Psych · General adult psychiatry — personality disorders
Dependent personality disorder
Also known as DPD · Dependent PD · Cluster C dependent · Dependent personality · Asthenic personality (historical)
Exam-exhaustive fellowship reference on dependent personality disorder — DSM-5-TR ≥5 of 8 criteria, ICD-11 severity and trait mapping, Bornstein interactionist dependency model, differentials (AVPD, BPD, depression, culture), post-separation risk and IPV, CBT for autonomy and schema therapy, pharmacotherapy only for comorbidity. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Dependent personality disorder (DPD) is a lower-prevalence but high-yield Cluster C topic. FRANZCP MEQs demand the ≥5 of 8 threshold (exam trap versus AVPD/OCPD four-item cut-offs), post-breakup risk formulation, and a treatment plan that promotes autonomy without abandoning the patient. MRCPsych CASC tests non-stigmatising explanation and boundary-safe care. ABPN items test DSM criteria, Bornstein's active-as-well-as-passive dependency model, and discrimination from borderline and avoidant PD. This topic is written so a candidate who has read nothing else can answer at consultant depth.[1][2][3]
Overview and definition
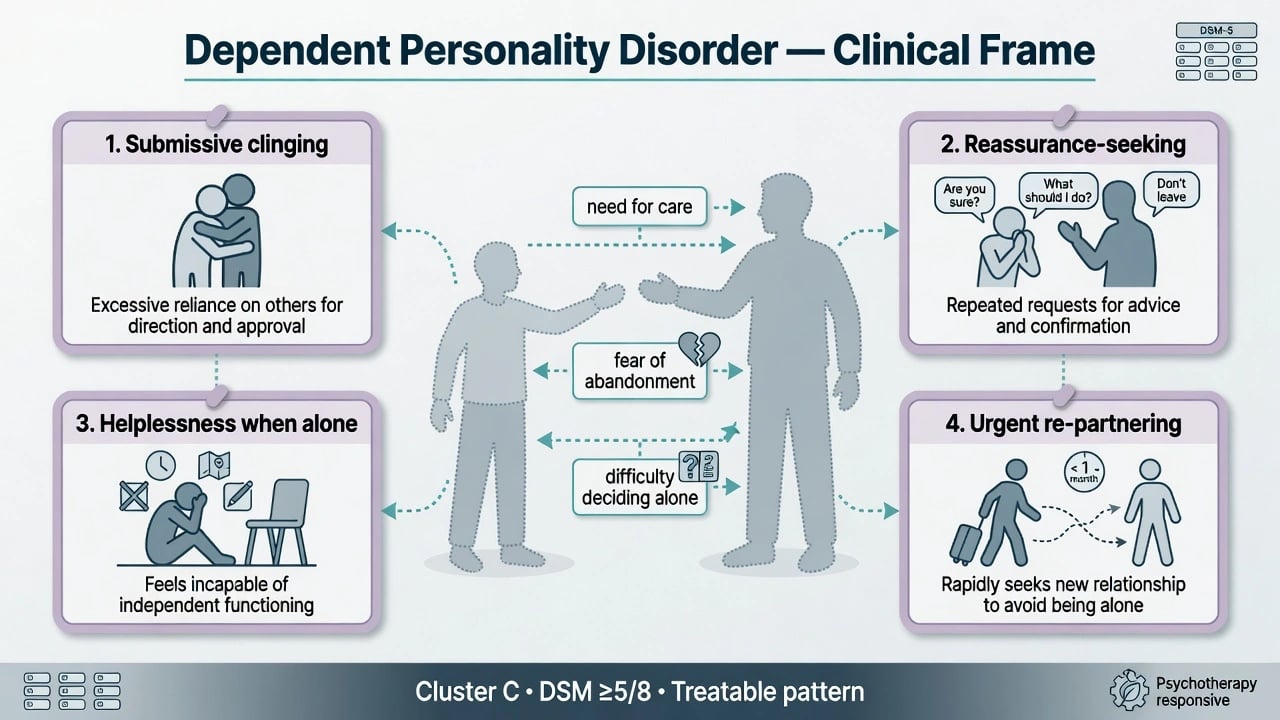
DPD is an enduring, inflexible pattern of excessive need to be taken care of that leads to submissive and clinging behaviour and fears of separation, beginning by early adulthood, present across contexts, and causing distress or impairment — not better explained solely by another mental disorder, substance, or medical condition. The person typically feels unable to function alone, seeks others to assume major life responsibilities, and may urgently re-partner after losses. That caretaking-need pattern is the fellowship discriminator from avoidant personality disorder (fear of evaluation) and from many borderline presentations (abandonment fear with affective instability and identity disturbance).[1][2][3]
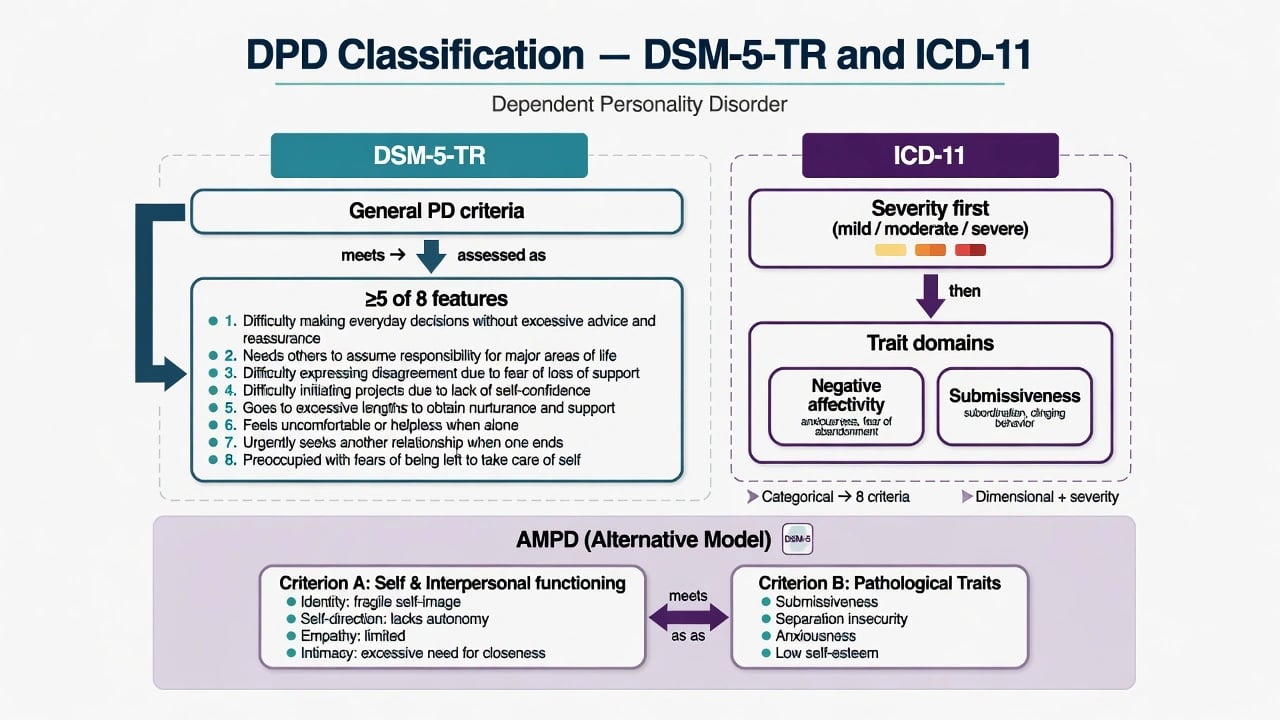
DSM-5-TR structure you must reproduce. After general personality disorder criteria are met, DPD requires five or more of eight features: (1) difficulty making everyday decisions without an excessive amount of advice and reassurance from others; (2) needs others to assume responsibility for most major areas of his or her life; (3) difficulty expressing disagreement with others because of fear of loss of support or approval (do not include realistic fears of retribution); (4) difficulty initiating projects or doing things on his or her own because of a lack of self-confidence in judgment or abilities rather than a lack of motivation or energy; (5) goes to excessive lengths to obtain nurturance and support from others, to the point of volunteering to do things that are unpleasant; (6) feels uncomfortable or helpless when alone because of exaggerated fears of being unable to care for himself or herself; (7) urgently seeks another relationship as a source of care and support when a close relationship ends; (8) is unrealistically preoccupied with fears of being left to take care of himself or herself.[1][4]
