Psych · General adult psychiatry — trauma and stressor-related disorders
Complex PTSD and trauma-informed care
Also known as Complex PTSD · cPTSD · CPTSD · Disorders of extreme stress not otherwise specified · DESNOS · Disturbances of self-organisation · DSO · Trauma-informed care · STAIR Narrative Therapy · DBT-PTSD · Phase-based trauma treatment
Exam-exhaustive fellowship reference on ICD-11 complex PTSD — PTSD core plus DSO triad, differential from PTSD and BPD, ITQ assessment, phase-based STAIR evidence and de Jongh critique, DBT-PTSD, trauma-focused therapies, adjunct pharmacotherapy doses, and trauma-informed care principles. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Complex PTSD is high-yield across FRANZCP MEQs, MRCPsych CASC communication stations, and ABPN trauma blueprints. Examiners test the ICD-11 architecture, the CPTSD–BPD differential, phase-based versus flexible trauma-focused sequencing, named protocols with evidence, drug doses, and whether "trauma-informed" is genuine service design or empty language.[2][6][10]
Overview and definition
ICD-11 complex PTSD (CPTSD) requires the three PTSD elements — re-experiencing the traumatic event(s) in the present, deliberate avoidance of trauma reminders, and a persistent sense of current threat (hypervigilance/exaggerated startle) — plus disturbances of self-organisation (DSO): affect dysregulation, a persistent negative self-concept (worthlessness, shame, guilt), and disturbances in relationships (difficulty sustaining closeness or feeling close to others). Symptoms cause significant impairment and are not better explained by another condition alone.[1][2]
Prolonged or repeated trauma from which escape is difficult (childhood abuse, captivity, organised violence, coercive control, institutional abuse) is the typical context, but diagnosis is driven by the symptom structure, not trauma type alone. Single-incident trauma can still produce complex presentations in vulnerable people; prolonged trauma does not automatically produce CPTSD.[1][2][3]
