Psych · General adult psychiatry
Functional neurological symptom disorder (conversion)
Also known as Functional neurological disorder · FND · FNSD · Conversion disorder · Functional neurological symptom disorder · Dissociative neurological symptom disorder · Functional seizures · Dissociative seizures · PNES · Functional movement disorder
Exam-exhaustive fellowship reference on functional neurological symptom disorder (conversion/FND) — DSM-5-TR and ICD-11 nosology, positive rule-in signs, predictive processing and agency models, FND clinic pathways, specialist physiotherapy, CBT for functional seizures (CODES/LaFrance), pejorative-language avoidance, prognosis, and exam discriminators. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship examiners no longer accept “medically unexplained after negative MRI, so conversion.” They want a registrar who can name positive signs, frame FND as a network/function disorder, deliver a non-stigmatising explanation, and activate physio and psychological pathways while keeping dual pathology and risk in view.[1][3][19]
Overview and definition
Functional neurological symptom disorder (FNSD), commonly called functional neurological disorder (FND) and historically conversion disorder, describes clinically recognisable alterations of voluntary motor or sensory function — weakness, movement disorders, sensory loss, speech change, swallowing symptoms, or attacks resembling epilepsy — that are incompatible with recognised neurological disease mechanisms yet cause genuine distress and disability.[1][2][3]
Modern teaching rejects mind–body dualism. Symptoms are real and involuntary from the patient’s perspective; they arise from disordered nervous-system function (attention, prediction, agency, motor planning) rather than a classic structural lesion explaining the phenotype.[1][7][8]
Classification and diagnostic criteria
DSM-5-TR
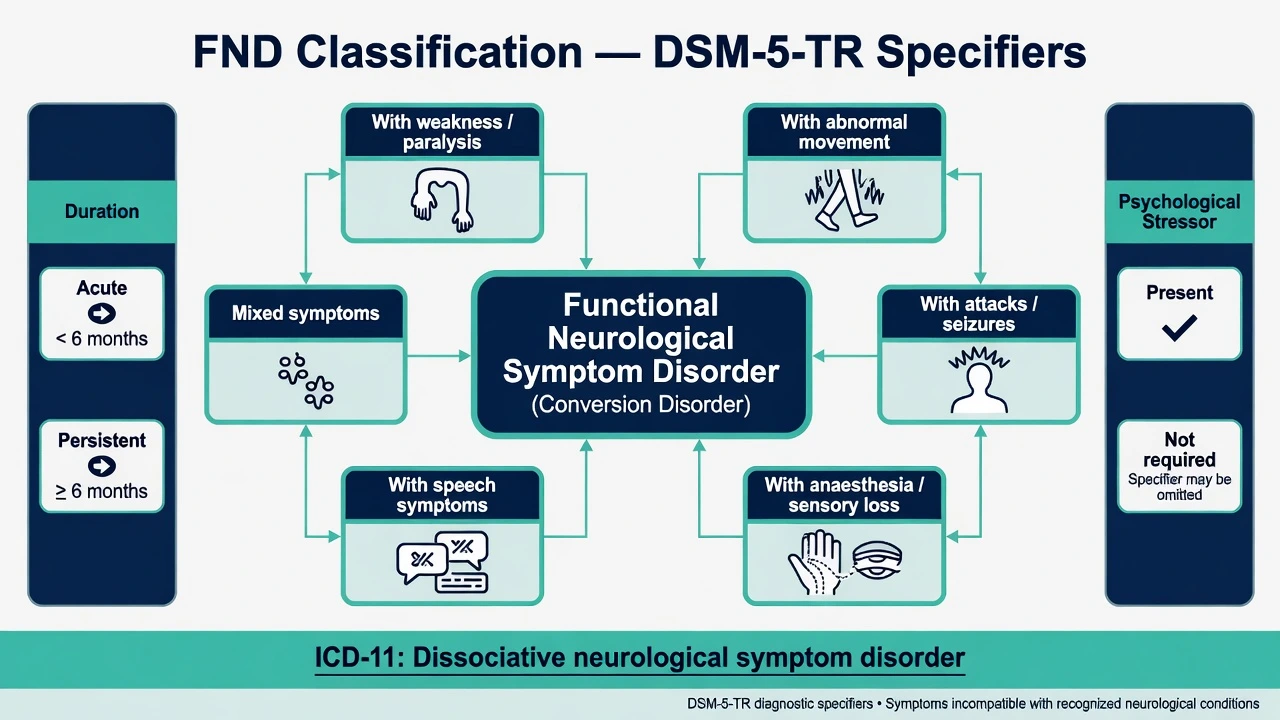
Core requirements (exam paraphrase): one or more symptoms of altered voluntary motor or sensory function; clinical findings provide evidence of incompatibility between the symptom and recognised neurological or medical conditions; the symptom is not better explained by another medical or mental disorder; and the symptom or deficit causes clinically significant distress or impairment or warrants medical evaluation.[1][3]
