Psych · General adult psychiatry — psychotic disorders
Delusional disorder
Also known as Paranoia · Persistent delusional disorder · Simple delusional disorder · Othello syndrome · de Clérambault syndrome · Paranoid disorder
Exam-exhaustive fellowship reference on delusional disorder — DSM-5-TR and ICD-11 criteria; subtypes (persecutory, jealous, erotomanic, somatic, grandiose); discrimination from schizophrenia and mood psychosis; engagement without collusion; limited RCT evidence for antipsychotics (Cochrane); risk by subtype; late-life care; RANZCP/APA-oriented guidance. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Delusional disorder is the examinable “quiet psychosis”: high conviction, often low surface chaos, and high potential for relationship, forensic, and medical harm. Fellowship answers fail when they treat it as mild schizophrenia, argue the patient out of the belief, or ignore Othello violence risk while debating nosology.[1][2][7]
Overview and definition
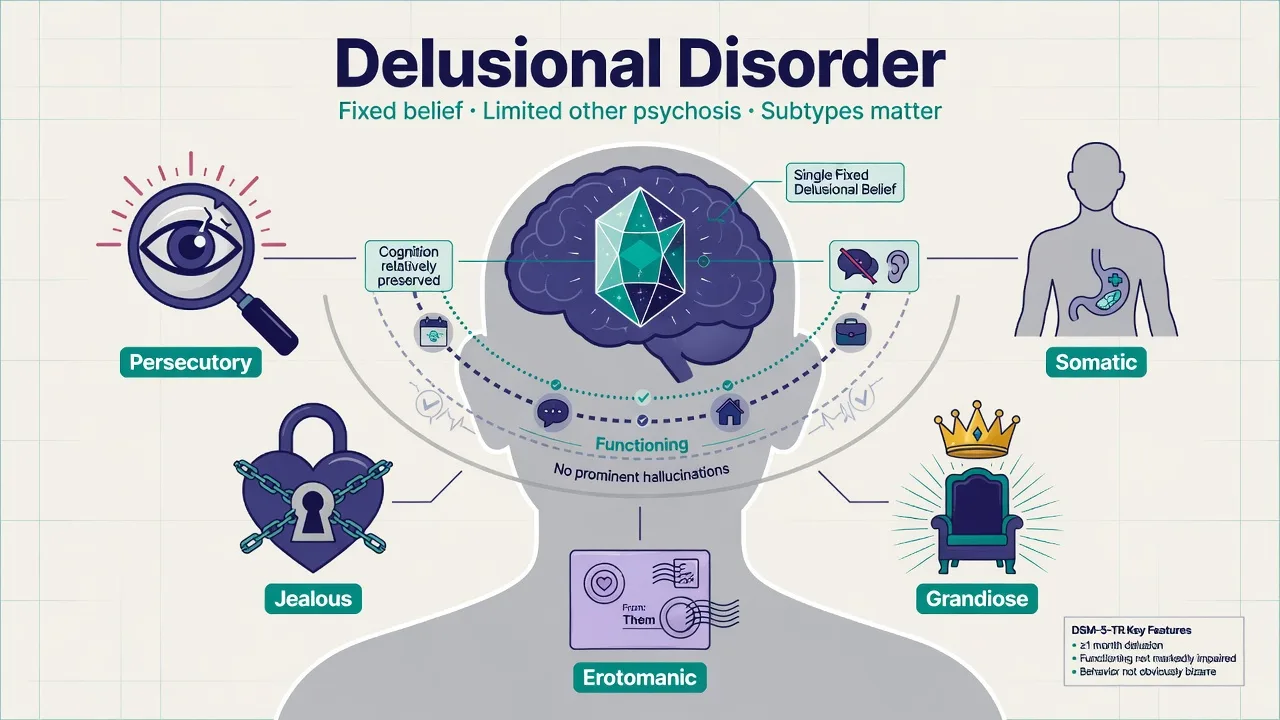
Delusional disorder is defined by the presence of one or more delusions of sufficient duration (DSM-5-TR operational threshold ≥1 month) in the absence of a full schizophrenia Criterion A picture. Hallucinations, if present, are not prominent and are typically related to the delusional theme; behaviour is not markedly odd or bizarre outside delusional content; and functioning is often not markedly impaired except as a direct consequence of the delusion.[2][7][19]