DSM-5-TR retains a four-cluster PTSD architecture and does not include a formal CPTSD category. Similar clinical pictures may be coded as PTSD (with or without dissociative symptoms) plus comorbid personality, depressive, or other stressor-related diagnoses. Always name which manual you are using in the exam answer.[2][17]
Classification
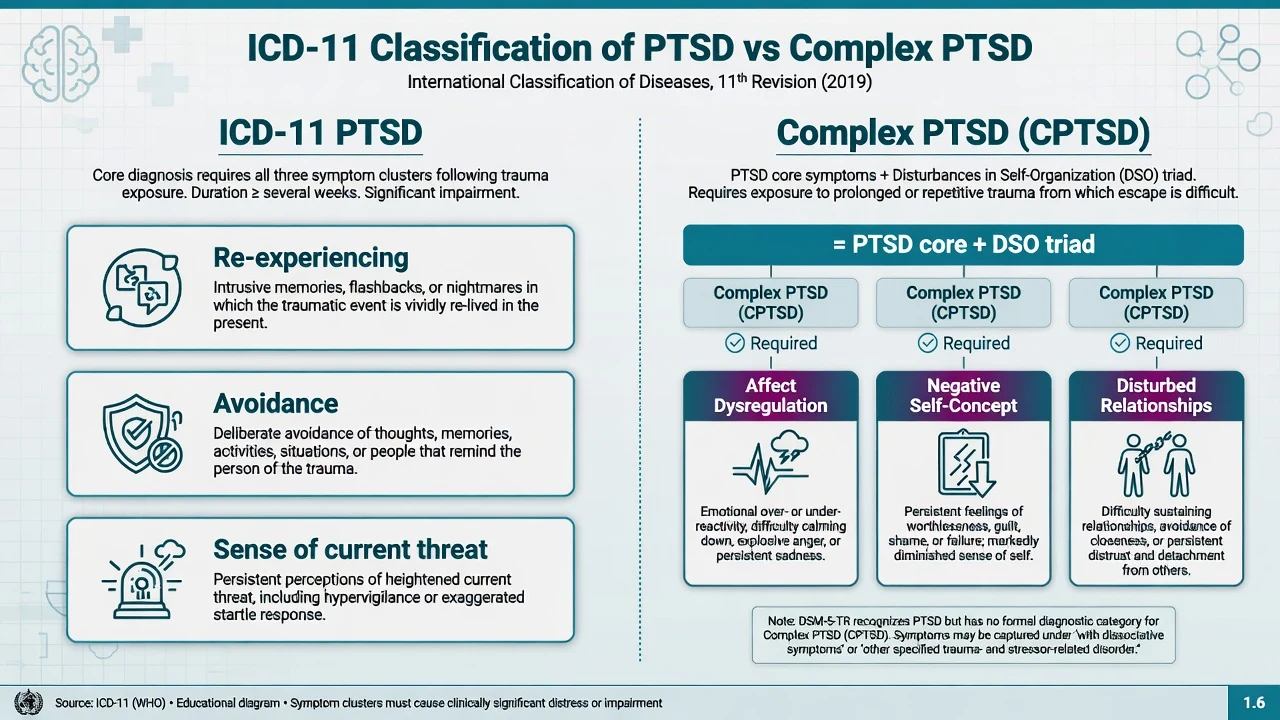
ICD-11 PTSD
- Re-experiencing in the present
- Avoidance of reminders
- Sense of current threat
- No requirement for full DSO triad
ICD-11 CPTSD
- All PTSD core elements
- Affect dysregulation
- Negative self-concept
- Relational disturbance
DSM-5-TR PTSD
- Four clusters >1 month
- Specifiers incl. dissociative
- No formal CPTSD category
- Comorbidity captures DSO-like features
Historical DESNOS
- Earlier complex trauma construct
- Informed CPTSD debate
- Not ICD-11 formal label
- Useful formulation language only
Latent profile analyses support separable PTSD and CPTSD symptom classes rather than a single severity continuum alone, which underpins the ICD-11 split for teaching and measurement.[3]
Epidemiology and risk factors
Headline patterns candidates must own
Risk factors for complex presentations. Early-onset interpersonal trauma, cumulative trauma load, disrupted attachment, ongoing threat, low social support, prior psychiatric morbidity, and secondary stressors (poverty, discrimination, housing insecurity). Protective factors include stable relationships, timely culturally safe care, and access to evidence-based trauma therapies.[2][17]
Pathophysiology and mechanisms
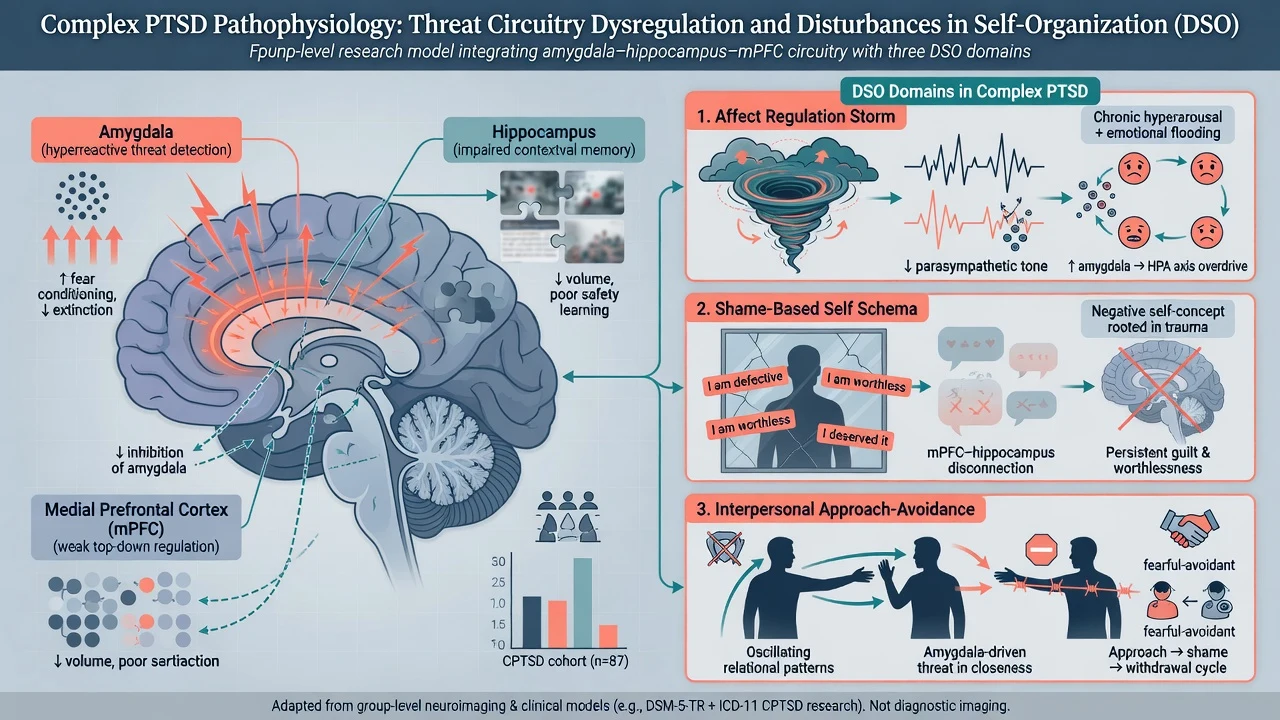
Fear learning. Conditioned threat responses with impaired extinction and overgeneralisation of danger cues underpin intrusion and hypervigilance — shared with PTSD.[17]
