Psych · General adult psychiatry — clinical high risk / attenuated psychosis
Clinical high risk and attenuated psychosis syndrome
Also known as Clinical high risk · CHR · CHR-P · Ultra-high risk · UHR · Attenuated psychosis syndrome · APS · At-risk mental state · ARMS · Prodromal psychosis · CAARMS · SIPS · BLIPS
Exam-exhaustive fellowship reference on clinical high risk (CHR) and ultra-high risk (UHR) for psychosis — APS/BLIPS/genetic-risk criteria, CAARMS and SIPS instruments, conversion rates and predictors, DSM-5-TR attenuated psychosis syndrome as Section III construct, indicated prevention evidence (CBT, omega-3 equipoise, antipsychotics not first-line), monitoring and escalation to FEP. Distinct from the first-episode psychosis pathway monograph. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Clinical high risk for psychosis (also called ultra-high risk, at-risk mental state, or prodromal risk in older literature) is one of the highest-yield early-intervention topics after frank first-episode psychosis. Examiners test whether you can define the three UHR boxes, quote realistic conversion rates without fatalism, name CAARMS/SIPS, distinguish DSM-5-TR attenuated psychosis syndrome as a research construct, and defend a stepped plan that does not default to long-term antipsychotics.[1][2][18][21]
This monograph is the risk state and indicated prevention leaf. The operational pathway once frank psychosis is established lives in the first-episode psychosis topic.[7][21]
Overview and definition
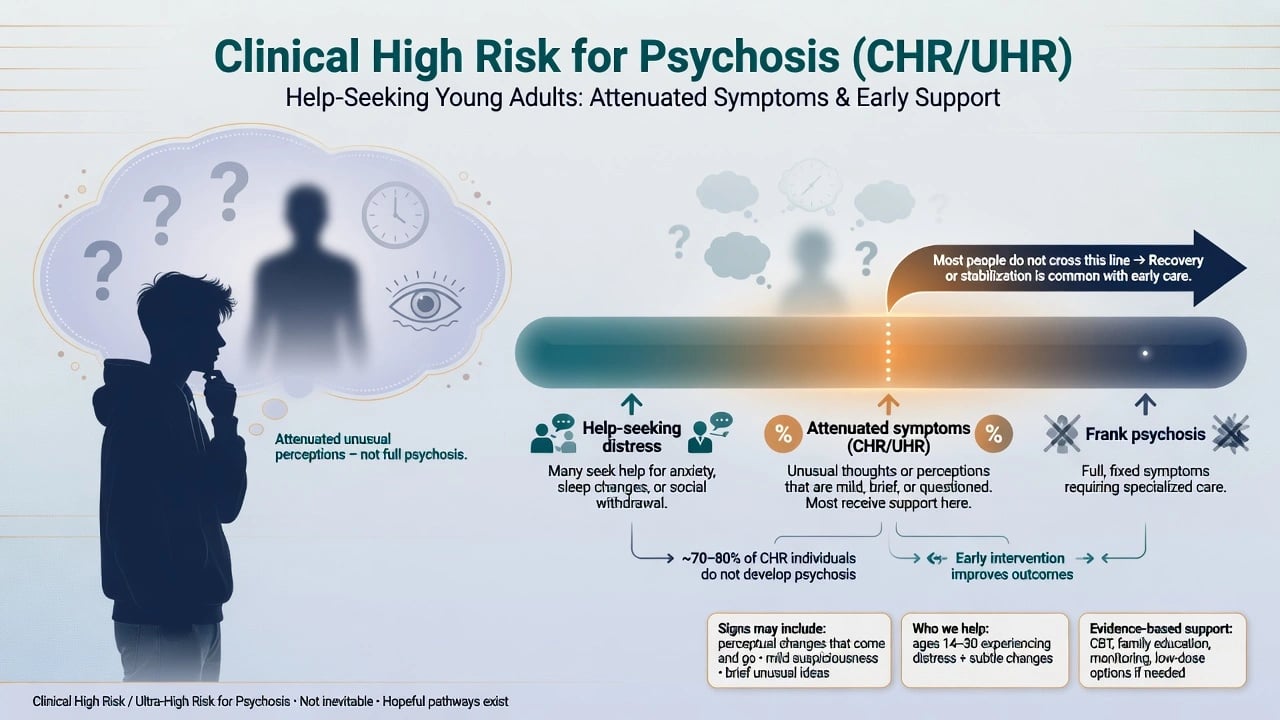
CHR / CHR-P / UHR describe help-seeking individuals with subthreshold or briefly threshold psychotic experiences plus clinical need (distress, functional drop, or help-seeking) who do not yet meet criteria for a full psychotic disorder requiring FEP pathway care. The constructs are service and research categories, not a single DSM primary diagnosis you stamp for life.[1][3][7]
Attenuated Psychosis Syndrome (APS) in DSM-5 / DSM-5-TR is listed as a condition for further study (Section III) — attenuated delusions, hallucinations, or disorganised speech of sufficient severity/frequency to warrant clinical attention, with intact reality testing enough that full psychotic disorder is not met, plus distress/disability and recent onset or worsening. It is not a fully authorised Axis-I-style primary code for routine lifelong labelling.[18]
Why the construct exists. Indicated prevention aims to detect people already distressed and enriched for later psychosis risk, offer care for current morbidity, and possibly reduce transition — while accepting large false-positive rates if the label is used carelessly outside help-seeking enriched samples.[4][7]
