Psych · General adult psychiatry — factitious disorder and malingering
Factitious disorder and malingering
Also known as Munchausen syndrome · Munchausen by proxy · Factitious disorder imposed on self · Factitious disorder imposed on another · Fabricated or induced illness · Medical child abuse · Feigning · Symptom exaggeration · SIRS · Performance validity
Exam-exhaustive fellowship reference on factitious disorder (self and other) versus malingering — intentionality continuum, hospital and forensic assessment, collateral and documentation, ethics without collusion, FII/MCA safeguarding, validity testing, and non-punitive coordinated management. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship examiners use these presentations to test intentionality, ethics, safeguarding, and forensic reasoning — not merely a definition list. Candidates who only memorise "Munchausen equals hospital hopping" fail MEQs that require discrimination from FND and SSD, lawful information-sharing, and a plan that avoids collusion while remaining clinically humane.[2][17]
Overview and definition
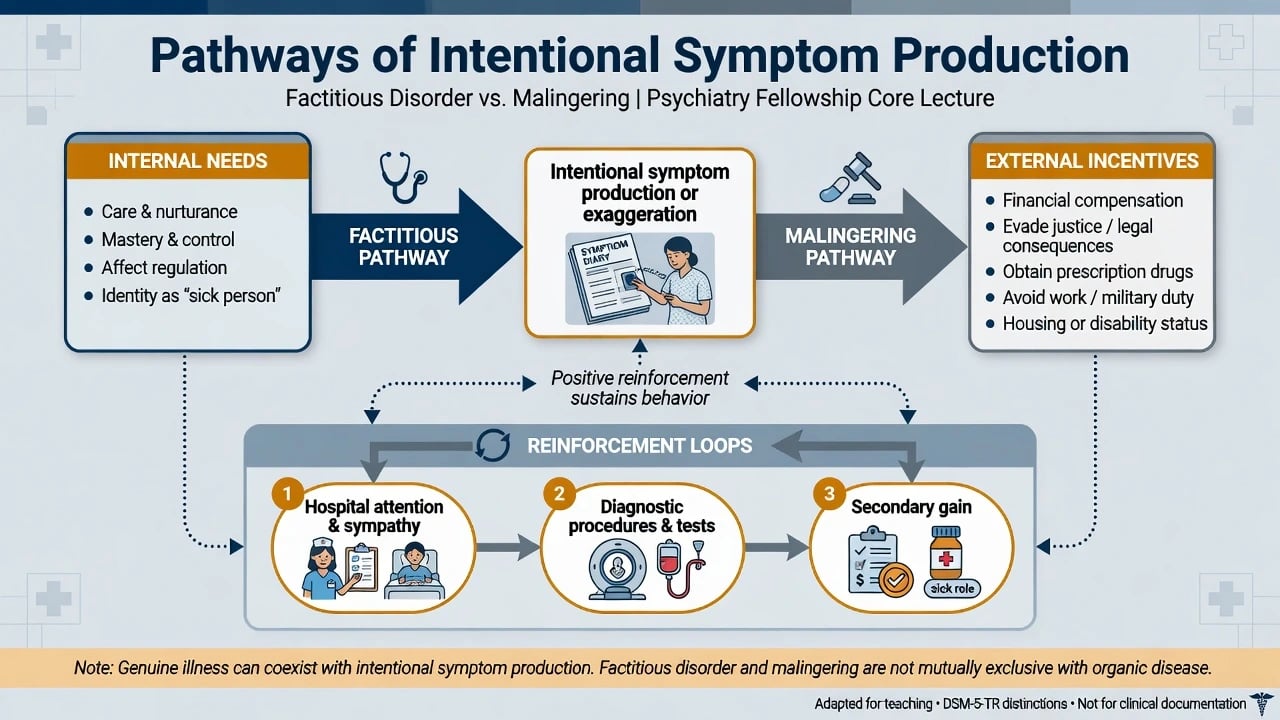
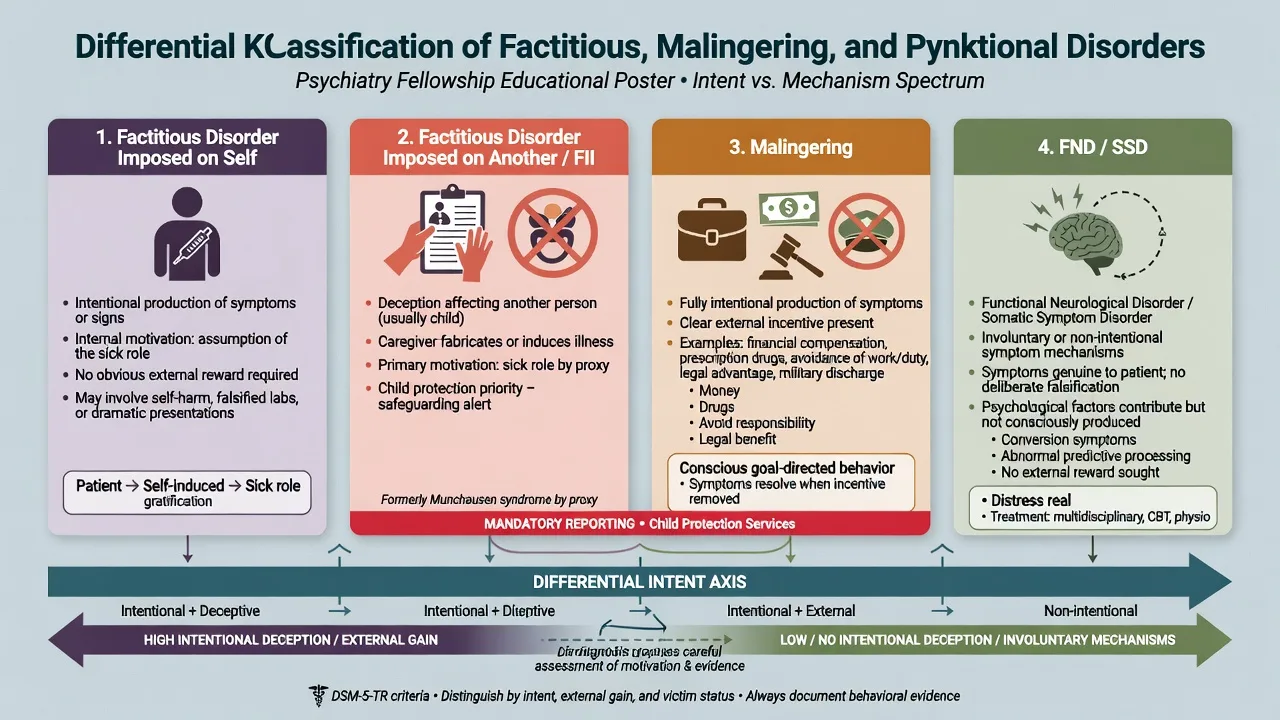
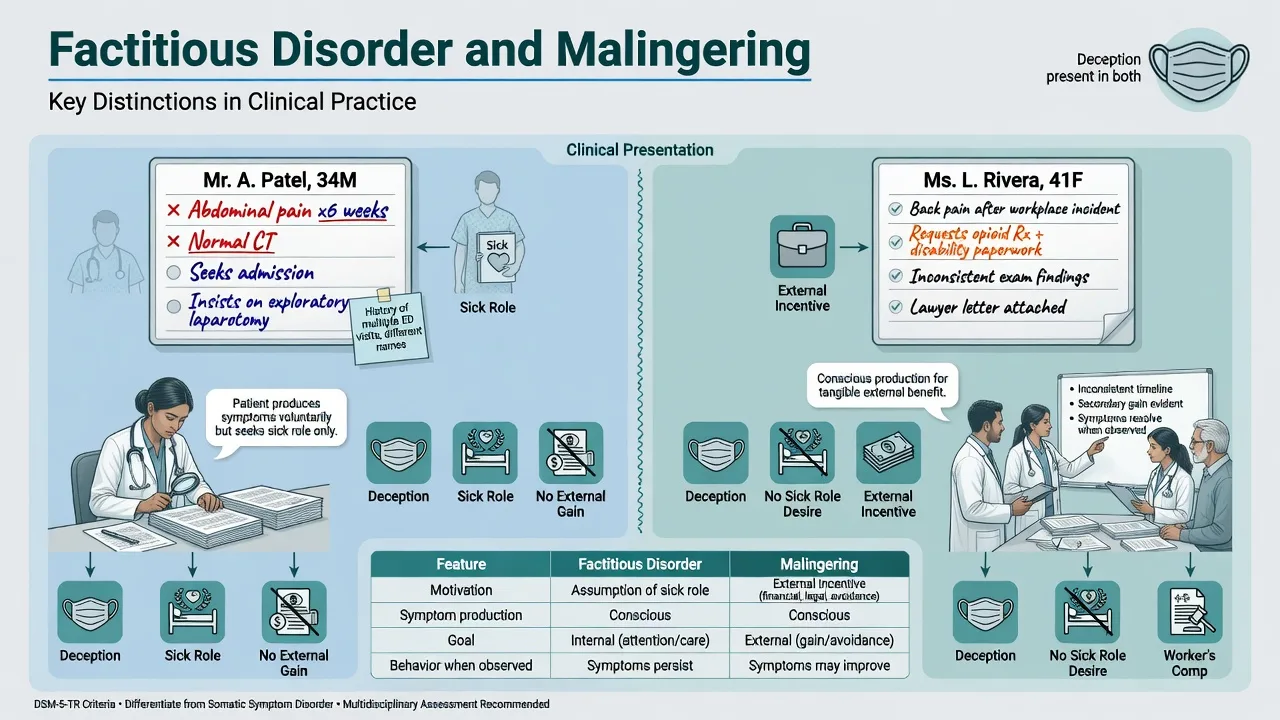