DSO mechanisms (exam depth). Affect dysregulation spans under-modulation (emotional flooding, rage, panic) and over-modulation (numbing, shutdown, dissociation). Negative self-concept is often shame-organised ("I am defective / I deserved it"). Relational disturbance reflects approach–avoidance, mistrust, and difficulty using others for co-regulation after interpersonal betrayal.[2][7]
Formulation bridges. Ehlers–Clark current-threat appraisals; biosocial emotion dysregulation (relevant when BPD co-occurs); attachment and mentalization disruption after caregiver trauma. State neurobiology as group-level research, never as a bedside diagnostic scan.[7][17]
Clinical presentation
Classic vignette: prolonged childhood sexual or physical abuse (or adult coercive control / torture), with intrusive trauma memories and nightmares, avoidance of intimacy or reminders, chronic hypervigilance, plus emotional storms or shutdown, deep shame and self-loathing, and unstable or distrustful relationships. Quote the patient ("I am still there"; "I destroy every relationship"; "I am worthless").[2][5]
MSE focus. Affect may swing between restricted and dysregulated; thought content often includes shame, foreshortened future and trauma-linked guilt; perception may include pseudo-hallucinatory flashbacks distinct from primary psychosis; insight into the trauma link is often present; risk assessment is mandatory every contact.[17]
Additional features examiners probe. Dissociation, somatisation, identity disturbance, revictimisation, substance use as self-medication, and difficulty trusting services after institutional harm.[2][7]
Differential diagnosis
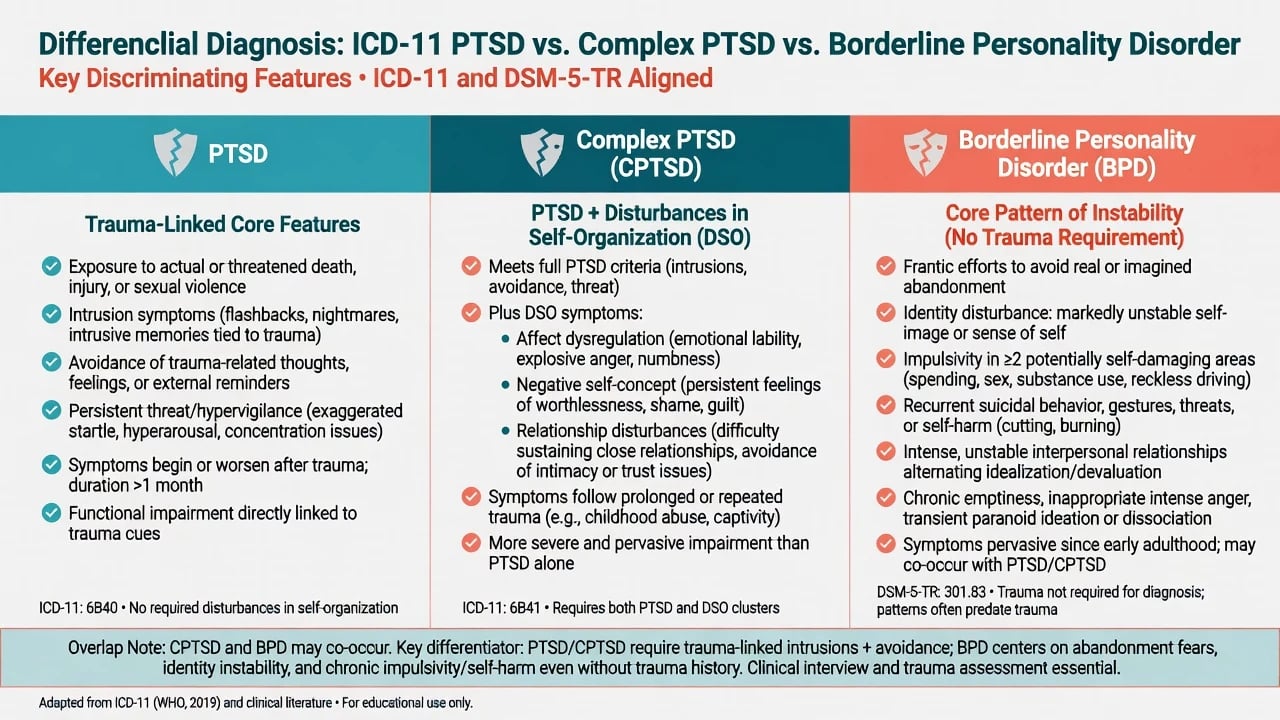
| Discriminator | PTSD (ICD-11) | CPTSD | BPD (DSM-5-TR pattern) |
|---|---|---|---|
| Trauma-linked intrusion/avoidance/threat | Required | Required | Not required |
| DSO triad (affect, self, relationships) | Not full requirement | Required | Emotion dysregulation common; different organising frame |
