Psych · General adult psychiatry — early psychosis pathway
First-episode psychosis
Also known as FEP · First episode psychosis · Early psychosis · Early intervention in psychosis · First-episode schizophrenia · Duration of untreated psychosis · DUP · Coordinated specialty care · OPUS · RAISE · NAVIGATE
Exam-exhaustive fellowship reference on the first-episode psychosis pathway — definition and DUP, organic exclusion, early intervention evidence (OPUS, RAISE), low-dose antipsychotic starts, family intervention, substance comorbidity, relapse prevention and maintenance duration after FEP, vocational recovery (IPS). Distinct from the full schizophrenia spectrum monograph. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
First-episode psychosis (FEP) is not a single DSM-5-TR or ICD-11 diagnosis. It is the clinical and service pathway for a person presenting with a first clear psychotic episode — before chronic labels calcify and while the critical period for secondary prevention is still open. Fellowship examiners test whether you can run that pathway end-to-end: calculate DUP, exclude organic and substance mimics, choose and dose an antipsychotic like a first-episode specialist, recruit the family, plan relapse prevention, and keep work and study on the board. This topic is the FEP pathway monograph; the full schizophrenia spectrum taxonomy and clozapine TRS depth live in the related spectrum topic.[1][5][19]
Overview and definition
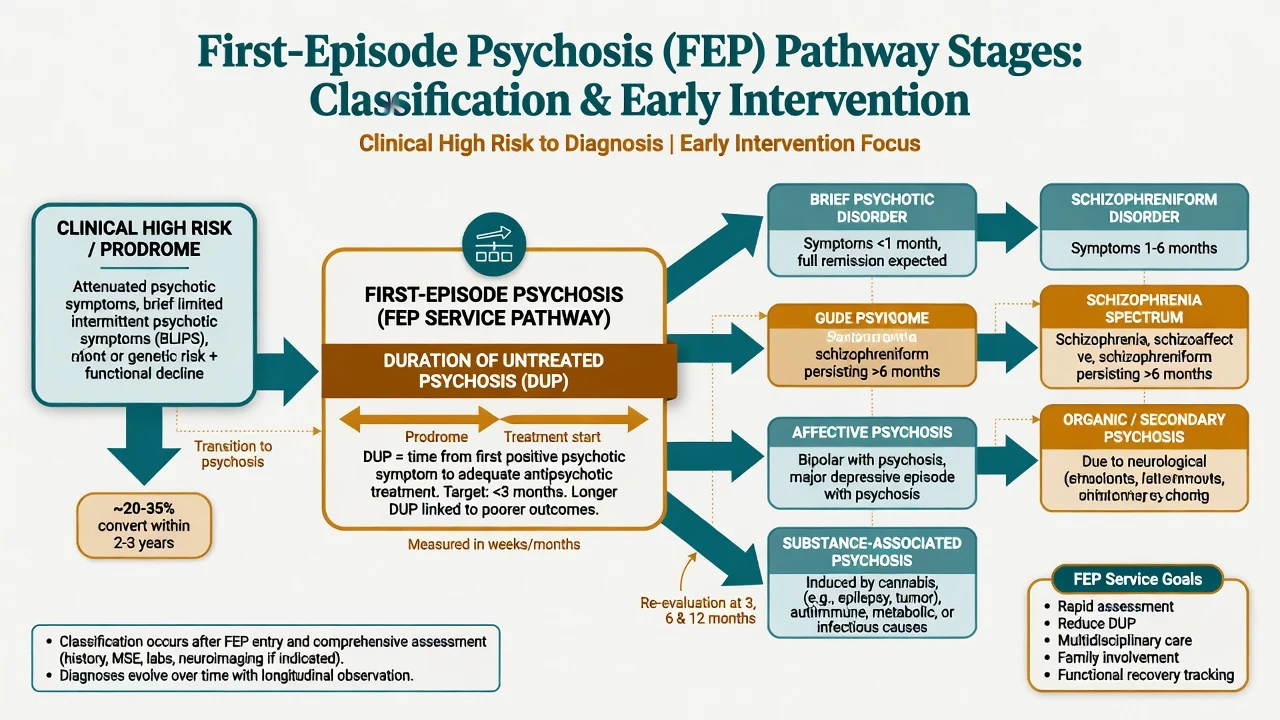
FEP means a first presentation of psychotic symptoms of clinical severity — delusions, hallucinations, disorganised speech or behaviour, often with functional decline — that warrants specialised assessment and treatment, after reasonable exclusion of delirium and primary medical causes. The working label at day one is often provisional (first-episode schizophrenia spectrum psychosis, schizophreniform, brief psychotic disorder, affective psychosis, substance-associated psychosis). Diagnosis is allowed to evolve over months as duration thresholds are met.[19]
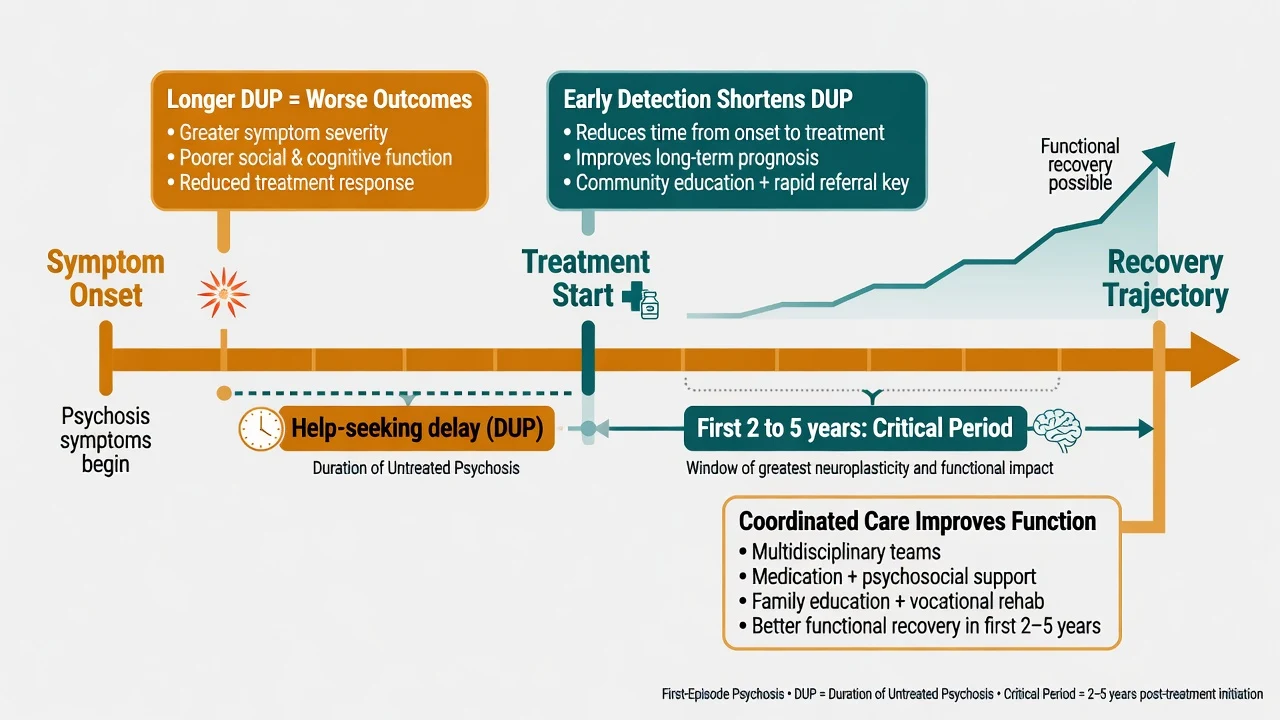
Duration of untreated psychosis (DUP) is the time from onset of frank psychotic symptoms to the start of adequate antipsychotic treatment (definitions vary slightly across studies). Duration of untreated illness (DUI) may include the prodrome. Longer DUP associates with poorer symptom and functional outcomes in systematic reviews — it is the modifiable lever that justifies early detection and early intervention orthodoxy.[1][2]
Critical period hypothesis (Birchwood framing). The first roughly 2–5 years after onset concentrate disability accumulation, suicide risk, and opportunity for intensive multi-element care. EIS models are built for this window, not for indefinite ultra-specialised care of every multi-episode patient.[3][5]
