Psych · General adult psychiatry — personality disorders
Cluster A and Cluster C personality disorders
Also known as Paranoid personality disorder · Schizoid personality disorder · Schizotypal personality disorder · Avoidant personality disorder · Dependent personality disorder · Obsessive-compulsive personality disorder · OCPD · Anankastic personality disorder · Cluster A · Cluster C
Exam-exhaustive fellowship reference on Cluster A (paranoid, schizoid, schizotypal) and Cluster C (avoidant, dependent, OCPD) personality disorders — DSM-5-TR criteria, ICD-11 severity and trait domains, epidemiology, mechanisms, differentials (ASD, social anxiety, OCD, schizophrenia spectrum), assessment, psychotherapy and limited pharmacotherapy, prognosis. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Cluster A and Cluster C personality disorders are high-yield general adult topics because examiners test criteria accuracy, high-stakes differentials, and whether you can build an alliance with distrustful, detached or rigid patients without therapeutic nihilism. A candidate who only knows borderline or antisocial content will fail these stems.[4][8][12]
Overview and definition
Personality disorder describes an enduring, inflexible pattern of inner experience and behaviour that deviates markedly from cultural expectations, is pervasive across contexts, begins by adolescence or early adulthood, is stable over time, and leads to distress or impairment — not better explained solely by another mental disorder, substance, or medical condition. Cluster labels are a DSM teaching scaffold, not a biological taxonomy: Cluster A is odd/eccentric; Cluster C is anxious/fearful. ICD-11 shifts emphasis to severity of personality dysfunction plus trait domain qualifiers rather than named categorical clusters.[2][20]
General rule for fellowship answers. Diagnose only with a longitudinal history and collateral. A single hostile interview is not paranoid PD; shyness is not avoidant PD; perfectionism at work is not OCPD. Late-onset “personality change” is an organic and affective red flag until proven otherwise.[4][8]
Classification and nosology
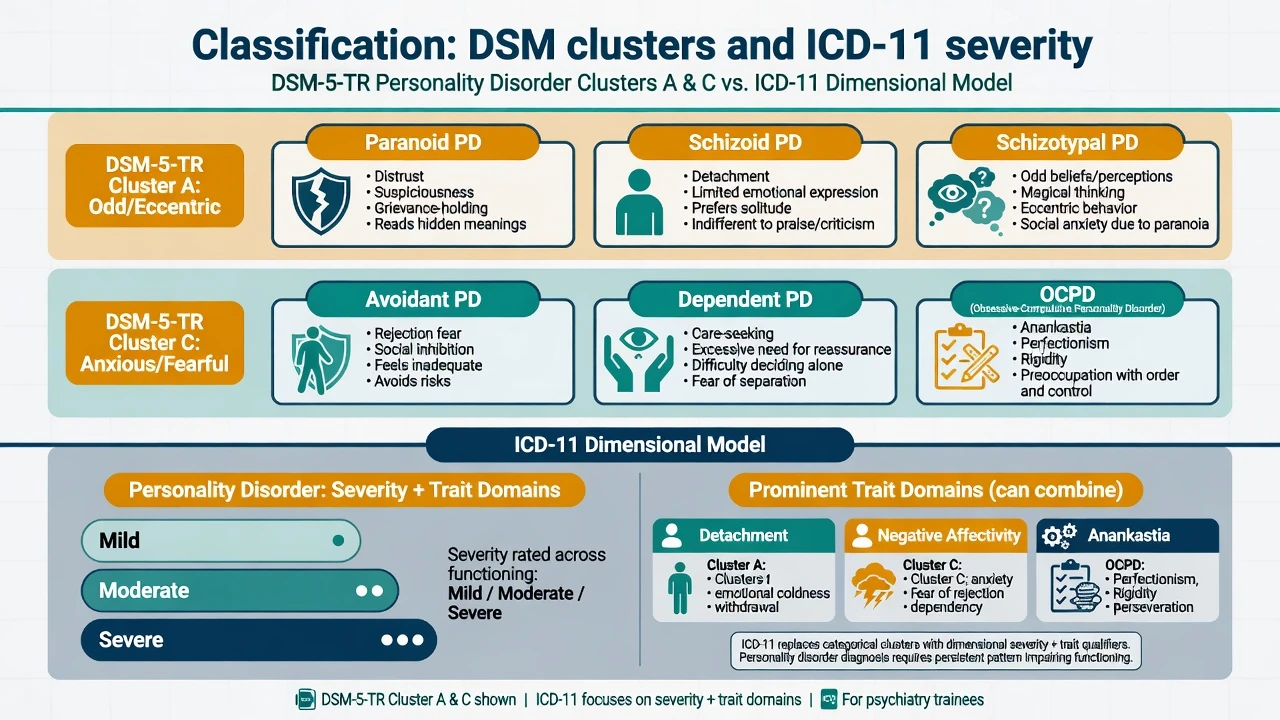
Cluster A (odd/eccentric)
- Paranoid: pervasive distrust and suspiciousness
- Schizoid: detachment and restricted affectivity
- Schizotypal: cognitive-perceptual oddness and interpersonal deficits
- Exam trap: spectrum adjacency of schizotypal with schizophrenia
Cluster C (anxious/fearful)
- Avoidant: social inhibition and rejection sensitivity
- Dependent: excessive need to be cared for
- OCPD (anankastic): order, perfectionism, control
- High comorbidity with anxiety and depression
ICD-11 framing
- Severity: mild / moderate / severe
- Trait domains include detachment, negative affectivity, anankastia
- Better for dimensional case discussion and stepped care
- Named patterns optional depending on local teaching
AMPD / formulation language
- Criterion A: self and interpersonal functioning impairment
- Criterion B: pathological traits (e.g. detachment, anankastia)
- Use in viva even if diagnosis is categorical
- Avoid pejorative shorthand
DSM-5-TR operational thresholds (exam checklist). After general PD criteria are met, each disorder has a criterion count that must be reproduced accurately in closed-book conditions. Paranoid PD: pervasive distrust with four or more of seven features (suspects exploitation, doubts loyalty, reluctant to confide, reads hidden demeaning meanings, bears grudges, perceives attacks on character not apparent to others and reacts angrily, recurrent unjustified suspicions of partner fidelity). Schizoid PD: detachment/restricted affect with four or more of seven (neither