Psych · General adult psychiatry — dissociative disorders
Depersonalization/derealization disorder
Also known as DPDR · DPD · Depersonalisation disorder · Derealisation disorder · Depersonalisation-derealisation disorder · Feeling unreal · Cambridge Depersonalization Scale · CDS
Exam-exhaustive fellowship reference on depersonalisation/derealisation disorder — DSM-5-TR/ICD-11 criteria with intact reality testing; 1–2% community prevalence; corticolimbic disconnection and Hunter CBT model; CDS/DES assessment; differentials from psychosis, panic, PTSD and cannabis; CBT open-trial evidence; fluoxetine RCT negative for core symptoms; lamotrigine mono vs add-on nuance; naltrexone open data. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
DPDR is a high-yield leaf within the dissociative disorders atlas. Examiners test phenomenology ("as if" language), the psychosis discriminator (reality testing), primary versus secondary symptoms, named instruments (CDS, DES), and honest appraisal of a thin pharmacologic evidence base against a usable CBT model.[1][2][6][7]
Overview and definition
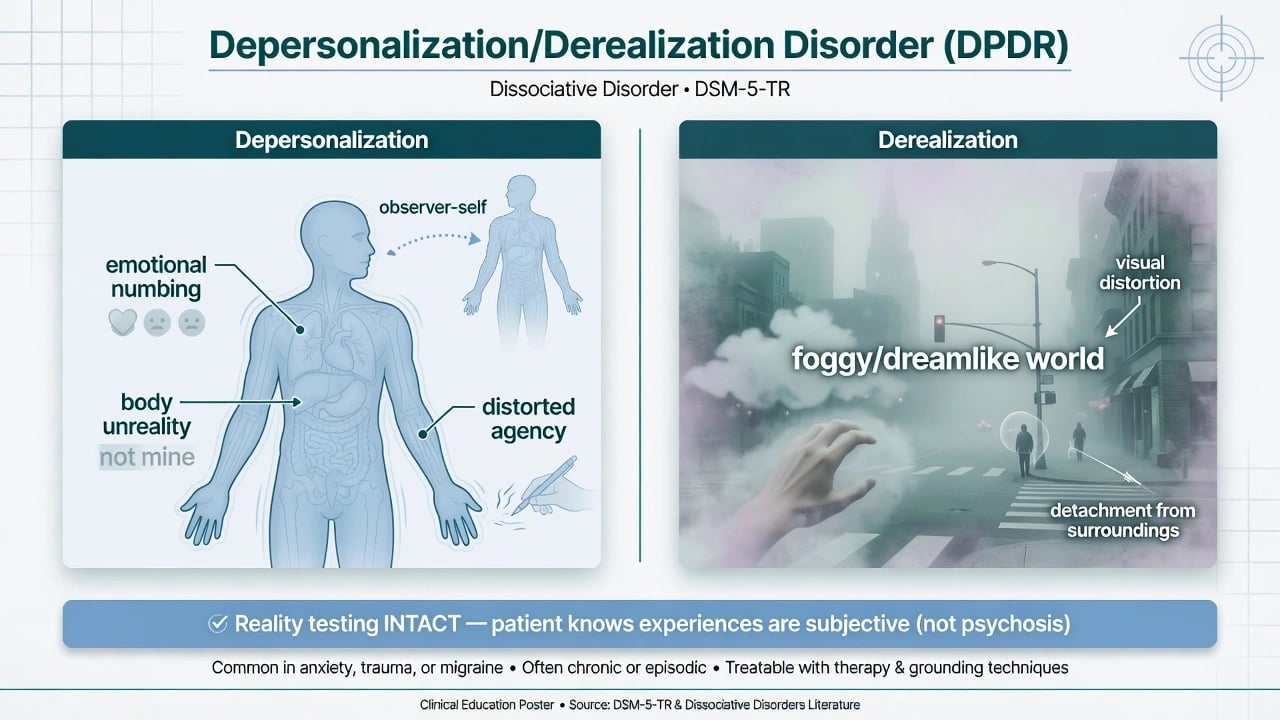
Depersonalisation is the experience of unreality, detachment, or being an outside observer with respect to one's thoughts, feelings, sensations, body, or actions (for example perceptual alterations, distorted sense of time, unreal or absent self, emotional or physical numbing).[1][10]
Derealisation is unreality or detachment with respect to surroundings (individuals or objects experienced as unreal, dreamlike, foggy, lifeless, or visually distorted).[1][2]
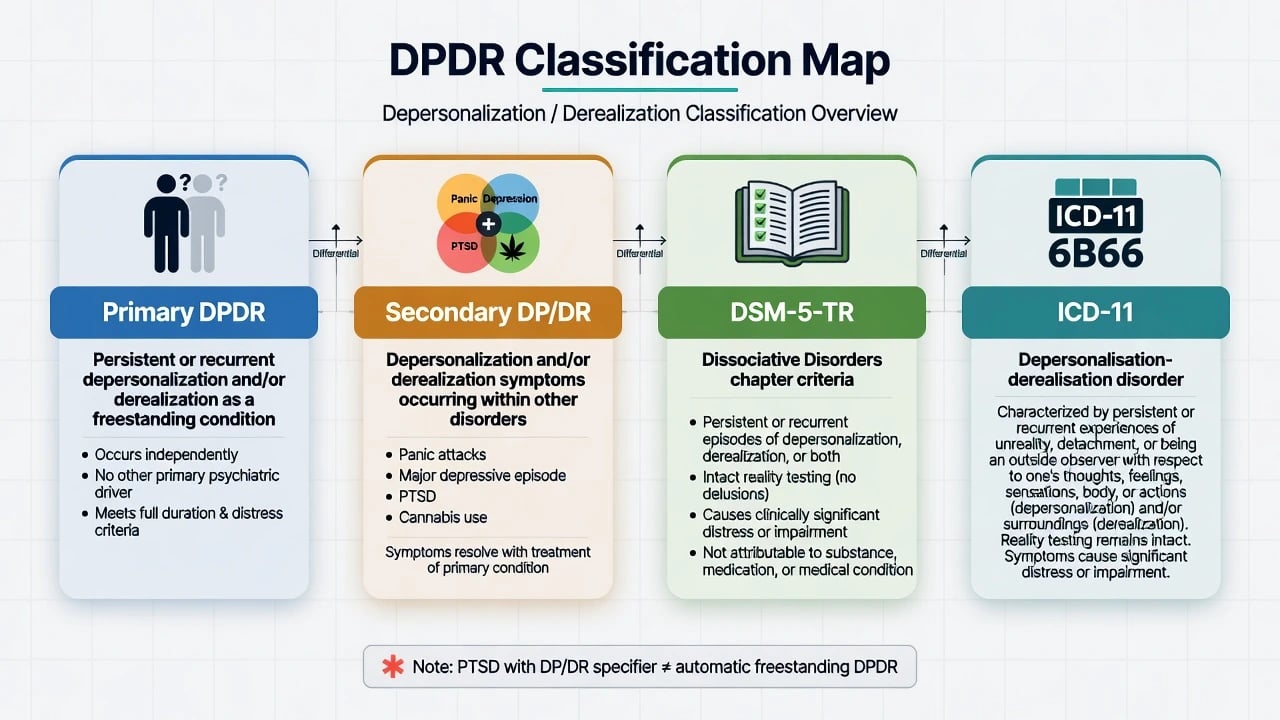
DPDR as a disorder requires that experiences are persistent or recurrent, cause clinically significant distress or impairment, and that during the depersonalisation or derealisation experiences, reality testing remains intact — the patient knows the experience is subjective, not a delusional claim that the external world has objectively changed into another planet or that the self has been replaced by an impostor in a psychotic sense.[1][2]
Symptoms are not attributable to physiological effects of a substance (for example cannabis) or another medical condition (for example seizures), and are not better explained by another mental disorder such as schizophrenia, panic disorder, major depression, acute stress disorder, PTSD, or another dissociative disorder.[1]