ICD-11 framing. Personality disorder is graded by severity of self and interpersonal dysfunction (mild, moderate, severe), then qualified with trait domain descriptors. DPD-like presentations typically map to negative affectivity (anxiousness, separation insecurity) with prominent submissiveness and impaired self-direction; the DSM cluster label is a teaching scaffold, not a biological taxon. Name which system you are applying when thresholds are examined.[1][16]
AMPD language (exam polish). Criterion A: impairment in identity (self as incompetent without others), self-direction (reliance on external guidance), empathy (over-attunement to caretaker approval), and intimacy (submissive, caretaking-focused relationships). Criterion B traits often include submissiveness, anxiousness, and separation insecurity.[1][16]
Classification and nosology
DSM-5-TR categorical
- General PD criteria + ≥5 of 8 features
- Cluster C (anxious/fearful) teaching scaffold
- Urgent re-partnering and fear of being left alone are high-yield
- Must begin by early adulthood and be pervasive
ICD-11 dimensional
- Severity of personality dysfunction first
- Trait domains: negative affectivity, submissiveness
- Optional named pattern language varies by service
- Better for stepped-care intensity decisions
Criteria dimensionality
- Gude: attachment vs dependent behavioural clusters within criteria
- Not a single homogeneous trait
- Formulation can target attachment anxiety and competence separately
- Supports AMPD-style trait language
Normal dependence
- Not diagnosable without pervasive impairment
- Cultural interdependence is not DPD
- Illness-related care-seeking can be adaptive
- Ask functional cost and self-schema of incompetence
DPD is not ordinary need for support during stress. Temporary reliance during medical illness, migration, or acute crisis does not meet the longitudinal PD standard. Conversely, many people with DPD also meet criteria for major depression or anxiety disorders; examiners reward dual diagnosis when both operational thresholds are met rather than forced either/or rhetoric.[1][4][6]
Epidemiology and risk factors
Headline epidemiology candidates must own
Community prevalence for DPD is lower than for several other PDs in large US survey data, but clinical impact is out of proportion when depression, suicide risk after losses, and exploitation are considered. Global meta-analysis of community personality disorder prevalence contextualises method dependence of rates. Twin work supports substantial heritability for dependent PD when carefully measured by interview and questionnaire methods.[5][6][9]
Risk and aetiology. Overprotective or authoritarian parenting, early loss or separation, modelling of helpless care-seeking, and insecure (often preoccupied) attachment feed a self-view of incompetence without a caretaker. Gender and cultural factors influence recognition and help-seeking. None of these factors alone makes the diagnosis; late-onset new dependence is an organic and affective red flag until proven otherwise.[1][3][5]