desires nor enjoys close relationships including family, almost always chooses solitary activities, little interest in sexual experiences with another person, takes pleasure in few activities, lacks close friends other than first-degree relatives, appears indifferent to praise or criticism, emotional coldness/detachment/flattened affectivity). Schizotypal PD: social and interpersonal deficits with cognitive-perceptual distortions and eccentricity, five or more of nine (ideas of reference, odd beliefs/magical thinking, unusual perceptual experiences, odd thinking and speech, suspiciousness/paranoid ideation, inappropriate or constricted affect, odd/eccentric/peculiar behaviour or appearance, lack of close friends other than first-degree relatives, excessive social anxiety that does not diminish with familiarity and tends to be associated with paranoid fears). Avoidant PD: social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation, four or more of seven. Dependent PD: excessive need to be taken care of leading to submissive and clinging behaviour and fears of separation, five or more of eight. OCPD: preoccupation with orderliness, perfectionism and mental/interpersonal control at the expense of flexibility, openness and efficiency, four or more of eight (details/rules/lists/order/organisation/schedules to the point that major point of activity is lost; perfectionism that interferes with task completion; excessive devotion to work and productivity; overconscientious/inflexible about morality/ethics/values; unable to discard worn-out or worthless objects; reluctant to delegate; adopts a miserly spending style toward self and others; rigidity and stubbornness).[8][12][16][17]
Epidemiology and risk factors
Headline epidemiology candidates must own
Community prevalence estimates differ by instrument, threshold and culture, but the fellowship takeaway is consistent: personality disorders are common enough to matter in every general adult clinic, disable function, and co-travel with mood, anxiety, substance and neurodevelopmental conditions. Torgersen’s Norwegian community sample, the NCS-R interview study, NESARC US data, and the 2025 global systematic review/meta-regression jointly destroy the myth that PD is a rare boutique diagnosis.[1][2][3][4]
Risk and aetiology. Childhood adversity and trauma associate with schizotypal severity and cognitive-perceptual load; temperamental behavioural inhibition and rejection sensitivity feed avoidant patterns; overprotective or authoritarian parenting narratives appear in dependent formulations; anankastic temperament and modelling of rigid standards feed OCPD. Twin data support moderate heritability for avoidant and dependent PD when carefully measured. None of these factors alone makes the diagnosis.[8][12][19]
Pathophysiology and mechanisms
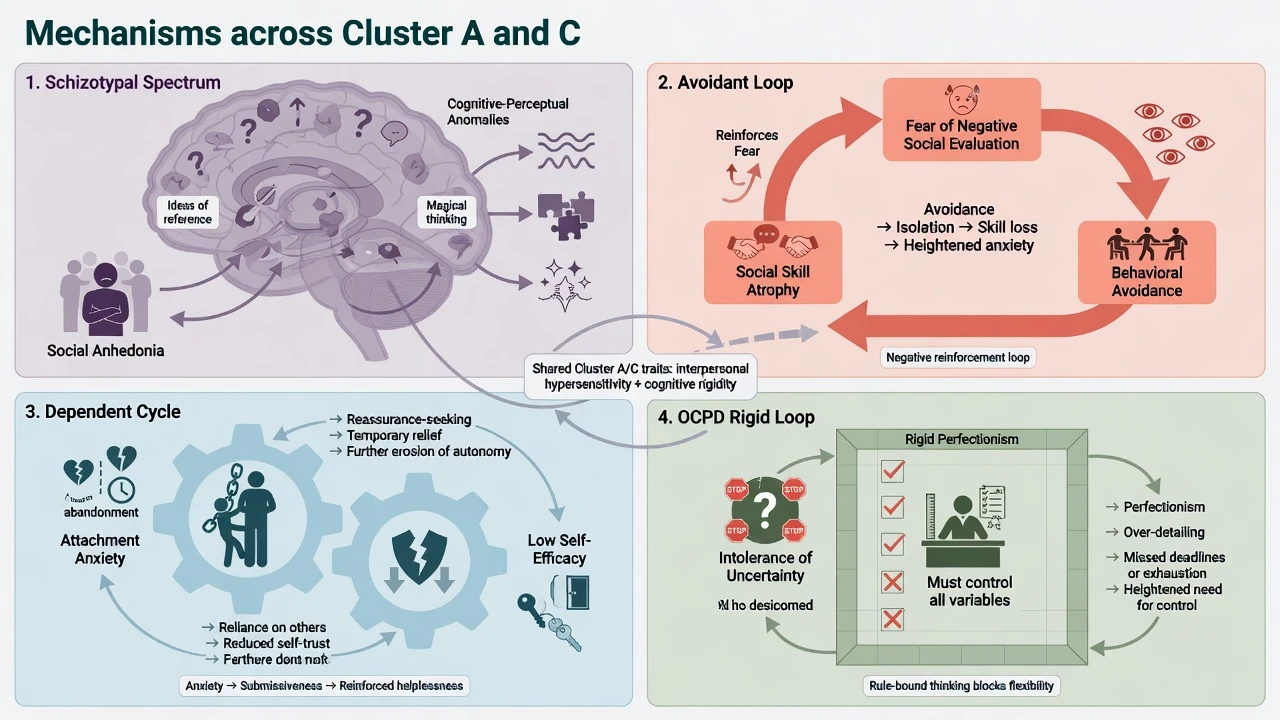
Schizotypal / spectrum mechanisms. Schizotypal PD sits on a clinical continuum with schizophrenia-spectrum vulnerability: cognitive-perceptual anomalies, social anhedonia, odd speech and interpersonal wariness without meeting full psychosis thresholds. Group-level research (sensory gating, cognitive control, trauma-amplified severity) informs formulation but does not diagnose individuals. A subset of people with schizotypal disorder transition toward schizophrenia — longitudinal monitoring matters.[7][8]
Paranoid mechanisms. Threat-biased appraisal, externalising blame, and attachment insecurity produce a self-reinforcing distrust loop. This is not the same as a fixed false belief held with delusional intensity; the distinction is examinable and clinically decisive.[9]