[19]Classification
Clinical high risk / UHR
- Attenuated or brief limited intermittent psychotic symptoms
- Most do not convert to frank psychosis
- Offer monitoring, substance advice, functional support
- Do not start antipsychotics routinely for CHR alone without specialist rationale
FEP service entry
- Clear psychotic symptoms needing treatment
- Provisional spectrum or affective formulation
- DUP clock stops when adequate treatment starts
- Multi-element care begins immediately
Evolving DSM-5-TR labels
- Brief psychotic: under 1 month with return to premorbid
- Schizophreniform: 1–6 months
- Schizophrenia: continuous signs at least 6 months including active phase
- Affective / substance / organic categories when criteria fit
What FEP is not
- Not synonymous with treatment-resistant schizophrenia
- Not a licence to skip organic work-up
- Not automatic lifelong high-dose polypharmacy
- Not a reason to abandon education or employment goals
ICD-11 note. Schizophrenia requires at least 1 month of symptoms; DSM-5-TR uses a 6-month continuous-signs threshold. State which manual you are using in multi-board answers.[19]
Epidemiology and risk factors
Headline FEP numbers
Incidence of non-affective psychosis clusters in late adolescence and early adulthood. Risk factors relevant at first presentation include family history, obstetric complications, urban upbringing, migration and social defeat, childhood adversity, and cannabis use — especially frequent high-potency THC products in youth. EU-GEI linked daily and high-potency cannabis use to variation in psychotic disorder incidence across Europe.[14]
TIPS early detection. Population early-detection strategies can shorten DUP and improve clinical presentation at entry compared with detection as usual — proof that systems, not only biology, move outcomes.[20]
Pathophysiology
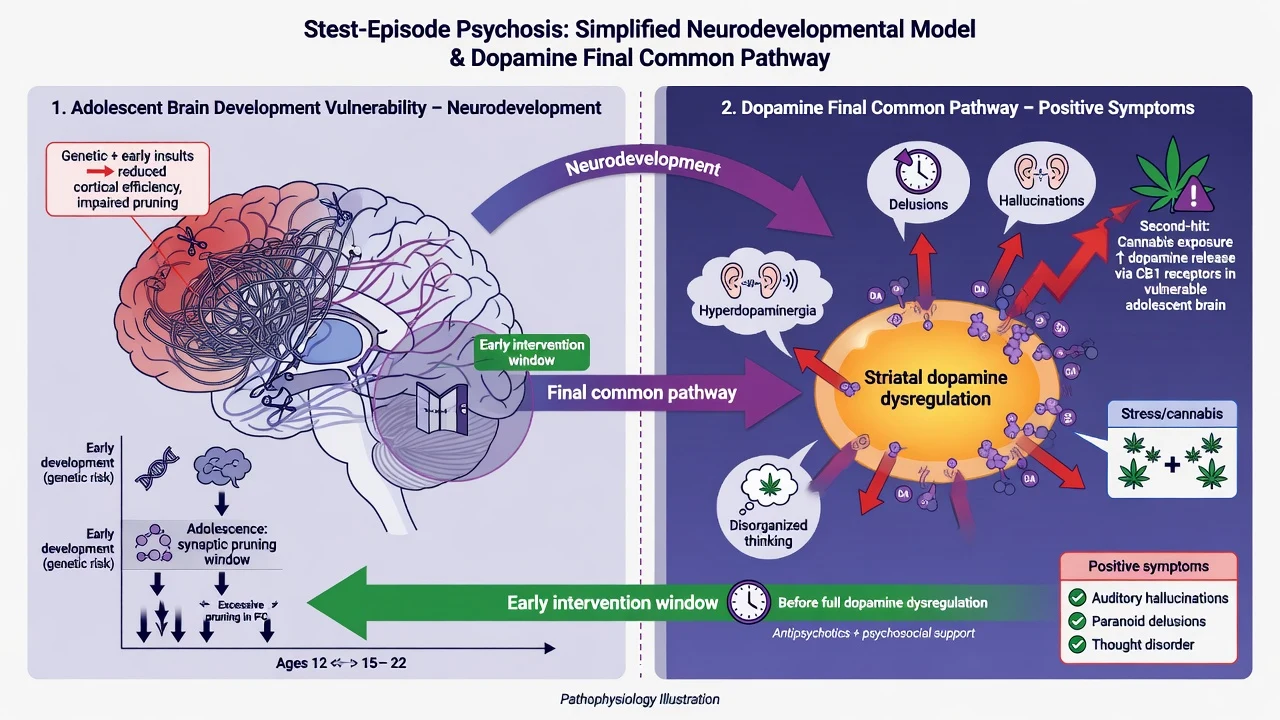
Dopamine hypothesis version III (Howes and Kapur). Upstream developmental, genetic and environmental factors converge on a final common pathway of striatal dopamine dysregulation. Excess presynaptic striatal dopamine synthesis and release links to positive symptoms and to the efficacy of D2 receptor blockade. Prefrontal dopaminergic hypofunction helps explain negative and cognitive symptoms that pure D2 blockade often fails to fix.[9]
Why FEP is dose-sensitive. First-episode patients often respond at lower antipsychotic doses and are more vulnerable to extrapyramidal and other adverse effects than multi-episode cohorts. EUFEST demonstrated effectiveness of several agents at relatively low first-episode dosing strategies in open randomised comparison.[7][8]