Symptom-type specifiers include weakness or paralysis, abnormal movement, swallowing symptoms, speech symptoms, attacks or seizures, anaesthesia or sensory loss, special sensory symptoms, or mixed symptoms.[1][3]
Additional specifiers: acute episode (less than 6 months) versus persistent (6 months or more); with psychological stressor versus without psychological stressor. Critically for exams: a stressor is not required for diagnosis.[1][12]
ICD-11
ICD-11 places related presentations under dissociative neurological symptom disorder, reflecting international nosology that links motor/sensory functional symptoms to dissociative frameworks while clinical practice still uses FND language widely.[2][3]
Historical language
Terms such as hysteria, conversion, psychogenic, and non-organic appear in older literature. Prefer functional neurological disorder / functional seizures / functional movement disorder in clinical speech and documentation; avoid pejorative “pseudo-” framing that implies fabrication.[1][4][19]
Epidemiology and risk
In large Scottish neurology outpatient series, roughly one-third of new patients were assessed as having symptoms largely or completely unexplained by organic disease, and new alternative neurological diagnoses rarely appeared later solely to overturn those assessments when diagnosis was careful.[9]
FND presentations are among the commonest reasons for neurology referral after headache in many services; epidemiology is summarised in the Handbook of Clinical Neurology chapter by Carson and Lehn, with phenotype-specific incidence and prevalence varying by setting and case definition.[11]
Patients with unexplained neurological symptoms show high rates of disability, psychological distress, and unemployment, often comparable to or exceeding those with many established neurological diseases.[10]
Stressful life events and maltreatment are associated with conversion/FND in meta-analysis, but they are neither necessary nor sufficient; many patients have no clear trauma narrative, and many people with trauma never develop FND.[12]
Pathophysiology and mechanisms
Predictive coding
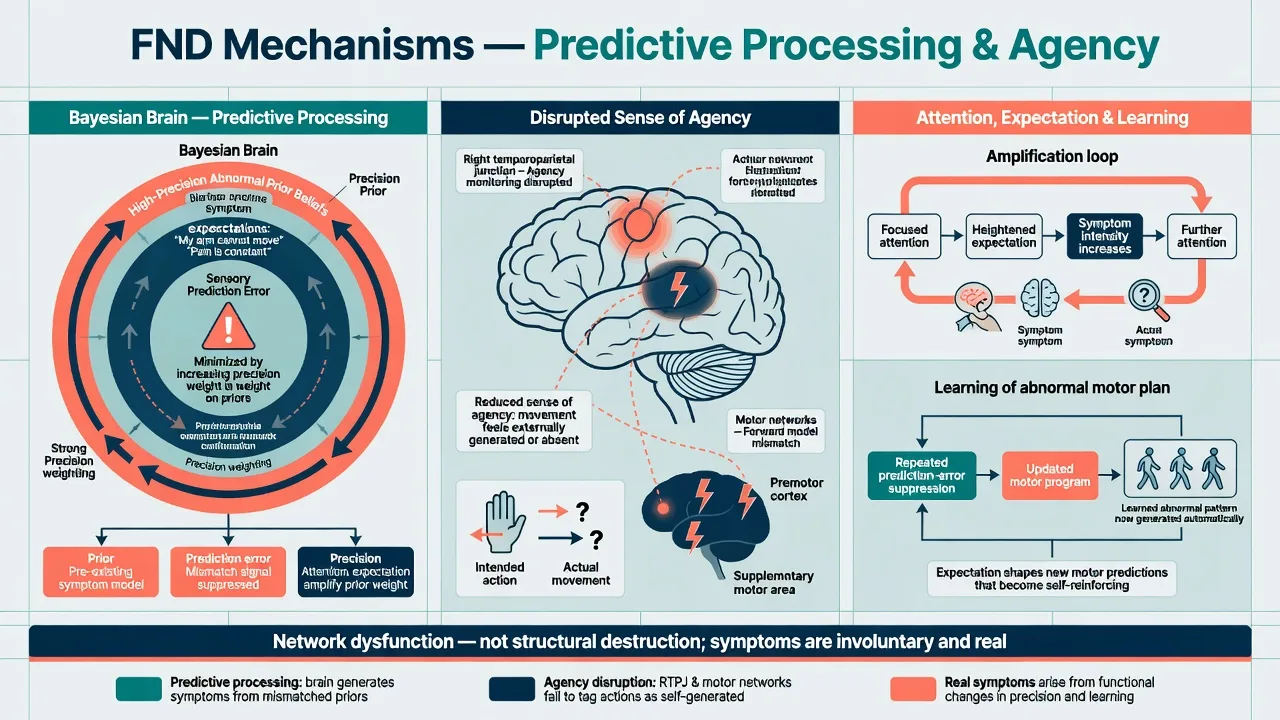