| Abandonment fear / identity diffusion / emptiness | Variable | Relational disturbance present | Core pattern features |
| Onset organising around trauma | Yes | Yes | Personality pattern often earlier/pervasive |
| Dual diagnosis | — | Possible with BPD | Possible with PTSD/CPTSD |
Clinical guides emphasise that CPTSD and BPD can co-occur; trauma-linked re-experiencing and avoidance distinguish trauma diagnoses, while abandonment-centred impulsivity and identity diffusion weigh toward BPD. Latent class work supports separable PTSD, CPTSD and BPD-related classes rather than one label for all emotion dysregulation.[5][6][7]
Also discriminate MDD alone, bipolar spectrum, primary psychosis (flashbacks vs novel psychotic percepts with thought disorder), ADHD/autism with emotion dysregulation, substance-induced states, and organic personality change with neurological red flags.[17]
Clinical and bedside assessment
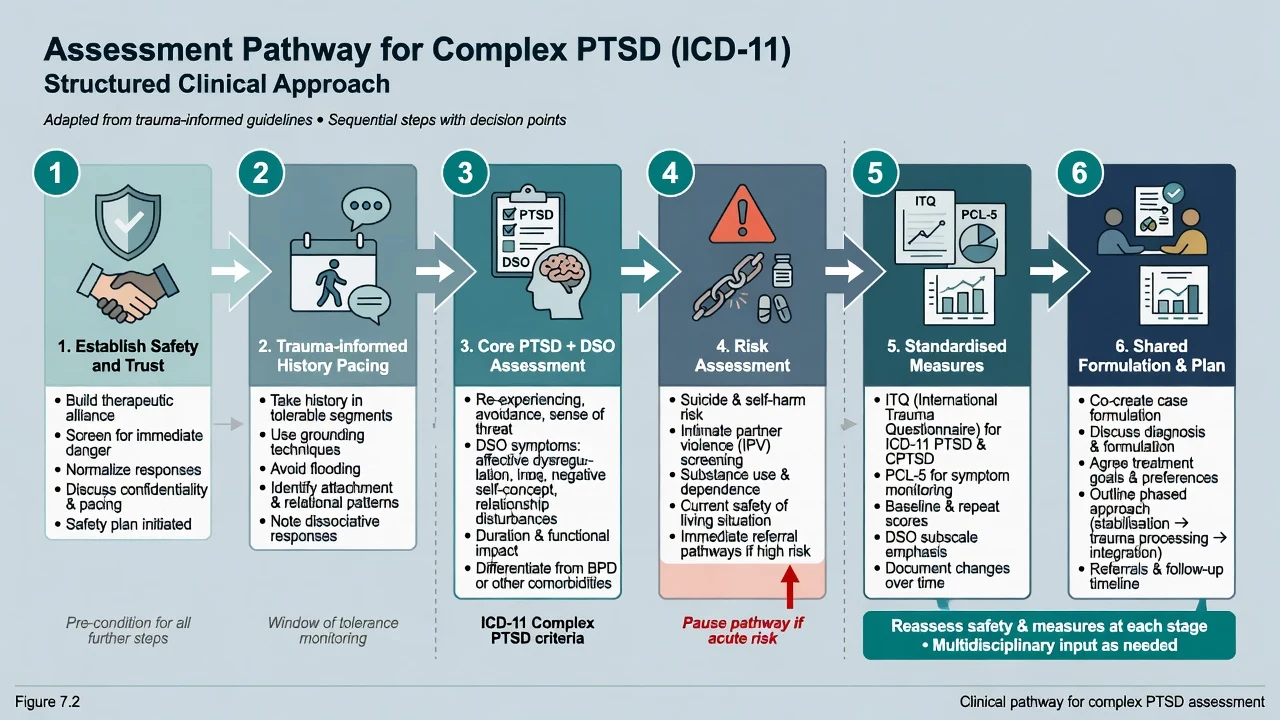
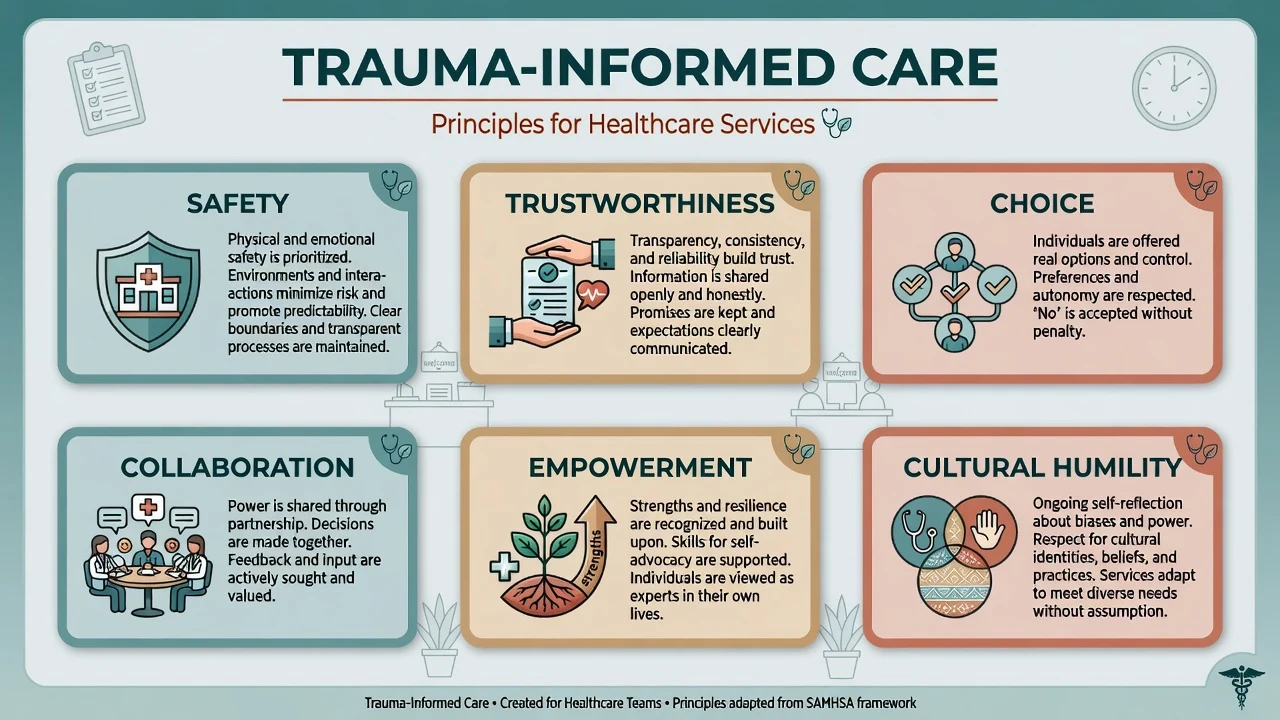
Trauma-informed interview. Safety, trustworthiness, choice, collaboration, empowerment, cultural humility. Obtain enough detail to establish trauma exposure and symptom linkage without forcing a graphic recount in the first minutes. Offer control over pacing, breaks, gender-of-clinician preference and interpreter use.[16][20]
History structure. Trauma chronology and ongoing threat; PTSD core and DSO features with functional impact; depression, dissociation, substance use; medical/TBI; prior treatments (therapy type, dose/adequacy, medications); supports and legal/housing issues.[2]
Risk. Suicide, self-harm, violence, IPV, child protection, vulnerability to revictimisation. Collaborative safety plan and means restriction. Capacity is decision-specific. Involuntary care uses local Mental Health Act principles — least restrictive; do not invent section numbers for the wrong jurisdiction.[16]
Measures.