Factitious disorder imposed on self (FDIS). The person falsifies physical or psychological signs or symptoms, or induces injury or disease, in association with identified deception. The deceptive behaviour is evident even in the absence of obvious external rewards, and is not better explained by another mental disorder such as a delusional disorder with somatic content. Presentation may be predominantly physical, psychological, or mixed.[2][12][15]
Factitious disorder imposed on another (FDIA). The same deceptive process is directed at another person (classically a child; also vulnerable adults). The diagnosis is assigned to the perpetrator. Clinical and legal systems also use fabricated or induced illness (FII) and medical child abuse (MCA) language — candidates should name the local framework and not treat the labels as interchangeable without context.[7][8]
Malingering. Intentional production of false or grossly exaggerated symptoms, motivated by external incentives (financial compensation, disability benefits, obtaining controlled drugs, avoiding work or military duty, evading criminal responsibility). Malingering is not classified as a mental disorder in DSM-5-TR; it is a condition that may be a focus of clinical attention. Partial exaggeration of genuine illness is common and clinically important.[2][16][10]
Legacy terms. Asher described Munchausen syndrome as a dramatic, chronic, hospital-migrating pattern of factitious illness behaviour — a severe clinical stereotype within the broader factitious spectrum, not a separate modern DSM code.[1] Historical "Munchausen by proxy" maps largely onto FDIA/FII/MCA work.[7]
ICD-11. ICD-11 retains factitious disorder constructs emphasising intentional production or feigning of symptoms or disability not better explained by another mental disorder; state the manual you are using in the viva and avoid hybrid criteria.[12]
Classification
FDIS
- Intentional falsification/induction
- Identified deception
- Sick-role / care-seeking driver
- External reward not required
FDIA / FII
- Deception imposed on another
- Diagnosis of perpetrator
- Safeguarding primacy
- Multi-agency response
Malingering
- Intentional production/exaggeration
- External incentive primary
- Not a mental disorder
- Context: legal, drugs, duty
FND / SSD
- Not intentional deception
- FND: involuntary motor/sensory
- SSD: distress about symptoms
- Different alliance tasks
Key nosological friction. DSM-5 moved factitious disorder among somatic symptom and related disorders and emphasised deception; critics note conceptual and clinical difficulty distinguishing factitious, malingering, and some somatic presentations when intent is inferred rather than observed.[15][12] Fellowship answers state uncertainty honestly while still making a working formulation for safety and disposition.