Edwards and colleagues’ Bayesian account frames functional symptoms as disorders of inference: abnormally strong prior beliefs about symptom states, weighted with high precision, overwhelm contradictory sensory evidence and generate the experienced phenotype (for example “my leg will not move”).[7]
Sense of agency
Patients experience movements as involuntary despite physiology that can look voluntary. Resting-state fMRI work in functional movement disorder shows altered connectivity linked to impaired self-agency, including right temporoparietal junction–related networks.[8]
Shared mechanisms across subtypes
Hallett and colleagues synthesise shared mechanisms across functional seizures, functional movement disorders, persistent postural-perceptual dizziness (PPPD), and functional cognitive disorder, supporting a unified FND construct with phenotype-specific expression.[2]
Psychological processes (attention, expectation, dissociation, learned avoidance) and social context (iatrogenic language, disability systems) interact with these neural mechanisms — a biopsychosocial model, not pure Freudian conversion of repressed conflict as the sole explanation.[1][7][12]
Clinical presentation
Functional weakness
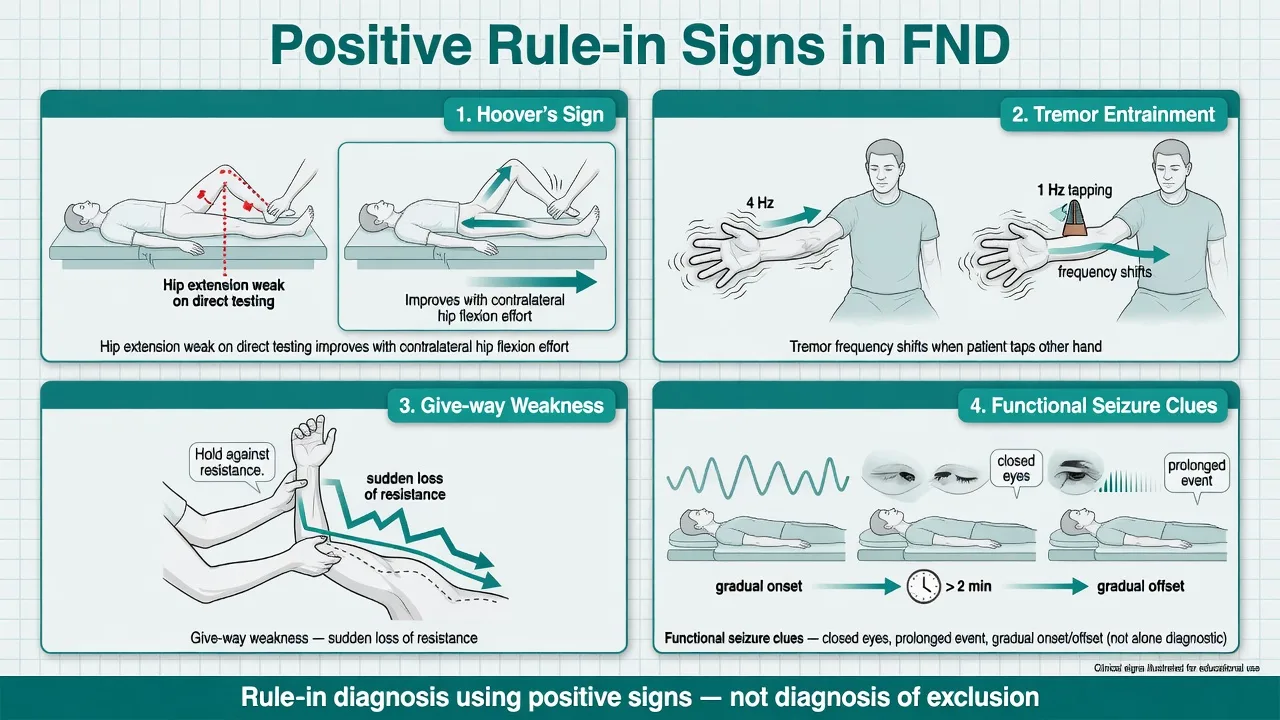
Typically sudden onset, often after injury, panic, or medical encounter; inconsistency between formal power testing and automatic movement; Hoover’s sign (hip extension weak on direct testing improves with contralateral hip flexion effort); hip abductor sign; give-way weakness; collapsing gait patterns that do not map to a single upper-motor-neurone lesion.[5][6][4]
Functional movement disorders
Tremor that is variable, distractible, and entrainable to a contralateral paced movement; functional dystonia often fixed (inverted ankle, clenched fist) after minor trauma; functional myoclonus and gait disorders with characteristic positive signs.[1][5]
Functional / dissociative seizures
Also called psychogenic non-epileptic seizures (PNES) in older literature. Clues include prolonged events, closed eyes, asynchronous thrashing, waxing/waning course, and rapid recovery in some patients — no single bedside feature is pathognomonic; dual epilepsy and FND can coexist. When uncertainty remains, video-EEG is the reference standard for seizure classification.[2][15][16]