[6] [10]Classification
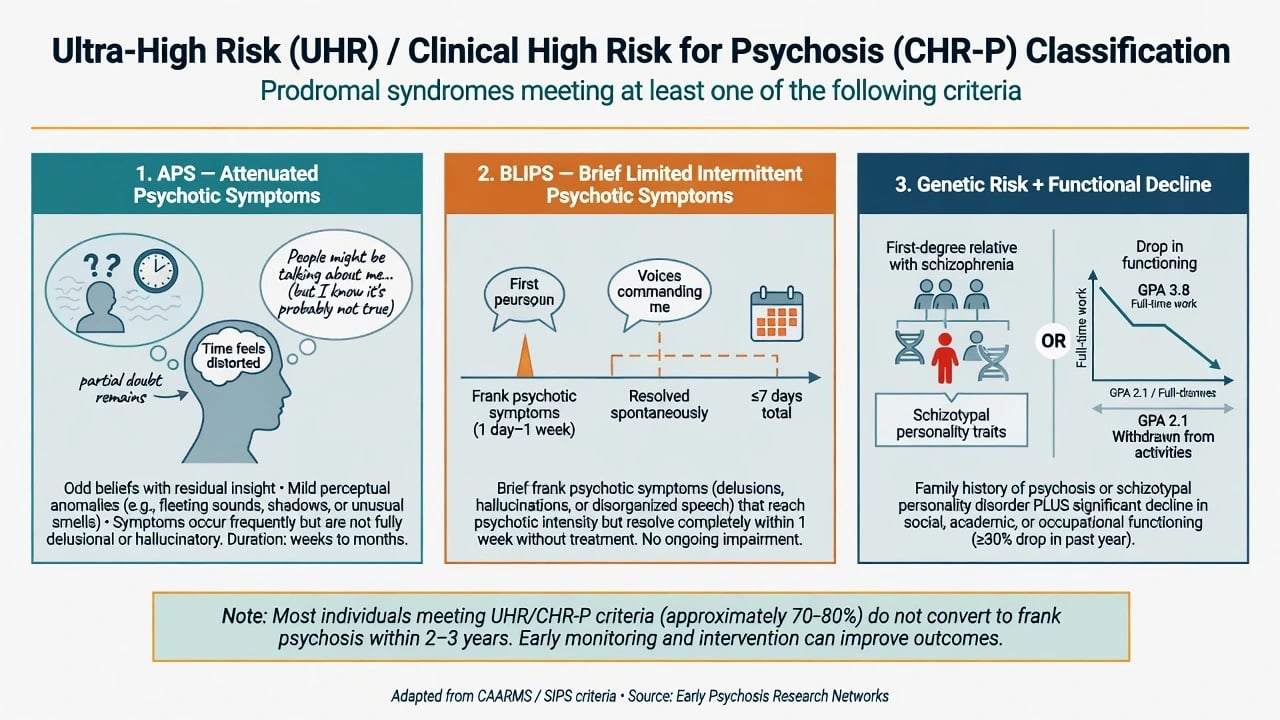
The three classic UHR / CHR entry groups
APS / attenuated positives
- Odd beliefs with residual doubt or partial insight
- Perceptual anomalies that are brief, questioned, or not fully externalised
- Mild thought disorder or referential ideas without fixed conviction
- Commonest CHR pathway into services
BLIPS
- Brief frank psychotic symptoms that resolve
- Historically framed as limited duration and frequency thresholds on structured tools
- Highest transition risk among the three groups in stratified meta-analysis
- Recurrent non-resolving BLIPS → reassess for FEP
Genetic risk + decline (GRD)
- First-degree relative with psychotic disorder and/or schizotypal traits
- Plus significant functional decline (often operationalised ~30% drop)
- Lowest transition risk of the three classic boxes
- Still needs functional and comorbidity care
Not CHR
- Sustained full-threshold psychosis → FEP pathway
- Isolated oddness without clinical need or structured criteria
- Primary delirium/organic syndrome
- Using 'prodrome' for late-onset first psychosis after 40
CAARMS (Comprehensive Assessment of At-Risk Mental States) operationalises UHR groups with severity, frequency and duration anchors used widely in Australasian and international research services.[1]
SIPS / SOPS (Structured Interview for Prodromal Syndromes / Scale of Prodromal Symptoms) operationalises parallel North American CHR syndromes (attenuated positive symptom syndrome, brief intermittent psychotic syndrome, genetic risk and deterioration).[2]
Basic symptoms (COPER/COGDIS) capture subjectively experienced cognitive-perceptual disturbances (German tradition) and can complement positive-symptom UHR criteria rather than replace them.[20]
ICD-11 / DSM-5-TR divergence for exams. Neither manual makes UHR a routine full clinical diagnosis equivalent to schizophrenia. DSM offers APS for further study; ICD-11 clinicians may code related phenomena under other primary syndromes plus Z-type risk/service language depending on jurisdiction. State the research instrument and clinical need, not a fake universal ICD code for "prodrome."[18][21]
Epidemiology and risk
Headline CHR numbers examiners expect