Schizoid mechanisms. Detachment, restricted affective range and preference for solitude can reflect negative schizotypy, autistic social-communication differences, or a true anhedonic detached style. Differential work with developmental history is mandatory.[18]
Avoidant mechanisms. Social-evaluative fear, core beliefs of inadequacy, and behavioural avoidance maintain skill atrophy and confirm fears — a loop continuous with social anxiety disorder but often more pervasive in self-concept and occupational constriction.[12][13]
Dependent mechanisms. Attachment anxiety, low self-efficacy and submissive care-seeking under stress maintain reliance on others and collapse after losses or relationship rupture.[19]
OCPD mechanisms. Anankastia — rigid standards, intolerance of uncertainty, perfectionism and control — is often ego-syntonic. That is the key mechanism contrast with OCD’s ego-dystonic obsessions and compulsions.[15][16][17]
Clinical presentation
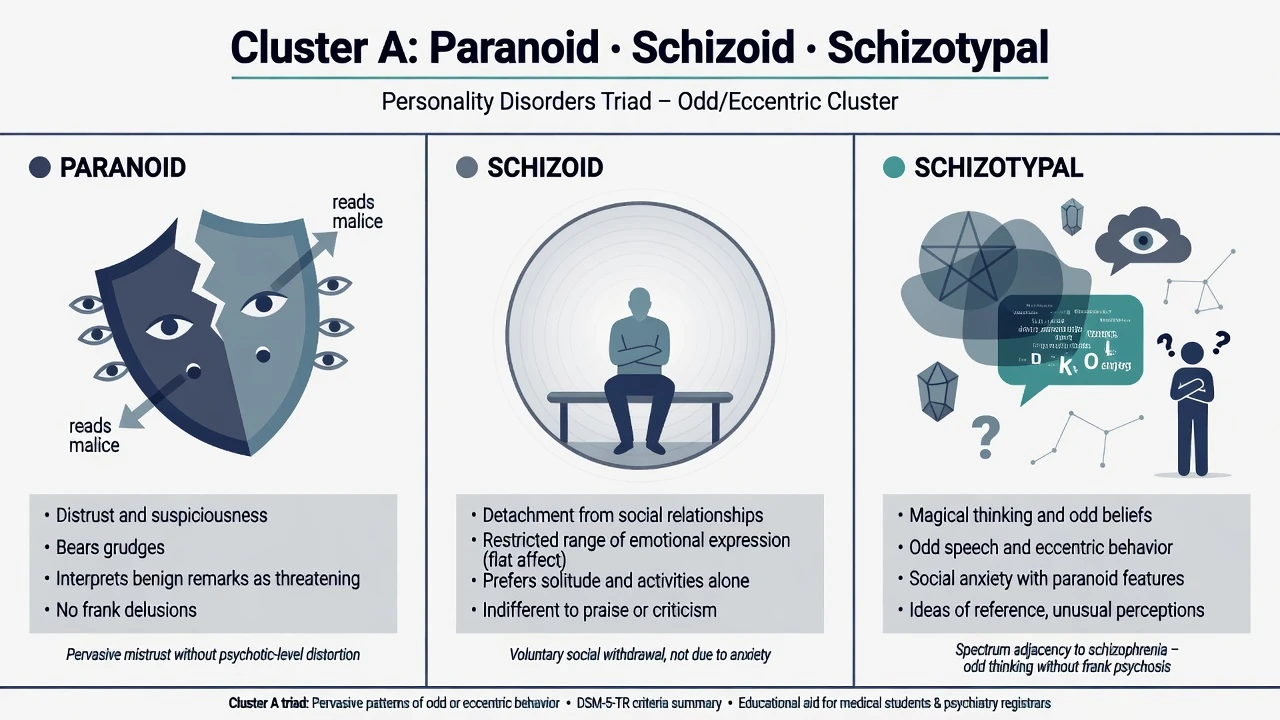
Paranoid PD. Patients expect exploitation, misread neutral remarks, keep grudges, and may appear cold, argumentative or litigious. MSE: guarded rapport, suspicious thought content without clear delusional conviction or first-rank phenomena, limited trust in the interviewer. They present via workplace conflict, marital jealousy, or refusal of investigations rather than asking for “help with paranoia.”[9]
Schizoid PD. Solitary lifestyle, emotional coldness, indifference to praise or criticism, few close relationships, and little desire for sexual or intimate closeness. They may be brought by relatives for “asociality” or depression, not self-referred for loneliness. Discriminate carefully from autism and negative-symptom schizophrenia.[18]
Schizotypal PD. Odd beliefs or magical thinking, unusual perceptions, ideas of reference, eccentric appearance or speech, constricted or inappropriate affect, and social anxiety that is often paranoid rather than purely self-conscious. Function may be preserved enough to avoid psychosis services until crisis, substance use or depression forces contact.[7][8]
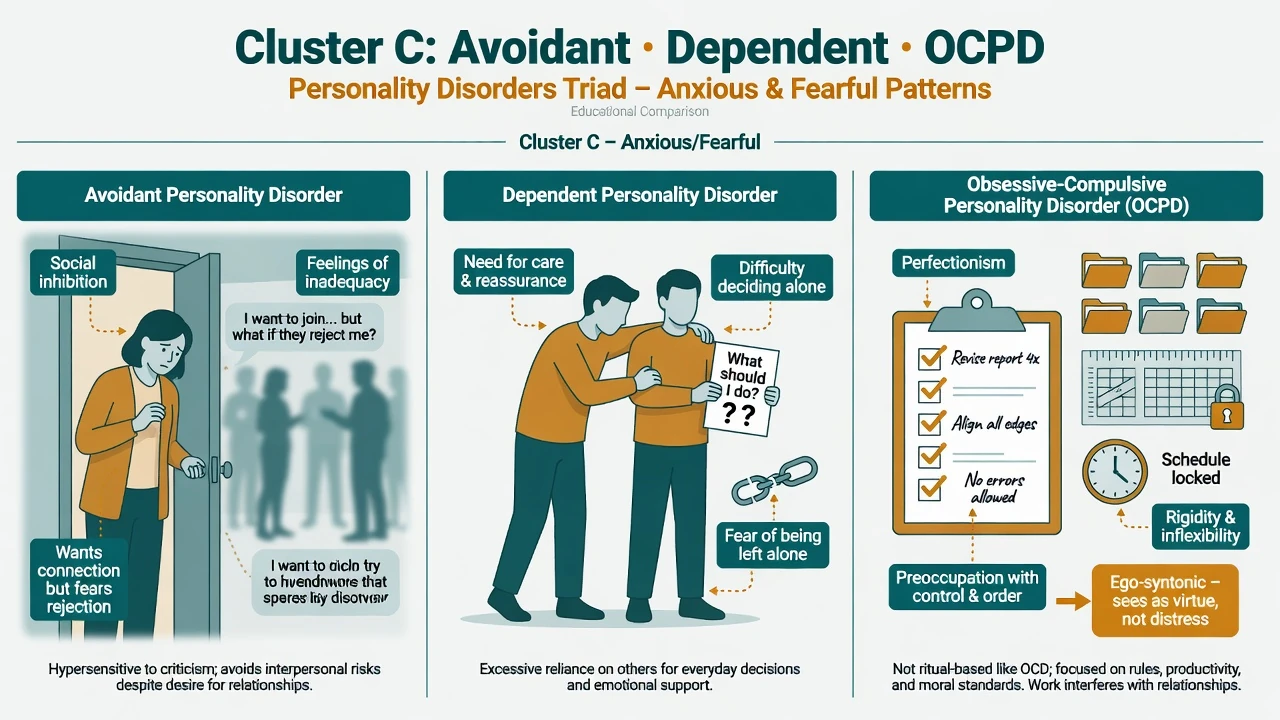
Avoidant PD. Desires relationships but avoids occupational, social and intimate risks for fear of criticism, rejection or embarrassment; views self as socially inept or inferior; is unusually reluctant to take personal risks. MSE often shows anxious affect, self-deprecating content and marked anticipatory anxiety — not the flat detachment of schizoid PD.[12][13]
Dependent PD. Difficulty making everyday decisions without excessive advice, needs others to assume responsibility for major life areas, difficulty expressing disagreement for fear of loss of support, urgently seeks another relationship when a close one ends, and is unrealistically preoccupied with fears of being left to care for self. Crises often follow separation, illness of a carer, or discharge from hospital without a support plan.[19]
OCPD. Rigid perfectionism that delays completion, excessive devotion to work, overconscientious morality, reluctance to delegate, miserly spending style in some, and stubbornness. Patients often experience traits as correct standards rather than symptoms; partners and colleagues experience obstruction and conflict. Do not confuse with OCD rituals unless true obsessions and compulsions are present — co-occurrence is common and both can be diagnosed.[14][15][16][17]
Differential diagnosis
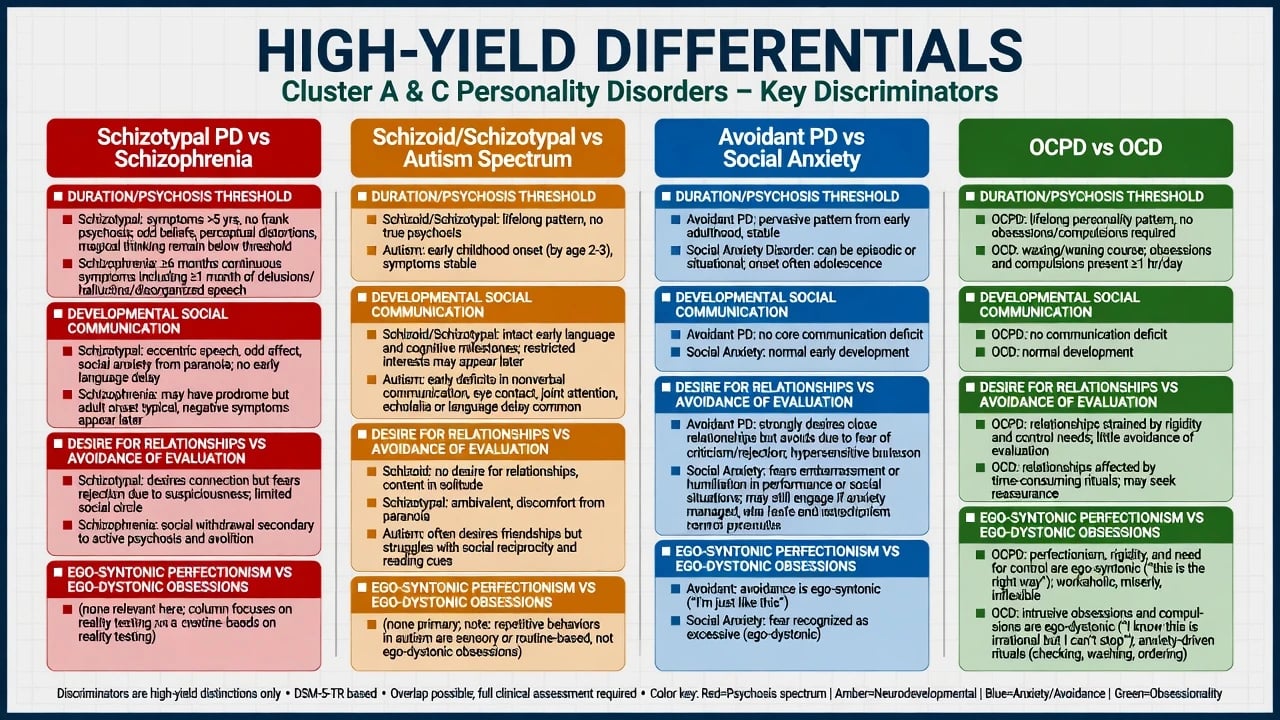
Schizotypal vs schizophrenia
- Schizotypal: oddness without sustained frank psychosis or marked deterioration required for schizophrenia
- Schizophrenia: delusions/hallucinations, disorganisation, negative symptoms, functional collapse thresholds
