor activity; not actively relating to environment |
| 2 | Catalepsy | Passive induction of a posture held against gravity |
| 3 | Waxy flexibility | Slight, even resistance to positioning by examiner |
| 4 | Mutism | No, or very little, verbal response (exclude established aphasia) |
| 5 | Negativism | Opposition or no response to instructions or external stimuli |
| 6 | Posturing | Spontaneous and active maintenance of a posture against gravity |
| 7 | Mannerism | Odd, circumstantial caricature of normal actions |
| 8 | Stereotypy | Repetitive, abnormally frequent, non-goal-directed movements |
| 9 | Agitation | Not influenced by external stimuli (excited pole) |
| 10 | Grimacing | Odd facial expressions maintained |
| 11 | Echolalia | Mimicking another's speech |
| 12 | Echopraxia | Mimicking another's movements |
Diagnostic contexts in DSM-5-TR: (1) catatonia associated with another mental disorder (specifier) — e.g. bipolar, major depression, schizophrenia spectrum; (2) catatonic disorder due to another medical condition — medical cause established; (3) unspecified catatonia — full syndrome but insufficient data for aetiology, or clinician chooses not to specify.[5][6]
ICD-11 contrast
ICD-11 treats catatonia as a clinical entity that can accompany mental disorders, medical conditions, or substance use — aligning with the "independent syndrome" argument rather than locking catatonia inside schizophrenia alone.[4][5][22]
Bush-Francis scales (exam-critical)
Bush and colleagues standardised examination and rating:[1]
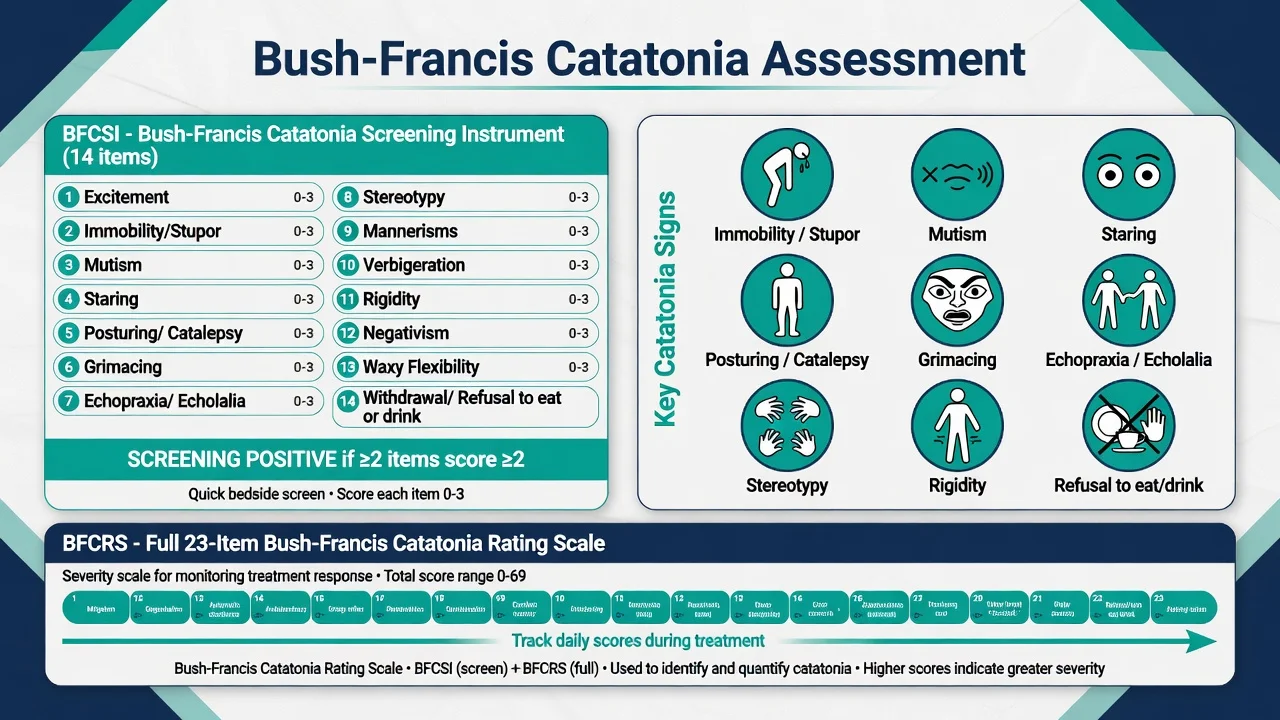
- Bush-Francis Catatonia Screening Instrument (BFCSI): first 14 items of the scale; used for detection.
- Screening threshold (classic teaching): two or more of the first 14 items rated ≥2 supports a positive screen and full examination.