Epidemiology and risk factors
True population prevalence is unknown because cases are concealed, under-coded, and published as case series rather than community surveys.[3][12] Yates and Feldman systematically reviewed 455 published factitious cases, documenting medical and psychiatric presentations, high rates of healthcare contact, and patterns useful for clinical suspicion without providing a clean community prevalence.[3] Reich and Gottfried described factitious disorders in a teaching hospital with multi-system presentations and substantial utilisation and iatrogenic risk.[4] Krahn and colleagues characterised patients who "strive to be ill," reinforcing the chronic, treatment-seeking phenotype of physical factitious disorder in tertiary centres.[5]
Risk and enrichment contexts. Some series show female predominance for non-wandering hospital factitious presentations and enrichment of healthcare training or medical knowledge; classic Munchausen wanderers are often described as male in historical literature — treat sex ratios as series-dependent, not universal law.[3][1] Personality disorder comorbidity, childhood illness or trauma histories, and attachment disruption appear in clinical formulations but are not pathognomonic.[13] For malingering, base rates rise sharply in compensation-seeking, litigation, and forensic contexts compared with routine clinical care — Mittenberg and colleagues quantified high rates of symptom exaggeration/malingering across referral settings in a survey of neuropsychologists, underscoring the need for base-rate-aware assessment rather than rare-disease thinking in high-stakes evaluations.[10][16]
FDIA/FII. Young children carry the highest risk of severe harm and death; mothers are the most frequently identified perpetrators in published series, but fathers and other carers also offend — never use gender stereotypes as a screening test.[7][8]
Pathophysiology and mechanisms
There is no diagnostic blood test, scan, or EEG for factitious disorder or malingering. Mechanisms are behavioural, interpersonal, and contextual.[2]
Psychological maps for factitious presentations. Proposed drivers include need for care and the sick role, mastery over medical systems, regulation of intolerable affect through illness identity, dependency and masochistic dynamics, and reinforcement from attention, procedures, and admissions.[13][5] These are formulation tools, not proven single-cause pathways.
Malingering as instrumental behaviour. External incentives organise feigning; coaching and internet scripts can improve sophistication. Genuine illness may coexist with exaggeration — binary "all fake" thinking is a clinical error.[16][10]
Detection science (forensic/neurocognitive interface). Slick, Sherman and Iverson proposed criteria for malingered neurocognitive dysfunction integrating evidence from definite negative response bias, discrepancies, and secondary gain context — later updated in multidimensional frameworks for neuropsychological practice.[9] Rogers and colleagues developed structured detection strategies (e.g. SIRS) for feigned mental disorders using rare symptoms, symptom combinations, and severity patterns that genuine patients rarely endorse at the same rate.[11][16] Relation to FND: intentional deception must be distinguished from involuntary functional symptoms; Bass and Halligan map the clinical boundary carefully for neurologists and psychiatrists.[17]
Clinical presentation