Sensory, speech, and mixed
Non-anatomical sensory loss, functional dysphonia or stuttering, swallowing symptoms, and mixed motor-sensory presentations are common; always screen for comorbidity and dual disease.[1][2]
Differential diagnosis
FND
- Positive rule-in signs
- Incongruence with disease pathways
- Symptoms experienced as involuntary
- Treat with explanation + MDT rehab/psych
Structural / disease neurology
- UMN/LMN or seizure patterns fit disease
- Imaging/EEG may confirm
- May coexist with FND
- Disease-specific therapy
Factitious / malingering
- Intentional production (evidence required)
- Secondary gain or sick role motivations
- Rare as pure explanation of FND clinics
- Not default when signs positive
Somatic symptom disorder
- Excessive health anxiety/behaviour around symptoms
- May overlap with FND
- Focus is cognition/behaviour about illness
- Different treatment emphasis
Always keep stroke, MS, myasthenia, GBS, epilepsy, movement-disorder disease, catatonia, and autoimmune encephalitis active when red flags appear. Positive FND signs support FND; they do not license skipping emergency pathways when the presentation could still be stroke or status.[3][19]
Assessment
Structure the history around onset, triggers, fluctuations, attention effects, prior functional symptoms, injury, panic, and health-system contacts. Perform a full neurological exam aiming for positive signs, not only “normal power.” Show selected signs to the patient when it helps understanding.[4][5][6]
Psychiatric assessment: mood, anxiety, PTSD, dissociation, personality, substance use, social stressors, suicide and self-harm risk, driving and occupational safety, capacity, and cultural explanatory models — without forcing a conversion narrative.[3][12][19]
Investigations
Investigations are hypothesis-driven. Endless negative tests do not “prove” FND and may reinforce illness threat. Use MRI, EEG, labs, and other tests when differential diagnosis demands them or dual pathology is plausible. Video-EEG for uncertain seizure-like events remains essential in many patients.[1][3][16]
Acute and emergency management
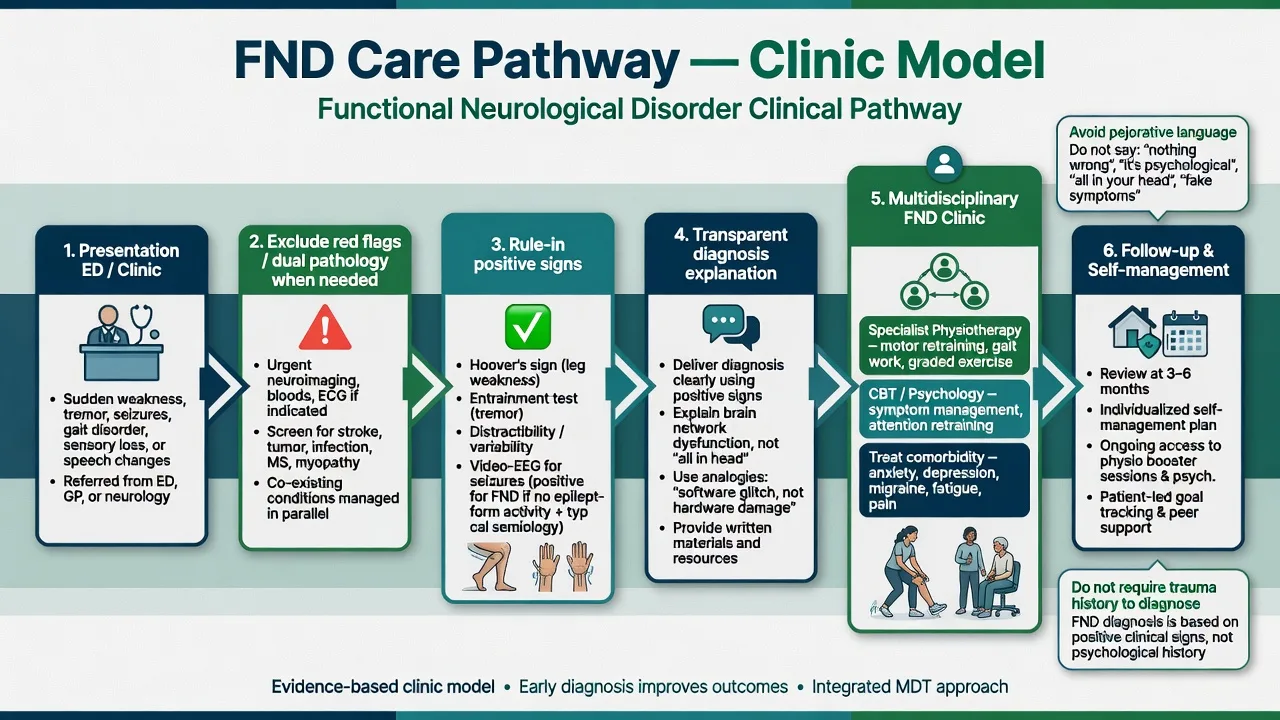