- Bush-Francis Catatonia Rating Scale (BFCRS): full 23 items for severity and serial monitoring (items scored 0–3).[1][23]
Know the concept and threshold, not a memorised 23-line scoring manual for viva. Examiners want structured exam language, not vague "looks catatonic."[1][8]
Phenotypes examiners name
| Phenotype | Core picture | Immediate concern |
|---|---|---|
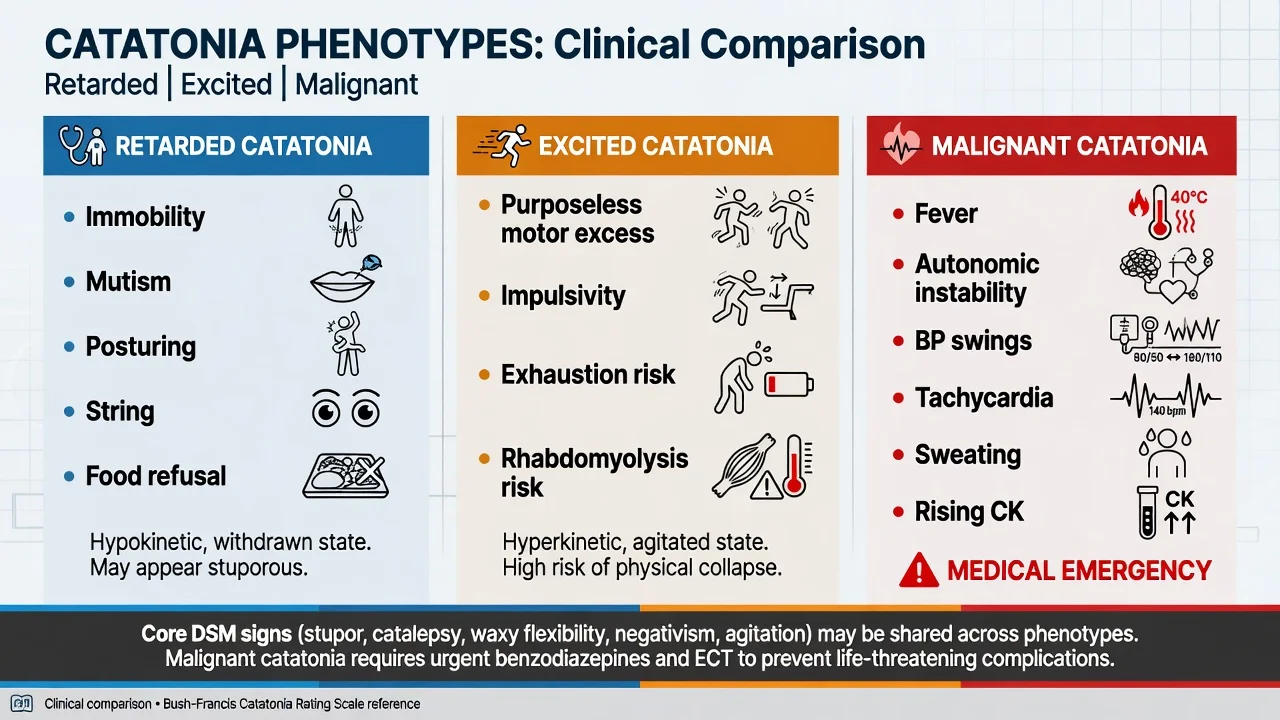
| Retarded (stuporous) | Mutism, immobility, posturing, staring, food/fluid refusal | Dehydration, VTE, aspiration, pressure injury |
| Excited | Purposeless motor excess, impulsivity, exhaustion | Rhabdomyolysis, hyperthermia, injury |
| Malignant | Catatonic signs plus fever and autonomic instability (± rising CK) | Multi-organ failure; early ECT |
Periodic catatonia (Leonhard tradition) remains an examinable historical/clinical subtype of recurrent, often familial, bipolar-like motor episodes — know the name and that modern practice still treats acute episodes with benzos/ECT while managing the primary mood/psychotic illness.[3][21]
Epidemiology and risk factors