Pathophysiology and mechanisms
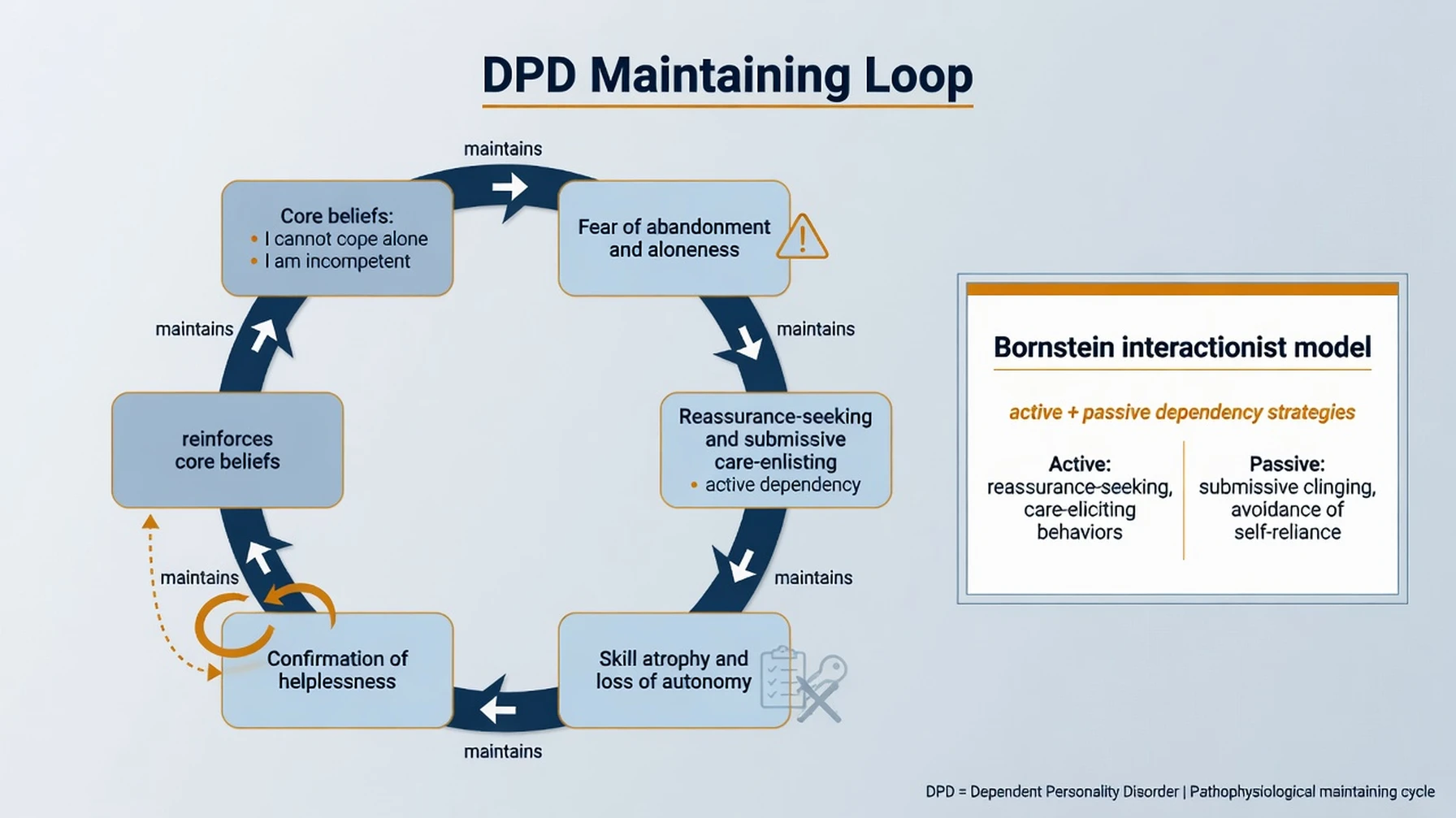
Cognitive-behavioural loop. Core beliefs (“I cannot cope alone / I am incompetent”) and conditional assumptions (“If I disagree or act independently, I will be abandoned”) generate anxiety. Safety behaviours (excessive reassurance-seeking, deferring decisions, volunteering for unpleasant tasks to keep support, urgent re-partnering) reduce short-term anxiety but prevent mastery and produce skill atrophy — confirming the original belief.[1][2][3]
Bornstein interactionist model. Dependency is not only passive clinging. Dependent people may use active strategies to secure support (care-eliciting behaviour, compliance, strategic self-presentation). Dependency can be adaptive in some contexts and maladaptive in others — mature viva language rejects one-dimensional “weak character” framing.[2][3]
Attachment and schema model. Preoccupied attachment, separation anxiety schemas, and early maladaptive schemas of dependence/incompetence, abandonment, subjugation, and self-sacrifice organise intimacy. Dimensional analyses of DPD criteria support related but separable attachment and dependent-behaviour clusters — useful for formulation targets beyond a single label.[1][4]
Clinical presentation
Core picture. Patients struggle to decide everyday matters without advice; ask partners or parents to manage finances, health, and housing; avoid disagreement; feel panicked alone; and may move quickly into a new relationship after a breakup. MSE: deferential manner, apologetic disagreement, catastrophic language about independence, idealisation of potential caretakers (including clinicians). Insight into the cost of dependence may coexist with terror of autonomy.[1][3]
Occupational presentation. Under-functioning relative to ability when unsupervised, excessive checking with supervisors, career choices that preserve a caretaker relationship, and paralysis when expected to initiate projects.[1]
Crisis presentation. After separation, bereavement, or threatened abandonment, comorbid major depression and suicidal ideation can escalate rapidly. Dependency and related traits have been linked to elevated suicidality risk in clinical samples with addictive disorders — treat the risk, not the stereotype of “attention-seeking.” Assess for intimate partner violence and exploitation of submissiveness.[13][14]
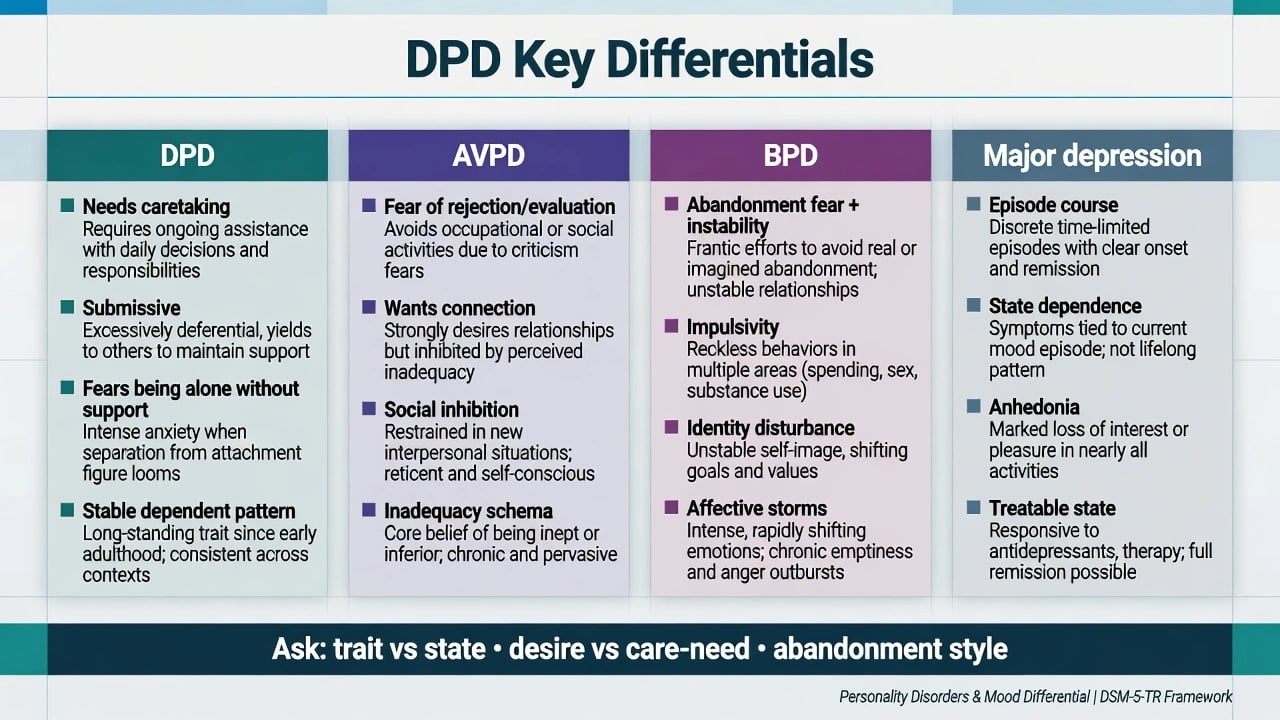
Differential diagnosis
DPD vs AVPD
- DPD: needs others to take responsibility; fears being alone without care
- AVPD: wants connection but fears criticism/rejection/evaluation
- DPD may cling; AVPD often avoids intimacy
- Both Cluster C — dual traits possible
DPD vs BPD
- DPD: more stable submissive dependent pattern
- BPD: affective instability, impulsivity, identity disturbance, self-harm patterns
- Both fear abandonment — ask how abandonment is managed