Historical nosology (viva line). Kendler’s review of “paranoia / simple delusional disorder” defended its nosologic validity against collapse into schizophrenia — a still-useful framing for exams that ask whether delusional disorder is “just incomplete schizophrenia.”[1] Opjordsmoen’s “partial psychosis” concept captures the same clinical intuition: circumscribed psychotic process with relatively preserved residual function and cognition compared with schizophrenia averages.[2][12]
ICD-11. ICD-11 uses persistent delusional disorder language for enduring delusional syndromes not better explained by schizophrenia, mood disorder with psychosis, or substance/medical causes. State the manual in the stem and avoid inventing identical day-count wording across systems when the exam specifies ICD.[2][7]
Bizarre content trap. Classic teaching emphasised non-bizarre (possible) themes. Contemporary DSM nosology allows bizarre delusions in delusional disorder if other criteria are met — do not fail a stem solely because content is bizarre.[7][19]
Classification and subtypes
| Subtype | Core false belief | Exam eponym / cue | Priority risk |
|---|---|---|---|
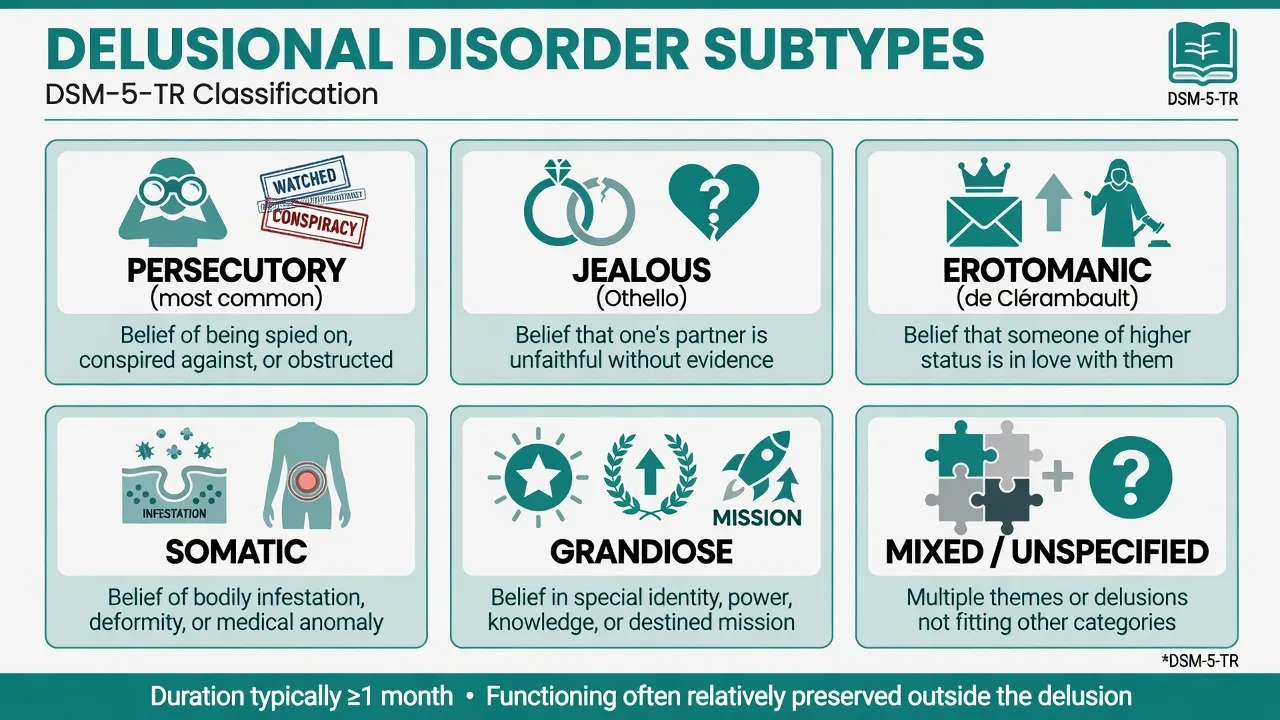
| Persecutory | Conspired against, spied on, obstructed | Most common in many series | Defensive violence, legal conflict |
| Jealous | Partner is unfaithful without adequate evidence | Othello | Partner-directed violence |
| Erotomanic | Another person (often higher status) is in love with them | de Clérambault | Stalking, boundary breach |
| Somatic | Bodily disease, deformity, infestation, odour, malfunction | Interface with BDD/illness anxiety/Ekbom-type themes | Self-surgery, medical shopping |