Solmi and colleagues' meta-analysis found a pooled prevalence of catatonia of about 9% in clinical samples, with substantial heterogeneity by setting, diagnostic criteria, and whether a structured scale was used — under-detection is therefore expected when clinicians do not examine systematically.[11]
Risk contexts: bipolar mania and depression, schizophrenia spectrum, autism and intellectual disability, postpartum states, medical/neurological illness (including autoimmune encephalitis), substance intoxication/withdrawal, and abrupt benzodiazepine withdrawal in susceptible patients.[9][10][21][23]
Pathophysiology
No single molecule explains all catatonia. Viva-ready mechanisms:[7][21][23]
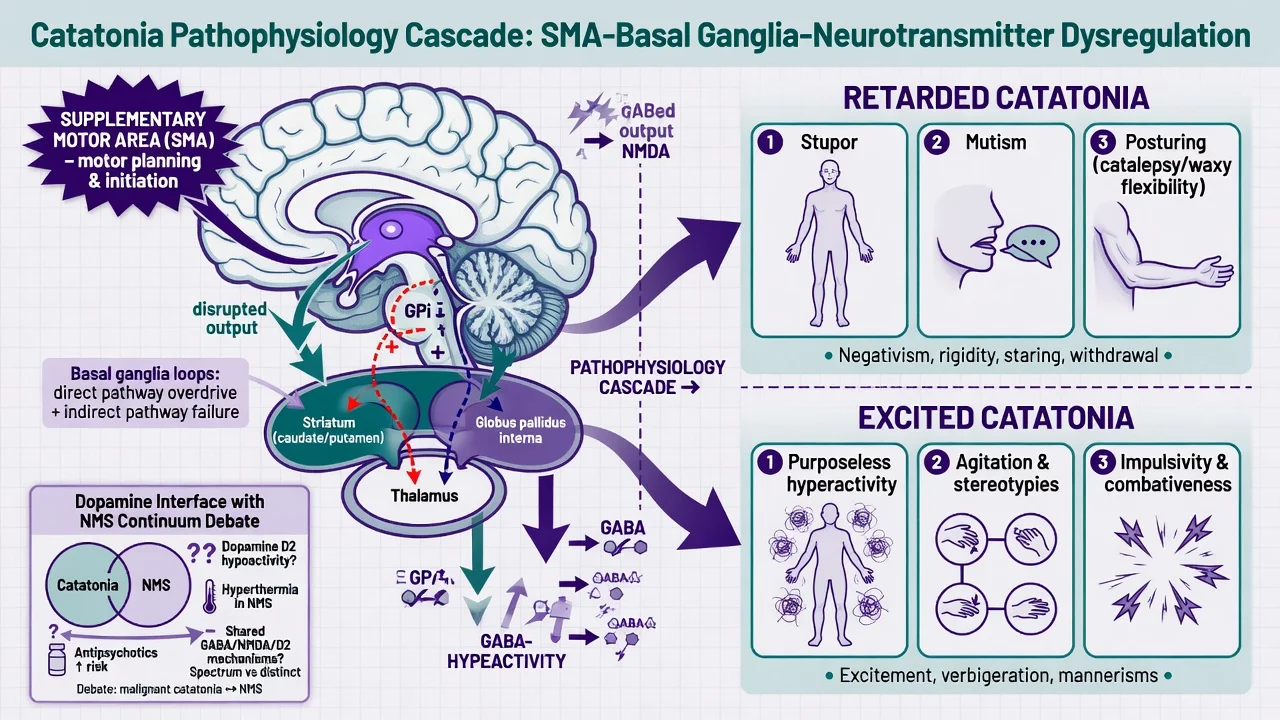
- GABAergic hypoactivity — clinical support from rapid response to lorazepam and sometimes zolpidem.
- Glutamatergic (NMDA) dysregulation — links to ECT mechanisms and anti-NMDA receptor encephalitis presentations.
- Motor network dysfunction — supplementary motor area (SMA), basal ganglia loops, and cortical inhibition abnormalities (Walther et al., Lancet Psychiatry 2019).