- Do not collapse every clingy crisis into BPD
DPD vs depression
- MDD: state withdrawal, anhedonia, often episodic
- DPD: lifelong pattern from early adulthood
- Depression can amplify dependence — treat both
- Suicide risk rises when they co-occur after loss
DPD vs culture
- Collectivist interdependence is not pathology
- DPD: pervasive incompetence schema and impairment
- Ask functional cost and distress
- Avoid ethnocentric over-diagnosis
Other essential discriminators. Separation anxiety disorder (anxiety-disorder frame; can co-occur across lifespan). Agoraphobia (fear of situations rather than interpersonal caretaking need). Histrionic PD (attention-seeking theatricality more than submissive care-need). Substance-related dependence is not personality dependence. Late-onset organic personality change (TBI, frontotemporal, endocrine). Always place mood, trauma, and safeguarding on the board.[1][3]
Clinical and bedside assessment
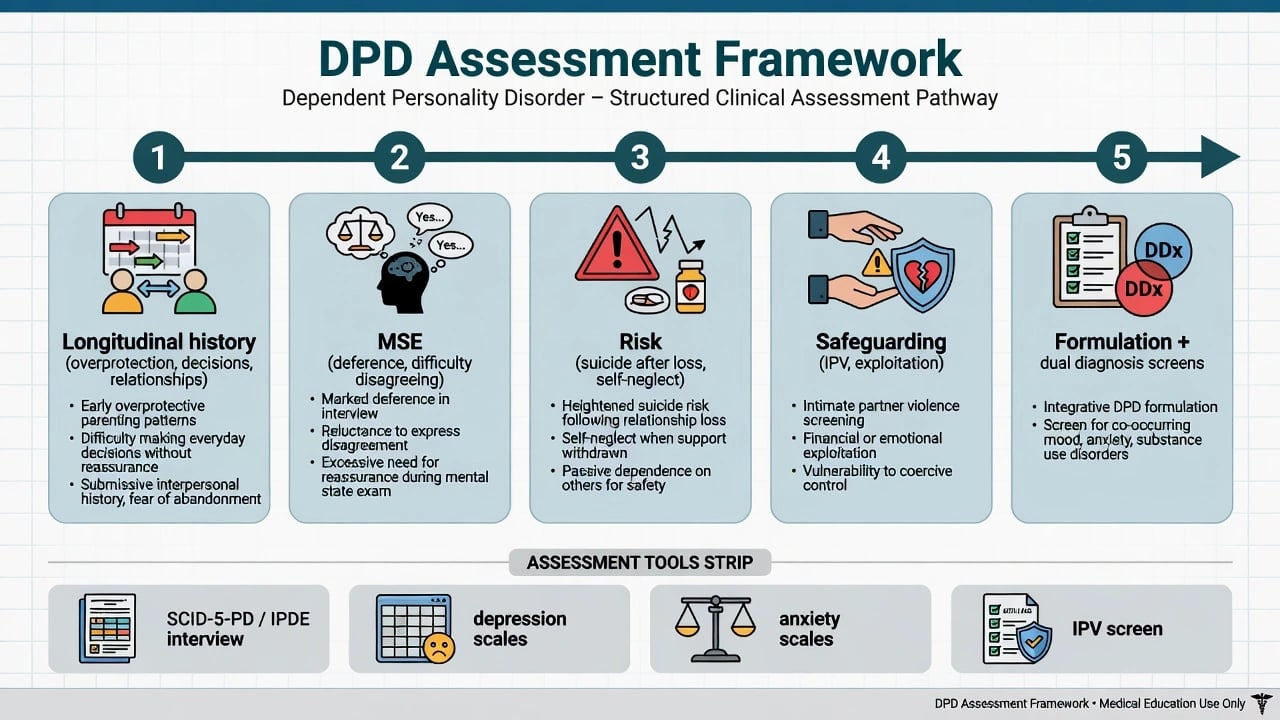
History structure. Developmental overprotection, criticism, or loss; decision-making across life domains; relationship chronology including urgent re-partnering; occupational autonomy; substance use; prior therapy; what the patient wants help with today (often depression or a crisis after loss, not “personality”). Obtain collateral when minimisation or caretaker control limits the history.[1][3]
MSE focus. Rapport (deferential, idealising), affect anxiety, thought content (incapacity alone), insight, judgement about staying in unsafe relationships, and alliance quality — watch for early recruitment of the clinician as permanent caretaker.[1]
Risk. Suicide and self-harm risk rise with comorbid depression and after relationship loss. Assess isolation, self-neglect, access to means, and inability to manage basic needs alone. Capacity is decision-specific. Safeguarding is mandatory when submissiveness is exploited (IPV, financial abuse, coercive control).[13][14]
Tools (conceptual). SCID-5-PD / IPDE for categorical PD diagnosis; depression and anxiety rating scales; IPV screens. Tools support — they do not replace — clinical diagnosis.[1]
Investigations
DPD has no laboratory gold standard. Investigate to exclude mimics and prepare for medication when used: TSH, FBC, U&E, LFT, glucose/lipids, pregnancy test when relevant, urine drug screen when substances may explain behaviour, ECG when cardiac risk or QTc-risk drugs are planned. Neuroimaging or EEG only when late-onset change, focal neurology, seizures, or cognitive decline fire. Screen systematically for major depression, anxiety disorders, other PD traits, substance use, and IPV because they change the map more than the DPD label alone.[1][15]
Management — acute / emergency
Acute principles. Validate fear of being alone without care without becoming the permanent substitute partner. Do not make every decision for the patient in crisis if collaborative micro-choices are safe. Assess IPV and exploitation. Use jurisdiction-specific Mental Health Act principles when statutory criteria are met; do not invent section numbers.[1][14]