| Grandiose | Special identity, power, discovery, mission | Overlaps mania differential | Financial/legal recklessness |
| Mixed / Unspecified | Multiple themes or no single dominant theme | — | Theme-specific |
Epidemiology and risk factors
Numbers and framing candidates must own
Strictly defined delusional disorder is less common than schizophrenia in clinical services; population studies of psychotic disorders show a broader psychosis spectrum when carefully ascertained.[14][7] Do not invent a single universal lifetime percentage as dogma — own the comparative rarity and later-onset tendency relative to schizophrenia, and the need for organic vigilance in late-life presentations.[9][14]
Risk correlates. Premorbid personality disorder is enriched in some delusional-disorder samples and associates with clinical severity markers — personality does not replace the psychotic diagnosis but informs engagement and prognosis.[22] Genetic data are limited; family and spectrum debates continue rather than a unique Mendelian story.[21][1]
Pathophysiology and mechanisms
There is no unique “delusional-disorder circuit” examiners expect you to invent. Viva-safe synthesis as a partial psychosis with continuum and affective scaffolds:[2][17][20][24]
- Partial psychosis with relatively circumscribed positive symptoms and better average residual function/cognition than schizophrenia on many comparisons.[2][10][11][12]
- Dopamine final common pathway language still explains why D2-modulating antipsychotics can reduce conviction/preoccupation/distress for some patients, even when belief does not fully extinguish.[17][8]