Cannabis as second hit. High-THC exposure is associated with increased incidence risk and, after onset, continued use predicts earlier relapse — dual-diagnosis work is pathophysiology-informed secondary prevention, not moral lecturing.[14][15]
Clinical presentation
Prodrome. Months of social withdrawal, falling academic or work performance, sleep disruption, mood change, attenuated unusual beliefs, and sometimes escalating cannabis. Not every prodrome converts; do not over-promise prediction.[19]
Frank FEP. Positive symptoms dominate the exam stem: persecutory or referential delusions, auditory verbal hallucinations (commentary, arguing, commands), formal thought disorder, passivity phenomena. Negative and cognitive deficits are often already present and predict function. Affective symptoms may signal affective psychosis or comorbidity — chronology matters.[19]
Atypical presentations examiners love. Late-onset first psychosis (intensify organic work-up), perinatal first presentation, high-functioning university student with preserved facade and hidden command content, culture-shaped delusional content that is still fixed and impairing, and substance-comorbid FEP where psychosis outlasts intoxication.[19]
Differential diagnosis
Win the differential on attention, tempo, physical signs, mood chronology, and course after abstinence — not on a shopping list.[19]
Delirium
- Inattention and fluctuation are core
- Medical illness, drugs, withdrawal
- Visual hallucinations more common
- Treat the cause first
Substance-induced
- Timeline locked to intoxication or withdrawal
- Methamphetamine, high-THC cannabis, synthetics
- May resolve with abstinence or unmask primary illness
- Urine screen supports never excludes
Affective psychosis
- Mood episode is primary and persistent
- Psychosis often mood-congruent (not absolute)
- Treat mood and psychosis together
- Schizoaffective needs psychosis without mood for at least 2 weeks
Organic / autoimmune
- Fever, seizure, dysautonomia, movement disorder
- NMDAR encephalitis pattern in young adults
- Late onset, HIV, syphilis, B12, thyroid, steroids
- Investigate before chronic labelling
Also keep OCD with poor insight, PTSD with dissociative phenomena, autism with atypical beliefs, and personality (schizotypal, paranoid, borderline) on the board.[19]
Clinical and bedside assessment
Structure every FEP assessment the same way examiners mark: safety, collateral, DUP, MSE, risk, substance, capacity/legal status, family, function and physical exam.[5][19]
- Safety and observations (including capillary glucose).