- Dopamine interface — continuum debate with neuroleptic malignant syndrome and malignant catatonia (Northoff); clinically treat physiology and exposure history, not the debate alone.[7][18][17]
Clinical presentation
Retarded pole
Immobility, mutism, staring, posturing/catalepsy, waxy flexibility, negativism, grimacing, and withdrawal from food and drink dominate. Patients may appear "uncooperative" when they have a motor syndrome — a classic mislabel trap.[1][9][22]
Excited pole
Purposeless, excessive motor activity not directed by external goals; risk of exhaustion, injury, and rhabdomyolysis. May be mistaken for mania, stimulant intoxication, or "agitated delirium" without a catatonia exam.[21][17]
Malignant catatonia
Philbrick and Rummans described the lethal end of the spectrum: catatonic features with hyperthermia and autonomic instability, historically high mortality without definitive treatment. Contemporary intensivist reviews reiterate multi-organ risk and the need for critical-care support plus benzodiazepines and ECT.[16][17][8]
Atypical and special presentations
Fluctuating mixed features, catatonia of autism (regression, odd posturing, refusal), and medical catatonia without a prior psychiatric history are high-yield traps.[10][23]
Differential diagnosis — discriminators
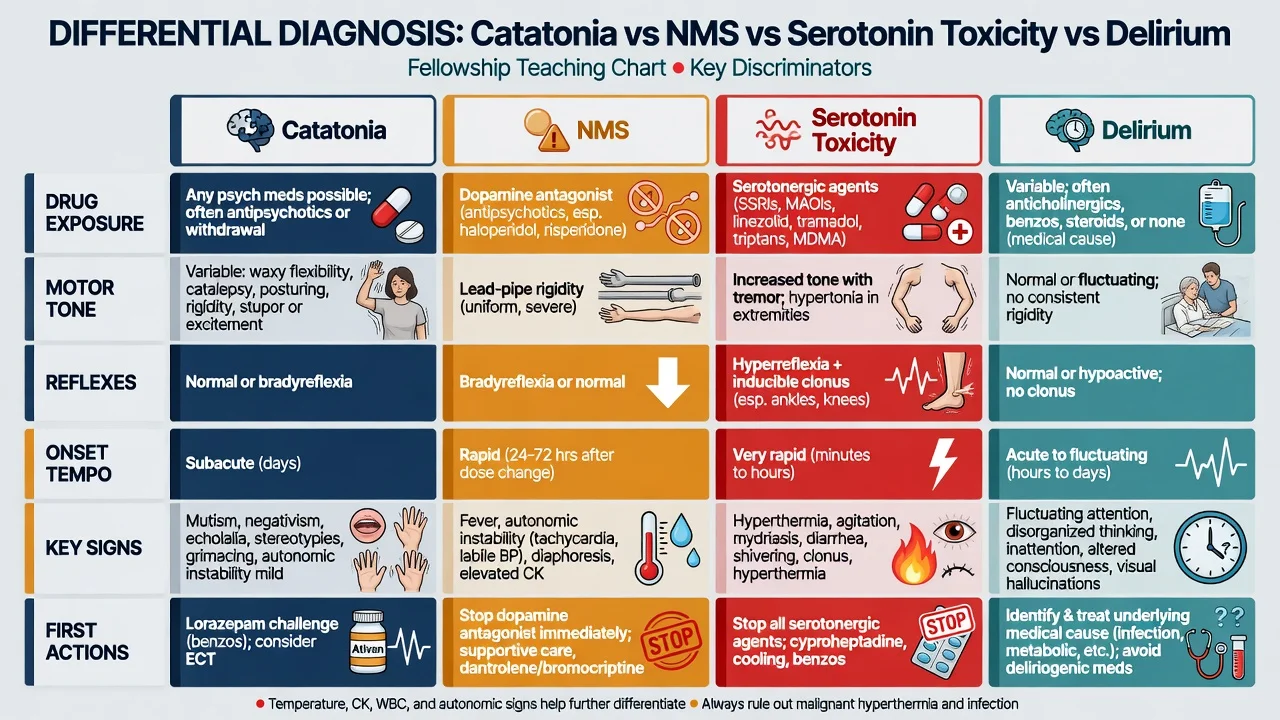
- ≥3 of 12 psychomotor signs
- Psychiatric or medical cause
- Lorazepam challenge diagnostic-therapeutic
- ECT highly effective if needed
- May lack extreme fever early
- Dopamine antagonist or agonist withdrawal
- Lead-pipe rigidity, autonomic storm, fever
- IEC thresholds (fever >38.0 C ×2; CK ≥4× ULN)
- Stop all DA antagonists first
- Overlaps malignant catatonia
- Serotonergic agents
- Clonus, hyperreflexia, myoclonus
- Faster onset often hours
- GI hyperactivity common
- Stop serotonergics; benzos ± cyproheptadine
- Fluctuating attention/awareness
- Medical driver
- Motor signs not specific catatonia cluster
- Treat cause; avoid missing concurrent catatonia
- May coexist with medical catatonia
Other can't-miss mimics: non-convulsive status epilepticus, locked-in syndrome, severe parkinsonism/EPS, acute dystonia, elective mutism, conversion/functional neurological symptom disorder, hypoactive delirium, and anti-NMDA (and other autoimmune) encephalitis.[10][21][22]
Clinical and bedside assessment
- ABCDE and vital signs every assessment if malignant risk.
- Structured catatonia exam (Bush-Francis technique): observe posture, speech, motor activity; test for catalepsy/waxy flexibility; document echolalia/echopraxia, negativism, grimacing.[1]
- Full MSE, capacity, and least-restrictive legal basis under local law (do not invent foreign section numbers).
- Medication timeline: antipsychotics (including depot/PRN), antiemetic D2 blockers, serotonergics, benzodiazepine withdrawal.
- Collateral: onset tempo, mood/psychotic prodrome, autism baseline, postpartum, infection, seizures.