Management — definitive and stepwise
Psychotherapy first-line
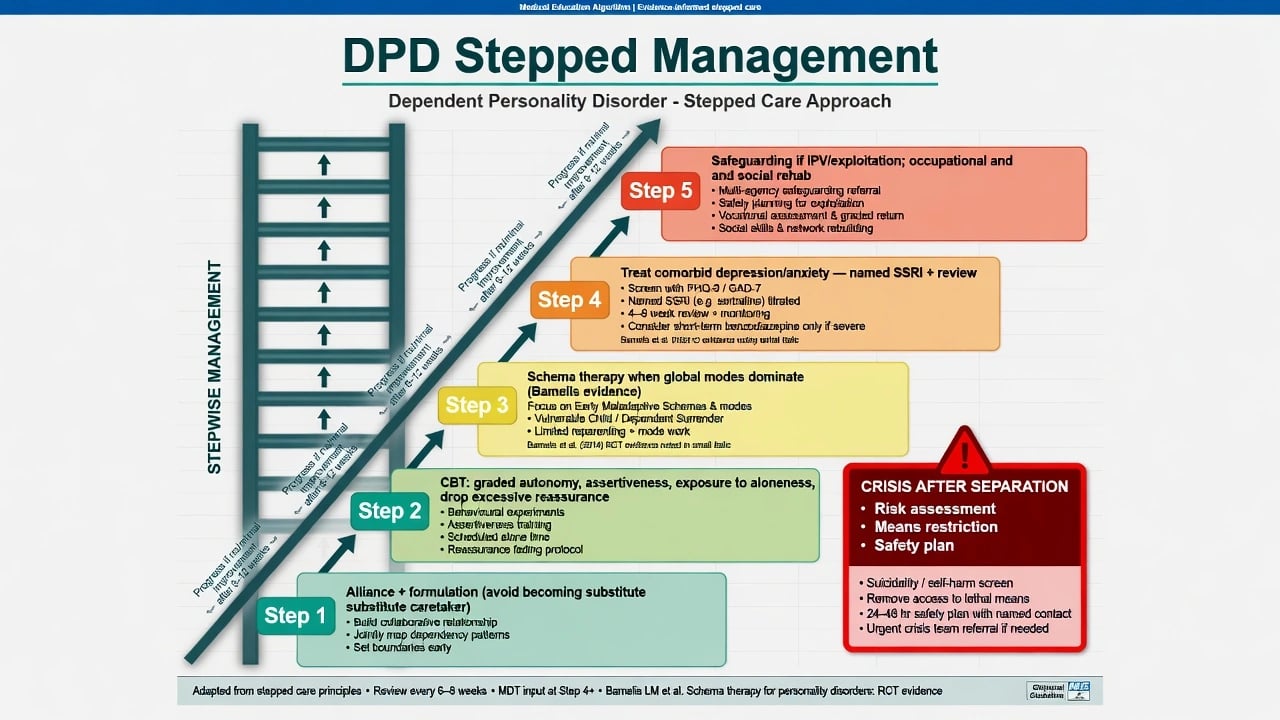
Structured psychological treatment that builds autonomy while preserving alliance is the core of definitive care. Reviews of DPD emphasise that dependency is under-researched relative to its clinical importance, but cognitive-behavioural and schema-focused approaches are the most examinable evidence-informed options, drawing on broader PD psychotherapy trials.[1][10][12]
CBT ingredients examiners expect by name. Collaborative formulation of helplessness and abandonment fears; hierarchy of independent decisions and brief aloneness exposures; behavioural experiments testing “I cannot cope alone”; assertiveness and disagreement practice; reduction of excessive reassurance-seeking; graded responsibility for finances, appointments, and work tasks; relapse planning for post-loss crises. Family work when enmeshment maintains dependence — without shaming cultural care roles.[1][2][3]
Schema therapy. When global dependence/incompetence and abandonment modes dominate, schema therapy targets early maladaptive schemas and modes. A multicentre RCT of schema therapy for personality disorders (Bamelis and colleagues) demonstrated clinical effectiveness versus clarification-oriented psychotherapy and treatment as usual in a mixed PD sample that included substantial Cluster C pathology — the named trial beyond BPD-only evidence. Commentary has specifically highlighted schema therapy as effective for avoidant, dependent, and obsessive-compulsive personality disorders within that evidence programme. Economic evaluation supported its value in that research stream.[10][11][12]
Alliance stance. Warmth, predictability, and explicit autonomy goals beat rescuer collusion. Predict and repair the rupture when the patient experiences therapy boundaries as abandonment. Dropout and crisis re-presentations are often formulation problems, not “manipulation.”[1][2]
Pharmacotherapy — comorbidity only
No medication treats DPD as a whole. Drugs are for comorbid major depression, anxiety disorders, or other Axis I targets, with measurement and review dates. Network meta-analysis of antidepressants for adult major depression supports multiple SSRIs as acceptable first-line options when depression is present; choose one agent and pair with psychotherapy rather than using pills as a permanent substitute for autonomy work.[15]
Named adult example when an examiner forces a plan (individualise; check local product information). For comorbid major depression without bipolarity: sertraline 50 mg orally once daily, review in 1–2 weeks for activation, anxiety increase and suicidality (especially under age 25), titrate toward a therapeutic range commonly 50–150 mg daily as tolerated, with a response review at 6–12 weeks at an adequate dose and limited early supply if overdose risk is elevated after a relationship crisis. Counsel sexual side effects and discontinuation syndrome.[15]