- Paranoia continuum: ideas of reference and persecution exist dimensionally in the general population; clinical delusions sit at the extreme of conviction, distress, and behavioural impact.[20]
- Affective and personality core: irritability, shame, attachment threat, and suspicious cognitive style may scaffold persecutory and jealous systems without reducing the case to pure personality disorder.[24][22]
- Neuropsychology: subtle social-cognitive and executive findings are reported; gross dementia-level impairment should redirect the differential.[23][12]
Clinical presentation
MSE language. Systematised delusion(s) held with high conviction and often elaborate “evidence”; affect congruent with theme (wary, jealous, infatuated, disgusted with body); speech goal-directed outside theme; sensorium clear; cognition grossly intact on bedside screen; insight typically poor regarding the belief but sometimes preserved for need for sleep/stress help.[2][10]
Preserved role function at work or in public, with chaos concentrated in the relational domain of the delusion, is a classic tip toward delusional disorder rather than active multi-domain schizophrenia.[7][12]
Late-life. Older adults may present with first-episode persistent delusions amid isolation, sensory impairment, medical comorbidity, or evolving neurodegenerative disease — always dual-track psychiatric and organic formulation.[9]
Shared/induced delusions. A close dyad may share a delusional system (historically folie à deux). Assess both parties, power dynamics, and separation effects carefully; the secondary partner may improve with distance and support.[2]