For acute weakness presentations that could be stroke, complete local stroke pathways first. Once red flags are addressed, early transparent diagnosis reduces iatrogenic harm from repeated imaging, unnecessary operations, and antiepileptic escalation.[3][4]
Definitive management and the FND clinic model
Diagnostic explanation as treatment
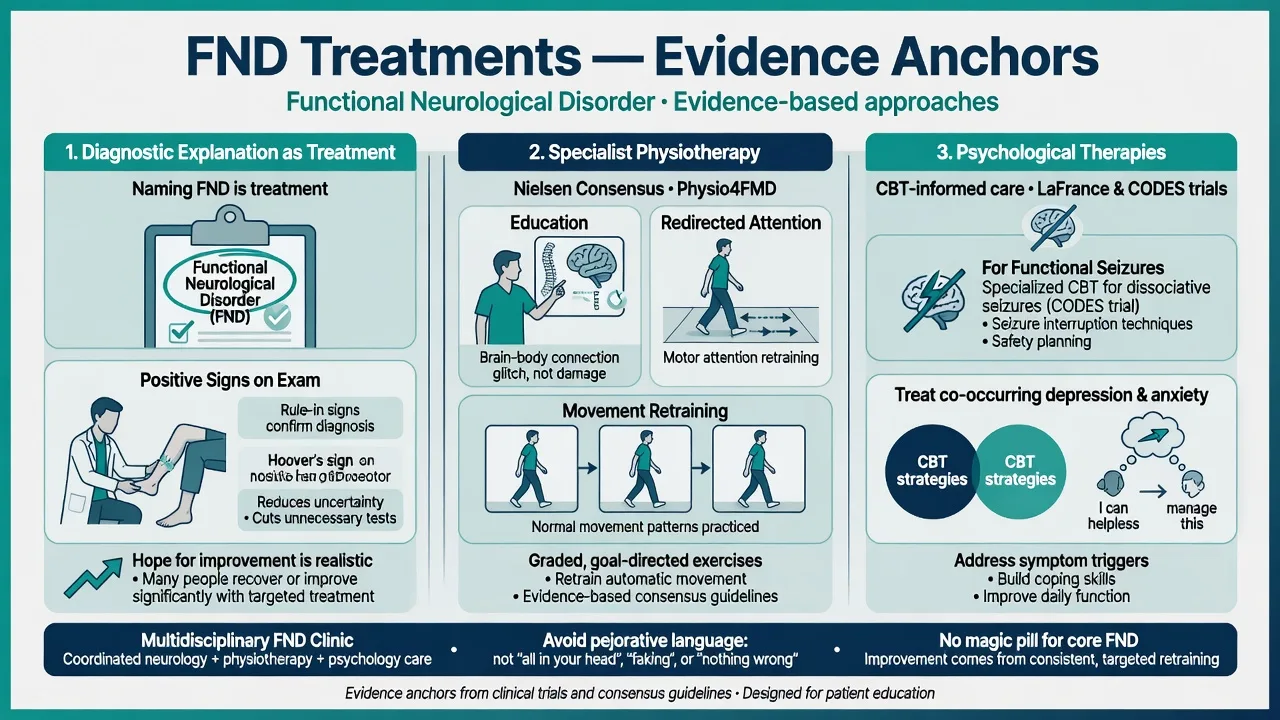
Stone, Aybek, Perez and colleagues emphasise structured explanation: name the condition (FND / functional seizures), explain how you know using positive signs, state that symptoms are real and not invented, emphasise potential for improvement because pathways are not permanently destroyed, and provide written information and a clear next step.[3][4][19]
Specialist physiotherapy
Nielsen consensus recommendations place physiotherapy centrally for functional motor disorders: education, reduce self-directed attention on the symptom, retraining of automatic movement, and self-management in a non-judgemental frame.[13]
Physio4FMD (England and Scotland) is a pragmatic multicentre phase 3 RCT of specialist physiotherapy for functional motor disorder versus treatment as usual — know the trial name, setting, and that specialist physio is a core evidence-linked intervention, while interpreting primary and secondary outcomes carefully from the paper rather than sloganising results.[14]
Psychological therapies for functional seizures
LaFrance’s multicentre pilot RCT supported CBT-informed psychotherapy for PNES with seizure reduction and broader clinical gains in the CBT arm.[15]
CODES (Goldstein et al., Lancet Psychiatry 2020) compared dissociative-seizure-specific CBT plus standardised medical care versus standardised medical care alone. Examiners expect honesty: the primary seizure-frequency endpoint and secondary/quality-of-life findings must be described accurately from the trial — CBT remains a key evidence-based psychological approach, and standardised diagnostic explanation and neurology/psychiatry care matter for all arms.[16]
Pharmacotherapy
There is no disease-modifying drug for core FND motor phenotypes. Treat comorbid depression, anxiety, PTSD, and migraine with standard agents and monitoring. Do not use antipsychotics to “stop conversion.” After clear functional seizures without epilepsy, plan supervised AED withdrawal when appropriate.[1][3][15]
Multidisciplinary clinic