Clinical series emphasise long mean duration before specialist recognition, high distress, and frequent anxiety/depressive comorbidity — Simeon's consecutive 117-case update remains a classic clinical portrait for viva depth.[3]
Classification
DSM-5-TR places DPDR among the dissociative disorders with DID, dissociative amnesia, and other specified/unspecified dissociative disorders. ICD-11 retains depersonalisation-derealisation disorder as a named entity within dissociative disorders teaching maps.[1]
Primary versus secondary. Primary DPDR is freestanding. Secondary DP/DR symptoms commonly accompany panic attacks, severe depression, PTSD (including the dissociative subtype specifier), and substance intoxication — diagnose freestanding DPDR only when criteria are met and not better explained by the other condition.[1][4][15]
Primary DPDR
- Persistent/recurrent DP and/or DR
- Intact reality testing
- Distress/impairment required
- Not better explained by other disorder
Panic-linked DP/DR
- Often limited to attacks
- Fear of dying/losing control central
- Treat panic pathway first
- May leave residual DPDR
PTSD dissociative subtype
- Full PTSD plus DP/DR
- Emotion overmodulation model
- Trauma-focused care with pacing
- Not automatic freestanding DPDR
Psychosis mislabel trap
- Delusional conviction vs 'as if'
- Thought disorder/hallucinations absent in pure DPDR
- Insight usually preserved
- Avoid antipsychotic-only pathway
Epidemiology and risk factors
Headline epidemiology (exam numbers)
Hunter and colleagues' systematic review remains the classic epidemiology anchor: transient DP/DR symptoms are common in the general population and at traumatic moments, whereas population surveys using diagnostic interviews place clinically significant DP/DR roughly in the 1–2% range.[4] Yang and colleagues' later systematic review synthesises general-population rates for depersonalisation-derealisation disorder around 1%, with higher rates in clinical samples and a signal toward adolescents/young adults.[5]
Precipitants and risk context. Severe stress, panic, cannabis and other substances, and trauma exposure are frequently cited precipitants in clinical series; comorbidity with anxiety and depression is high; functional impairment can be severe despite preserved orientation.[2][3][4] DES meta-analysis work shows dissociation scores elevated across many psychiatric disorders — elevated DES is not DPDR-specific diagnosis.[18]
Pathophysiology and maintaining models
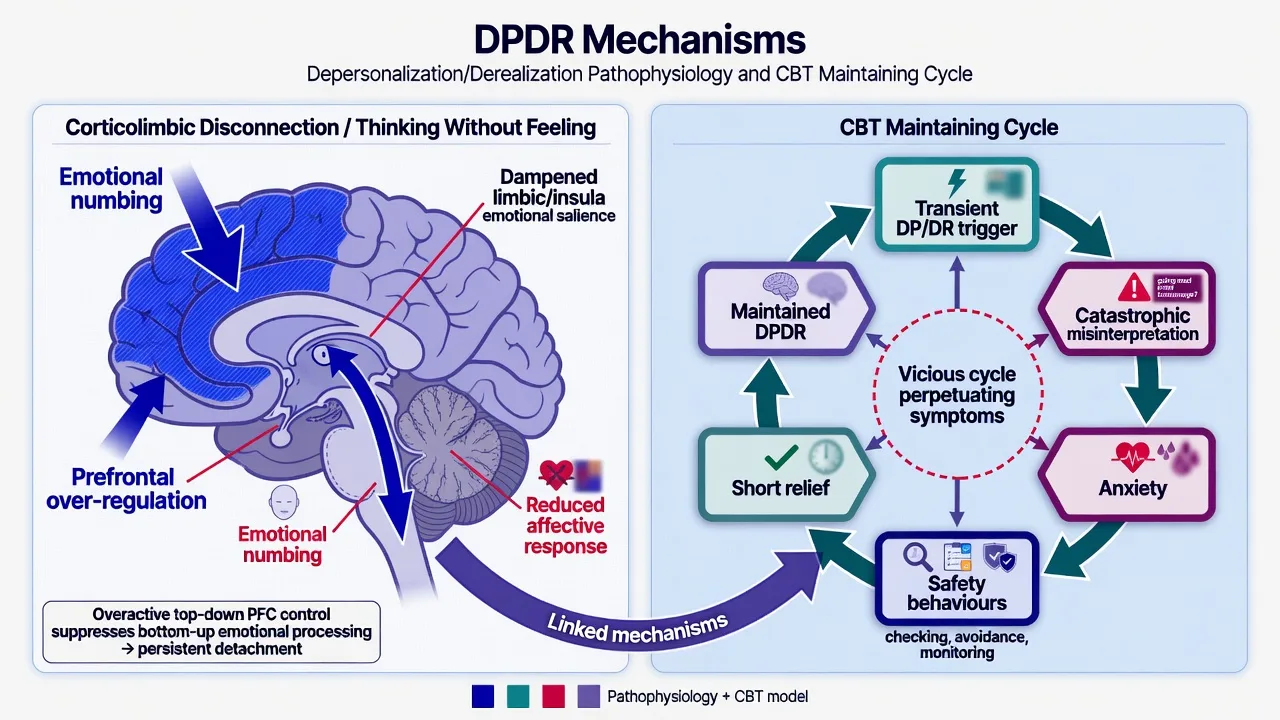