- Duration and illness course decide; monitor conversion risk
- Treat emerging psychosis on a psychosis pathway
Schizoid/schizotypal vs ASD
- ASD: early developmental social communication differences, restricted/repetitive patterns, sensory profile
- Schizoid: detachment often without early language delay pattern of ASD
- Schizotypal: magical thinking and ideas of reference less typical of classic ASD framing
- Dual formulation possible — do not force either/or
Avoidant PD vs social anxiety
- Continuum is real; many with AVPD meet SAD criteria
- AVPD: more pervasive inadequacy schema and life constriction
- SAD: can be more performance- or situation-bound
- Treat exposure and CBT principles for both; add broader PD work when global
OCPD vs OCD
- OCPD: ego-syntonic perfectionism and control
- OCD: ego-dystonic obsessions and compulsions, often time-consuming
- Co-occurrence common (meta-analytic signal) — diagnose both when present
- ERP + SSRI algorithms target OCD, not OCPD alone
Other essential discriminators. Paranoid PD versus delusional disorder (fixed false belief of delusional intensity, often narrower theme, later onset possible). Avoidant versus schizoid (desire for connection present vs low desire). Dependent versus BPD (submissive clinging without the full BPD affective instability, identity disturbance and self-harm pattern — though traits can co-occur). OCPD versus autism-related rigidity and versus anorexia-related perfectionism. Always include substances, mood disorders, PTSD and medical personality change on the board.[12][14][15][18]
Clinical and bedside assessment
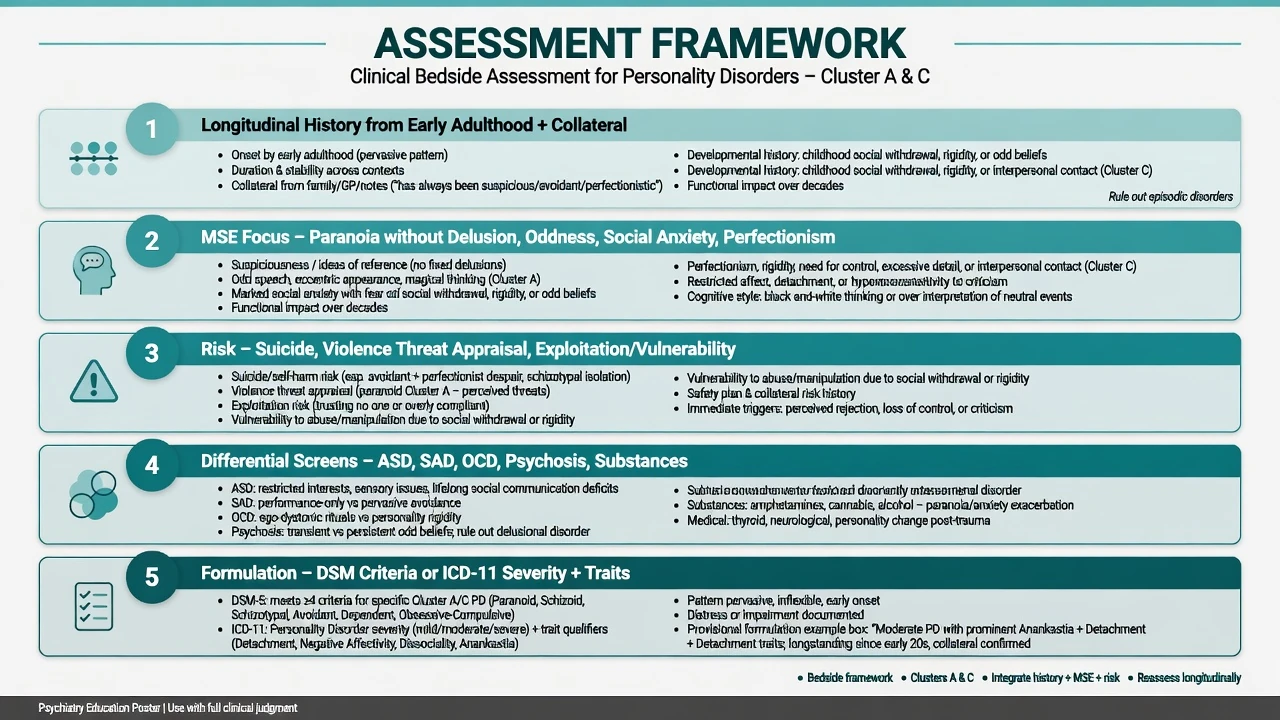
History structure. Developmental trajectory from school age; friendships and romantic patterns; occupational performance under evaluation; trauma and attachment; substance use; prior diagnoses (especially ASD, OCD, SAD, psychosis); what the patient wants help with today. Obtain collateral early for schizoid minimisation and paranoid distortion.[8][12]
MSE focus. Rapport (guarded, aloof, anxious, perfectionistic control of the interview), thought content (suspiciousness vs delusion), perceptual phenomena, odd speech, affect range, insight (often limited in OCPD and paranoid PD), and capacity for collaborative work. Document how the interpersonal style appears in the room.[8]
Risk domains examiners expect. Suicide and self-harm risk rises with comorbid depression and crises (especially dependent and avoidant patients after losses). Violence risk in paranoid presentations is about threat appraisal, grievance, and access to means — not a stereotype. Vulnerability and exploitation risk are central in dependent PD. Self-neglect and isolation matter in severe schizoid/schizotypal presentations. Capacity is decision-specific; safeguarding duties are local and statutory.[4][9]
Tools (conceptual). SCID-5-PD / IPDE for structured categorical diagnosis; ICD-11 severity instruments in services adopting dimensional practice; SAD, OCD, ASD and psychosis-risk screens when indicated. Tools support — they do not replace — clinical diagnosis.[20]
Investigations
There is no laboratory gold standard for personality disorder. Investigate to exclude mimics and prepare for medication when used: TSH, FBC, U&E, LFT, glucose/lipids and BMI if antipsychotics considered, pregnancy test when relevant, urine drug screen when substances may explain behaviour, ECG when cardiac risk or QTc-risk drugs are planned. Neuroimaging or EEG when late-onset change, focal neurology, seizures or cognitive decline fire. Screen systematically for depression, SAD, OCD, ASD and emerging psychosis because they change the treatment map.[7][11][18]
Management — acute / emergency
