Psych · General adult psychiatry — dissociative disorders
Dissociative disorders
Also known as Dissociative identity disorder · DID · Multiple personality disorder · Depersonalisation · Derealisation · DPDR · Dissociative amnesia · Dissociative fugue · OSDD
Exam-exhaustive fellowship reference on dissociative disorders — DID with balanced trauma vs sociocognitive evidence, DPDR, dissociative amnesia, DES/SCID-D assessment, differentials from psychosis and BPD, phase-oriented ISSTD care, TOP DD outcomes, risk and iatrogenic pitfalls. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Dissociation is high-yield for FRANZCP MEQs, MRCPsych CASC differential stations, and ABPN-style items because examiners test nosology, the trauma versus sociocognitive debate, discrimination from psychosis, and safe management. This topic is written so a candidate who has read nothing else can defend DID carefully with evidence, describe DPDR and amnesia, and avoid both dismissive nihilism and uncritical certainty.[2][3][4]
Overview and definition
Dissociation refers to a disruption of and/or discontinuity in the normal integration of consciousness, memory, identity, emotion, perception, body representation, motor control, or behaviour. Transient dissociative experiences can occur under extreme stress; dissociative disorders are diagnosed when symptoms are persistent or recurrent, cause distress or impairment, and are not better explained by substance use, another medical condition, or a culturally sanctioned practice.[1]
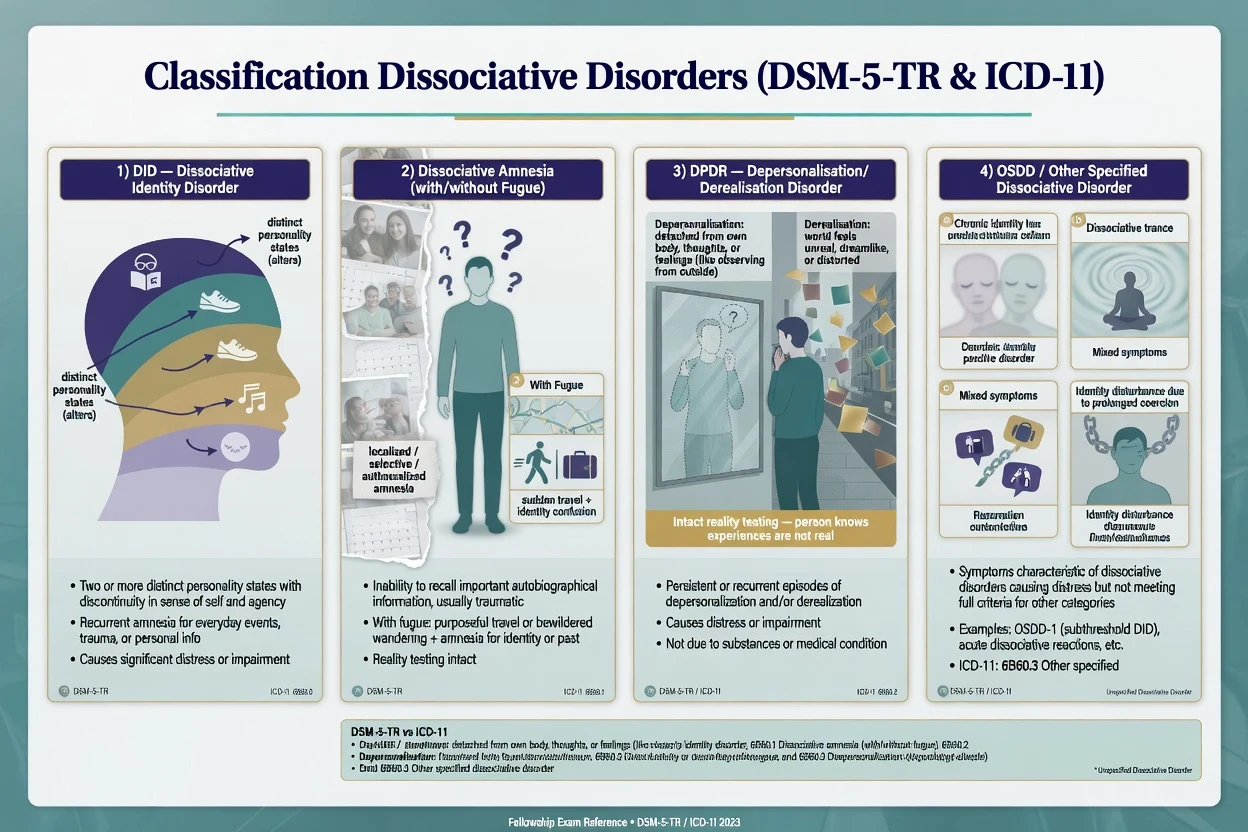
DSM-5-TR core entities examiners expect by name: dissociative identity disorder (DID); dissociative amnesia (with dissociative fugue as a specifier/context of purposeful travel or bewildered wandering); depersonalisation/derealisation disorder (DPDR); and other specified / unspecified dissociative disorder for clinically significant presentations that do not meet full criteria for a named entity.[1]
DID (evidence-based wording). Disruption of identity characterised by two or more distinct personality states (in some cultures described as an experience of possession), with discontinuity in sense of self and agency, accompanied by related alterations in affect, behaviour, consciousness, memory, perception, cognition and/or sensory-motor functioning. Recurrent gaps in the recall of everyday events, important personal information and/or traumatic events that are inconsistent with ordinary forgetting. Symptoms cause clinically significant distress or impairment, are not a normal part of a broadly accepted cultural or religious practice, and are not attributable to substance or another medical condition. In children, symptoms are not better explained by imaginary playmates or fantasy play.[1][2]
DPDR. Persistent or recurrent experiences of depersonalisation (unreality or detachment from one's thoughts, feelings, sensations, body or actions) and/or derealisation (unreality or detachment from surroundings), with reality testing remaining intact during the experiences — the patient knows the experience is not externally "true" in a delusional sense.[1][14]