- International Trauma Questionnaire (ITQ): validated self-report operationalisation of ICD-11 PTSD and CPTSD symptom structure.[4]
- PCL-5: 20-item DSM-5-oriented severity and monitoring tool; does not replace clinical diagnosis or risk assessment.[21]
- Specialist structured interviews (e.g. CAPS-5 for DSM PTSD) when needed for research or complex diagnostic clarification.
Investigations
There is no diagnostic biomarker or MRI for CPTSD. Investigate to exclude mimics and prepare safely for medication: TSH, FBC, U&E, LFT as indicated; ECG when cardiac risk; pregnancy test when relevant; urine drug screen when substance contribution is plausible; sleep study if OSA suspected; neuroimaging only with neurological red flags. Serial ITQ/PCL-5 supports measurement-based care.[4][21][17]
Management — acute / resuscitation
Immediate priorities. Physical safety, medical needs, psychological first aid principles (calm information, contact restoration, practical support). Avoid forced single-session mandatory debriefing of all survivors as universal prevention. Manage acute suicidality, agitation, panic and withdrawal with appropriate pathways; avoid reflexive long-term benzodiazepines for core complex trauma symptoms.[16][17]
Management — definitive and stepwise
Trauma-informed care (systems level)
Trauma-informed care redesigns services so they minimise retraumatisation and maximise engagement. Core principles taught across health systems include safety, trustworthiness, choice, collaboration, empowerment, and cultural humility — building on Harris and Fallot's trauma-informed service design lineage and later public-health elaborations.[20][16]
In practice: transparent processes, predictable appointments, consent for physical contact and trauma detail, shared decision-making, avoidance of coercive practices where safe alternatives exist, staff supervision for secondary trauma, and cultural safety for Indigenous, refugee and minority patients.[20]
Phase-based treatment — evidence and critique
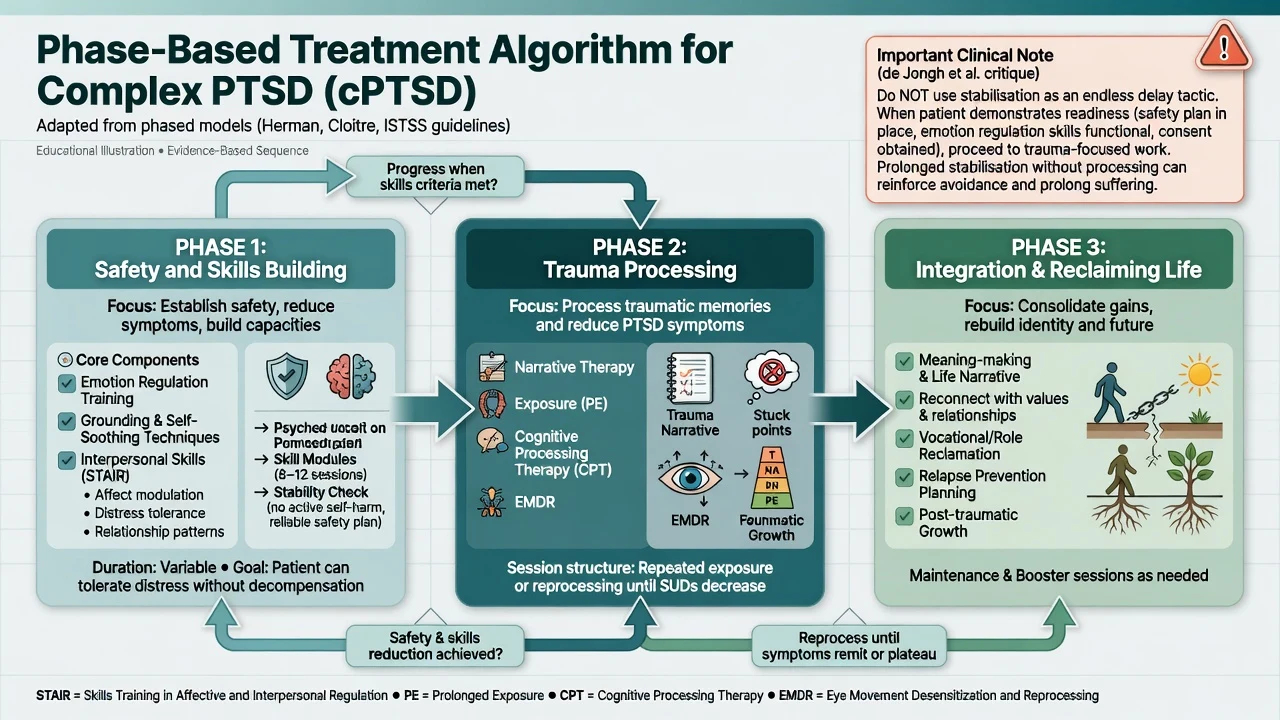
STAIR then trauma work. Skills Training in Affective and Interpersonal Regulation followed by exposure/narrative processing has RCT support in women with childhood-abuse-related PTSD, improving emotion regulation and PTSD outcomes compared with supportive controls or less complete sequences in foundational trials.[8][9]
Do not weaponise stabilisation. De Jongh and colleagues critically argue that current complex-PTSD guideline language can be misread as requiring prolonged phase-based delay for all patients labelled "complex," even when trauma-focused therapy is indicated and feasible. Exam stance: use skills modules and safety work as needed, then proceed to trauma processing when safety, consent and basic regulation allow — avoid both reckless flooding and therapeutic avoidance disguised as endless Phase 1.[10]
Head-to-head work comparing PE, intensified PE and STAIR+PE in childhood-abuse-related PTSD further informs flexible sequencing rather than one mandatory path for every patient.[14]
Trauma-focused psychological therapies
Meta-analyses of psychological interventions targeting CPTSD symptom domains show benefit for PTSD and DSO-related outcomes with multi-component trauma-focused approaches; trauma-focused CBT family therapies and related protocols remain central, with heterogeneity by sample and measures.[11][15]
| Approach | Exam-level mechanism | When candidates mention it |
|---|---|---|
| Prolonged exposure (PE) | Extinction via imaginal and in vivo exposure | Core TF option; adaptable with skills support |