Neurobiology (viva depth, not a bedside test). Functional imaging work including Phillips and colleagues' "thinking without feeling" framing supports reduced emotional responsiveness with altered limbic-related processing and relatively increased regulatory prefrontal activity — a corticolimbic disconnection / overmodulation pattern consistent with subjective emotional numbing.[9] Sierra and David synthesise depersonalisation as a selective impairment of self-awareness featuring disembodiment and subjective emotional numbing with intact reality testing.[10]
CBT maintaining model (Hunter). Transient DP/DR experiences are common under stress. In vulnerable individuals, catastrophic misinterpretation (for example "I am going mad," "my brain is permanently damaged," "I will never return") generates anxiety; symptom monitoring, avoidance, and safety behaviours briefly reduce fear but maintain selective attention and the chronic disorder loop.[7] This model is the backbone of specialised CBT and of CASC psychoeducation scripts.[7][8]
Pharmacologic hypotheses. Glutamate-release reduction motivated lamotrigine trials; endogenous opioid dysregulation motivated naltrexone open work — both are hypothesis-driven and must be taught with evidence quality caveats, not as proven disease mechanisms.[12][13][14]
Clinical presentation
Patients use "as if" language: watching themselves from outside; rubbery or detached limbs; muffled sound; foggy or two-dimensional surroundings; emotional deadness without primary delusional explanation. Fear of permanent madness or neurological ruin is common and feeds the CBT cycle.[2][3][7]
MSE. Orientation usually preserved; thought form not primarily disordered; reality testing intact for the unreality experiences; affect may appear restricted or anxious; insight typically good that experiences are subjective; risk must still be assessed carefully because despair and comorbid depression elevate suicide concern.[2][3]
Course patterns. Continuous versus episodic; abrupt onset after panic or cannabis versus insidious; long duration before correct labelling is classic in specialist series.[3]
Differential diagnosis
Key discriminators for exam answers:[1][2]
- Primary psychotic disorder: delusional conviction that self/world has truly transformed; thought disorder; hallucinations as primary process — versus "as if" unreality with intact insight in DPDR.[1][2]
- Panic disorder: DP/DR confined to attacks versus persistent freestanding symptoms between attacks.[4]