Dissociative amnesia. Inability to recall important autobiographical information, usually of a traumatic or stressful nature, that is inconsistent with ordinary forgetting. Patterns may be localised, selective, generalised, continuous or systematised; fugue presentations add travel or wandering with identity confusion or assumption of a new identity in classic descriptions.[1]
Classification
DID
- ≥2 distinct personality states / identity disruption
- Recurrent amnesia inconsistent with ordinary forgetting
- Distress/impairment required
- Not cultural practice, substance or medical
Dissociative amnesia
- Autobiographical memory gap
- Usually trauma/stress linked
- Fugue: travel/wandering context
- Reality testing otherwise intact
DPDR
- Depersonalisation and/or derealisation
- Reality testing intact (key discriminator)
- Persistent/recurrent with impairment
- Primary vs secondary to panic/depression/substance
OSDD / ICD-11 partial
- Clinically significant but subthreshold
- Partial DID concepts in ICD-11
- Possession-form presentations need cultural formulation
- Avoid forcing a full DID label
ICD-11 pointers. ICD-11 retains dissociative identity disorder and describes partial DID, depersonalisation-derealisation disorder, dissociative amnesia, and trance/possession-related categories that require cultural competence. In the exam, name the manual and avoid inventing hybrid criteria.[1]
Related but not identical. PTSD with dissociative symptoms (depersonalisation or derealisation) is a specifier within trauma- and stressor-related disorders, not automatically a freestanding dissociative disorder. Conversion/functional neurological symptom disorder and somatic presentations may co-occur and need separate formulation.[16][1]
Epidemiology and risk factors
Numbers and patterns candidates should own
Lyssenko and colleagues' meta-analysis of DES scores across psychiatric diagnoses shows the highest mean dissociation scores in dissociative disorders, with elevated means also in PTSD, borderline personality disorder and conversion disorder relative to many other categories — useful for viva framing of comorbidity, not for diagnosing from a score alone.[5]
Community samples report non-trivial rates of dissociative disorders with substantial comorbidity and functional impairment; a Turkish general-population study of women found lifetime dissociative disorder diagnoses including DID at about 1% and higher rates of other specified/DDNOS-type presentations, with childhood trauma associations.[6] A US community cohort similarly linked dissociative disorders to impairment and Axis I/II comorbidity.[18] In psychiatric outpatients, structured assessment identifies a clinically meaningful prevalence of dissociative disorders that is often missed in routine care.[7]
Risk associations. Childhood sexual abuse, physical abuse, neglect and other chronic interpersonal trauma are strongly associated with pathological dissociation in multiple lines of research, without proving a single necessary pathway in every case.[3][6] Ongoing threat, poor social support, and high suggestibility contexts are formulation-relevant. Do not treat social-media identity language as diagnostic by itself; assess function, amnesia, distress and differential carefully.[4]