- Risk: not eating/drinking, immobility (VTE), aspiration, self-injury if excited.[8][9][22]
Investigations
| Domain | Tests | When / why |
|---|---|---|
| Baseline | FBC, U&E, LFT, glucose, CRP, CK, ECG | Hydration, rhabdo, metabolic, QTc before treatment |
| Infection | Cultures, CXR, LP if indicated | Fever, meningism, encephalitis suspicion |
| Neuro | CT/MRI, EEG | First-episode, focal signs, seizures, unexplained |
| Autoimmune | Autoimmune encephalitis panel (incl. anti-NMDA) | Atypical, new psychosis + catatonia, seizures, young patient |
| Endocrine/metabolic | TFTs, B12, etc. as indicated | Medical catatonia work-up |
| Directed tox | As indicated | Intoxication/withdrawal context |
Oldham's systematic review emphasises that hospital catatonia often has a medical cause — proportions vary by setting, but the practical rule is: always consider medical aetiology, especially in CL psychiatry and first presentations.[10]
Do not delay life-saving lorazepam or ECT for an endless test list once the syndrome is clear and the patient is deteriorating.[8][17]
Management — resuscitation
Immediate priorities: airway protection and aspiration precautions; IV access and volume repletion; external cooling if hyperthermic; continuous monitoring; VTE prophylaxis and pressure care (immobility kills via PE); stop dopamine antagonists if NMS/malignant overlap plausible; emergency legal framework when incapacitous for life-saving treatment under jurisdiction-specific statutes.[8][17][9]
Management — definitive and stepwise
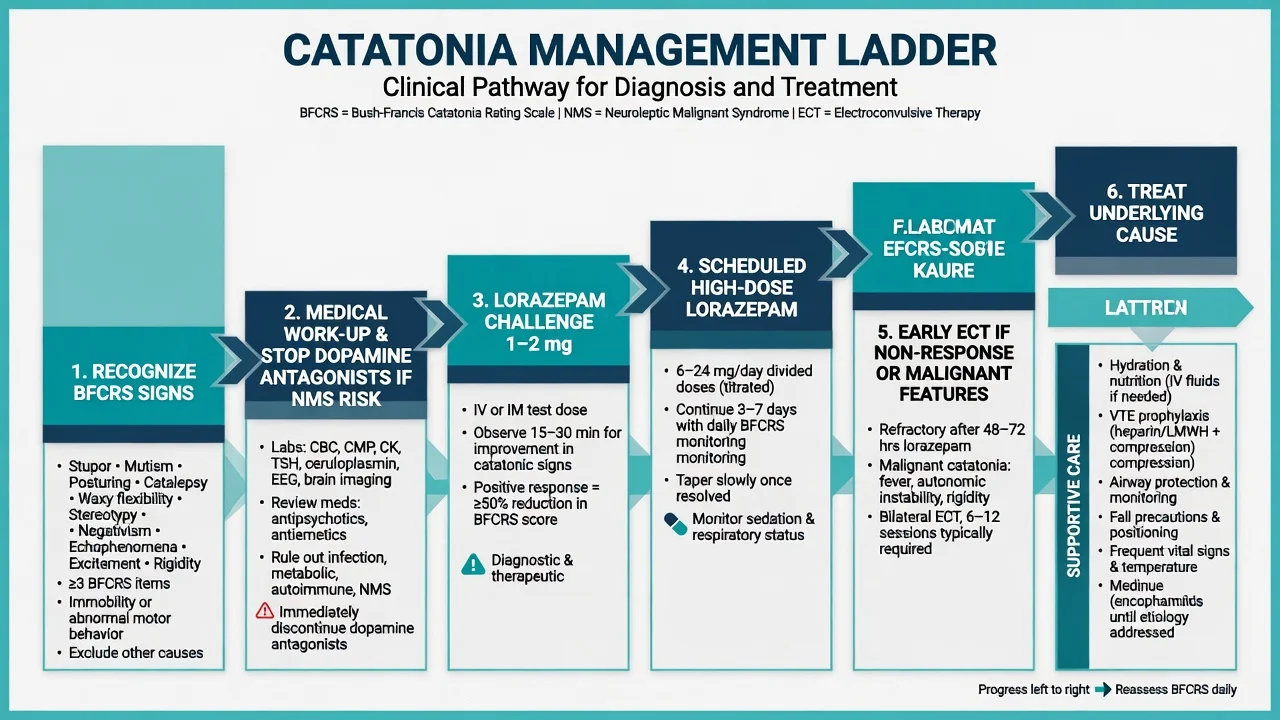
Lorazepam challenge (diagnostic and therapeutic)
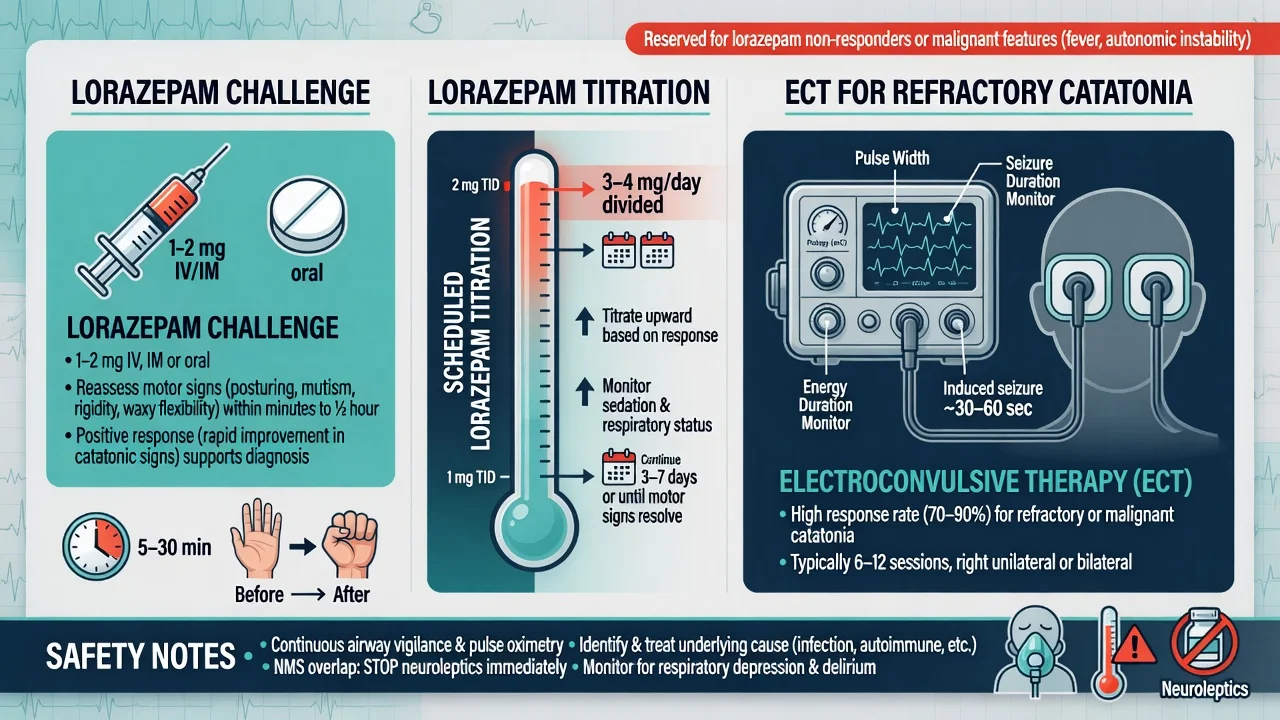
Bush part II and subsequent practice established benzodiazepines and ECT as core treatments.[2][9][8]
Typical challenge (attribute as standard teaching; titrate to local protocol): Give lorazepam 1–2 mg IV, IM, or oral (IV/IM preferred if not swallowing); reassess catatonic signs within roughly 5–30 minutes (route-dependent); a clear reduction in signs supports the diagnosis and predicts further benzo responsiveness.[2][9][15][22]
Tibrewal and colleagues reported high lorazepam response rates in a developing-country series — useful as an effectiveness signal, not a universal percentage to over-quote.[15]
Scheduled high-dose benzodiazepines
After a positive challenge (or strong clinical suspicion), schedule lorazepam and titrate to motor response with airway and sedation monitoring. Daily totals in responsive patients often reach multi-milligram divided regimens under specialist supervision; BAP 2023 provides consensus framing for modern practice. Taper slowly after resolution to avoid withdrawal-provoked relapse.[8][9][12][23]
Parenteral lorazepam availability has been intermittent in Australia — use oral or alternative parenteral benzodiazepines per local formulary while preserving the principle of adequate GABA-ergic treatment and early ECT access.[8][22]
ECT