| CPT | Challenge stuck points (safety, trust, power, esteem, intimacy) | Strong interpersonal-violence evidence base |
| TF-CBT / trauma-focused CT | Update threat appraisals and memory meanings | First-line framing in many guidelines |
| EMDR | Dual-attention processing of trauma memory | Preference/access alternative among TF therapies |
| STAIR Narrative Therapy | Skills then narrative trauma processing | Childhood-abuse / complex presentations |
| DBT-PTSD | DBT skills + trauma-focused modules | Complex childhood-abuse presentations; RCT vs CPT |
PE has foundational RCT support in PTSD generally; choice among bona fide trauma-focused modalities is guided by preference, availability, comorbidity and therapist competence.[22][15][16]
DBT-PTSD. In women survivors of childhood abuse with complex PTSD presentations, a multicentre RCT found DBT-PTSD superior to CPT on PTSD severity outcomes, supporting a modular skills-plus-trauma protocol for highly complex presentations.[12]
Network and component meta-analytic work on interventions after complex traumatic events supports multi-component psychological care addressing PTSD and comorbidity, with pharmacotherapy as adjunct rather than sole care.[13]
Pharmacotherapy — agent, dose, monitoring
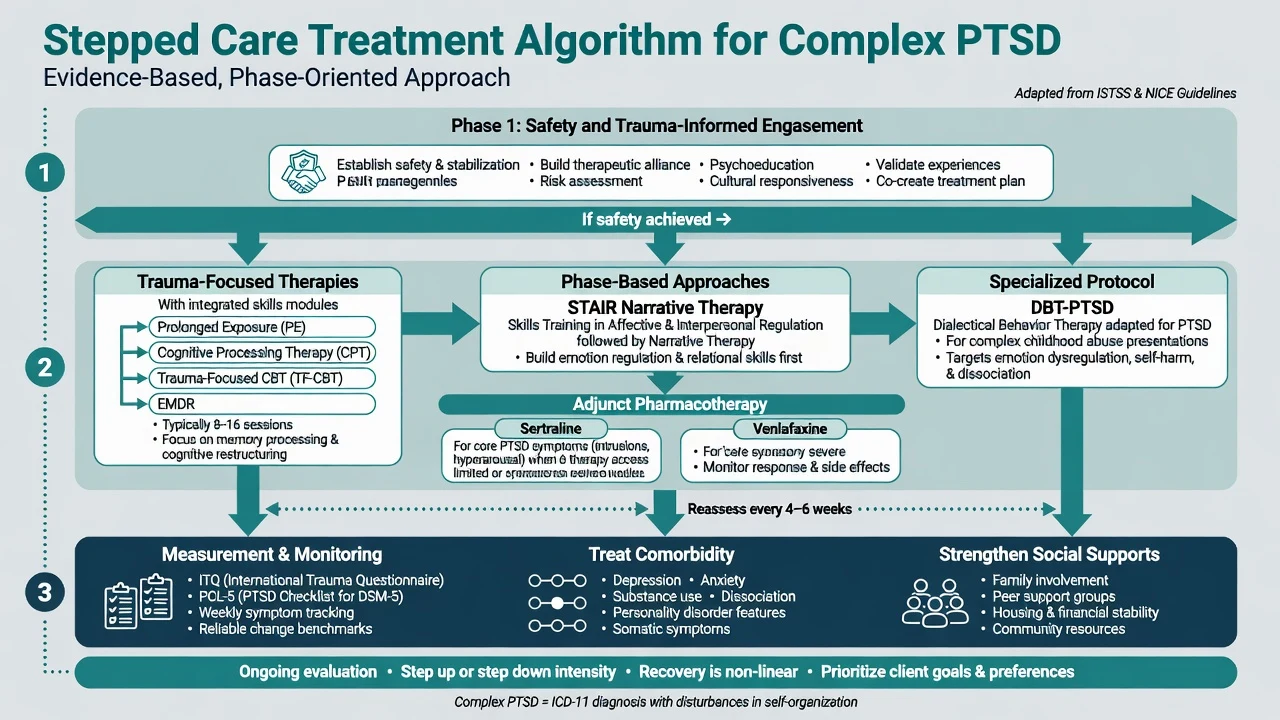
Medication does not replace trauma-focused psychological treatment when that treatment is available and acceptable. When chosen (preference, limited therapy access, severe comorbid depression/anxiety, partial response), first-line evidence for PTSD symptoms supports certain SSRIs and venlafaxine XR.[18][19][13]
| Agent | Typical adult start | Common range | Monitoring notes |
|---|---|---|---|
| Sertraline | 25–50 mg orally daily | 50–200 mg daily | Sexual dysfunction, GI effects; review early for activation/suicidality |
| Paroxetine | 20 mg orally daily | 20–50 mg daily | Anticholinergic/discontinuation risk; pregnancy caution |
| Venlafaxine XR | 75 mg orally daily | 75–225 mg daily | Monitor BP; discontinuation symptoms |
Typical adult oral ranges for exam answers; individualise and check local product information.[18][19]
Adequate trial. Therapeutic dose for about 6–12 weeks for core PTSD response assessment, adherence check, side-effect management, and parallel psychotherapy whenever possible. Avoid long-term benzodiazepines as default for complex trauma hyperarousal; reserve antipsychotics for true comorbidity or specialist contexts, not uncomplicated CPTSD.[17][18]
Australian and New Zealand practice draws on national ASD/PTSD guidance traditions and trauma service models: trauma-focused psychological therapies first-line where skilled therapists exist; specialist trauma or veteran pathways for complex presentations; SSRIs/SNRIs as pharmacologic options; cultural safety expectations in Indigenous and refugee care.[16]
Specific subtypes and scenarios
Childhood abuse pathway. STAIR Narrative Therapy and DBT-PTSD have direct trial relevance; expect high shame, dissociation and trust barriers.[9][12]
IPV and coercive control. Safety planning and protection pathways co-equal therapy; exposure homework is unethical while the patient remains in immediate violent danger.[16][20]
Refugee/torture trauma. Interpreter, cultural formulation, medical sequelae of torture, asylum stress as ongoing threat — CPTSD features common in specialist clinics.[2]
Military/veteran. High cumulative load; moral injury as a formulation concept (not a DSM diagnosis); veteran-competent services and TF protocols.[17]