Pathophysiology
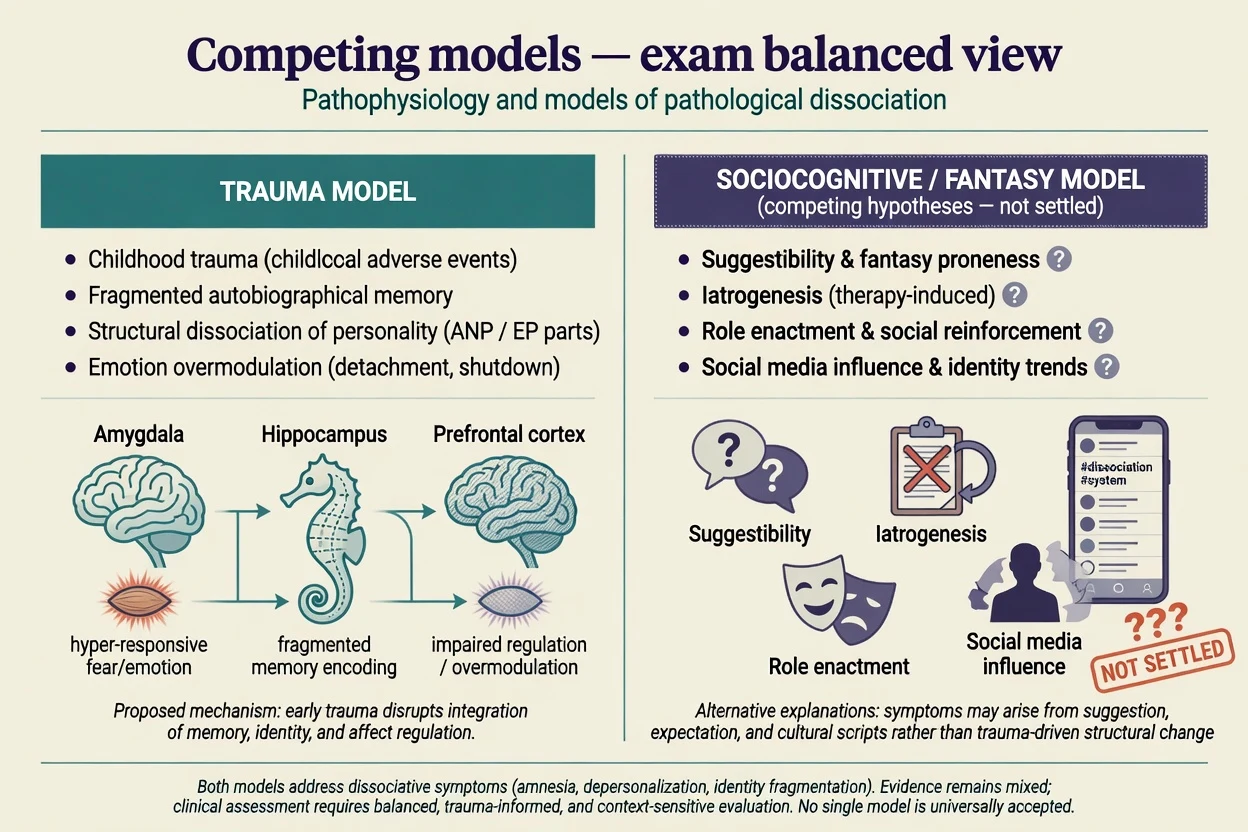
Trauma model. Pathological dissociation is conceptualised as a trauma-related failure to integrate aspects of experience, memory and identity, with childhood interpersonal trauma as a major risk context. Dalenberg and colleagues evaluated evidence for trauma versus fantasy models and concluded that the data more strongly support a trauma-related account of pathological dissociation, while still requiring rigorous methods to avoid circularity.[3] Structural dissociation models (apparently normal personality versus emotional parts) are useful clinical maps, not proven neuroimaging diagnoses.[2]
Sociocognitive / fantasy model. Critics emphasise suggestibility, fantasy proneness, iatrogenic shaping in therapy, media scripts and role enactment as alternative or contributing pathways to identity fragmentation presentations.[4] A balanced fellowship answer acknowledges these risks without reducing all DID to factitious play. Lynn and colleagues review competing models and call for integrative, falsifiable research programmes.[4]
Psychobiology (research depth, not bedside test). Studies of authentic versus simulated identity states report distinguishable psychobiological patterns, arguing against a simple "all acting" account for every case, while still not providing a clinical biomarker.[17] Depersonalisation has been framed with corticolimbic disconnection and emotional numbing hypotheses — prefrontal over-regulation dampening limbic affective colouring of experience.[14] PTSD research supports a dissociative subtype with emotion overmodulation contrasting with undermodulated re-experiencing profiles at the group level.[16]
Clinical presentation
DID. Patients may describe time loss, finding belongings they do not recall acquiring, being told of behaviours they do not remember, hearing internal dialogues or "voices" of self-states, sudden shifts in demeanour/age/skills, and somatic symptoms. Internal voices are often experienced as inside the head and related to parts of self rather than as classic third-person external hallucinations with thought disorder — but overlap and comorbidity exist, so do not use a single feature as a hard rule.[2]
DPDR. Unreality of self (watching oneself from outside; emotional deadness; body feels alien) and/or unreality of the world (dreamlike, foggy, visually distorted surroundings). Anxiety and depression commonly co-travel. Insight that the experience is subjective is typical and exam-critical.[14]
Dissociative amnesia / fugue. Gaps for personal events; inability to recall identity or past in severe forms; purposeful travel or wandering in fugue presentations with later recovery of memory in many cases. Safety risks include vulnerability while amnestic.[1]