Hospital FDIS (physical). Inconsistent history and findings; eagerness for invasive procedures; extensive surgical scars; unusual knowledge of medical terminology; symptoms that worsen under observation or improve when unsupervised; laboratory values incompatible with claimed physiology; doctor-shopping and discharge against advice when confronted.[4][5][3] Asher's original description captured dramatic wandering careers and tall medical storytelling as a clinical stereotype.[1]
Psychiatric factitious. Feigned psychosis, PTSD, amnesia, or suicidality with atypical scripts, inconsistent MSE over time, and admissions timed to psychosocial crises without corresponding risk trajectory — still assess real suicide risk seriously; people who feign can also die by suicide.[2][18]
FDIA/FII clues (victim-focused). Recurrent unexplained illness; symptoms witnessed only by one carer; laboratory or video inconsistencies; carer insisting on further invasive tests; multiple hospital migrations; sibling histories of unusual illness; carer appearing oddly calm or over-involved with staff.[7]
Malingering clues (none pathognomonic alone). Medicolegal context; marked discrepancy between claimed disability and observed function; non-cooperation with assessment; antisocial history; symptom reports that track incentive more than pathophysiology.[10][14][16]
MSE language. Describe consistency of symptoms across time and setting, quality of detail, response to non-leading probes, observed versus reported function, and engagement with treatment that would reduce secondary gain. Avoid pejorative labels in the MSE section; record behaviours and discrepancies factually.[2][18]
Differential diagnosis
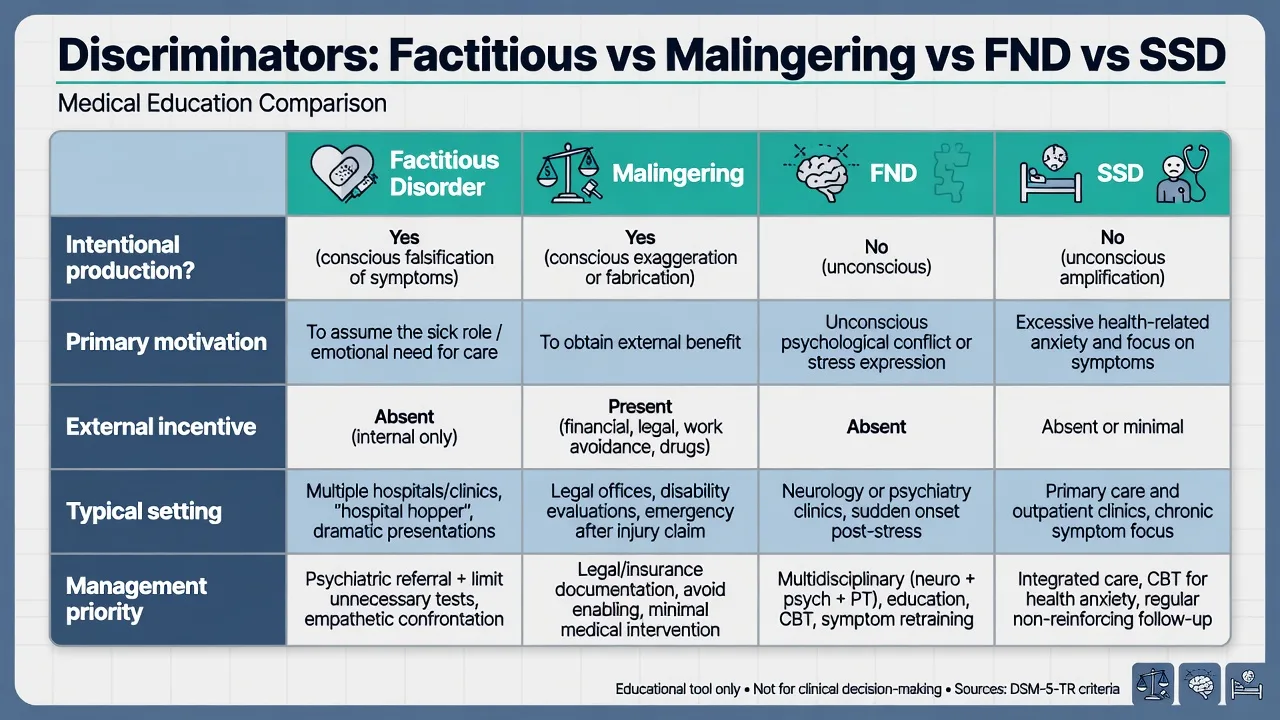
| Axis | Favours FDIS | Favours malingering | Favours FND | Favours SSD / IAD |
|---|---|---|---|---|
| Intentional production | Yes (deception) | Yes | No (involuntary) | No |
| Primary driver | Sick role / care / mastery | External incentive | Symptom generation mechanisms | Health anxiety / somatic distress |
| External reward | Not required | Central | Not defining | Not defining |
| Typical exam trap | Called "malingering" without incentive | Called "factitious" to soften legal language | Called "faking" | Endless investigation without formulation |
| First management task | Harm reduction, non-collusion | Clarify role, report within law, treat real illness | Explain both-and, rehab | Stepped psychological care |
| Differential axes synthesised for exam use from clinical reviews.[2][17][15] |
Also exclude true undiagnosed disease, substance intoxication/withdrawal, medication effects, primary psychosis with somatic delusions, borderline personality crises with self-injury that is not aimed at medical deception, and cultural idioms of distress. In children, rare genetic and metabolic disease must be actively considered before FDIA is concluded.[7][2]
Clinical and bedside assessment
Team before confrontation. Bass and Halligan emphasise multidisciplinary assessment, careful information gathering, and planned communication rather than lone accusation on the ward round.[2][18]
Collateral and records. With appropriate consent or legal authority, obtain GP notes, prior hospital attendances, pharmacy data, imaging, and pathology. Timelines expose incompatible multi-hospital careers. Supervised specimens and observation when the patient or carer is absent may reveal discrepancies.[5][4]
Risk domains. Self-induced medical harm; iatrogenic harm from procedures; child or adult safeguarding; staff boundary violations; flight risk after discovery. Capacity is decision-specific — ability to understand, retain, use/weigh, and communicate a particular decision under local law; deception does not automatically equal incapacity.[2]