- MDD: anhedonia and psychomotor change without unreality phenomenology as the core complaint.[2]
- PTSD / dissociative subtype: full trauma syndrome with DP/DR specifier; emotion overmodulation model informs care — not automatic freestanding DPDR.[15]
- Substance-induced: temporal link to cannabis, ketamine, hallucinogens; reassess after washout.[3][4]
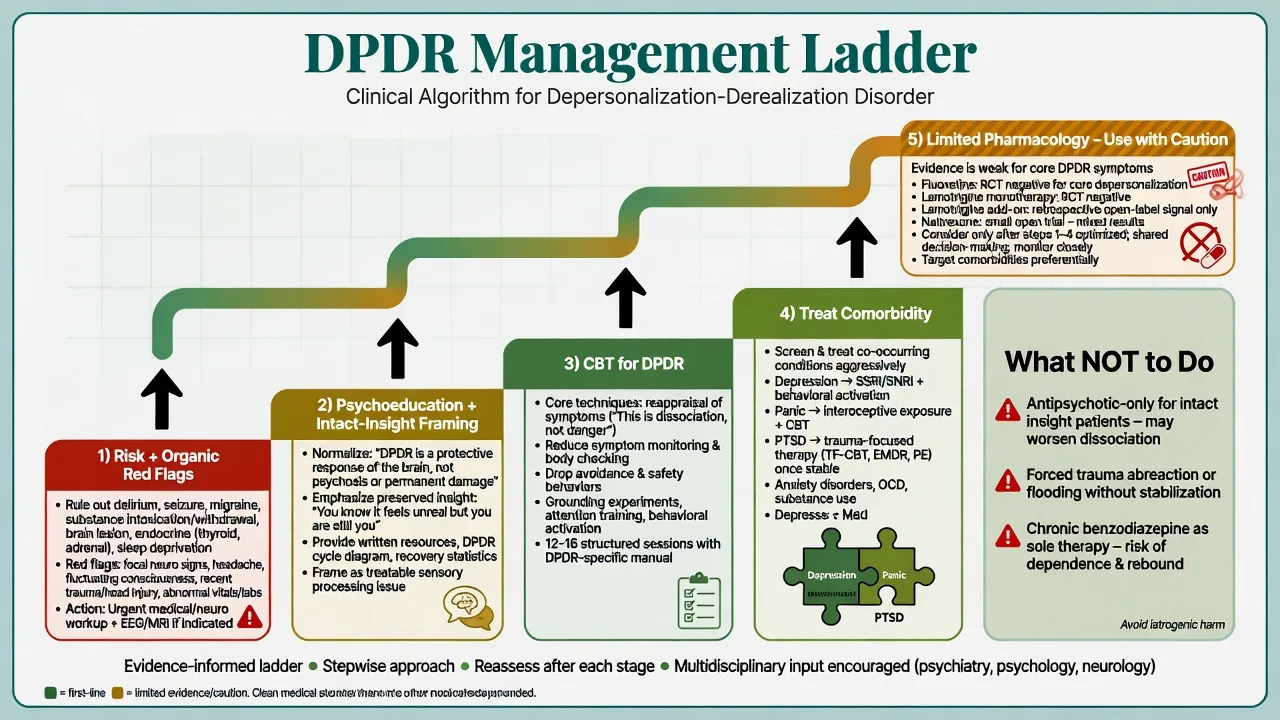
- Organic: TLE/partial seizures, migraine, encephalitis, TBI, vestibular disease, severe sleep deprivation — especially late first onset or neurological clues.[2]
- Other dissociative disorders: identity discontinuity and amnesia point toward DID/OSDD rather than pure DPDR.[1][17]
Clinical and bedside assessment
History structure. Onset (age, abrupt vs insidious); continuous versus episodic; triggers (panic, cannabis, sleep loss, interpersonal stress); hours per day spent monitoring unreality; catastrophic appraisals; safety behaviours and avoidance; prior labels (often "anxiety" or incorrectly "psychosis"); trauma history paced and consented; functional impact.[2][3][7]
Risk. Structured suicide assessment is mandatory. Chronic unreality plus depression and hopelessness about recovery are high-yield risk drivers, not "only soft neurotic symptoms."[2][3]
Scales used in DPDR assessment:[6][16][17]
- Cambridge Depersonalization Scale (CDS): frequency and duration of depersonalisation symptoms over the last six months — specialist severity tracking tool.[6]
- Dissociative Experiences Scale (DES): broad dissociation screen; elevated scores warrant fuller assessment but do not alone equal DPDR diagnosis.[16][18]
- SCID-D / SCID-D-R: structured interview covering amnesia, depersonalisation, derealisation, identity confusion and alteration when the differential includes broader dissociative disorders.[17]
Investigations
There is no diagnostic MRI, EEG signature, or blood test that proves primary DPDR. Investigate to exclude organic mimics and to prepare safely for any medication used for comorbidity: TSH, B12/folate, basic metabolic panel as indicated; urine drug screen when substance contribution is plausible; ECG before agents with cardiac risk; EEG/neuroimaging when seizure clues, focal neurology, encephalitic red flags, or unexplained late onset appear.[2][9] Serial CDS or DES and depression/anxiety scales support measurement-based care.[6][16]
Management — acute risk and resuscitation