- Collateral — parents, partners, flatmates, GP, school.
- DUP calculation — date of first clear psychotic symptom to adequate treatment.
- Full MSE with quoted examples of delusion and hallucination content.
- Risk — suicide, self-harm, violence, vulnerability, neglect, absconding, weapons, childcare.
- Substance timeline with last use and potency/frequency.
- Capacity for the specific treatment decision; legal status under local Mental Health Act principles (least restrictive; do not invent foreign section numbers).
- Family system and carer burden.
- Function — study, work, self-care, housing.
- Physical examination with neurological attention when red flags fire.[19]
Investigations
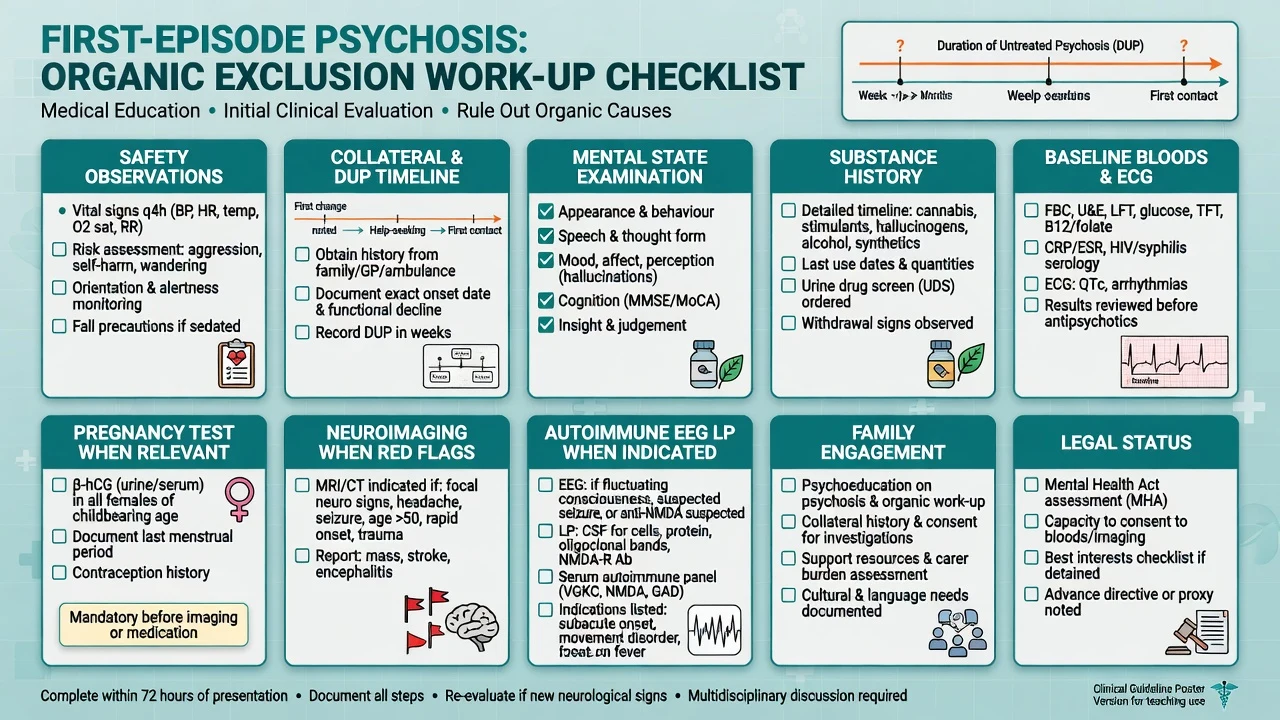
Imaging and special tests when red flags fire: atypical first episode, late onset, focal neurology, seizure, profound cognitive change, immunosuppression, suspected encephalitis (EEG, LP, autoimmune panel as directed). Urine drug screen supports the substance timeline but never excludes primary psychosis.[19]
Management — resuscitation of the acute crisis
De-escalate verbally; offer oral medication first; use intramuscular agents only when needed for safety; monitor airway, respiration, QTc and consciousness; never combine intramuscular olanzapine with a parenteral benzodiazepine; exclude hypoglycaemia and other organic drivers. Choose community EIS versus admission using risk, insight, support and medical need — least restrictive setting that is still safe.[19]
Management — definitive and stepwise
Early intervention multi-element care
OPUS (Denmark). Intensive early intervention (assertive outreach, family involvement, social skills) improved 1-year outcomes versus standard treatment; 5-year follow-up showed some attenuation of between-group differences after the intensive phase ended — an exam pearl about maintaining quality after the specialised window.[3][4]
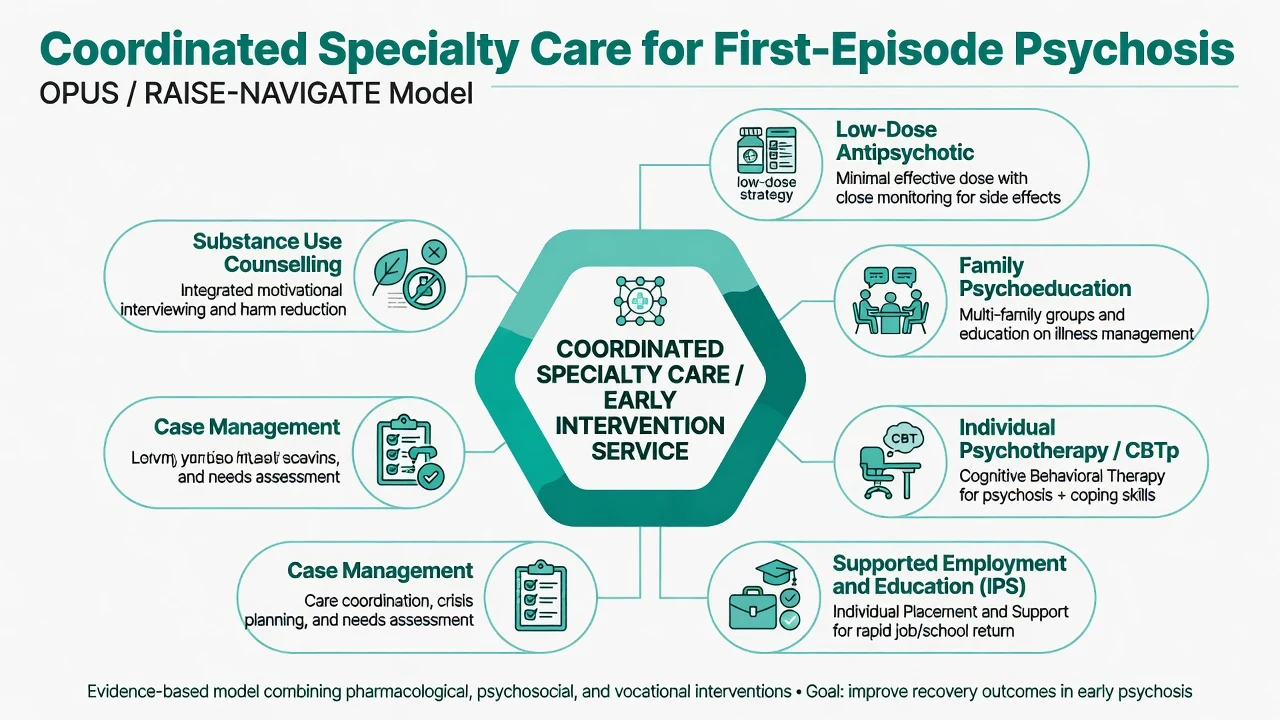
RAISE-ETP (NAVIGATE model, USA). Comprehensive coordinated specialty care improved quality of life and other outcomes versus community care as usual at 2 years in first-episode psychosis.[5]
Meta-analytic synthesis. Early intervention services outperform treatment as usual across multiple outcomes in early-phase psychosis — the case for specialised multi-element teams is not local fashion; it is evidence-based systems design.[6]
Core modules examiners expect you to name form part of the OPUS/RAISE multi-element package rather than medication alone.[5][6]
- Low-dose antipsychotic with monitoring
- Family psychoeducation / family intervention
- Individual psychological therapy access (including CBTp where available)
- Assertive case management / care coordination
- Substance use counselling (especially cannabis)
- Supported education and employment (IPS)
- Physical health monitoring
- Crisis and relapse plan[12][18]
Antipsychotic start doses in FEP