ECT is definitive for inadequate benzodiazepine response, malignant catatonia, life-threatening refusal of food/fluids, and severe excited catatonia with medical compromise. Series report high response rates (often cited in the order of ~80–100% depending on sample and endpoint — Raveendranathan; Luchini reviews). Bilateral electrode placement is commonly used for severe catatonia; plan with anaesthesia and medical teams.[13][14][2][8][17]
Zolpidem and other adjuncts
Zolpidem appears in case literature and a recent systematic review as an alternative or adjunct when benzodiazepines are limited — evidence is weaker than for lorazepam/ECT; name it as examinable adjunct, not first-line standard.[24][12]
Antipsychotics and mood treatments
Treat the underlying mood or psychotic disorder once the motor syndrome is stabilising. Antipsychotics alone are not the treatment of the catatonic motor syndrome; introduce cautiously only after benzodiazepine cover (or ECT) and after NMS has been excluded — high-potency D2 blockade can worsen the NMS/malignant pathway.[8][9][12][18]
Systematic treatment evidence
Pelzer's systematic review supports benzodiazepines and ECT as the treatments with the strongest cumulative evidence base; quality of trials is limited (few RCTs), so guideline consensus (BAP 2023) carries heavy weight in viva answers.[12][8]
Specific subtypes and scenarios
| Scenario | Pearls |
|---|---|
| Affective catatonia | Common; treat motor syndrome + mood episode (may need ECT for both) |
| Schizophrenia-associated | Still use benzos/ECT for motor signs; do not only escalate antipsychotics |
| Medical/CL catatonia | High medical-cause probability — investigate aggressively |
| Anti-NMDA encephalitis | Catatonia + new psychosis ± seizures/dysautonomia — immunotherapy pathway |
| Autism/ID | Regression and odd motor phenomena; environmental + benzos/ECT specialist pathways |
| Perinatal | High stakes; ECT often preferred when severe with obstetric-anaesthesia planning |
| Malignant vs NMS | Stop DA antagonists; benzos + early ECT; ICU support |
| Excited / "lethal" catatonia | Historical continuum with malignant form — resuscitate, benzos, ECT |
Complications and pitfalls
- Pulmonary embolism from immobility (preventable death).
- Aspiration, dehydration, acute kidney injury, pressure injury, contractures.
- Rhabdomyolysis in excited/malignant phenotypes.
- Mislabeling as "behavioural" or "willful."
- Antipsychotic-only strategies precipitating NMS.
- Delayed ECT in malignant catatonia.
- Missing autoimmune encephalitis.
- Abrupt benzodiazepine cessation after high-dose treatment.[16][17][8][10]
Prognosis and disposition
With timely benzodiazepines and/or ECT, motor recovery is often excellent. Prognosis then tracks the underlying psychiatric or medical disease and any organ complications. Step down when the patient is eating, drinking, mobilising, and BFCRS scores are falling; continue cause-specific treatment and a written relapse plan (early re-challenge with lorazepam, rapid ECT re-access).[9][13][8][23]