Differential diagnosis
| Differential | Points toward this | Points toward delusional disorder |
|---|---|---|
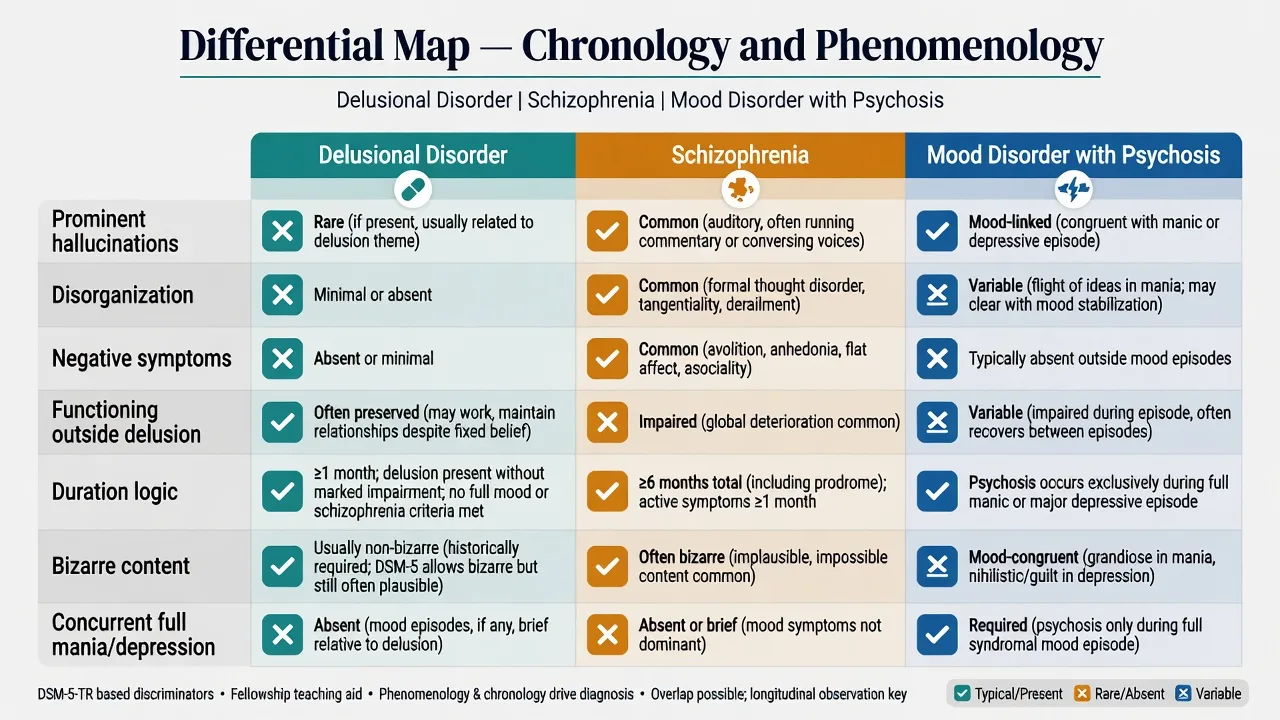
| Schizophrenia | Prominent hallucinations, disorganisation, negative symptoms, broad functional collapse | Circumscribed delusions; limited other Criterion A; better residual function |
| Mood disorder with psychosis | Full mania/MDD; psychosis only during mood | Delusions persist euthymic; mood symptoms brief or secondary |
| Paranoid personality | Lifelong suspicious style; overvalued ideas; less fixed false belief | True delusion with conviction/unshakeability meeting psychotic threshold |
| OCD / BDD / illness anxiety | Insight spectrum; intrusive ego-dystonic quality common | Fixed false belief without obsessional quality |
| Substance/medication | Timeline tied to intoxication/withdrawal/agent | Persists well beyond substance window |
| Organic (delirium, encephalitis, dementia, sensory loss) | Fluctuating attention, neurology, cognitive plunge | Clear sensorium, stable psychiatric course after work-up |
Clinical and bedside assessment
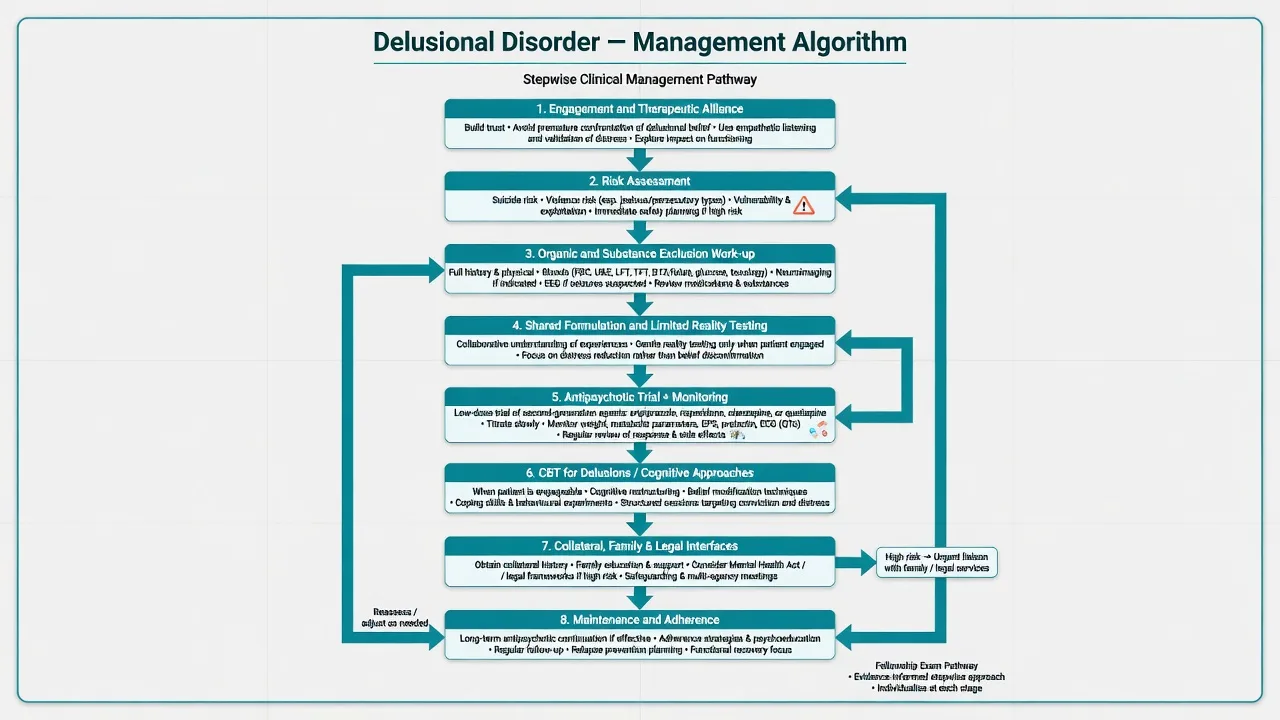
Structure as alliance + theme map + risk + organic screen + collateral + capacity.[15][16]
- Engagement first — explore content and function of the belief without collusion or humiliation.[5][15]
- Duration, onset, systematisation, acting-on-belief, substances, sleep, mood, prior treatment.
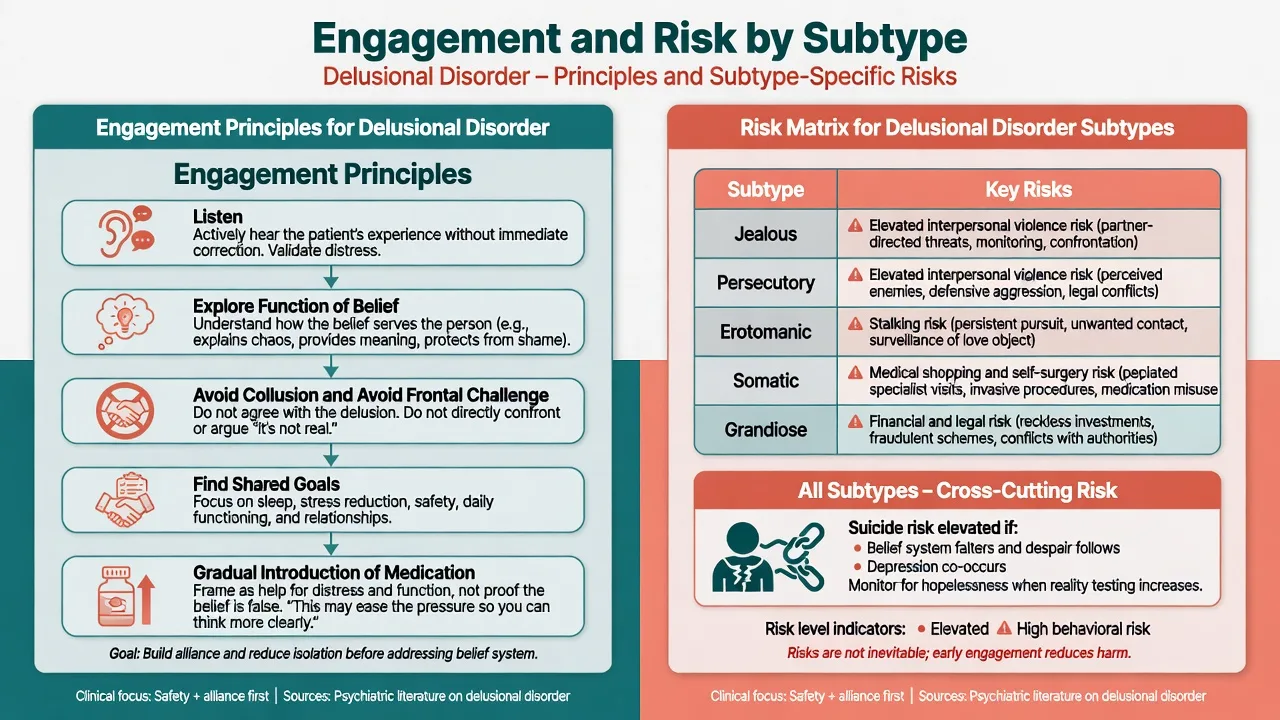
- Risk by subtype (see management figure): suicide, partner violence, stalking, self-surgery, financial harm, child protection.