Start low, titrate to the minimum effective dose, and plan an adequate trial of roughly 4–6 weeks at a therapeutic dose with adherence support before declaring failure. Shared decision-making and side-effect education drive adherence more than paternalistic high dosing.[7][8][19]
| Agent (oral) | Typical FEP starting approach | Practical notes |
|---|---|---|
| Aripiprazole | 10 mg once daily (range often 5–15 mg) | Favourable metabolic profile; watch akathisia |
| Risperidone | 1–2 mg daily; titrate toward 2–4 mg | Prolactin and EPS risk rise with dose |
| Olanzapine | 5–10 mg at night | Effective; high metabolic burden — monitor hard |
| Amisulpride | Often 200–400 mg daily in FEP ranges | Prolactin; renal dosing awareness |
| Quetiapine | Higher doses needed for antipsychotic effect | Sedation; metabolic effects; not always first pick |
| Haloperidol | Low-dose strategies (often 1–4 mg) in FEP trials | EPS risk; still a legitimate option when used carefully |
| [7][8] |
Exact licensed ranges and product information vary by jurisdiction — state the agent, starting dose, titration plan, and monitoring, not a vague "start an atypical."[7][8][19]
Monitoring schedule (minimum). Baseline as above; early clinical review within days; metabolic recheck (weight, BMI, glucose/HbA1c, lipids, BP) at intervals such as 1 month, 3 months, then regularly; ECG when risk factors or QT-risk drugs; prolactin if symptoms or high-risk agent; EPS/akathisia every visit. Akathisia is frequently misread as agitation or anxiety — examine before automatic dose increases.[19]
Long-acting injectables (LAIs). Consider early when adherence is uncertain, insight is fragile, or the patient prefers not to take daily oral tablets. LAIs are adherence tools, not a substitute for true treatment-resistance pathways.[19]
Family work
Family intervention for schizophrenia-spectrum illness reduces relapse and hospitalisation risk in systematic review evidence. In FEP, family psychoeducation is not optional garnish: explain the illness model, early warning signs, communication patterns, and how to respond to non-adherence without criticism that raises expressed emotion.[12]
Substance — especially cannabis
Counsel frequency, potency and continuation. Continued cannabis after onset associates with higher relapse risk in observational FEP cohorts. Integrate motivational approaches with psychosis care; do not wait for perfect abstinence before treating psychosis.[15][14]
Vocational recovery
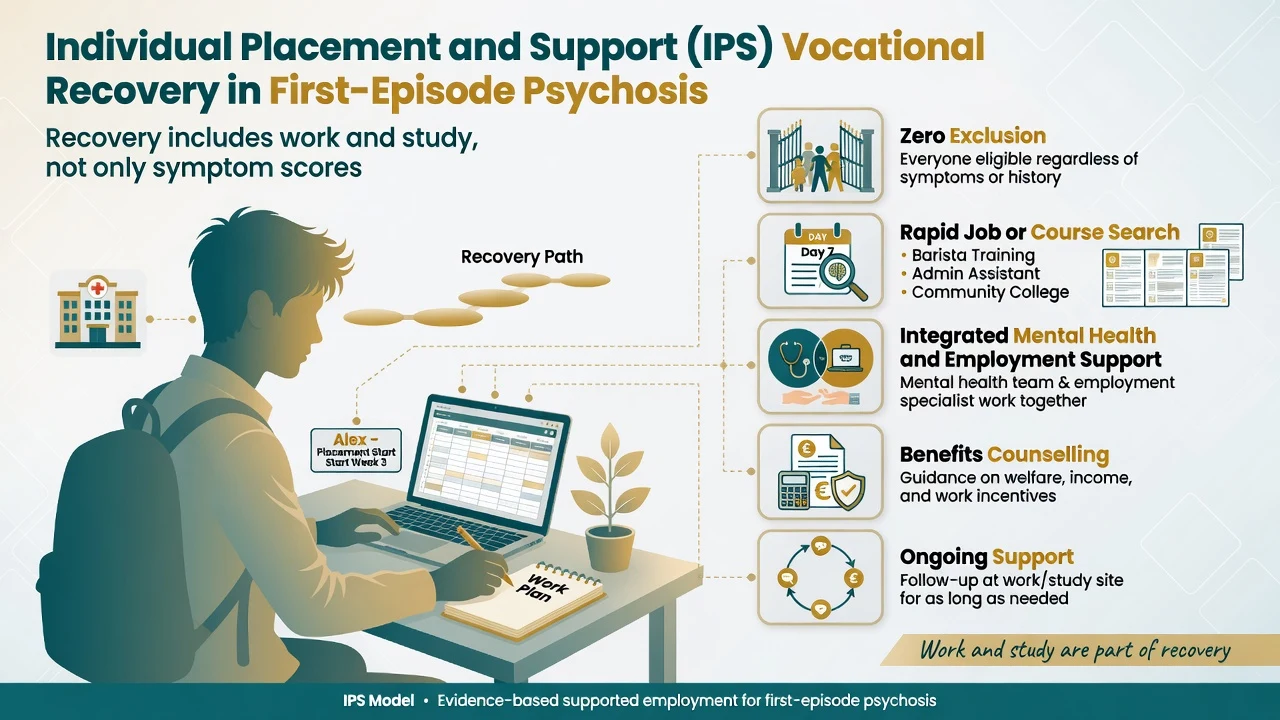
Individual Placement and Support (IPS) improved vocational recovery in a randomised trial of first-episode psychosis — zero exclusion, rapid job or course search, integrated mental health and employment support, and ongoing support. Recovery is measured in roles and function, not only PANSS points.[18]
Relapse prevention and maintenance duration
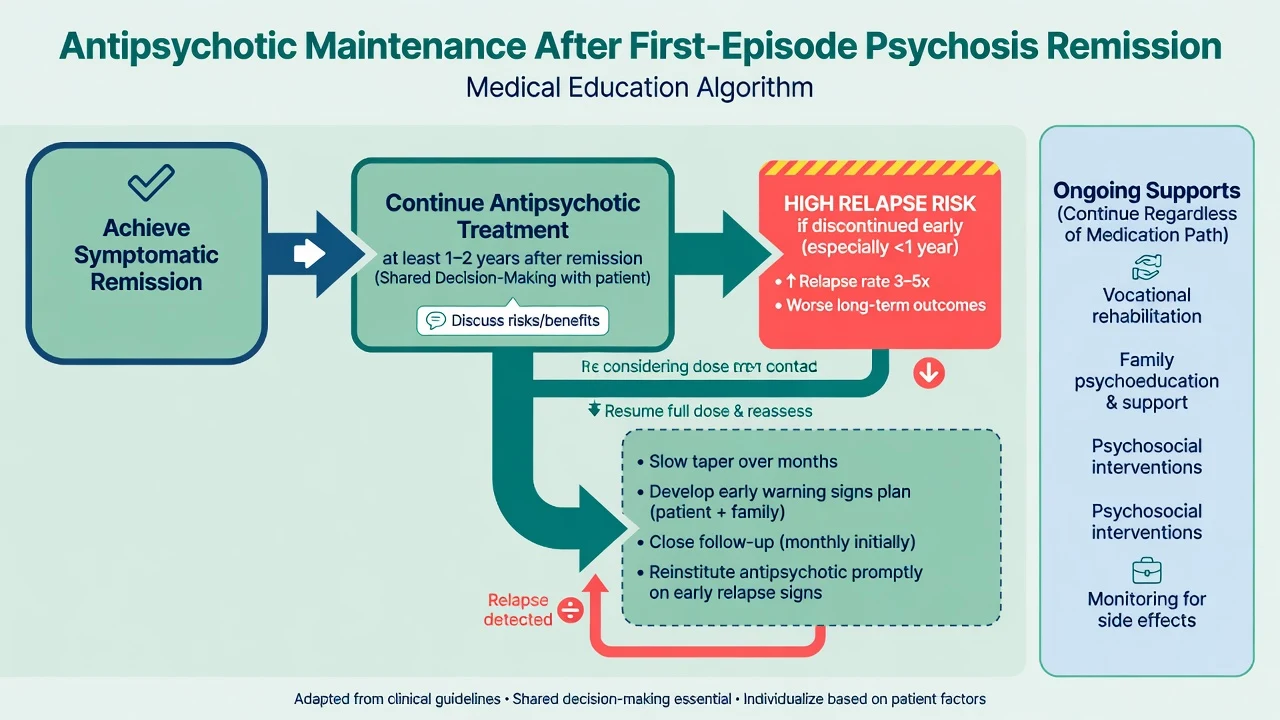