Early meta-analysis of clinical high-risk samples estimated substantial transition risk accumulating over 1–3 years of follow-up (classically cited near one in three by three years in enriched help-seeking cohorts).[4] Updated synthesis shows heterogeneous and often lower transition probabilities as services expand and samples dilute — examiners still accept a working range that most people do not convert within medium-term follow-up.[6][7]
Stratified risk. Meta-analytic stratification shows BLIPS groups carry the highest transition risk, attenuated symptom groups intermediate risk, and genetic-risk-plus-decline the lowest among the classic three — do not treat all CHR labels as identical risk.[5]
Long-term course (PACE 400). Long-term follow-up of a large UHR cohort demonstrates that transition can still occur beyond early years, but many never develop a psychotic disorder; non-psychotic outcomes and persistent disability remain clinically important even without conversion.[10]
Prediction enrichment. Multisite NAPLS work and European EPOS prediction research support combining clinical severity, function, and other markers to refine risk beyond crude UHR status alone — useful for research and specialist services, not as a bedside crystal ball.[8][9]
Comorbidity load. Depressive and anxiety disorders are extremely common in ARMS/CHR samples and drive distress and help-seeking; they must be treated on their own merits and can influence trajectory discussions.[19]
Cannabis. High-frequency and high-potency cannabis use contributes to variation in psychotic disorder incidence at population level (EU-GEI) and is a high-yield counselling target in any CHR plan.[23]
Pathophysiology / mechanisms
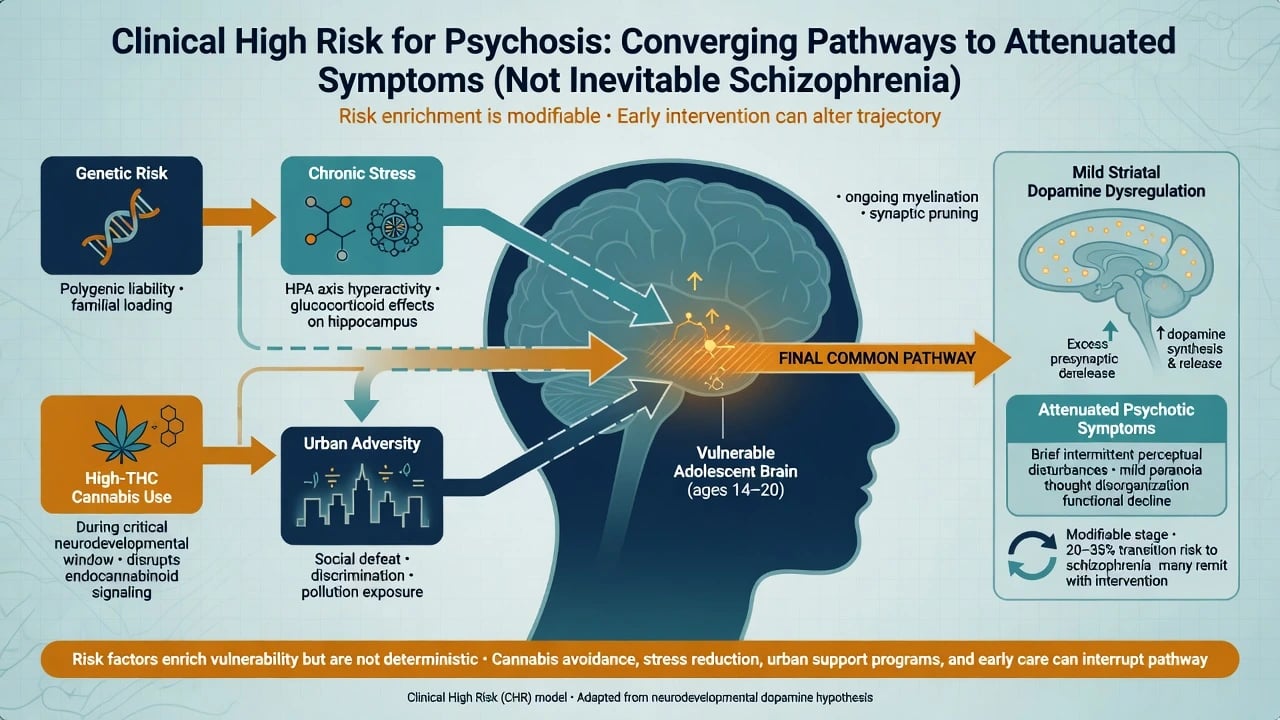
Think risk enrichment, not fate. Polygenic liability, developmental stress, social defeat, and cannabis exposure can converge on stress–vulnerability pathways and mild striatal dopamine dysregulation that maps onto attenuated positives — the same pharmacological final common pathway later targeted in frank psychosis, but without equating CHR with established schizophrenia neurobiology.[7][23]
Basic symptoms sit conceptually earlier as subjectively felt cognitive-perceptual disturbances before fully externalised attenuated positives — a useful viva layer when examiners ask about continental European traditions.[20]
Clinical presentation
Attenuated positive symptoms. The person reports ideas of reference they still half-reject ("maybe people are talking about me, but I know it is probably anxiety"), fleeting perceptual anomalies (shadows, name being called, brief murmurs) with preserved reality testing, mild suspiciousness, or odd magical thinking that has intensified and is impairing study or relationships.[1][2]