- Capacity for treatment and other decisions; least-restrictive legal pathway under local statute (do not invent foreign section numbers).
- Collateral is often decisive — families may describe years of quiet systematisation missed in a single MSE.
- Scales conceptually: PANSS positive items for change; research paranoia scales (e.g. GPTS family) for dimensional framing — not required for diagnosis.[20][16]
Investigations
Before antipsychotics, complete a physical-health baseline aligned with schizophrenia-spectrum standards.[15][16]
- Bloods: FBC, U&E/eGFR, LFT, fasting glucose or HbA1c, lipids; TFT when indicated.
- ECG: QTc and cardiac risk before many antipsychotics (historical pimozide caution is a classic exam line).[6][8]
- BMI/BP/waist; pregnancy test when relevant.
- Urine drug screen supports formulation; negative does not exclude primary DD.
- CT/MRI, EEG, autoimmune work-up when first presentation is atypical, late, focal, seizure-associated, or cognitively collapsing.[9][15]
- Sensory assessment (vision/hearing) in older adults.[9]
- Somatic subtype: rule out genuine medical disease once, then coordinate liaison care to prevent endless invasive procedures.[8]
Management — acute and emergency
Agitation. De-escalate; oral medication before IM when safe; follow local rapid-tranquillisation protocol.[15][16]
Medical mislabel. Fever, fluctuating attention, rigidity after antipsychotics, or new neurology — rethink delirium, encephalitis, NMS rather than “non-compliant DD.”[15]
Management — definitive and stepwise
Engagement model
Successful care almost always hinges on alliance: listen and validate distress (not the false belief); explore what the belief does for the person (meaning, control, threat detection); avoid collusion (“yes, they are spying”) and avoid humiliating frontal challenge (“that’s ridiculous”); negotiate shared goals (sleep, stress, safety, work performance, relationship damage control); and frame medication as help for pressure, preoccupation, sleep, and function — not as a loyalty test that the belief is false.[5][6][15]
Antipsychotic treatment — evidence honesty
Cochrane review finds insufficient high-quality randomised evidence specific to delusional disorder treatments — exam answers must not invent a gold-standard RCT hierarchy unique to DD.[3][4] Historical and clinical literature (including Munro’s pimozide-era work and later SGA series) still supports offering an antipsychotic with careful monitoring, often with partial benefit on preoccupation, anxiety, and behaviour even when the belief persists.[5][6][8]
Seventy years of antipsychotic use in delusional disorder show evolving agent preference (older high-potency/pimozide emphasis toward modern second-generation agents) without a definitive head-to-head winner in pure DD RCTs.[8] Aripiprazole has published clinical reports in delusional disorder and is a reasonable first-line candidate when metabolic sparing and lower sedation are priorities.[13]
Illustrative adult oral frameworks (individualise; localise to product information, age, comorbidity, prior response; schizophrenia-spectrum dosing evidence informs practice where DD-specific RCTs are thin):
| Agent | Typical adult oral approach | Key monitoring |
|---|---|---|
| Aripiprazole | Often start 5–10 mg daily; common target 10–15 mg daily (up to 30 mg if needed and tolerated) | Akathisia, impulse-control rare signals |
| Risperidone | Often 1–2 mg daily; titrate toward 2–6 mg | Prolactin, EPS |
| Olanzapine | Often 5–10 mg nightly; titrate toward 10–20 mg | Weight, glucose, lipids, sedation |
| Quetiapine | Sedating option; titrate by indication (e.g. toward 300–600 mg divided/nightly as tolerated for psychosis ranges) | Metabolic, BP, sedation |
| Haloperidol (selected cases) | Low–moderate potency dosing with EPS vigilance | EPS, QTc, NMS |
| Historical pimozide | Exam pearl only — cardiac/QTc caution; not automatic first line in modern practice | ECG |
| Dose ranges above are illustrative adult frameworks drawn from clinical DD series, historical treatment reviews, comparative antipsychotic evidence, and schizophrenia-spectrum physical-health monitoring standards — always individualise.[13][18][15][16][6][8] |
Trial adequacy. Allow a fair window at a therapeutic dose (often in the order of 4–6 weeks) with adherence checked before declaring failure; success metrics include reduced acting-on-belief, sleep, anxiety, and functional friction — not only full belief extinction.[5][15][16]
LAI. Consider long-acting injectable antipsychotics when non-adherence drives relapse risk and the patient accepts the rationale within an alliance model.[15][16]
Psychological and social interventions
- CBT-informed approaches for delusions: collaborative empiricism, graded reality testing, work on worry/safety behaviours, and behavioural experiments when engagement allows.[5][15]
- Family education without triangulation into the delusional system.