Stabilise medically if intoxicated or organically unstable. In crisis, use grounding and reorientation, reduce sensory overload and compulsive symptom-checking, and deliver early psychoeducation that symptoms are recognised and non-psychotic when reality testing is intact. Treat acute severe depression or panic as priority pathways when they drive risk.[2][7]
Management — definitive and stepwise
Psychoeducation and engagement (do this first)
Explain the "as if" nature of symptoms, intact reality testing, and the CBT cycle in plain language. Validate distress without colluding with the belief that the brain is irreversibly destroyed. Name that transient DP/DR is common under stress and that chronic disorder is maintainable by monitoring and catastrophic meanings.[7][8]
First-line psychological treatment — CBT for DPDR
Specialised CBT includes: reappraisal of catastrophic meanings of DP/DR; reduction of safety behaviours, avoidance, and continuous symptom monitoring; behavioural experiments; attention training away from unreality scanning; anxiety and depression strategies as needed.[7][8]
Hunter and colleagues' open study of individual CBT in 21 patients with depersonalisation disorder found significant improvements in patient-defined DP/DR severity and standardised dissociation, depression, anxiety, and functioning measures at post-treatment and six-month follow-up — examinable as the best known dedicated psychological evidence, while remaining non-RCT.[8]
Pharmacotherapy — limited evidence, treat comorbidity
Honest evidence map candidates must recite:[11][12][13][14]
- Fluoxetine RCT (Simeon 2004): randomised controlled trial found fluoxetine was not efficacious for depersonalisation disorder as a core treatment, despite common clinical use of SSRIs — use SSRIs primarily for comorbid depression/anxiety, not as a promised core-DPDR cure.[11]
- Lamotrigine monotherapy small crossover RCT (Sierra 2003): placebo-controlled crossover did not show significant advantage of lamotrigine alone.[12]
- Lamotrigine add-on retrospective series (Sierra 2006): among 32 cases, a substantial subset experienced clinically meaningful reduction when lamotrigine was combined with antidepressant medication — signal only, not a first-line universal mandate.[13]
- Naltrexone open trial (Simeon 2005): prospective open treatment (dose strategies up to 100 mg/day then higher-dose cohort up to 250 mg/day in the reported design; mean dose around 120 mg/day in the series) with average ~30% symptom reduction on dissociation scales — promising but uncontrolled.[14]