Forensic and civil assessment. Clarify whether you are a treating clinician or independent expert. Informed consent to the scope of assessment. Use structured interviews and validity testing as indicated (SIRS family, SIMS screens, MMPI validity scales, performance validity tests), always interpreted against base rates and possible coaching.[11][9][10][16]
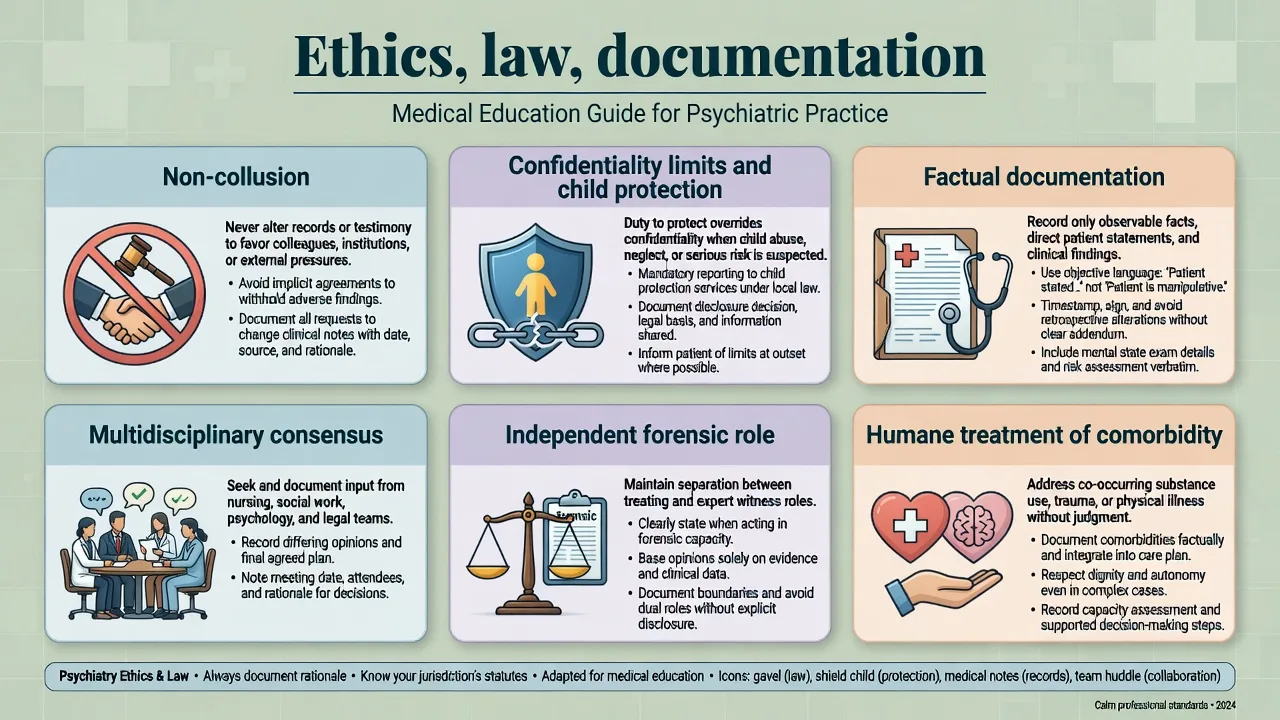
Documentation standard. Record observable facts, sources of collateral, multidisciplinary discussions, and the care plan. Prefer descriptive language ("urine toxicology positive for insulin secretagogue; patient denied access") over premature courtroom labels in shared records when safety and fairness require caution — while still communicating risk clearly to the team.[2][18]
Investigations
Investigations are targeted to protect the patient from harm and to test specific hypotheses (e.g. simultaneous insulin and C-peptide in hypoglycaemia; toxicology; culture of injected material). Endless "rule-out everything" cascades are themselves a form of iatrogenic collusion.[2][5] Do not order tests solely to "prove" psychological origin. In FDIA, prioritise the child's medical safety and use covert strategies only within local legal and ethical frameworks.[7] Psychometric validity instruments support formulation in cognitive and psychiatric feigning evaluations but never replace collateral synthesis.[9][11][16]
Management — acute / resuscitation
Treat sepsis, hypoglycaemia, bleeding, overdose, and acute behavioural disturbance using standard medical and local agitation pathways. Deception does not justify punitive restraint or withholding analgesia for objectively documented injury. Pause non-essential invasive procedures while the team reconvenes.[2][18]
Management — definitive, without collusion
Core principles (factitious disorder)
Eastwood and Bisson systematically reviewed management strategies and found a limited evidence base without high-quality RCTs; clinical practice rests on case series, expert consensus, and harm-reduction logic.[6] Bass and Halligan outline practical challenges: engagement is difficult, confrontation is double-edged, and system coordination is essential.[2]
- Single coordinated plan with a named consultant and GP continuity; limit redundant specialists and procedures.[2][6]
- No collusion: do not certify false diagnoses, prescribe solely to maintain the sick-role deception, or write letters that invent disability.[2][14]
- Communication: many centres prefer a carefully planned, non-punitive discussion that presents inconsistencies, expresses concern for harm, and offers ongoing care; some use face-saving formulations that shift toward rehabilitation without forced confession. Solo public shaming is harmful.[6][18]
- Treat comorbidity: depression, anxiety, PTSD, substance use, and personality disorder pathways with standard evidence-based care. There is no specific drug that extinguishes factitious behaviour. If an antidepressant is used for comorbid major depression (example only — individualise): sertraline often started at 50 mg orally daily (sometimes 25 mg in anxious or medically frail patients), titrated by clinical response and tolerability, with monitoring for activation, hyponatraemia risk in older adults, sexual side effects, and suicide risk discussion in younger patients — this treats depression, not deception.[13][6]
- Psychotherapy: supportive engagement, exploratory/psychodynamic work, or schema-informed approaches in willing patients; outcomes are often modest, especially in chronic wandering phenotypes.[6][13]