- Occupational and legal support when grandiose or persecutory themes threaten finances or court involvement.
- Multidisciplinary collaboration for somatic subtype and forensic interfaces.[8]
Regional guidance
ANZ (RANZCP). Apply schizophrenia and related disorders guideline principles: comprehensive assessment, physical health, recovery orientation, least-restrictive care, and antipsychotic use with metabolic monitoring — adapted to the engagement-heavy reality of delusional disorder.[15]
USA (APA). Schizophrenia practice guideline frameworks for antipsychotic choice, shared decision-making, and monitoring transfer where an antipsychotic is used.[16]
UK/other. NICE psychosis/schizophrenia pathways inform CBTp access and physical health checks; pure DD may sit under related-disorder care depending on local service design. Always localise legal statutes. Core psychosis care standards still apply when antipsychotics are used.[15][16]
Subtypes and special scenarios
Jealous (Othello)
- Partner monitoring, accusations, 'evidence' gathering
- Highest domestic violence exam yield
- Safety plan for partner and children
- Do not mediate as 'relationship counselling' alone
Persecutory
- Workplace/neighbour conspiracy themes common
- Defensive aggression risk
- Legal complaints and counter-complaints
- Sleep and substance use as amplifiers
Erotomanic
- de Clérambault pattern
- Stalking and boundary breaches
- Protect named third parties
- Clear professional boundaries in team
Somatic
- Infestation, odour, deformity, organ dysfunction
- Liaison with dermatology/ENT/GP
- Prevent unnecessary surgery
- Rule-out once, then psychiatric lead
Late-life. Prioritise sensory correction, social isolation, medical comorbidity, and neurodegenerative differentials while still treating distressing delusional systems.[9]
Cultural formulation. Distinguish culturally sanctioned beliefs from pathological delusions using collateral, distress, disability, and deviation from the person’s cultural reference group — never use “culture” as a reason to ignore risk.[15]
Complications and pitfalls
- Misdiagnosing schizophrenia as “just delusional disorder” and under-treating multi-domain psychosis — or the reverse, over-labelling high-functioning DD as schizophrenia.[7][10]
- Collusion or frontal challenge destroying alliance.[5]
- Missing Othello violence risk.[7]
- Antipsychotic metabolic, EPS, prolactin, and QTc harms — monitor as for schizophrenia-spectrum care.[15][16][18]
- Iatrogenic harm from endless somatic investigation or exploratory surgery.[8]
- Ignoring comorbid depression and suicide when the belief system falters or isolation deepens.[15][24]
Prognosis and disposition
Course is often chronic with fluctuating conviction. Partial response is common and clinically valuable. Predictors include engagement quality, adherence, substance use, forensic escalation, support network, and comorbid mood/personality load.[2][5][12]
Disposition. Most patients are managed in outpatient/community settings if risk is contained. Admit for high violence/suicide risk, diagnostic uncertainty with organic red flags, or failed community containment. Relapse signatures: rising preoccupation, acting-on-belief, sleep collapse, substance use, treatment cessation.[15][9]
Exam pearls
Key takeaways
- Delusional disorder is a partial psychosis with fixed delusions and relatively limited other psychotic features — defend the boundary with schizophrenia using phenomenology and function, not vibes.[1][2][7]
- Subtype names risk — Othello and de Clérambault are not trivia; they are safety algorithms.[7]