If lamotrigine is considered as a specialist off-label add-on after comorbidity treatment and CBT framing, follow slow rash-risk titration as for psychiatric use of lamotrigine (teaching start often 25 mg orally daily with gradual increases per product information), counsel on serious rash including SJS/TEN, and frame as experimental/adjunctive rather than proven first-line monotherapy.[12][13]
What not to do. Antipsychotic-only pathways for intact-insight pure DPDR; chronic high-dose benzodiazepines as sole strategy; aggressive memory recovery or abreactive trauma work without stabilisation; therapeutic nihilism that blocks CBT access.[2][7][11]
Subtypes and high-yield scenarios
Cannabis-precipitated DPDR. Classic stem: first intense unreality after cannabis, then weeks–months of persistent symptoms with catastrophic fear of brain damage — psychoeducation, stop cannabis, CBT for appraisals, reassess diagnosis after abstinence.[3][4][7]
Panic-limited versus freestanding. If DP/DR occurs only during panic attacks, prioritise panic disorder treatment; if continuous between attacks, freestanding DPDR criteria may be met.[4]
PTSD interface. When full PTSD is present with DP/DR, use trauma-informed care and the dissociative subtype concept rather than forcing a pure DPDR label.[15]
Adolescent onset. Peak window; school avoidance; social media health searching that feeds catastrophic appraisals — family-inclusive psychoeducation and CBT framing.[3][5][7]
Complications and pitfalls
Misdiagnosis as schizophrenia; missing seizure/organic mimics; iatrogenic reinforcement via endless unfocused "brain damage" investigations without addressing appraisals; under-treating depression and suicide risk; overselling SSRI or lamotrigine as definitive cures; colluding with perpetual online DPDR checking forums that maintain monitoring.[2][7][11][12]
Prognosis and disposition
Untreated course is often chronic or fluctuating; long duration before correct diagnosis is common in specialist series.[3] Prognosis improves with early accurate psychoeducation, CBT access, cannabis cessation, and treatment of panic/depression. Disposition is usually outpatient specialised psychological therapy with measurement-based follow-up; step up for suicide risk or severe functional collapse.[2][8]
Special populations
Youth. Peak onset; developmental language for unreality; cannabis risk counselling; avoid premature chronic identity as "broken brain."[3][5]
Older adults. Late first onset raises organic threshold (seizure, medication effects, neurodegeneration).[2]