CPTSD with BPD. Dual formulation allowed; combine structured personality-disorder skills pathways (e.g. DBT elements) with trauma-focused sequencing rather than forcing one exclusive label.[6][12]
Complications and pitfalls
- Retraumatising assessment or coercive institutional practices.
- Endless stabilisation that never reaches trauma processing when the patient is ready.[10]
- Premature flooding without skills support in highly unstable/dissociative patients.
- Mutual-exclusion myths (trauma equals CPTSD; BPD cannot co-exist with CPTSD).
- Token SSRI doses or declaring therapy "failed" after two irregular sessions.
- Benzodiazepine dependence; polypharmacy; staff splitting; clinician secondary trauma without supervision.[7][17]
Prognosis and disposition
Meaningful improvement is achievable with structured multi-component care. Predictors of harder course include ongoing threat, severe substance dependence, profound dissociation, poor alliance and inadequate treatment dose. Disposition ladder: GP and community psychology; specialist trauma services; personality-disorder pathways when BPD co-occurs; crisis teams; voluntary or involuntary inpatient care when risk demands. Functional goals (relationships, parenting, work, reclaiming life) matter as much as scale points.[11][13][16]
Special populations
Children and adolescents. Developmental expression differs; trauma-focused CBT adapted for youth is first-line in paediatric pathways — full CAP depth is a related specialty topic. Caregiver safety is essential.[16]
Pregnancy and lactation. Prioritise psychotherapy when accessible; if an SSRI is needed, individualise risk–benefit (sertraline often discussed favourably). Untreated severe risk is not "safer" by default.[18]
Older adults. Delayed recognition of early-life trauma, medical comorbidity, falls and SSRI hyponatraemia risk require careful agent choice.[17]
Indigenous peoples, refugees and cultural minorities. Cultural safety, interpreter use, community supports; avoid pathologising cultural grief while still offering effective trauma care.[16][20]
Evidence, guidelines and controversies
Landmark threads: ICD-11 proposals (Maercker); evidence review (Brewin); latent profiles (Cloitre); ITQ validation (Hyland); PTSD/CPTSD/BPD discrimination (Cloitre, Karatzias, Ford); STAIR trials (Cloitre 2002, 2010); de Jongh critical analysis of phase-based guidelines; Karatzias CPTSD treatment meta-analysis; Bohus DBT-PTSD RCT; Coventry complex trauma network meta-analysis; Oprel PE/STAIR comparisons; Cochrane psychotherapy evidence; ISTSS guideline methodology; sertraline and venlafaxine pharmacotherapy; Harris/Fallot trauma-informed design.[1][2][8][9][10][11][12][13][16][20]
Controversies to defend both sides. Mandatory phase-based care versus flexible early trauma-focused therapy; CPTSD nosology versus dimensional personality models; whether "trauma-informed" reforms services or becomes empty branding without TF treatment access.[6][10][20]
Exam pearls
COMPLEX
- CPTSD formula: PTSD + DSO (affect, self, relationships).[1][2]
- ITQ operationalises ICD-11 PTSD/CPTSD; PCL-5 monitors DSM-oriented severity.[4][21]
- STAIR+processing is tested sequencing; de Jongh warns against indefinite Phase 1.[8][10]
- DBT-PTSD has RCT support versus CPT in complex childhood-abuse presentations.[12]
- Drugs with doses: sertraline 50–200 mg; venlafaxine XR 75–225 mg (adult typical ranges).[18][19]
- CASC first move: safety, choice, collaboration — then nosology and treatment plan.