Antipsychotic maintenance substantially reduces relapse versus placebo across schizophrenia trials.[13] After a first episode, medication discontinuation carries high recurrence risk in systematic review data.[11] Relapse predictors after FEP response include medication non-adherence and persistent symptoms among other factors.[10][17]
Practical fellowship stance (align with RANZCP and peer guidelines): after first-episode remission, plan guided maintenance rather than unsupervised early stop.[19][11]
- After remission of a first episode, continue antipsychotic treatment for at least 1–2 years (longer if residual symptoms, prior relapse, high risk, or patient preference for security).[11][19]
- Any deprescribing is a planned experiment: slow taper, written early-warning plan, rapid reinstitution pathway, close follow-up.[11]
- Wunderink dose-reduction/discontinuation strategy showed complex long-term functional findings at 7 years and remains controversial — do not quote it as a licence for unsupervised early stop; use it to discuss trade-offs under specialist supervision.[16]
Specific subtypes and scenarios
Schizophrenia-spectrum FEP. Run the full EIS package; track duration toward schizophreniform versus schizophrenia thresholds; keep TRS/clozapine pathway ready if two adequate trials fail.[19]
Affective first-episode psychosis. Mood chronology and family history steer toward bipolar or depressive psychosis pathways; antipsychotics may still be needed acutely while mood stabilisers or antidepressants are chosen carefully.[19]
Cannabis-associated FEP. Dual formulation until course after reduced use clarifies primary versus substance-driven illness.[15]
Late-onset first presentation. Organic intensification is mandatory; do not copy-paste youth FEP algorithms without medical depth.[19]
Transition out of EIS. After typically 2–3 years of specialised care (service-dependent), step down to adult community care with a written relapse plan — OPUS long-term data remind you that gains can fade if intensity collapses abruptly.[4]
Complications and pitfalls
- Metabolic syndrome, diabetes, weight gain (especially olanzapine), QTc prolongation, EPS, tardive dyskinesia, hyperprolactinaemia, akathisia mislabelled as agitation.[19]
- Premature fatalism ("schizophrenia forever") destroying engagement.[19]
- Missing encephalitis or other organicity.[19]
- Declaring treatment failure after days at a token dose, or after non-adherence.[19]
- Endless antipsychotic switches without clozapine when TRRIP-style resistance criteria are met (hand off to spectrum/TRS topic).[19]
- Ignoring family and vocational domains while chasing dose numbers.[12][18]
- Early unsupervised antipsychotic stop after a first good remission.[11][17]
Prognosis and disposition
Better prognostic signals include shorter DUP, female sex, acute onset, mood features, good premorbid function, and early engagement with multi-element care. Poorer signals include long DUP, early onset in males, prominent primary negative symptoms, ongoing cannabis, and non-adherence.[1][2][17]