- Information-sharing within privacy law to prevent multi-hospital iatrogenic harm; document lawful basis.[2]
Malingering-specific management
Clarify role (treating vs independent). Report findings to the referring legal or administrative body within consent and duty. Treat any genuine medical or psychiatric illness humanely. Do not invent a factitious or other psychiatric diagnosis merely to soften the language of external-incentive feigning when the formulation is malingering.[16][14][2] Military and disability contexts require the same intentionality analysis with organisational policy awareness.[14]
FDIA / FII management
Bass and Glaser emphasise early multi-agency recognition, protection of the child, careful medical evaluation for true disease, and structured management that separates the child's needs from the carer's psychopathology.[7] Bass and Jones describe high rates of personality disorder, somatising, and factitious histories among perpetrators in a case series — informing adult psychiatry input without delaying protection.[8]
Specific subtypes and scenarios
Classic Munchausen wanderer. Multi-hospital surgical career; scars; pseudologia; rapid discharge against advice — prioritise harm reduction and information-sharing.[1][4]
C-L factitious case conference pattern. Complex medical admissions with inconsistencies; psychiatry facilitates team formulation and non-collusive plan.[18]
Psychiatric factitious on the ward. Feigned psychosis or PTSD scripts — use serial MSE, collateral, and structured feigning assessment when stakes are high.[11][16]
Civil litigation TBI/PTSD. High base rates of exaggeration; performance and symptom validity essential; partial valid injury common.[10][9]
ED drug-seeking. External incentive for opioids may be malingering and/or substance use disorder — treat withdrawal and OUD pathways without moralisation while refusing unjustified controlled prescriptions.[14][16]
Dermatology / plastic surgery interface. Artefactual lesions and repeated procedures — joint plans to stop unnecessary surgery.[3]
Complications and pitfalls
Classic failures: iatrogenic multi-organ harm from procedures; missing real disease after labelling someone "factitious"; collusion and false certificates; team splitting; punitive staff responses; delayed child protection; confusing FND with faking; over-reading a single validity scale; and documentation that is either recklessly pejorative or dangerously vague.[2][15][7][16]
Prognosis and disposition
Course is often chronic, especially in classic wandering factitious patterns and untreated FDIA systems.[3][5] Better trajectories associate with engagement, treated comorbidity, stable single-team care, and cessation of multi-hospital migration.[6] Disposition: shared C-L/GP plan; outpatient psychiatry when engaged; safeguarding permanence for children at risk; forensic/administrative pathways for pure malingering once genuine illness is addressed.[2][7]
Special populations
Children as victims. Safeguarding first; paediatric leadership; adult psychiatry for perpetrator assessment when appropriate.[7][8]
Healthcare workers. Access to drugs and devices; occupational health and regulator interfaces; still require fair process and evidence.[3][5]
Older adults / care homes. FDIA by carers; also genuine multi-morbidity that must not be dismissed.[7]
Forensic/prison. Elevated malingering base rates coexist with high true mental illness prevalence — dual vigilance.[16][10]
Cultural contexts. Do not pathologise culturally sanctioned expressions of distress as deception; use cultural formulation.[2]
Evidence, guidelines and regional differences