Perinatal. Treat comorbid depression/anxiety with collaborative obstetric–psychiatry risk–benefit discussion; CBT principles remain core for DPDR appraisals.[2][8]
Cultural formulation. Soul loss or spirit-detachment idioms require cultural humility; still assess reality testing, impairment, and risk without automatic pathologising of culturally sanctioned experiences.[1]
Regional practice deltas
ANZ (FRANZCP): Emphasise formulation, risk, intact-insight differential from FEP pathways, and honest evidence limits for drugs; trauma-informed pacing if trauma history present. UK (MRCPsych): CASC psychoeducation stations and Hunter CBT model are high-yield; CDS as named instrument. US (ABPN): DSM-5-TR criteria wording, Simeon trial names, and primary vs secondary DPDR. MD/DNB/NEET-SS: Phenomenology, psychosis differential, precipitants (cannabis/panic), and treatment evidence hierarchy.[1][2][7][11]
Evidence and guidelines — named anchors
Deploy under pressure: Spiegel (DSM-5 dissociative nosology); Simeon overview and 117-case series; Hunter epidemiology and CBT model/open trial; Yang prevalence SR; Sierra and Berrios CDS; Phillips thinking without feeling; Sierra and David self-awareness; Simeon fluoxetine RCT; Sierra lamotrigine mono RCT and add-on retrospective; Simeon naltrexone open trial; Lanius PTSD dissociative subtype; Bernstein DES; Steinberg SCID-D; Lyssenko DES meta-analysis.[1][2][3][4][5][6][7][8][9][11][15]
There is no single RANZCP or NICE "DPDR-only" clinical practice guideline equivalent to major mood CPGs. Exam answers rest on phenomenology + named trial evidence + CBT model + comorbidity guidelines for anxiety/depression when relevant.[2][8][11]
Exam pearls
Classic stems: cannabis-then-chronic unreality; continuous DP/DR after panic attacks; "brain damage" fear with normal work-up; mislabelled "psychosis" on antipsychotics without thought disorder; adolescent school refusal with foggy world and intact insight.[3][4][7][11]
Landmark names to deploy: Simeon, Hunter, Sierra, Berrios, Phillips, David, Spiegel, Lanius, Yang, Steinberg.[1][2][4][6][7][9][15]
References
- [1]Spiegel D, Lewis-Fernández R, Lanius R, Vermetten E, Simeon D Dissociative disorders in DSM-5 Annu Rev Clin Psychol, 2013.PMID 23394228
- [2]Simeon D Depersonalisation disorder: a contemporary overview CNS Drugs, 2004.PMID 15089102
- [3]Simeon D, Knutelska M, Nelson D, Guralnik O Feeling unreal: a depersonalization disorder update of 117 cases J Clin Psychiatry, 2003.PMID 14628973