Remission is symptom control; recovery includes function, roles, relationships and personal meaning. Disposition: EIS versus inpatient, then community follow-up intensity matched to risk, with crisis contacts and family involved under privacy law.[5][18]
Special populations
Youth and students. Preserve education pathways; involve family without infantilising the young adult; address online delusional content and peer substance culture.[18]
Perinatal. Urgent joint perinatal psychiatry; risk-benefit of antipsychotics; mother-infant bonding and safeguarding.[19]
Intellectual disability or autism. Adapted communication; avoid diagnostic overshadowing; careful capacity assessment.[19]
Indigenous and culturally diverse families. Cultural formulation, interpreter use, family structure respect, and awareness that content of beliefs is culturally shaped while form (conviction, distress, impairment) remains clinical.[19]
Older adult late-onset. Organic first; lower starting doses; fall and QTc risk.[19]
Evidence, guidelines and regional differences
RANZCP schizophrenia and related disorders guidance emphasises comprehensive care, early intervention principles, physical health monitoring, family involvement, and thoughtful maintenance after first episode. Local EIS branding varies by state and district health service — the multi-element principles travel even when the logo does not.[19]
Landmark list to name in viva: Marshall and Perkins (DUP), TIPS (early detection), OPUS, RAISE-ETP, Correll EIS meta-analysis, EUFEST, Pharoah family intervention, Leucht maintenance meta-analysis, Zipursky discontinuation risk, Wunderink dose-reduction controversy, Di Forti/Schoeler cannabis, Killackey IPS.[1][2][3][5][6][18]
Exam pearls
[5] [11] [18]RECOVER
Self-test: 19-year-old with 4-month DUP and nightly cannabis
Working pathway: FEP with dual substance formulation. Baseline bloods and ECG, EIS referral, shared-decision low-dose antipsychotic (e.g. aripiprazole 10 mg daily), family psychoeducation, cannabis motivational work, safety plan, IPS or education support. State provisional diagnosis (not lifelong schizophrenia on day one). If two adequate trials fail later, escalate toward clozapine pathway rather than endless polypharmacy.[5][15][19]
References
- [1]Marshall M, Lewis S, Lockwood A, et al. Association between duration of untreated psychosis and outcome in cohorts of first-episode patients: a systematic review Arch Gen Psychiatry, 2005.PMID 16143729
- [2]Perkins DO, Gu H, Boteva K, et al. Relationship between duration of untreated psychosis and outcome in first-episode schizophrenia: a critical review and meta-analysis Am J Psychiatry, 2005.PMID 16199825
- [3]Petersen L, Nordentoft M, Jeppesen P, et al. Improving 1-year outcome in first-episode psychosis: OPUS trial Br J Psychiatry Suppl, 2005.PMID 16055817