MSE language examiners want. Quote content, rate conviction (0–100%), insight fragments, frequency, and impact on behaviour. Fixed conviction with acting-as-if-true and no residual doubt is not attenuated — that is frank delusion territory and may already be FEP.[1]
Functional decline. Falling grades, social withdrawal, sleep collapse, and occupational drop often bring families to clinic even more than the odd beliefs themselves.[3]
BLIPS presentation. A short run of frank voices or persecutory certainty that remits within the tool's duration rules — history taking must pin start, stop, and residual insight carefully.[5]
Atypical stems. High-functioning student hiding symptoms; cultural content that is still new, distressing and impairing; cannabis-amplified perceptual oddness; autism with atypical beliefs needing careful discrimination; adolescent trauma with hypervigilance mislabelled as paranoia.[19][21]
Differential diagnosis
Win the differential on insight residual, duration, organicity, substance timeline, and mood chronology.[7][21]
| Competing label | Discriminators favouring that label | Discriminators favouring CHR/UHR |
|---|---|---|
| Frank FEP | Fixed delusions/hallucinations, sustained full threshold, behavioural conviction | Residual doubt, intermittent attenuated intensity, structured tools still subthreshold |
| Substance-induced | Tight lock to intoxication/withdrawal; remits with abstinence | Symptoms outlast substance windows; UHR criteria independent of use (still treat both) |
| OCD / poor insight | Ego-dystonic intrusive thoughts with resistance rituals | Externally attributed unusual beliefs more than classic obsessions |
| PTSD / dissociation | Trauma chronology, flashbacks, dissociative gaps | New referential/perceptual content without trauma phenomenology |
| Autism-related oddness | Lifelong social-communication pattern | Clear recent intensification beyond baseline autistic traits |
| Schizotypal personality | Enduring pattern from early adulthood | Recent worsening plus functional drop meeting UHR duration rules |
| Organic / autoimmune | Fever, seizure, focal signs, cognitive crash | Isolated attenuated positives in medically well youth |
| [7][21] |
Assessment
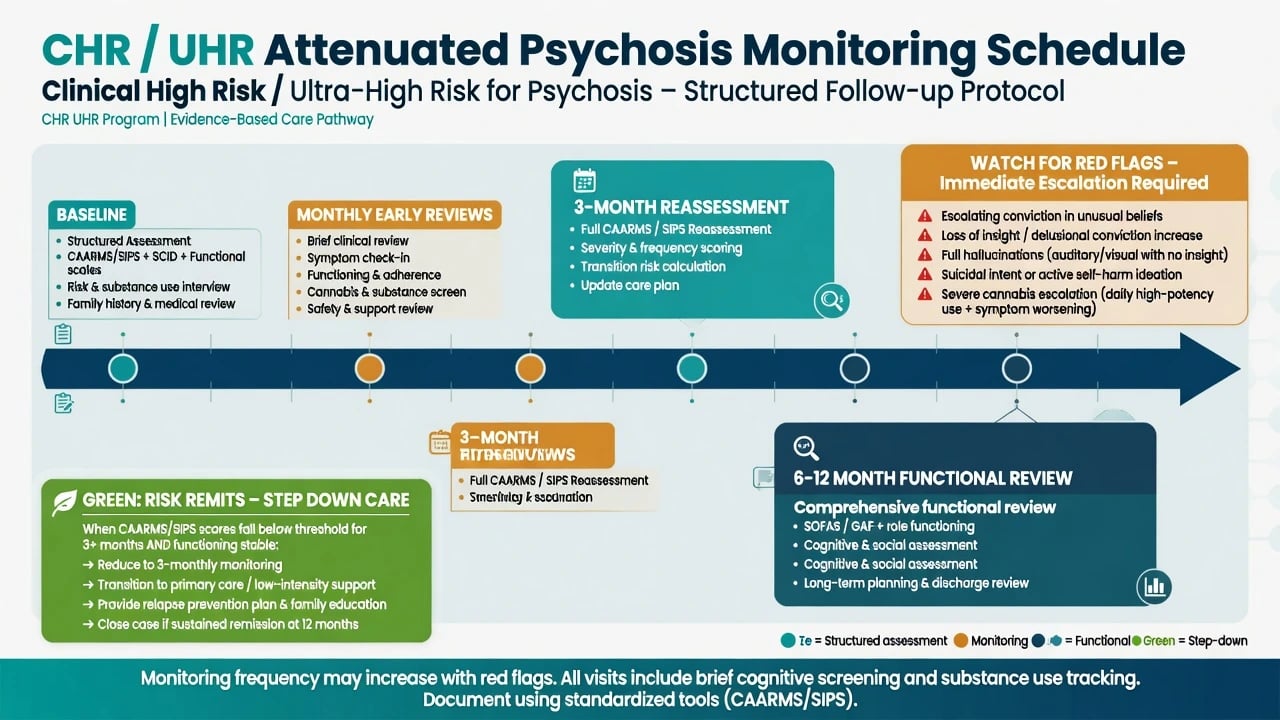
Structure every CHR assessment for the viva with safety, collateral, structured symptom inventory, function, family history, substance use, comorbidity, capacity, CAARMS or SIPS when available, and physical examination when red flags fire.[1][2][19][21]
- Safety first — suicide, self-harm, violence, vulnerability, child protection.