Acute paranoid agitation. Prioritise safety of patient and staff, de-escalation, low-stimulus environment, and medical exclusion of substances/delirium. Short-term pharmacological sedation follows local emergency rapid-tranquillisation protocols with monitoring when required for imminent risk — not a new long-term “paranoid sedative regimen.” Legal status uses jurisdiction-specific Mental Health Act principles when statutory criteria are met; do not invent section numbers.[9]
Dependent/avoidant crisis after loss. Full suicide risk assessment, means restriction, practical support, and a time-limited plan that neither abandons nor collusively over-rescues. Link to named follow-up rapidly.[12]
Management — definitive and stepwise
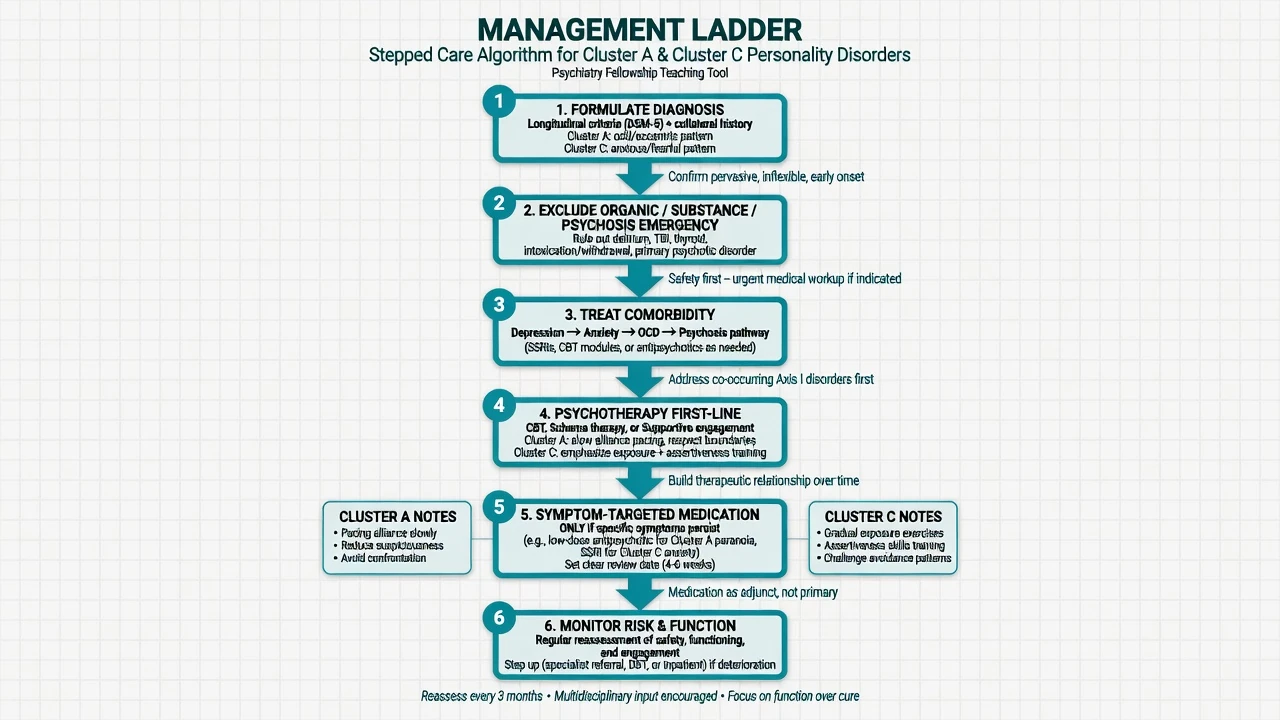
Psychotherapy first-line
Specialised and structured psychological treatments are the core of definitive care. A multicentre RCT of schema therapy for personality disorders (Bamelis and colleagues) demonstrated clinical effectiveness versus clarification-oriented psychotherapy and treatment as usual in a mixed PD sample that included substantial Cluster C pathology — a high-yield named trial for fellowship answers beyond BPD-only evidence.[5][6]
Cluster A engagement principles. Go slowly. Predictable structure beats early deep interpretation. Collaborative empiricism is cautious: challenge threats with data only after some alliance exists. Supportive therapy, social skills work, and CBT adaptations for suspicious or odd thinking have a role; evidence density is thinner than for BPD but recent Cluster A intervention reviews support psychosocial approaches as the primary frame, with pharmacotherapy adjunctive and uncertain for core traits.[9][11]
Schizotypal-specific. Systematic reviews describe limited, low-certainty evidence for low-dose antipsychotics for cognitive-perceptual symptoms and mixed psychosocial data; GRADE-style updates continue to emphasise cautious, individualised use and the need for better trials. Social skills training, CBT for ideas of reference/magical thinking (carefully), and monitoring for transition to schizophrenia are clinical pillars. If frank psychosis emerges, treat as psychosis, not as personality failure.[7][10][11]
Avoidant PD. CBT with graded exposure, cognitive restructuring of inadequacy beliefs, and social skills practice is first-line psychologically. Because of continuum with SAD, evidence-based SAD pathways apply: structured CBT; when medication is indicated for comorbid SAD/depression, use a standard SSRI approach with monitoring. Example adult starting language when an examiner forces a named plan (individualise; check local product information): sertraline 50 mg orally once daily, review in 1–2 weeks for activation, anxiety increase and suicidality (especially under age 25), titrate toward a therapeutic SAD/depression range (commonly 50–150 mg daily as tolerated) with a measurement plan and a review date — this treats anxiety/depression comorbidity, not “the personality” as a drug target. Schema therapy and interpersonal strategies address broader self-concept and avoidance of intimacy.[5][12][13]
Dependent PD. Therapy targets assertiveness, problem-solving, graded independence tasks, and the dependency dynamic in the therapeutic relationship (avoid recreating a permanent rescuer). Crisis planning for anticipated losses. Treat comorbid depression/anxiety with the same agent-level standards as elsewhere.[5][19]