Ideal care is an FND clinic model: neurology (or neuropsychiatry) for diagnosis and dual-pathology surveillance; physiotherapy (and OT/SLP as needed); psychology/psychiatry for CBT-informed care and comorbidity; shared non-pejorative language across the team.[1][3][13]
ANZ / FRANZCP: Use local CL neuropsychiatry and neurology pathways; document capacity and Mental Health Act issues only when concurrent psychiatric risk or lack of capacity arises — FND itself is usually voluntary care. Align language with modern FND education resources.[3][19]
UK / MRCPsych: NICE-oriented FND recognition and stepped MDT care; CASC communication stations reward Stone-style explanation and avoidance of pejorative terms.[4][19]
US / ABPN: DSM-5-TR criteria language; FND clinics in academic centres; PNES pathways with epilepsy monitoring units.[1][15]
Prognosis and disposition
Untreated or late-recognised FND often has a guarded prognosis, with many patients still symptomatic at follow-up in systematic reviews.[17]
In a 14-year case-control study of functional limb weakness, misdiagnosis was rare, symptoms frequently persisted, disability remained substantial, and mortality was higher than expected — underscoring that FND is not trivial and needs active management rather than discharge with “normal scan.”[18]
Favourable factors commonly cited include early diagnosis, acceptance of the FND formulation, shorter symptom duration, and a collaborative therapeutic alliance; chronic pain, multi-symptom burden, and entrenched disability systems worsen outlook.[17][18]
Special populations
Children and adolescents: family-inclusive care, school reintegration, avoid blaming the child; rule-in signs still apply with developmental adaptation.[3][19]
Older adults: higher dual-pathology risk; careful stroke and neurodegenerative exclusion.[3]
Pregnancy and perinatal: differentiate functional seizures from eclampsia and epilepsy; medication choices for comorbidity follow usual perinatal psychopharmacology principles.[3]
Cultural contexts: collaborate with the patient’s explanatory model; do not pathologise culturally sanctioned trance experiences as FND by default.[4]
Complications and pitfalls
Other high-yield traps: diagnosis of exclusion only; requiring trauma; defaulting to malingering; missing dual disease; iatrogenic AED burden; unnecessary surgery; therapeutic nihilism.[1][3][18]