- Collateral — family, school, GP, digital behaviour change.
- Symptom inventory — onset, frequency, conviction, insight, behavioural impact.
- Functional trajectory — study/work/self-care drop with dates.
- Family history of psychotic illness; developmental and trauma history.
- Substance timeline — cannabis frequency, THC potency, stimulants, last use.
- Comorbidity screen — depression, anxiety, OCD, PTSD, autism.
- Capacity for the specific decision (sharing information, psychological treatment, off-label medication if contemplated).
- Structured instrument — CAARMS or SIPS when available in specialist service.
- Physical examination and observations when red flags fire.[1][2][21]
Investigations
For pure attenuated presentations without medical red flags: focused history, physical exam as indicated, urine drug screen as adjunct, and full metabolic/ECG baseline before any antipsychotic if one is later justified. Imaging, EEG, LP or autoimmune panels follow red flags (late onset, seizure, fever, focal neurology, rapid cognitive decline) — not as a ritual for every anxious 17-year-old with fleeting shadows.[21]
When the threshold is crossed into FEP, complete the full first-episode baseline suite immediately (weight/BMI, BP, glucose or HbA1c, lipids, FBC, U&E, LFT, ECG QTc, pregnancy test when relevant).[21]
Acute / emergency management
De-escalate; assess risk; treat agitation with least restrictive means; involve family; document safety plan and crisis contacts. Do not use high-dose antipsychotics as default "psychosis prevention" in the ED for isolated attenuated symptoms without specialist rationale. If frank psychosis is present, switch to FEP acute pathway (oral first, IM when needed for safety; avoid IM olanzapine with parenteral benzodiazepine).[7][21]
Definitive management — stepped indicated prevention
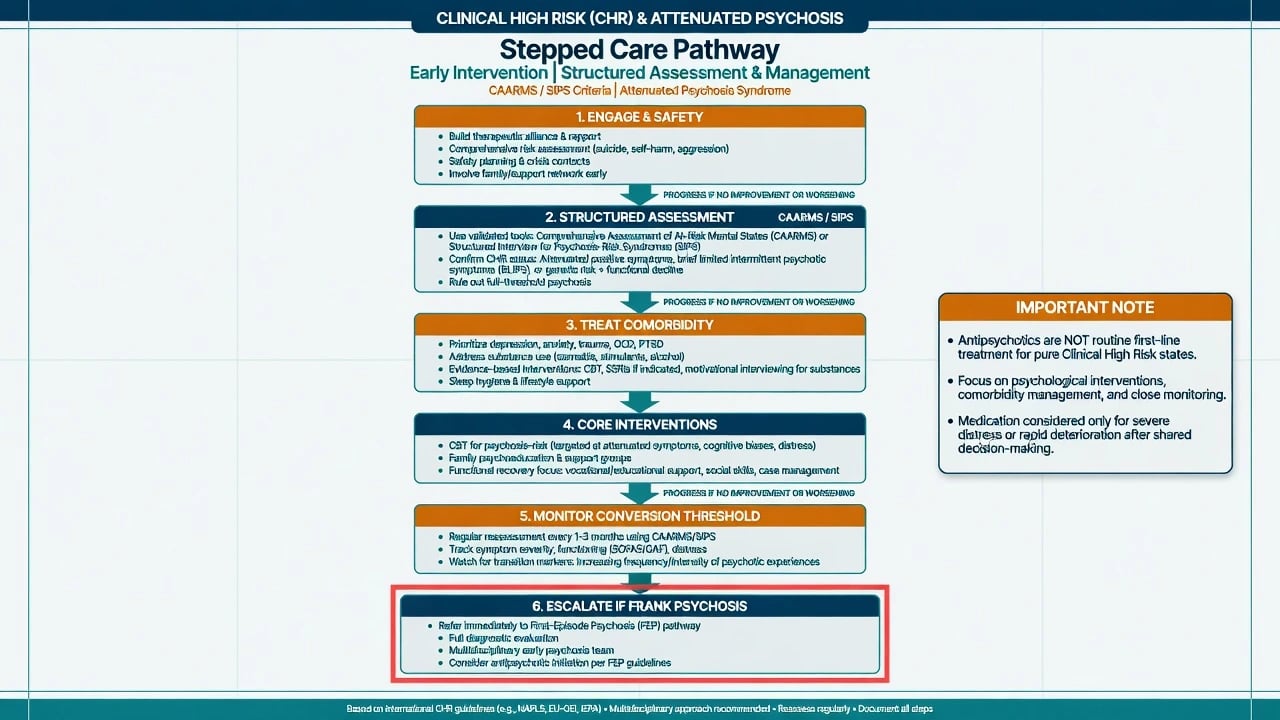
Core principles
- Engage and reduce stigma — explain risk language carefully; avoid fatalism.