MSE language. Appearance may shift mid-interview; affect may be restricted or incongruent with reported trauma; thought form usually preserved outside crisis; thought content may include trauma themes and self-state descriptions; perception may include internal voices; cognition may show autobiographical gaps with intact registration of new information; insight variable; risk assessment mandatory.[2][10]
Differential diagnosis
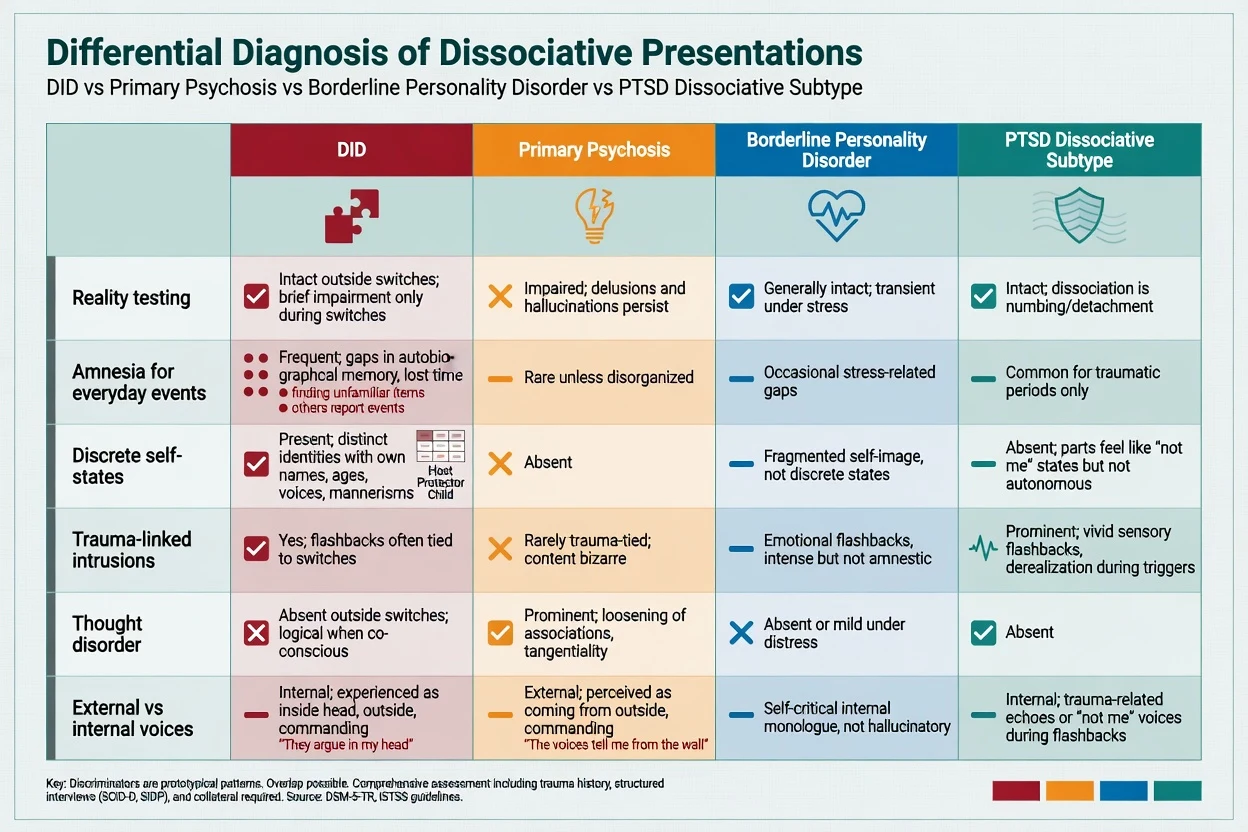
| Discriminator | Favours DID / DD | Favours primary psychosis | Favours BPD | Favours PTSD dissoc. subtype |
|---|---|---|---|---|
| Reality testing | Generally intact outside switches | Impaired; delusions persist | Usually intact | Intact |
| Amnesia for everyday events | Frequent, inconsistent with ordinary forgetting | Uncommon unless disorganised | Occasional stress gaps | Mainly for trauma periods |
| Identity | Discrete self-states | No true alternate identities | Chronic emptiness / unstable self-image | "Not me" states without autonomous parts system |
| Voices | Often internal, related to parts | Often external, with thought disorder/delusions | Self-critical internal monologue | Trauma-echo phenomena |
| Course | Long, trauma-linked | First-rank/negative symptoms pattern | Relational/affective instability core | Trauma cluster criteria met |
| Key discriminators for exam use; overlap and dual diagnosis possible.[2][16] |
Also exclude substance-induced states (cannabis, ketamine, hallucinogens), complex partial seizures / TLE, delirium, autoimmune encephalitis, TBI sequelae, sleep disorders, and factitious disorder / malingering when secondary gain, marked inconsistency, or medico-legal context dominates — assess non-punitively and document carefully.[1][2]
Clinical and bedside assessment
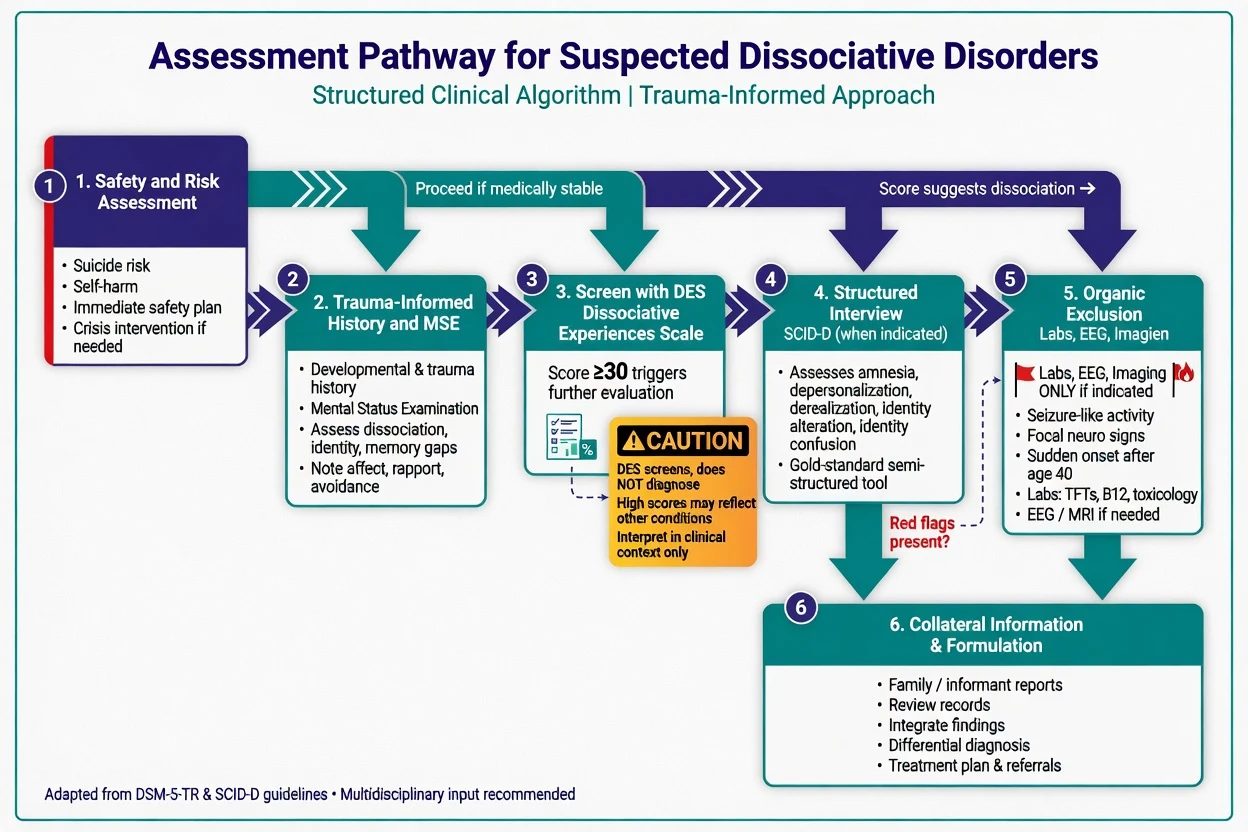
Trauma-informed interview. Prioritise safety, pacing, consent and collaboration. Establish enough history to understand identity continuity, amnesia and trauma context without forcing graphic trauma excavation in the first minutes. Avoid leading questions that suggest specific abuse narratives or "alters". Use interpreters and cultural formulation for possession-form experiences.[11][2]
DES (Dissociative Experiences Scale). Bernstein and Putnam developed the DES as a self-report measure of dissociative experiences for research and clinical screening.[9] High scores raise suspicion and track severity but do not diagnose DID; elevated scores also occur in PTSD, BPD and other conditions.[5][9]
SCID-D / SCID-D-R. Structured clinical interview assessing amnesia, depersonalisation, derealisation, identity confusion and identity alteration — used for diagnostic clarification and treatment planning when trained interviewers are available.[10]
Risk. Suicide attempts and self-injury are elevated in outpatient dissociative samples relative to comparison psychiatric outpatients; assess intent, plan, means, past behaviour, protective factors, and child protection issues every time.[8] Capacity is decision-specific. Legal status uses local mental health law — least restrictive; do not invent section numbers for the wrong jurisdiction.