Landmark anchors: Asher 1951; Bass and Halligan 2014 Lancet assessment/management; Yates and Feldman 455-case review; Eastwood and Bisson management systematic review; Krahn "strive to be ill"; Bass and Glaser FII; Bass and Jones perpetrator psychopathology; Slick MND criteria; Mittenberg base rates; Rogers detection strategies and contemporary overviews.[1][2][3][6][5][7][8][9][10][11][16]
FRANZCP candidates emphasise RANZCP ethical practice, local mental health and child protection legislation (state/territory specific — do not invent section numbers), mandatory reporting duties, and C-L coordination. Document lawful basis for information-sharing between hospitals.[2][7]
Exam pearls
NO COLLUDE — management checklist
Additional high-yield traps: Asher describes a stereotype, not all factitious disorder; FDIA is diagnosed in the perpetrator; validity tests need base rates; confrontation is optional and planned, never a ritual of moral victory; treat real depression and real wounds even when deception coexists.[1][7][10][6]
References
- [1]Asher R Munchausen's syndrome Lancet, 1951.PMID 14805062
- [2]Bass C, Halligan P Factitious disorders and malingering: challenges for clinical assessment and management Lancet, 2014.PMID 24612861
- [3]Yates GP, Feldman MD Factitious disorder: a systematic review of 455 cases in the professional literature Gen Hosp Psychiatry, 2016.PMID 27302720
- [4]Reich P, Gottfried LA Factitious disorders in a teaching hospital Ann Intern Med, 1983.PMID 6881779
- [5]Krahn LE, Li H, O'Connor MK Patients who strive to be ill: factitious disorder with physical symptoms Am J Psychiatry, 2003.PMID 12777276
- [6]Eastwood S, Bisson JI Management of factitious disorders: a systematic review Psychother Psychosom, 2008.PMID 18418027
- [7]Bass C, Glaser D Early recognition and management of fabricated or induced illness in children Lancet, 2014.PMID 24612863
- [8]Bass C, Jones D Psychopathology of perpetrators of fabricated or induced illness in children: case series Br J Psychiatry, 2011.PMID 21804147
- [9]Slick DJ, Sherman EM, Iverson GL Diagnostic criteria for malingered neurocognitive dysfunction: proposed standards for clinical practice and research Clin Neuropsychol, 1999.PMID 10806468
- [10]Mittenberg W, Patton C, Canyock EM, Condit DC Base rates of malingering and symptom exaggeration J Clin Exp Neuropsychol, 2002.PMID 12650234
- [11]Rogers R, Kropp PR, Bagby RM, Dickens SE Faking specific disorders: a study of the Structured Interview of Reported Symptoms (SIRS) J Clin Psychol, 1992.PMID 1401150
- [12]Caselli I, Poloni N, Ielmini M, Diurni M Epidemiology and evolution of the diagnostic classification of factitious disorders in DSM-5 Psychol Res Behav Manag, 2017.PMID 29270035
- [13]Jafferany M, Khalid Z, McDonald KA, Shelley AJ Psychological Aspects of Factitious Disorder Prim Care Companion CNS Disord, 2018.PMID 29489075
- [14]Schnellbacher S, O'Mara H Identifying and Managing Malingering and Factitious Disorder in the Military Curr Psychiatry Rep, 2016.PMID 27752984
- [15]Ross CA Problems With Factitious Disorder, Malingering, and Somatic Symptoms in DSM-5 Psychosomatics, 2019.PMID 30527844
- [16]Rogers R, Bender SD, Hartigan SE An overview of malingering and deception in neuropsychiatric cases Behav Sci Law, 2024.PMID 38047870
- [17]Bass C, Halligan P Factitious disorders and malingering in relation to functional neurologic disorders Handb Clin Neurol, 2016.PMID 27719868
- [18]Margolis M, Wong TL, Shmuts R, Taylor JB Consultation-Liaison Case Conference: A Case of Factitious Disorder Imposed on Self J Acad Consult Liaison Psychiatry, 2023.PMID 37499871