Evidence and guidelines
Core reviews: Espay et al. JAMA Neurology 2018; Hallett et al. Lancet Neurology 2022; Aybek and Perez BMJ 2022; Stone et al. BMJ 2020; Bennett et al. practical review 2021.[1][2][3][4][19]
Treatment anchors: Nielsen physiotherapy consensus 2015; Physio4FMD 2024; LaFrance 2014; CODES 2020.[13][14][15][16]
Exam pearls
- Rule-in with Hoover’s, entrainment, distractibility, and carefully interpreted seizure signs — not “normal MRI equals FND.”[5][6]
- Stressor not required.[1][12]
- FND ≠ feigning; malingering needs separate evidence.[1][4]
- Name Physio4FMD, CODES, and LaFrance trials honestly.[14][16][15]
- Long-term data: expert FND diagnosis is usually stable; disability can persist — treat actively.[18]
- CASC: structure, empathy, plain language, positive-sign demonstration concept, written info, follow-up plan.[4]
One-page summary
FND is a common, disabling, potentially reversible neuropsychiatric condition diagnosed by positive signs and treated by explanation + specialist physiotherapy + psychological therapies + comorbidity care inside a respectful multidisciplinary clinic. Drop pejorative language, do not demand trauma, protect against dual pathology and iatrogenic harm, and keep hope realistic rather than fatalistic.[1][3][13][16]
References
- [1]Espay AJ, Aybek S, Carson A, et al. Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders JAMA Neurol, 2018.PMID 29868890
- [2]Hallett M, Aybek S, Dworetzky BA, et al. Functional neurological disorder: new subtypes and shared mechanisms Lancet Neurol, 2022.PMID 35430029
- [3]Aybek S, Perez DL Diagnosis and management of functional neurological disorder BMJ, 2022.PMID 35074803
- [4]Stone J, Burton C, Carson A Recognising and explaining functional neurological disorder BMJ, 2020.PMID 33087335
- [5]Daum C, Hubschmid M, Aybek S The value of 'positive' clinical signs for weakness, sensory and gait disorders in conversion disorder: a systematic and narrative review J Neurol Neurosurg Psychiatry, 2014.PMID 23467417
- [6]Daum C, Gheorghita F, Spatola M, et al. Interobserver agreement and validity of bedside 'positive signs' for functional weakness, sensory and gait disorders in conversion disorder: a pilot study J Neurol Neurosurg Psychiatry, 2015.PMID 24994927