- [4]Hunter EC, Sierra M, David AS The epidemiology of depersonalisation and derealisation. A systematic review Soc Psychiatry Psychiatr Epidemiol, 2004.PMID 15022041
- [5]Yang J, Millman LSM, David AS, Hunter ECM The Prevalence of Depersonalization-Derealization Disorder: A Systematic Review J Trauma Dissociation, 2023.PMID 35699456
- [6]Sierra M, Berrios GE The Cambridge Depersonalization Scale: a new instrument for the measurement of depersonalization Psychiatry Res, 2000.PMID 10725532
- [7]Hunter EC, Phillips ML, Chalder T, Sierra M, David AS Depersonalisation disorder: a cognitive-behavioural conceptualisation Behav Res Ther, 2003.PMID 14583413
- [8]Hunter EC, Baker D, Phillips ML, Sierra M, David AS Cognitive-behaviour therapy for depersonalisation disorder: an open study Behav Res Ther, 2005.PMID 16005701
- [9]Phillips ML, Medford N, Senior C, et al. Depersonalization disorder: thinking without feeling Psychiatry Res, 2001.PMID 11756013
- [10]Sierra M, David AS Depersonalization: a selective impairment of self-awareness Conscious Cogn, 2011.PMID 21087873
- [11]Simeon D, Guralnik O, Schmeidler J, Knutelska M Fluoxetine therapy in depersonalisation disorder: randomised controlled trial Br J Psychiatry, 2004.PMID 15231553
- [12]Sierra M, Phillips ML, Ivin G, Krystal J, David AS A placebo-controlled, cross-over trial of lamotrigine in depersonalization disorder J Psychopharmacol, 2003.PMID 12680746
- [13]Sierra M, Baker D, Medford N, Lawrence E, Patel M, Phillips ML, David AS Lamotrigine as an add-on treatment for depersonalization disorder: a retrospective study of 32 cases Clin Neuropharmacol, 2006.PMID 16960469
- [14]Simeon D, Knutelska M An open trial of naltrexone in the treatment of depersonalization disorder J Clin Psychopharmacol, 2005.PMID 15876908
- [15]Lanius RA, Vermetten E, Loewenstein RJ, Brand B, Schmahl C, Bremner JD, Spiegel D Emotion modulation in PTSD: Clinical and neurobiological evidence for a dissociative subtype Am J Psychiatry, 2010.PMID 20360318
- [16]Bernstein EM, Putnam FW Development, reliability, and validity of a dissociation scale J Nerv Ment Dis, 1986.PMID 3783140
- [17]Steinberg M Advances in the clinical assessment of dissociation: the SCID-D-R Bull Menninger Clin, 2000.PMID 10842445
- [18]Lyssenko L, Schmahl C, Bockhacker L, Vonderlin R, Bohus M, Kleindienst N Dissociation in Psychiatric Disorders: A Meta-Analysis of Studies Using the Dissociative Experiences Scale Am J Psychiatry, 2018.PMID 28946763