Self-test: 30-second viva opener
"ICD-11 complex PTSD is PTSD core plus disturbances of self-organisation — affect dysregulation, negative self-concept and relational disturbance — typically after prolonged interpersonal trauma. I assess with trauma-informed pacing, risk and ITQ/PCL-5, distinguish BPD using abandonment and identity discriminators while allowing comorbidity, deliver skills-supported trauma-focused therapy such as STAIR sequencing, PE/CPT/EMDR or DBT-PTSD without endless stabilisation delay, and use sertraline or venlafaxine as adjuncts when indicated inside a trauma-informed service."[2][6][11][12]
References
- [1]Maercker A, Brewin CR, Bryant RA, Cloitre M, et al. Diagnosis and classification of disorders specifically associated with stress: proposals for ICD-11 World Psychiatry, 2013.PMID 24096776
- [2]Brewin CR, Cloitre M, Hyland P, Shevlin M, et al. A review of current evidence regarding the ICD-11 proposals for diagnosing PTSD and complex PTSD Clin Psychol Rev, 2017.PMID 29029837
- [3]Cloitre M, Garvert DW, Brewin CR, Bryant RA, et al. Evidence for proposed ICD-11 PTSD and complex PTSD: a latent profile analysis Eur J Psychotraumatol, 2013.PMID 23687563
- [4]Hyland P, Shevlin M, Brewin CR, Cloitre M, et al. Validation of post-traumatic stress disorder (PTSD) and complex PTSD using the International Trauma Questionnaire Acta Psychiatr Scand, 2017.PMID 28696531
- [5]Cloitre M, Garvert DW, Weiss B, Carlson EB, et al. Distinguishing PTSD, Complex PTSD, and Borderline Personality Disorder: A latent class analysis Eur J Psychotraumatol, 2014.PMID 25279111
- [6]Karatzias T, Bohus M, Shevlin M, Hyland P, et al. Distinguishing between ICD-11 complex post-traumatic stress disorder and borderline personality disorder: clinical guide and recommendations for future research Br J Psychiatry, 2023.PMID 37381070
- [7]Ford JD, Courtois CA Complex PTSD, affect dysregulation, and borderline personality disorder Borderline Personal Disord Emot Dysregul, 2014.PMID 26401293
- [8]Cloitre M, Koenen KC, Cohen LR, Han H Skills training in affective and interpersonal regulation followed by exposure: a phase-based treatment for PTSD related to childhood abuse J Consult Clin Psychol, 2002.PMID 12362957
- [9]Cloitre M, Stovall-McClough KC, Nooner K, Zorbas P, et al. Treatment for PTSD related to childhood abuse: a randomized controlled trial Am J Psychiatry, 2010.PMID 20595411
- [10]De Jongh A, Resick PA, Zoellner LA, van Minnen A, et al. CRITICAL ANALYSIS OF THE CURRENT TREATMENT GUIDELINES FOR COMPLEX PTSD IN ADULTS Depress Anxiety, 2016.PMID 26840244
- [11]Karatzias T, Murphy P, Cloitre M, Bisson J, et al. Psychological interventions for ICD-11 complex PTSD symptoms: systematic review and meta-analysis Psychol Med, 2019.PMID 30857567
- [12]Bohus M, Kleindienst N, Hahn C, Müller-Engelmann M, et al. Dialectical Behavior Therapy for Posttraumatic Stress Disorder (DBT-PTSD) Compared With Cognitive Processing Therapy (CPT) in Complex Presentations of PTSD in Women Survivors of Childhood Abuse: A Randomized Clinical Trial JAMA Psychiatry, 2020.PMID 32697288
- [13]Coventry PA, Meader N, Melton H, Temple M, et al. Psychological and pharmacological interventions for posttraumatic stress disorder and comorbid mental health problems following complex traumatic events: Systematic review and component network meta-analysis PLoS Med, 2020.PMID 32813696
- [14]Oprel DAC, Hoeboer CM, Schoorl M, de Kleine RA, et al. Effect of Prolonged Exposure, intensified Prolonged Exposure and STAIR+Prolonged Exposure in patients with PTSD related to childhood abuse: a randomized controlled trial Eur J Psychotraumatol, 2021.PMID 34630934
- [15]Bisson JI, Roberts NP, Andrew M, Cooper R, Lewis C Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults Cochrane Database Syst Rev, 2013.PMID 24338345
- [16]Bisson JI, Berliner L, Cloitre M, Forbes D, et al. The International Society for Traumatic Stress Studies New Guidelines for the Prevention and Treatment of Posttraumatic Stress Disorder: Methodology and Development Process J Trauma Stress, 2019.PMID 31283056
- [17]Yehuda R, Hoge CW, McFarlane AC, Vermetten E, et al. Post-traumatic stress disorder Nat Rev Dis Primers, 2015.PMID 27189040
- [18]Brady K, Pearlstein T, Asnis GM, Baker D, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial JAMA, 2000.PMID 10770145
- [19]Davidson J, Baldwin D, Stein DJ, Kuper E, et al. Treatment of posttraumatic stress disorder with venlafaxine extended release: a 6-month randomized controlled trial Arch Gen Psychiatry, 2006.PMID 17015818
- [20]Harris M, Fallot RD Designing trauma-informed addictions services New Dir Ment Health Serv, 2001.PMID 11291263
- [21]Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation J Trauma Stress, 2015.PMID 26606250
- [22]Foa EB, Hembree EA, Cahill SP, Rauch SA, et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: outcome at academic and community clinics J Consult Clin Psychol, 2005.PMID 16287395