Disposition: medical HDU/ICU for malignant features; otherwise inpatient psychiatry or CL with nursing capacity for immobility care and legal frameworks for treatment.[17][8]
Special populations
- Older adults: medical causes more likely; benzodiazepine fall/respiratory risk — still treat the syndrome; consider earlier ECT.
- Children/adolescents and autism: same principles; specialist ECT pathways where indicated.
- Pregnancy: prioritise maternal survival; ECT is often preferred for severe catatonia with obstetric anaesthesia planning.
- Intellectual disability: baseline motor mannerisms complicate diagnosis — look for change from baseline.
- Parkinson disease / DLB: extreme caution with antipsychotics; NMS-like vulnerability.[8][10][13][23]
Evidence, guidelines, and regional practice
In Australia and New Zealand, catatonia is managed with local medical and ECT pathways. Parenteral lorazepam supply has been a practical constraint — preserve adequate benzodiazepine dosing by available routes and escalate to ECT early when oral strategies fail or malignant features appear. FRANZCP viva answers should name Bush-Francis, lorazepam challenge, BAP-aligned ladder, and NMS overlap without inventing statute numbers.[8][2][22]
Landmark names to drop in viva: Bush 1996 I/II; Fink and Taylor; Tandon/Heckers DSM-5 catatonia; Walther neural mechanisms; Solmi prevalence meta-analysis; Pelzer treatment review; Rosebush treatment; Philbrick malignant catatonia; BAP 2023.[1][2][3][5][7][8][11][12][16]
Exam pearls
CATATONIC
- Mutism alone is not catatonia — need the cluster (≥3 signs).[5]
- Positive lorazepam challenge is both diagnostic support and therapy.[2][9]
- Malignant catatonia is a medical emergency; ECT is not "last resort folklore."[16][17][8]
- Mood disorders frequently associate with catatonia — do not default to schizophrenia only.[4][11]
- Name BAP 2023 as the modern consensus management standard.[8]
- VTE prophylaxis for immobile patients is a preventable-death pearl.[17][8]
Self-test: 30-second stem
A 24-year-old woman becomes mute and immobile with posturing and negativism three days after a manic relapse. Temperature 38.7 C, HR 130, BP swinging, CK rising. She received IM olanzapine yesterday. What is your diagnosis set and first actions? Model: Malignant catatonia with NMS overlap. Stop dopamine antagonists; ABCDE, cooling, IV fluids, ICU/HDU; lorazepam now; urgent ECT planning; investigate infection/encephalitis; do not give more antipsychotic.[16][17][8][19]
References
- [1]Bush G, Fink M, Petrides G, et al. Catatonia. I. Rating scale and standardized examination Acta Psychiatr Scand, 1996.PMID 8686483
- [2]Bush G, Fink M, Petrides G, et al. Catatonia. II. Treatment with lorazepam and electroconvulsive therapy Acta Psychiatr Scand, 1996.PMID 8686484
- [3]Fink M, Taylor MA The catatonia syndrome: forgotten but not gone Arch Gen Psychiatry, 2009.PMID 19884605
- [4]Fink M, Shorter E, Taylor MA Catatonia is not schizophrenia: Kraepelin's error and the need to recognize catatonia as an independent syndrome in medical nomenclature Schizophr Bull, 2010.PMID 19586994