- Alliance-first care enables any pharmacotherapy; collusion and humiliation both fail.[5]
- Offer an antipsychotic with honest evidence limits (Cochrane) and full metabolic/cardiac monitoring; aripiprazole and other SGAs are reasonable modern choices.[3][13][8][15]
- Measure success by safety, distress, and function, not only full belief extinction.[5][12]
References
- [1]Kendler KS The nosologic validity of paranoia (simple delusional disorder). A review Arch Gen Psychiatry, 1980.PMID 7387341
- [2]Opjordsmoen S Delusional disorder as a partial psychosis Schizophr Bull, 2014.PMID 24421383
- [3]Skelton M, Khokhar WA, Thacker SP Treatments for delusional disorder Cochrane Database Syst Rev, 2015.PMID 25997589
- [4]Skelton M, Khokhar WA, Thacker SP Treatments for Delusional Disorder Schizophr Bull, 2015.PMID 26209547
- [5]Manschreck TC, Khan NL Recent advances in the treatment of delusional disorder Can J Psychiatry, 2006.PMID 16989110
- [6]Munro A, Mok H An overview of treatment in paranoia/delusional disorder Can J Psychiatry, 1995.PMID 8681259
- [7]González-Rodríguez A, Seeman MV Differences between delusional disorder and schizophrenia: A mini narrative review World J Psychiatry, 2022.PMID 35663297
- [8]González-Rodríguez A, Monreal JA, Natividad M, et al. Seventy Years of Treating Delusional Disorder with Antipsychotics: A Historical Perspective Biomedicines, 2022.PMID 36552037
- [9]González-Rodríguez A, Seeman MV, Izquierdo E, et al. Delusional Disorder in Old Age: A Hypothesis-Driven Review of Recent Work Focusing on Epidemiology, Clinical Aspects, and Outcomes Int J Environ Res Public Health, 2022.PMID 35805570
- [10]Muñoz-Negro JE, Ibáñez-Casas I, de Portugal E, et al. A Psychopathological Comparison between Delusional Disorder and Schizophrenia Can J Psychiatry, 2018.PMID 28595494
- [11]Muñoz-Negro JE, Ibanez-Casas I, de Portugal E, et al. A dimensional comparison between delusional disorder, schizophrenia and schizoaffective disorder Schizophr Res, 2015.PMID 26585220
- [12]Díaz-Caneja CM, Cervilla JA, Haro JM, et al. Cognition and functionality in delusional disorder Eur Psychiatry, 2019.PMID 30388425
- [13]Iannuzzi GL, Patel AA, Stewart JT Aripiprazole and Delusional Disorder J Psychiatr Pract, 2019.PMID 30849061
- [14]Perälä J, Suvisaari J, Saarni SI, et al. Lifetime prevalence of psychotic and bipolar I disorders in a general population Arch Gen Psychiatry, 2007.PMID 17199051
- [15]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [16]Keepers GA, Fochtmann LJ, Anzia JM, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia Am J Psychiatry, 2020.PMID 32867516
- [17]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164
- [18]Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis Lancet, 2013.PMID 23810019
- [19]Tandon R, Gaebel W, Barch DM, et al. Definition and description of schizophrenia in the DSM-5 Schizophr Res, 2013.PMID 23800613
- [20]Bebbington PE, McBride O, Steel C, et al. The structure of paranoia in the general population Br J Psychiatry, 2013.PMID 23661767
- [21]Cardno AG, McGuffin P Genetics and delusional disorder Behav Sci Law, 2006.PMID 16705657
- [22]de Portugal E, Díaz-Caneja CM, González-Molinier M, et al. Prevalence of premorbid personality disorder and its clinical correlates in patients with delusional disorder Psychiatry Res, 2013.PMID 23993136
- [23]Abdel-Hamid M, Brüne M Neuropsychological aspects of delusional disorder Curr Psychiatry Rep, 2008.PMID 18652791
- [24]Pellegrini R, Muñoz Negro JE, Ottoni R, et al. The Affective Core of Delusional Disorder Psychopathology, 2022.PMID 35272292