Avoid. Chronic benzodiazepines as the only treatment of separation anxiety features; polypharmacy stacking without targets; antipsychotics for “personality” in the absence of psychotic phenomena or another indication; making every prescribing decision for the patient without shared decision-making practice.[1][15]
Care system and disposition
Most patients are managed in outpatient psychotherapy and general adult pathways. Step up for acute suicide risk, severe depression, or self-neglect after loss. Step down when independent decision-making generalises and relationships become less exploitative. Occupational rehabilitation and graded living-skills work are part of recovery.[1][10]
Australian and New Zealand practice emphasises stepped mental health care, access to psychological therapies where available, trauma-informed engagement, and culturally safe practice. Local Mental Health Act provisions govern involuntary care — name least-restrictive principles, not invented foreign section numbers. Coordinate with primary care for SSRI prescribing and monitoring; use local IPV and family-violence pathways when exploitation is identified.[1][14]
Specific subtypes and scenarios
DPD + major depression after relationship breakdown. Treat depression and suicide risk aggressively; do not dismiss suicidality as “attention-seeking.” Sequence risk containment, antidepressant when indicated, and resume autonomy-focused psychotherapy when affective load allows.[1][13][15]
DPD with IPV / exploitation. Dual plan: safety and safeguarding first; therapy that does not pressure premature confrontation without safety; document capacity and coercive control. Dependency is a recognised clinical risk context for IPV dynamics.[14]
DPD vs BPD abandonment crisis. Use longitudinal pattern: affective storms, identity disturbance, and self-harm repertoire point toward BPD spectrum; stable submissive care-seeking without those features supports DPD — dual diagnosis is possible when both met.[1]
DPD + AVPD (Cluster C mixture). Both can co-occur; formulation must address evaluation fear and caretaking need separately in the hierarchy.[1]
Cultural interdependence versus DPD. Family-inclusive care in collectivist contexts is not automatically pathology; require pervasive incompetence schema and impairment.[1]
Iatrogenic service dependence. Repeated crisis admissions that make the service the caretaker without autonomy goals reinforce the disorder — plan micro-decisions, crisis alternatives, and planned step-down.[1]
Complications and pitfalls
Classic pitfalls: calling DPD “just clingy” and excluding from services; missing depression, IPV, or BPD; becoming the permanent decision-maker; polypharmacy without targets; diagnosing PD from a single crisis interview; pathologising cultural interdependence; ignoring post-separation suicide risk; inventing Mental Health Act section numbers.[1][13][14]
Prognosis and disposition