- Treat current morbidity — depression, anxiety, sleep, trauma, substance use.
- Psychological intervention first-line for the risk state in most guidelines and evidence syntheses.
- Family psychoeducation and functional recovery (education/work support).
- Monitor conversion threshold on a defined schedule.
- Escalate to FEP multi-element care the moment frank sustained psychosis is confirmed.[7][14][21][22]
Psychological therapies
Cognitive behavioural approaches targeting appraisal of anomalous experiences, safety behaviours, and distress have been tested in indicated prevention (including EDIE-2 multisite CBT evaluation) and in meta-analyses of prevention trials showing reduced transition at 12 months and longer in pooled analyses of psychological and other experimental strategies versus control conditions.[13][14]
Omega-3 fatty acids — exam equipoise
Amminger 2010 reported that long-chain omega-3 polyunsaturated fatty acids reduced transition versus placebo in a UHR sample — a landmark positive signal.[15] NEURAPRO (multicentre RCT) did not replicate a transition benefit of omega-3 versus placebo on the primary outcome, in a context of relatively low overall transition and high psychosocial care quality.[16] Fellowship stance: discuss as optional adjunct with honest equipoise; do not present omega-3 as proven mandatory prevention.[16][17]
Antipsychotics — not routine first-line for pure CHR
McGorry 2002 tested interventions including low-dose risperidone plus CBT versus needs-based care for subthreshold symptoms and reported reduced progression in the experimental arm during treatment, with attenuation of differences later — proof of concept for indicated prevention, not a mandate for universal long-term neuroleptics.[11] McGlashan olanzapine prodromal RCT suggested possible symptom benefit with clear metabolic cost and incomplete prevention certainty — classic exam trade-off.[12]
Network meta-analysis (Davies 2018) found no clear ranking of a single superior preventive intervention across trials — humility over hype.[17]
If a specialist starts an antipsychotic for severe attenuated distress, rapid deterioration, or near-threshold symptoms after shared decision-making, use FEP-like low doses with full monitoring (example approach often discussed: aripiprazole 5–10 mg orally daily with akathisia and metabolic monitoring) — and document the indication, consent, and review date. This is specialist, not default community practice for every APS research-criteria youth.[12][21]
Staged adaptive care
The STEP sequential multiple assignment randomised trial tests staged adaptive strategies targeting remission and functional recovery in UHR youth — exam pearl for modern sequential care thinking beyond a single one-size package.[22]
Regional deltas
RANZCP schizophrenia guidance emphasises early detection, youth-friendly services, and careful psychopharmacology — apply least-harm principles to subthreshold states.[21] NICE and APA early-psychosis frameworks prioritise psychological care, family work, and monitoring for at-risk presentations, with antipsychotics reserved when benefits clearly outweigh metabolic and stigma harms or when frank psychosis emerges. State your jurisdiction's youth early-psychosis pathway rather than inventing foreign section numbers.
Subtypes and scenarios
- APS + major depression: treat depression fully; do not wait for conversion to start an antidepressant when indicated; still monitor positives.[19]
- BLIPS recurrent: shorten review interval; low threshold to reclassify as FEP.[5]
- GRD without attenuated positives: functional rehabilitation and family work dominate; avoid over-medication.[5]
- Cannabis-amplified CHR: motivational reduction of high-THC use is core secondary prevention.[23]
- False-positive risk label: plan explicit step-down when criteria remit to limit stigma.[10]
Complications and pitfalls
- Premature identity as "schizophrenic" without frank illness.
- Metabolic harm from unnecessary long-term antipsychotics.[12]
- Missing suicide risk while obsessing over conversion percentages.[19]
- Missing organic disease under a fashionable CHR label.
- Ignoring family and school systems.