- [5]Tandon R, Heckers S, Bustillo J, et al. Catatonia in DSM-5 Schizophr Res, 2013.PMID 23806583
- [6]Heckers S, Tandon R, Bustillo J Catatonia in the DSM--shall we move or not? Schizophr Bull, 2010.PMID 19933711
- [7]Walther S, Stegmayer K, Wilson JE, et al. Structure and neural mechanisms of catatonia Lancet Psychiatry, 2019.PMID 31196794
- [8]Rogers JP, Oldham MA, Fricchione G, et al. Evidence-based consensus guidelines for the management of catatonia: Recommendations from the British Association for Psychopharmacology J Psychopharmacol, 2023.PMID 37039129
- [9]Rosebush PI, Mazurek MF Catatonia and its treatment Schizophr Bull, 2010.PMID 19969591
- [10]Oldham MA The Probability That Catatonia in the Hospital has a Medical Cause and the Relative Proportions of Its Causes: A Systematic Review Psychosomatics, 2018.PMID 29776679
- [11]Solmi M, Pigato GG, Roiter B, et al. Prevalence of Catatonia and Its Moderators in Clinical Samples: Results from a Meta-analysis and Meta-regression Analysis Schizophr Bull, 2018.PMID 29140521
- [12]Pelzer AC, van der Heijden FM, den Boer E Systematic review of catatonia treatment Neuropsychiatr Dis Treat, 2018.PMID 29398916
- [13]Luchini F, Medda P, Mariani MG, et al. Electroconvulsive therapy in catatonic patients: Efficacy and predictors of response World J Psychiatry, 2015.PMID 26110120
- [14]Raveendranathan D, Narayanaswamy JC, Reddi SV Response rate of catatonia to electroconvulsive therapy and its clinical correlates Eur Arch Psychiatry Clin Neurosci, 2012.PMID 22207031
- [15]Tibrewal P, Narayanaswamy J, Zutshi A, et al. Response rate of lorazepam in catatonia: a developing country's perspective Prog Neuropsychopharmacol Biol Psychiatry, 2010.PMID 20804808
- [16]Philbrick KL, Rummans TA Malignant catatonia J Neuropsychiatry Clin Neurosci, 1994.PMID 7908547
- [17]Connell J, Oldham M, Pandharipande P, et al. Malignant Catatonia: A Review for the Intensivist J Intensive Care Med, 2023.PMID 35861966
- [18]Northoff G Catatonia and neuroleptic malignant syndrome: psychopathology and pathophysiology J Neural Transm (Vienna), 2002.PMID 12486486
- [19]Gurrera RJ, Caroff SN, Cohen A, et al. An international consensus study of neuroleptic malignant syndrome diagnostic criteria using the Delphi method J Clin Psychiatry, 2011.PMID 21733489
- [20]Perry PJ, Wilborn CA Serotonin syndrome vs neuroleptic malignant syndrome: a contrast of causes, diagnoses, and management Ann Clin Psychiatry, 2012.PMID 22563571
- [21]Daniels J Catatonia: clinical aspects and neurobiological correlates J Neuropsychiatry Clin Neurosci, 2009.PMID 19996245
- [22]Rogers JP, Zandi MS, David AS The diagnosis and treatment of catatonia Clin Med (Lond), 2023.PMID 37236789
- [23]Rasmussen SA, Mazurek MF, Rosebush PI Catatonia: Our current understanding of its diagnosis, treatment and pathophysiology World J Psychiatry, 2016.PMID 28078203
- [24]Gunther M, Tran N, Jiang S Zolpidem for the Management of Catatonia: A Systematic Review J Acad Consult Liaison Psychiatry, 2025.PMID 39522949