Without treatment, dependent patterns are relatively stable and disabling in relationships and work. With structured CBT or schema-focused work and treatment of comorbidity, meaningful improvement is expected — DPD is not a life sentence of helplessness. Functional recovery (independent living, safer intimacy, occupational autonomy) may lag symptom reduction and needs explicit rehabilitation goals. Disposition is usually outpatient; reassess after losses and major transitions.[1][10][12]
Special populations
Youth. Distinguish emerging dependent patterns from normal developmental attachment. Avoid casual lifelong PD labels without longitudinal evidence. Early intervention for separation anxiety and family overcontrol may reduce entrenchment.[1]
Older adults. Lifelong DPD may decompensate after death of a caregiver partner. New late-life dependence is organic/mood until proven otherwise.[1]
Pregnancy and parenting. Support maternal autonomy and safety; screen IPV carefully; treat depression with appropriate agents and monitoring; minimise unnecessary polypharmacy.[14][15]
Cultural formulation. Collectivist kinship care, respect hierarchies, or help-seeking after discrimination is not automatically DPD. In ANZ practice, Indigenous cultural safety and family-inclusive care are competencies — do not pathologise kinship support systems.[1]
Evidence, guidelines and controversies
Phenomenology and models: Disney 2013 critical review; Bornstein interactionist and developmental dependency work; Gude dimensionality of DPD criteria.[1][2][3][4]
Epidemiology and risk: NESARC and NCS-R personality disorder prevalence; Torgersen community sample; Winsper global PD meta-analysis; Loas dependency–suicidality; Kane and Bornstein on dependency and IPV risk.[6][7][8][9][13][14]
Genetics: Gjerde heritability of avoidant and dependent PD.[5]
Treatment anchors: Bamelis schema therapy RCT and economic evaluation; Hopwood commentary on schema therapy for AVPD/DPD/OCPD; Cipriani network meta-analysis for antidepressant options in adult major depression comorbidity; ICD-11 dimensional framing updates.[10][11][12][15][16]
Mature controversies. Whether DPD should remain a categorical diagnosis versus ICD-11 severity-plus-traits only; gender bias in diagnosis; how actively to push autonomy without re-traumatising abandonment fear; and how to resource schema therapy outside specialist clinics.[1][16]
Exam pearls
DEPEND — viva checklist
DEPEND
≥5 of 8 DSM features after general PD criteria (not 4)
Excessive need to be cared for — core theme
Post-separation suicide risk and IPV screens
Exclude AVPD (evaluation fear) and BPD (instability)
No drug cures PD; SSRI for comorbid depression/anxiety
Do graded autonomy CBT / schema therapy — not rescuer collusion
60-second oral summary