Investigations
There is no diagnostic MRI, PET or blood test for DID or DPDR. Order investigations to exclude organic mimics and to prepare safely for medication used for comorbidity: TSH, B12/folate, U&E, LFT, glucose as indicated; urine drug screen when substance contribution is plausible; ECG before agents with cardiac risk; EEG/neuroimaging when seizure clues, focal neurology, first late-onset atypical presentation, or encephalitic red flags appear. Serial DES or symptom diaries support measurement-based care; specialised depersonalisation scales may track DPDR in research/specialist settings.[14][9]
Management — acute / resuscitation
Acute priorities. Medical ABC and organic exclusion when indicated; calm environment; orientation and grounding (five-senses, present-moment cues, safe-place imagery without forced trauma recall); reduce substance intoxication/withdrawal risks; collaborative safety planning and means restriction; consider brief admission if unable to keep self safe. Short-term symptomatic medication may be needed for severe agitation or insomnia, but avoid reflexive high-dose antipsychotics for non-psychotic internal voices and avoid long-term benzodiazepines as a dissociation "cure".[11][2]
Management — definitive and stepwise
Phase-oriented psychotherapy (DID / complex DD)
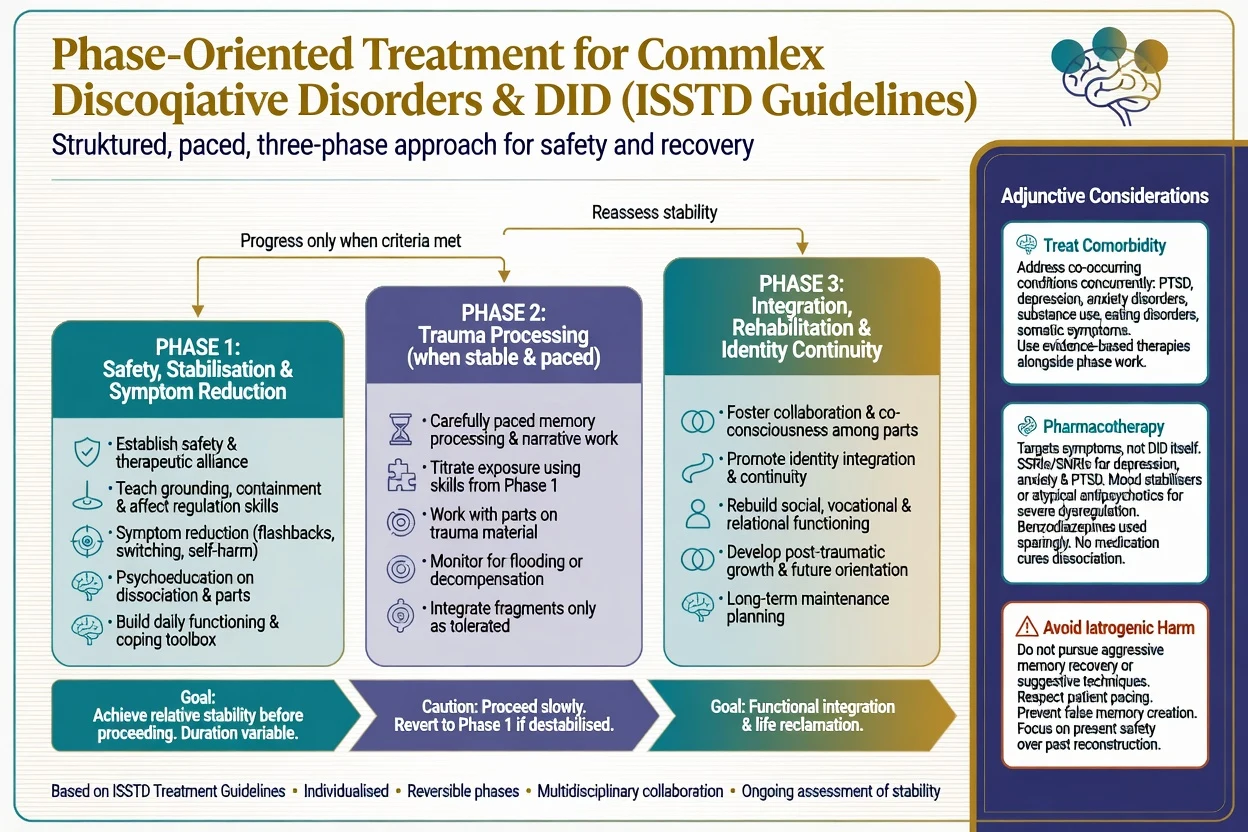
ISSTD adult DID guidelines describe a three-phase framework widely taught in fellowship settings:[11]
- Phase 1 — Safety, stabilisation, symptom reduction. Therapeutic alliance; psychoeducation; affect regulation and grounding; reduce self-harm and high-risk behaviours; improve daily functioning; treat acute comorbidity; establish collaborative communication among self-states without forcing premature fusion.