- [7]Edwards MJ, Adams RA, Brown H, Pareés I, Friston KJ A Bayesian account of 'hysteria' Brain, 2012.PMID 22641838
- [8]Maurer CW, LaFaver K, Ameli R, et al. Impaired self-agency in functional movement disorders: A resting-state fMRI study Neurology, 2016.PMID 27385746
- [9]Stone J, Carson A, Duncan R, et al. Symptoms 'unexplained by organic disease' in 1144 new neurology out-patients: how often does the diagnosis change at follow-up? Brain, 2009.PMID 19737842
- [10]Carson A, Stone J, Hibberd C, et al. Disability, distress and unemployment in neurology outpatients with symptoms 'unexplained by organic disease' J Neurol Neurosurg Psychiatry, 2011.PMID 21257981
- [11]Carson A, Lehn A Epidemiology Handb Clin Neurol, 2016.PMID 27719864
- [12]Ludwig L, Pasman JA, Nicholson T, et al. Stressful life events and maltreatment in conversion (functional neurological) disorder: systematic review and meta-analysis of case-control studies Lancet Psychiatry, 2018.PMID 29526521
- [13]Nielsen G, Stone J, Matthews A, et al. Physiotherapy for functional motor disorders: a consensus recommendation J Neurol Neurosurg Psychiatry, 2015.PMID 25433033
- [14]Nielsen G, Stone J, Lee TC, et al. Specialist physiotherapy for functional motor disorder in England and Scotland (Physio4FMD): a pragmatic, multicentre, phase 3 randomised controlled trial Lancet Neurol, 2024.PMID 38768621
- [15]LaFrance WC Jr, Baird GL, Barry JJ, et al. Multicenter pilot treatment trial for psychogenic nonepileptic seizures: a randomized clinical trial JAMA Psychiatry, 2014.PMID 24989152
- [16]Goldstein LH, Robinson EJ, Mellers JDC, et al. Cognitive behavioural therapy for adults with dissociative seizures (CODES): a pragmatic, multicentre, randomised controlled trial Lancet Psychiatry, 2020.PMID 32445688
- [17]Gelauff J, Stone J Prognosis of functional neurologic disorders Handb Clin Neurol, 2016.PMID 27719869
- [18]Gelauff JM, Carson A, Ludwig L, Tijssen MAJ, Stone J The prognosis of functional limb weakness: a 14-year case-control study Brain, 2019.PMID 31167232
- [19]Bennett K, Diamond C, Hoeritzauer I, et al. A practical review of functional neurological disorder (FND) for the general physician Clin Med (Lond), 2021.PMID 33479065