OCPD. CBT targeting perfectionism, rigidity, procrastination driven by impossible standards, and overcontrol; behavioural experiments that tolerate “good enough.” If true OCD is present, prioritise exposure and response prevention plus SSRI algorithms for OCD rather than only personality-focused work. Example when comorbid OCD requires pharmacotherapy (individualise): fluoxetine often started around 20 mg orally daily, titrated toward higher OCD ranges under specialist review (commonly toward 40–60 mg as tolerated, sometimes higher under specialist care) with sexual side-effect, activation and suicidality counselling and a clear response review at 8–12 weeks at an adequate dose — again treating OCD, not “curing OCPD.” Schema therapy can help when rigid modes dominate identity and relationships.[5][14][15][16][17]
Pharmacotherapy principles (all six disorders)
Avoid chronic benzodiazepines for long-term personality-related anxiety. Avoid stacking antipsychotics for chronic oddness without reassessing diagnosis. Always reassess whether the true target is OCD, SAD, depression or emerging psychosis.[11][16]
Care system and disposition
Most patients are managed in outpatient psychotherapy and general adult community pathways. Step up for acute risk, frank psychosis, severe self-neglect, or failed community containment. Step down when skills generalise and risk stabilises. Consistency of one agreed formulation reduces iatrogenic rupture with paranoid and OCPD patients who already expect criticism or betrayal.[5][9]
Australian and New Zealand practice emphasises stepped mental health care, trauma-informed and culturally safe engagement, and access to psychological therapies where available. Local Mental Health Act provisions govern involuntary care — name principles and least-restrictive practice, not invented foreign section numbers. Coordinate with early psychosis services when schizotypal features sit near the UHR/psychosis threshold.[7][20]
Specific subtypes and scenarios
Schizotypal at the early psychosis interface. Document attenuated psychotic symptoms, decline, family history, substance use, and duration. Refer or co-manage with early intervention services when thresholds approach psychosis criteria. Do not withhold antipsychotic consideration solely because a PD label exists if frank psychosis is present.[7][11]
Avoidant PD with workplace failure. Performance anxiety plus global avoidance of promotion, meetings and relationships. Combine exposure hierarchy with occupational liaison and depression screening.[12]
OCPD professional with burnout. High-functioning perfectionism masking marital conflict and delayed tasks. Therapy targets values-based flexibility; rule out OCD and depression.[16][17]
Dependent PD in coercive relationships. Safeguarding assessment, safety planning, and careful therapy that builds agency without cutting support abruptly.[19]
Paranoid PD refusing investigations. Collaborative risk–benefit discussion, second opinions, involving a trusted third party if the patient permits, and capacity assessment for specific decisions.[9]
Neurodiversity dual formulation. ASD and PD traits can co-occur; developmental history, sensory profile and social motivation quality prevent false dichotomies.[18]
Complications and pitfalls
Classic pitfalls: calling autism “schizoid”; missing OCD under an OCPD label; collapsing avoidant PD into “just shy”; confronting paranoid beliefs too early and destroying alliance; therapeutic nihilism (“Cluster A never engages”); polypharmacy for chronic anxiety or oddness; overlooking exploitation of dependent patients; missing depression that drives suicide risk; assuming all social withdrawal is negative-symptom schizophrenia without developmental context.[12][15][18]
Prognosis and disposition