- Over-promising that CBT or omega-3 "guarantees" no psychosis.[17]
Prognosis and disposition
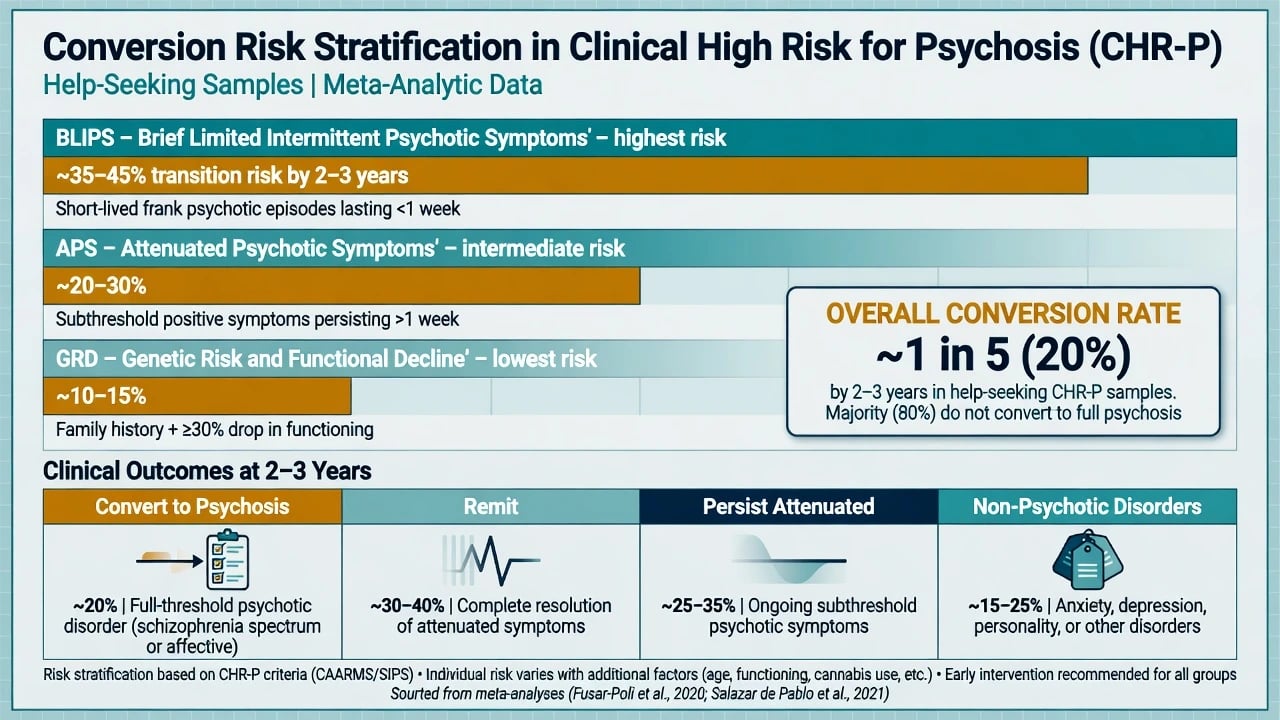
Prognosis. Many remit from the risk state; some persist with attenuated symptoms or non-psychotic disorders; a minority convert, with higher rates in BLIPS and in more severely impaired enriched samples.[5][6][10]
Disposition. Prefer specialist youth / early-psychosis assessment and monitoring clinics with clear escalation to multi-element FEP care. Step down when criteria remit and function stabilises. Keep crisis contacts active throughout.[7][21]
Practical monitoring cadence (service-dependent). Early reviews every 1–4 weeks while unstable; structured CAARMS/SIPS recheck at intervals such as 3 months; faster review if conviction, frequency, or risk escalate. Document conversion threshold language the whole team understands.[1][2][7]
Special populations
- Adolescents: assent/consent complexity; school liaison; avoid adult-style lifelong labelling.[21]
- Cultural formulation: unusual beliefs may be culturally sanctioned — still assess newness, distress, fixity, and impairment.[21]
- Autism / intellectual disability: baseline oddness versus true recent risk-state change.[21]
- Older adults: do not paste "UHR" onto late-onset presentations; run organic-first late-onset psychosis thinking.[21]
- Indigenous peoples (ANZ): culturally safe assessment, family/kin structures, and local service pathways under RANZCP principles.[21]
Evidence and guidelines
Landmark papers and how to use them in the viva are summarised below — name the trial or meta-analysis, state the clinical implication, and avoid over-claiming a single preventive magic bullet.[4][7][17]
| Landmark | What to say in the viva |
|---|---|
| Yung CAARMS; Miller SIPS | Structured operationalisation of UHR/CHR |
| Fusar-Poli 2012; Salazar de Pablo 2021 | Transition rates and updates |
| Fusar-Poli 2016 heterogeneity | BLIPS greater than APS greater than GRD risk |
| Cannon NAPLS; Ruhrmann EPOS | Prediction enrichment beyond crude status |
| Nelson PACE 400 | Long-term heterogeneity of outcomes |
| McGorry 2002; McGlashan 2006 | Early intervention drug/psychosocial experiments; harm–benefit |
| [1][2][4][5][8][9][10][11][12] | |
| Morrison EDIE-2; van der Gaag 2013 | CBT / prevention trial evidence |
| Amminger 2010 vs NEURAPRO 2017 | Omega-3 equipoise |
| Davies 2018 network meta | No single clear winner intervention |
| STEP 2023 | Staged adaptive UHR care |
| RANZCP 2016 | Regional early-detection and treatment principles |
Exam pearls
- Three boxes: APS, BLIPS, GRD.
- Most do not convert — say it out loud.