- [4]Bertelsen M, Jeppesen P, Petersen L, et al. Five-year follow-up of a randomized multicenter trial of intensive early intervention vs standard treatment for patients with a first episode of psychotic illness: the OPUS trial Arch Gen Psychiatry, 2008.PMID 18606949
- [5]Kane JM, Robinson DG, Schooler NR, et al. Comprehensive Versus Usual Community Care for First-Episode Psychosis: 2-Year Outcomes From the NIMH RAISE Early Treatment Program Am J Psychiatry, 2016.PMID 26481174
- [6]Correll CU, Galling B, Pawar A, et al. Comparison of Early Intervention Services vs Treatment as Usual for Early-Phase Psychosis: A Systematic Review, Meta-analysis, and Meta-regression JAMA Psychiatry, 2018.PMID 29800949
- [7]Kahn RS, Fleischhacker WW, Boter H, et al. Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomised clinical trial Lancet, 2008.PMID 18374841
- [8]Gardner DM, Murphy AL, O'Donnell H, et al. International consensus study of antipsychotic dosing Am J Psychiatry, 2010.PMID 20360319
- [9]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164
- [10]Robinson D, Woerner MG, Alvir JM, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder Arch Gen Psychiatry, 1999.PMID 10078501
- [11]Zipursky RB, Menezes NM, Streiner DL Risk of symptom recurrence with medication discontinuation in first-episode psychosis: a systematic review Schizophr Res, 2014.PMID 23972821
- [12]Pharoah F, Mari J, Rathbone J, et al. Family intervention for schizophrenia Cochrane Database Syst Rev, 2010.PMID 21154340
- [13]Leucht S, Tardy M, Komossa K, et al. Antipsychotic drugs versus placebo for relapse prevention in schizophrenia: a systematic review and meta-analysis Lancet, 2012.PMID 22560607
- [14]Di Forti M, Quattrone D, Freeman TP, et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study Lancet Psychiatry, 2019.PMID 30902669
- [15]Schoeler T, Petros N, Di Forti M, et al. Effects of continuation, frequency, and type of cannabis use on relapse in the first 2 years after onset of psychosis: an observational study Lancet Psychiatry, 2016.PMID 27567467
- [16]Wunderink L, Nieboer RM, Wiersma D, et al. Recovery in remitted first-episode psychosis at 7 years of follow-up of an early dose reduction/discontinuation or maintenance treatment strategy: long-term follow-up of a 2-year randomized clinical trial JAMA Psychiatry, 2013.PMID 23824214
- [17]Alvarez-Jimenez M, Priede A, Hetrick SE, et al. Risk factors for relapse following treatment for first episode psychosis: a systematic review and meta-analysis of longitudinal studies Schizophr Res, 2012.PMID 22658527
- [18]Killackey E, Allott K, Jackson HJ, et al. Individual placement and support for vocational recovery in first-episode psychosis: randomised controlled trial Br J Psychiatry, 2019.PMID 30251616
- [19]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [20]Melle I, Larsen TK, Haahr U, et al. Reducing the duration of untreated first-episode psychosis: effects on clinical presentation Arch Gen Psychiatry, 2004.PMID 14757590