Personality psychopathology is more plastic than older textbooks claimed. Longitudinal alternative-model and categorical follow-up work shows that many trait and disorder patterns improve over years, though functional recovery (work, intimacy) can lag and depends on comorbidity, substance use and engagement. Schizotypal presentations require ongoing vigilance for psychotic transition. Avoidant and OCPD patterns often improve when patients stay in structured therapy that targets the maintaining loops. Disposition is usually outpatient; hospitalisation is for acute risk or severe comorbidity, not for “having a PD.”[4][5][7]
Special populations
Youth. Distinguish emerging PD patterns from normal developmental shyness, identity formation and adolescent odd interests. ASD assessment is essential before permanent Cluster A labels. Early intervention for social anxiety and perfectionism can prevent entrenchment.[12][18]
Older adults. New late-life “paranoid personality” or sudden rigidity is organic/mood/substance until proven otherwise. Lifelong OCPD may decompensate after retirement when structure collapses; dependent PD may present after carer death.[4]
Pregnancy and parenting. Treat anxiety and depression carefully; assess dependent dynamics and safeguarding; minimise unnecessary polypharmacy.[12]
Cultural formulation. Interdependence in collectivist cultures is not dependent PD. Distrust of systems after discrimination is not automatically paranoid PD. In ANZ practice, Indigenous cultural safety and family-inclusive care are competencies, not optional extras.[4][20]
Evidence, guidelines and controversies
Epidemiology anchors: Torgersen 2001 community sample; Lenzenweger NCS-R 2007; Grant NESARC 2004; Shadid 2025 global meta-regression.[1][2][3][4]
Treatment anchors: Bamelis 2014 schema therapy RCT and 2015 economic evaluation; Kirchner 2018 and Gundersen 2026 schizotypal treatment reviews; Jakobsen 2017 antipsychotic systematic review; Cheli 2025 Cluster A psychosocial/pharmacological meta-analyses; Lampe and Malhi 2018 avoidant insights; Frandsen interpersonal SAD/AVPD work; Diedrich 2015, Pinto 2022 and Pozza 2021 for OCPD/OCD interface; Lugnegård 2012 for PD–ASD links; Gjerde 2012 heritability; Kim/Tyrer line on ICD-11 dimensional progress.[5][6][7][9][10][11][12][14][16][18][19][20]
Controversies worth a mature viva sentence. Whether categorical clusters should be abandoned entirely for ICD-11 severity; how aggressively to medicate schizotypal cognitive-perceptual symptoms given low-certainty evidence; whether AVPD is simply severe SAD; whether OCPD is better framed as anankastia trait than a discrete disorder.[12][16][20]
Exam pearls
A and C viva checklist
SPECTRUM
Schizotypal sits near schizophrenia spectrum — monitor conversion
Paranoid PD is distrust without frank delusion
Ego-syntonic OCPD vs ego-dystonic OCD
Collateral and longitudinal history mandatory
Therapy first (CBT/schema/supportive engagement)
Reject nihilism; treat comorbidity with named plans
Unmask ASD, SAD, OCD, organic mimics
Medication only for targets with review dates
60-second oral summary
Cluster A is odd/eccentric (paranoid distrust, schizoid detachment, schizotypal cognitive-perceptual oddness); Cluster C is anxious/fearful (avoidant rejection sensitivity, dependent care needs, OCPD anankastia). Diagnose longitudinally with DSM counts or ICD-11 severity plus traits. Discriminate ASD, SAD, OCD and schizophrenia-spectrum illness with developmental history, desire for relationships, ego-syntonicity and psychosis thresholds. Treat with alliance-first psychotherapy (CBT, schema therapy with Bamelis-level evidence, supportive adaptations for Cluster A); medicate comorbidity or short-term schizotypal targets only with review dates. Monitor schizotypal conversion risk and dependent/avoidant suicide risk after losses. Hope and structure beat stigma.[5][7][12][16][20]