- APS is DSM Section III, not a casual lifelong diagnosis.[18]
- CBT and comorbidity care before routine antipsychotics.[14][17]
- Omega-3: Amminger positive, NEURAPRO negative — equipoise.[15][16]
- When frank psychosis appears, stop debating CHR and run FEP care.[21]
- Cannabis reduction is high-yield and evidence-informed at population level.[23]
- Conversion risk is stratified, not flat.[5]
References
- [1]Yung AR, Yuen HP, McGorry PD, et al. Mapping the onset of psychosis: the Comprehensive Assessment of At-Risk Mental States Aust N Z J Psychiatry, 2005.PMID 16343296
- [2]Miller TJ, McGlashan TH, Rosen JL, et al. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability Schizophr Bull, 2003.PMID 14989408
- [3]Yung AR, Stanford C, Cosgrave E, et al. Testing the Ultra High Risk (prodromal) criteria for the prediction of psychosis in a clinical sample of young people Schizophr Res, 2006.PMID 16630707
- [4]Fusar-Poli P, Bonoldi I, Yung AR, et al. Predicting psychosis: meta-analysis of transition outcomes in individuals at high clinical risk Arch Gen Psychiatry, 2012.PMID 22393215
- [5]Fusar-Poli P, Cappucciati M, Borgwardt S, et al. Heterogeneity of Psychosis Risk Within Individuals at Clinical High Risk: A Meta-analytical Stratification JAMA Psychiatry, 2016.PMID 26719911
- [6]Salazar de Pablo G, Radua J, Pereira J, et al. Probability of Transition to Psychosis in Individuals at Clinical High Risk: An Updated Meta-analysis JAMA Psychiatry, 2021.PMID 34259821
- [7]Fusar-Poli P, Salazar de Pablo G, Correll CU, et al. Prevention of Psychosis: Advances in Detection, Prognosis, and Intervention JAMA Psychiatry, 2020.PMID 32159746
- [8]Cannon TD, Cadenhead K, Cornblatt B, et al. Prediction of psychosis in youth at high clinical risk: a multisite longitudinal study in North America Arch Gen Psychiatry, 2008.PMID 18180426
- [9]Ruhrmann S, Schultze-Lutter F, Salokangas RK, et al. Prediction of psychosis in adolescents and young adults at high risk: results from the prospective European prediction of psychosis study Arch Gen Psychiatry, 2010.PMID 20194824
- [10]Nelson B, Yuen HP, Wood SJ, et al. Long-term follow-up of a group at ultra high risk ("prodromal") for psychosis: the PACE 400 study JAMA Psychiatry, 2013.PMID 23739772
- [11]McGorry PD, Yung AR, Phillips LJ, et al. Randomized controlled trial of interventions designed to reduce the risk of progression to first-episode psychosis in a clinical sample with subthreshold symptoms Arch Gen Psychiatry, 2002.PMID 12365879
- [12]McGlashan TH, Zipursky RB, Perkins D, et al. Randomized, double-blind trial of olanzapine versus placebo in patients prodromally symptomatic for psychosis Am J Psychiatry, 2006.PMID 16648318
- [13]Morrison AP, French P, Stewart SL, et al. Early detection and intervention evaluation for people at risk of psychosis: multisite randomised controlled trial BMJ, 2012.PMID 22491790
- [14]van der Gaag M, Smit F, Bechdolf A, et al. Preventing a first episode of psychosis: meta-analysis of randomized controlled prevention trials of 12 month and longer-term follow-ups Schizophr Res, 2013.PMID 23870806
- [15]Amminger GP, Schäfer MR, Papageorgiou K, et al. Long-chain omega-3 fatty acids for indicated prevention of psychotic disorders: a randomized, placebo-controlled trial Arch Gen Psychiatry, 2010.PMID 20124114
- [16]McGorry PD, Nelson B, Markulev C, et al. Effect of ω-3 Polyunsaturated Fatty Acids in Young People at Ultrahigh Risk for Psychotic Disorders: The NEURAPRO Randomized Clinical Trial JAMA Psychiatry, 2017.PMID 27893018
- [17]Davies C, Cipriani A, Ioannidis JPA, et al. Lack of evidence to favor specific preventive interventions in psychosis: a network meta-analysis World Psychiatry, 2018.PMID 29856551
- [18]Tsuang MT, Van Os J, Tandon R, et al. Attenuated psychosis syndrome in DSM-5 Schizophr Res, 2013.PMID 23773295
- [19]Fusar-Poli P, Nelson B, Valmaggia L, et al. Comorbid depressive and anxiety disorders in 509 individuals with an at-risk mental state: impact on psychopathology and transition to psychosis Schizophr Bull, 2014.PMID 23180756
- [20]Schultze-Lutter F, Ruhrmann S, Fusar-Poli P, et al. Basic symptoms and the prediction of first-episode psychosis Curr Pharm Des, 2012.PMID 22239566
- [21]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [22]McGorry PD, Mei C, Amminger GP, et al. A Sequential Adaptive Intervention Strategy Targeting Remission and Functional Recovery in Young People at Ultrahigh Risk of Psychosis: The Staged Treatment in Early Psychosis (STEP) Sequential Multiple Assignment Randomized Trial JAMA Psychiatry, 2023.PMID 37378974
- [23]Di Forti M, Quattrone D, Freeman TP, et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study Lancet Psychiatry, 2019.PMID 30902669