- Phase 2 — Trauma processing. Carefully paced work with traumatic memories when the patient has sufficient stabilisation skills; titrate exposure; monitor for flooding, increased self-injury, or functional collapse; return to Phase 1 if needed.
- Phase 3 — Integration and rehabilitation. Greater identity continuity, relational and vocational recovery, relapse prevention. Full fusion is not the only acceptable outcome; improved cooperative functioning and reduced amnesia may be goals. Phase model summarised from ISSTD adult DID guidelines.[11]
Evidence quality (state honestly). Randomised trial evidence for DID-specific protocols remains limited relative to PTSD psychotherapies. Naturalistic multi-site TOP DD work and long-term follow-up suggest that patients in treatment with community clinicians can show gradual improvement in symptoms and adaptive functioning over years, supporting engaged specialist-informed care rather than therapeutic nihilism.[12][2] A systematic review literature on phase-oriented approaches continues to evolve; candidates should not oversell RCT certainty that does not exist.[11][12]
DPDR-specific care
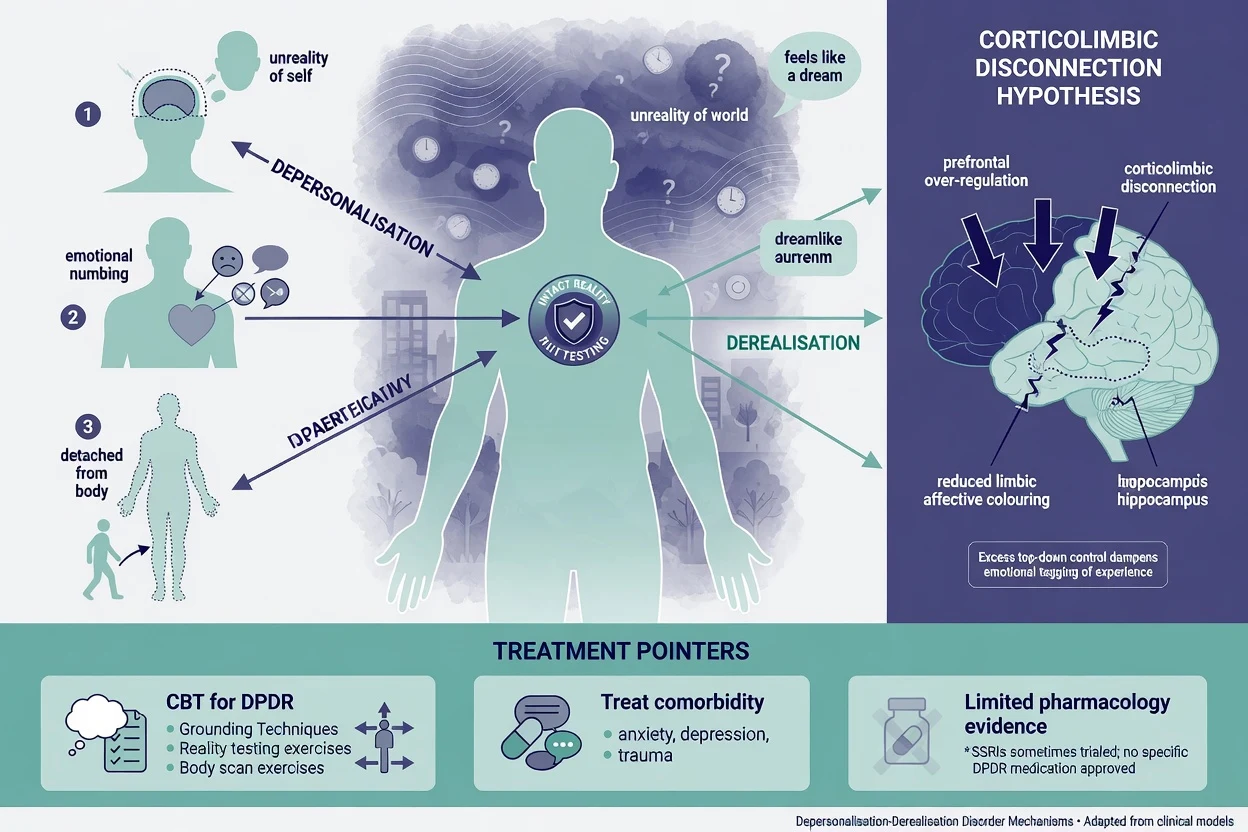
Cognitive-behavioural approaches targeting catastrophic appraisals of depersonalisation experiences, safety behaviours and attention processes showed benefit in an open study of individual CBT for depersonalisation disorder.[13] Simeon's overview remains a useful clinical map of presentation and treatment options.[14] Pharmacologic evidence is limited: lamotrigine as add-on has retrospective support in selected cases and is not a first-line universal cure; naltrexone and other agents have been explored in small open designs. Typical adult lamotrigine titration for psychiatric use (when chosen off-label for DPDR after specialist consideration) must follow rash-risk slow titration as for mood indications — e.g. start 25 mg orally daily with gradual increases per product information, watching for serious rash — and is best framed as experimental/adjunctive rather than definitive.[15][14] Treat comorbid depression, anxiety and PTSD with standard evidence-based therapies.