DPD is DSM ≥5/8 excessive need to be cared for with submissive clinging and separation fears after general PD criteria. Relatively uncommon in community surveys (~0.5% NESARC) but high clinical impact via depression, post-loss suicide risk, and exploitation. Discriminate AVPD (evaluation fear), BPD (instability), and cultural interdependence. Treat with alliance-preserving CBT for graded autonomy and assertiveness; use schema therapy when global modes dominate (Bamelis RCT). Medicate comorbid depression/anxiety with a named SSRI (e.g. sertraline 50 mg titrated) plus review — not polypharmacy as personality cure. Always assess IPV and do not become the permanent caretaker.[1][2][6][10][14][15]
References
- [1]Disney KL Dependent personality disorder: a critical review Clin Psychol Rev, 2013.PMID 24185092
- [2]Bornstein RF From dysfunction to adaptation: an interactionist model of dependency J Pers, 2012.PMID 22458867
- [3]Bornstein RF The dependent personality: developmental, social, and clinical perspectives Psychol Bull, 1992.PMID 1529038
- [4]Gude T, Hoffart A, Hedley L, Rø Ø The dimensionality of dependent personality disorder J Pers Disord, 2004.PMID 15615670
- [5]Gjerde LC, Czajkowski N, Røysamb E, Orstavik RE, et al. The heritability of avoidant and dependent personality disorder assessed by personal interview and questionnaire Acta Psychiatr Scand, 2012.PMID 22486635
- [6]Grant BF, Hasin DS, Stinson FS, Dawson DA, et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions J Clin Psychiatry, 2004.PMID 15291684
- [7]Lenzenweger MF, Lane MC, Loranger AW, Kessler RC DSM-IV personality disorders in the National Comorbidity Survey Replication Biol Psychiatry, 2007.PMID 17217923
- [8]Torgersen S, Kringlen E, Cramer V The prevalence of personality disorders in a community sample Arch Gen Psychiatry, 2001.PMID 11386989
- [9]Winsper C, Bilgin A, Thompson A, Marwaha S, et al. The prevalence of personality disorders in the community: a global systematic review and meta-analysis Br J Psychiatry, 2020.PMID 31298170
- [10]Bamelis LL, Evers SM, Spinhoven P, Arntz A Results of a multicenter randomized controlled trial of the clinical effectiveness of schema therapy for personality disorders Am J Psychiatry, 2014.PMID 24322378
- [11]Bamelis LL, Arntz A, Wetzelaer P, Verdoorn R, et al. Economic evaluation of schema therapy and clarification-oriented psychotherapy for personality disorders: a multicenter, randomized controlled trial J Clin Psychiatry, 2015.PMID 26579561
- [12]Hopwood CJ, Thomas KM Schema therapy is an effective treatment for avoidant, dependent and obsessive-compulsive personality disorders Evid Based Ment Health, 2014.PMID 25009174
- [13]Loas G, Guilbaud O, Perez-Diaz F, Verrier A, et al. Dependency and suicidality in addictive disorders Psychiatry Res, 2005.PMID 16233920
- [14]Kane FA, Bornstein RF Beyond passivity: Dependency as a risk factor for intimate partner violence J Nerv Ment Dis, 2016.PMID 26542755
- [15]Cipriani A, Furukawa TA, Salanti G, Chaimani A, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis Lancet, 2018.PMID 29477251
- [16]Kim YR, Tyrer P, Mulder R, King JD, et al. ICD-11 classification of personality disorder: there is no other way forward Br J Psychiatry, 2026.PMID 41906979