References
- [1]Torgersen S, Kringlen E, Cramer V The prevalence of personality disorders in a community sample Arch Gen Psychiatry, 2001.PMID 11386989
- [2]Lenzenweger MF, Lane MC, Loranger AW, Kessler RC DSM-IV personality disorders in the National Comorbidity Survey Replication Biol Psychiatry, 2007.PMID 17217923
- [3]Grant BF, Hasin DS, Stinson FS, Dawson DA, et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions J Clin Psychiatry, 2004.PMID 15291684
- [4]Shadid J, Ferrari AJ, Bach B, Sellbom M, et al. The global epidemiology of personality disorder: a systematic review and meta-regression Lancet Psychiatry, 2025.PMID 41197646
- [5]Bamelis LL, Evers SM, Spinhoven P, Arntz A Results of a multicenter randomized controlled trial of the clinical effectiveness of schema therapy for personality disorders Am J Psychiatry, 2014.PMID 24322378
- [6]Bamelis LL, Arntz A, Wetzelaer P, Verdoorn R, et al. Economic evaluation of schema therapy and clarification-oriented psychotherapy for personality disorders: a multicenter, randomized controlled trial J Clin Psychiatry, 2015.PMID 26579561
- [7]Kirchner SK, Roeh A, Nolden J, Hasan A Diagnosis and treatment of schizotypal personality disorder: evidence from a systematic review NPJ Schizophr, 2018.PMID 30282970
- [8]Rosell DR, Futterman SE, McMaster A, Siever LJ Schizotypal personality disorder: a current review Curr Psychiatry Rep, 2014.PMID 24828284
- [9]Cheli S, Wisepape CN, Witten CDY, Floridi M, et al. Psychosocial and pharmacological interventions for cluster a personality disorders: A systematic review and two exploratory meta-analyses Personal Disord, 2025.PMID 40111791
- [10]Jakobsen KD, Skyum E, Hashemi N, Schjerning O, et al. Antipsychotic treatment of schizotypy and schizotypal personality disorder: a systematic review J Psychopharmacol, 2017.PMID 28347257
- [11]Gundersen KB, Arnfred B, Albert N, Rasmussen AR, et al. Treatment of schizotypal disorder: A systematic review and GRADE evaluation of the certainty of evidence Schizophr Res, 2026.PMID 41421074
- [12]Lampe L, Malhi GS Avoidant personality disorder: current insights Psychol Res Behav Manag, 2018.PMID 29563846
- [13]Frandsen FW, Simonsen S, Poulsen S, Sørensen P, et al. Social anxiety disorder and avoidant personality disorder from an interpersonal perspective Psychol Psychother, 2020.PMID 30656823
- [14]Pozza A, Starcevic V, Ferretti F, Pedani C, et al. Obsessive-Compulsive Personality Disorder Co-occurring in Individuals with Obsessive-Compulsive Disorder: A Systematic Review and Meta-analysis Harv Rev Psychiatry, 2021.PMID 33666394
- [15]Mancebo MC, Eisen JL, Grant JE, Rasmussen SA Obsessive compulsive personality disorder and obsessive compulsive disorder: clinical characteristics, diagnostic difficulties, and treatment Ann Clin Psychiatry, 2005.PMID 16402751
- [16]Pinto A, Teller J, Wheaton MG Obsessive-Compulsive Personality Disorder: A Review of Symptomatology, Impact on Functioning, and Treatment Focus (Am Psychiatr Publ), 2022.PMID 37200888
- [17]Diedrich A, Voderholzer U Obsessive-compulsive personality disorder: a current review Curr Psychiatry Rep, 2015.PMID 25617042
- [18]Lugnegård T, Hallerbäck MU, Gillberg C Personality disorders and autism spectrum disorders: what are the connections? Compr Psychiatry, 2012.PMID 21821235
- [19]Gjerde LC, Czajkowski N, Røysamb E, Orstavik RE, et al. The heritability of avoidant and dependent personality disorder assessed by personal interview and questionnaire Acta Psychiatr Scand, 2012.PMID 22486635
- [20]Kim YR, Tyrer P, Mulder R, King JD, et al. ICD-11 classification of personality disorder: there is no other way forward Br J Psychiatry, 2026.PMID 41906979