Pharmacotherapy principles for DID / complex DD
Medications treat comorbidity and target symptoms (depression, PTSD, anxiety, insomnia, severe affective instability) rather than "curing" DID identity structure.[11][2] Prefer agents with evidence for the comorbid condition (e.g. SSRI for MDD/PTSD as appropriate) with usual monitoring. Avoid chronic polypharmacy. Antipsychotics are for true psychotic comorbidity or acute agitation pathways — not automatic for all internal voices. Benzodiazepines are not a long-term dissociation treatment.
What not to do
- Aggressive memory recovery, hypnosis-for-memory, or highly leading interviews that risk confabulation.[4][11]
- Premature intensive exposure without stabilisation in complex dissociation.[11]
- Dismissing all dissociation as factitious or validating every social-media self-diagnosis without assessment.[4]
- Indefinite "stabilisation only" that never offers skilled trauma-informed therapy when the patient is ready and safe.[11]
Specific subtypes and scenarios
Partial / OSDD presentations. Subthreshold identity disruption with clinically significant amnesia or dissociative symptoms is common; treat the functional problem with the same safety-first logic without overstating a full DID label.[1][2]
PTSD dissociative subtype. Meets PTSD criteria with depersonalisation/derealisation; emotion overmodulation model informs care; trauma-focused therapies remain relevant with careful pacing.[16]
Possession-form presentations. Cultural formulation first; distinguish culturally sanctioned practice from distress/impairment and from primary psychosis.[1]
Social media–influenced identity language. Explore function, amnesia, trauma, suggestibility and secondary gain carefully; neither mock nor rubber-stamp.[4]
Acute fugue. Safety, medical exclusion, identity restoration supports, protect from exploitation, gradual history reconstruction without leading.[1][11]
Complications and pitfalls
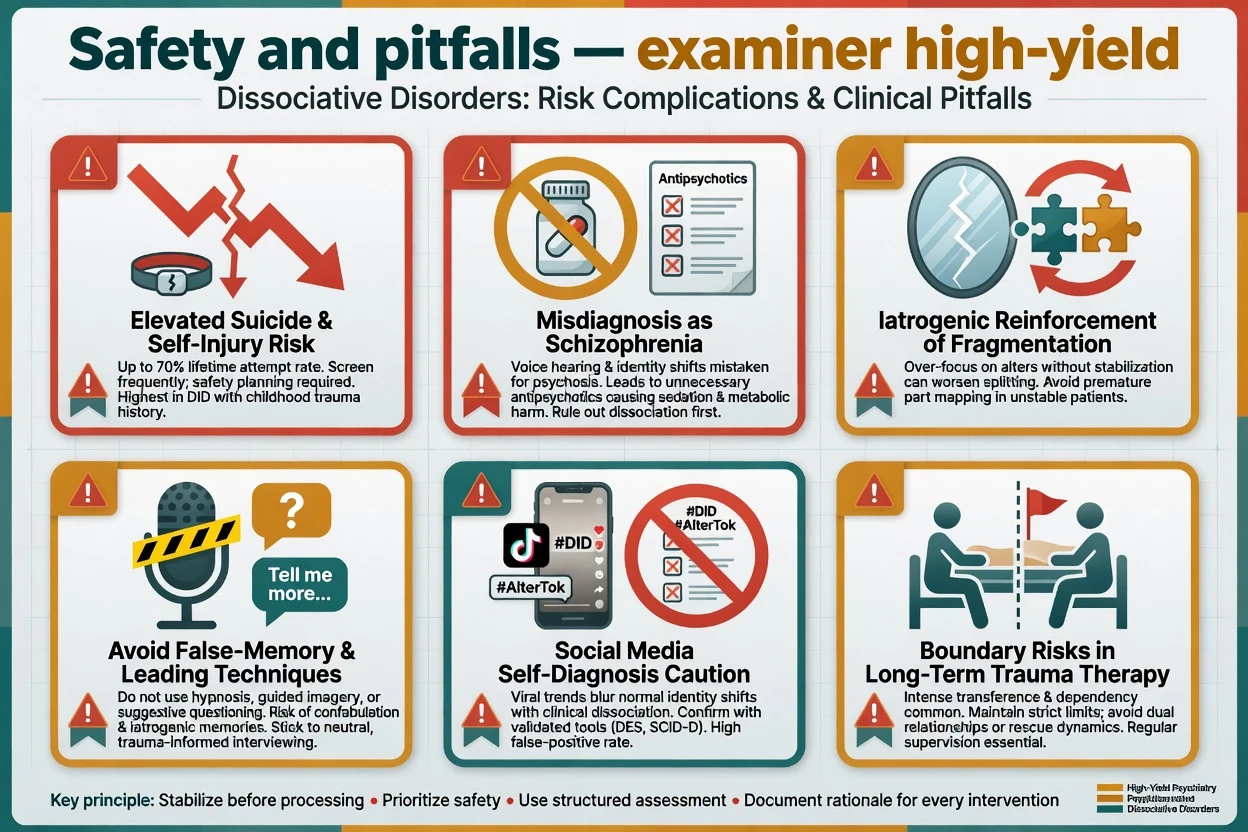
Classic failures: missing suicide risk; years of unnecessary high-dose antipsychotics for mislabelled "schizophrenia"; iatrogenic reinforcement of fragmentation; boundary violations in long trauma therapies; contested-memory litigation contexts; and therapeutic polarisation (everything is DID vs nothing is DID).[8][2][4]
Prognosis and disposition
Course is often chronic without treatment. Engaged, phase-oriented care can yield gradual gains over years in naturalistic cohorts.[12] Prognosis worsens with ongoing trauma, severe self-injury, untreated substance use, and chaotic care systems. Disposition: outpatient specialist psychotherapy when safe; crisis/inpatient care for acute high risk or severe dysfunction; stepped care and shared care with GP; clear follow-up and safety-net instructions.
Special populations
Adolescents. Developmental identity exploration is normal; diagnose DID only with rigorous criteria. Balance concern about social contagion/scripts with validation of distress and trauma screening.[1][2]
Older adults. Late presentation of amnesia needs medical exclusion; lifelong trauma histories may surface in care transitions.[1]
Perinatal. Prioritise mother–infant safety, treat depression/PTSD comorbidity with pregnancy-appropriate choices, and maintain grounding skills around birth triggers.[11][2]
Cultural / Indigenous contexts. Use cultural formulation; work with interpreters and cultural consultants; avoid pathologising sanctioned spiritual practice while still treating impairment and risk.[1]
Evidence, guidelines and regional differences
FRANZCP candidates should cite Dorahy's ANZJP empirical overview of DID, use trauma-informed public mental health frameworks, and access specialist psychotherapy where available. There is no single national "DID drug algorithm"; phase-oriented psychological care and comorbidity treatment dominate.[2][11]
Landmark anchors: Spiegel DSM-5 nosology review; Dalenberg trauma vs fantasy evaluation; Lyssenko DES meta-analysis; ISSTD treatment guidelines; Hunter CBT for DPDR; Foote prevalence and suicidality studies.[1][3][5][11][13][7][8]
Exam pearls
DISSOCIATE — bedside checklist
References
- [1]Spiegel D, Lewis-Fernández R, Lanius R, Vermetten E, Simeon D Dissociative disorders in DSM-5 Annu Rev Clin Psychol, 2013.PMID 23394228
- [2]Dorahy MJ, Brand BL, Sar V, Krüger C, Stavropoulos P Dissociative identity disorder: An empirical overview Aust N Z J Psychiatry, 2014.PMID 24788904
- [3]Dalenberg CJ, Brand BL, Gleaves DH, Dorahy MJ, Loewenstein RJ Evaluation of the evidence for the trauma and fantasy models of dissociation Psychol Bull, 2012.PMID 22409505
- [4]Lynn SJ, Maxwell R, Merckelbach H, Lilienfeld SO, Kloet DVH Dissociation and its disorders: Competing models, future directions, and a way forward Clin Psychol Rev, 2019.PMID 31494349
- [5]Lyssenko L, Schmahl C, Bockhacker L, Vonderlin R, Bohus M Dissociation in Psychiatric Disorders: A Meta-Analysis of Studies Using the Dissociative Experiences Scale Am J Psychiatry, 2018.PMID 28946763
- [6]Sar V, Akyüz G, Doğan O Prevalence of dissociative disorders among women in the general population Psychiatry Res, 2007.PMID 17157389
- [7]Foote B, Smolin Y, Kaplan M, Legatt ME, Lipschitz D Prevalence of dissociative disorders in psychiatric outpatients Am J Psychiatry, 2006.PMID 16585436
- [8]Foote B, Smolin Y, Neft DI, Lipschitz D Dissociative disorders and suicidality in psychiatric outpatients J Nerv Ment Dis, 2008.PMID 18195639
- [9]Bernstein EM, Putnam FW Development, reliability, and validity of a dissociation scale J Nerv Ment Dis, 1986.PMID 3783140
- [10]Steinberg M Advances in the clinical assessment of dissociation: the SCID-D-R Bull Menninger Clin, 2000.PMID 10842445
- [11]International Society for the Study of Trauma and Dissociation Guidelines for treating dissociative identity disorder in adults, third revision J Trauma Dissociation, 2011.PMID 21391103
- [12]Myrick AC, Webermann AR, Loewenstein RJ, Lanius R, Putnam FW Six-year follow-up of the treatment of patients with dissociative disorders study Eur J Psychotraumatol, 2017.PMID 28680542
- [13]Hunter EC, Baker D, Phillips ML, Sierra M, David AS Cognitive-behaviour therapy for depersonalisation disorder: an open study Behav Res Ther, 2005.PMID 16005701
- [14]Simeon D Depersonalisation disorder: a contemporary overview CNS Drugs, 2004.PMID 15089102
- [15]Sierra M, Baker D, Medford N, Lawrence E, Patel M Lamotrigine as an add-on treatment for depersonalization disorder: a retrospective study of 32 cases Clin Neuropharmacol, 2006.PMID 16960469
- [16]Lanius RA, Vermetten E, Loewenstein RJ, Brand B, Schmahl C Emotion modulation in PTSD: Clinical and neurobiological evidence for a dissociative subtype Am J Psychiatry, 2010.PMID 20360318
- [17]Reinders AA, Willemsen AT, Vos HP, den Boer JA, Nijenhuis ER Fact or factitious? A psychobiological study of authentic and simulated dissociative identity states PLoS One, 2012.PMID 22768068
- [18]Johnson JG, Cohen P, Kasen S, Brook JS Dissociative disorders among adults in the community, impaired functioning, and axis I and II comorbidity J Psychiatr Res, 2006.PMID 16337235