Psych · General adult psychiatry — anxiety disorders
Generalised anxiety disorder
Also known as GAD · Generalized anxiety disorder · Free-floating anxiety · Chronic worry disorder · Anxiety neurosis (historical)
Exam-exhaustive fellowship reference on generalised anxiety disorder — DSM-5-TR and ICD-11 criteria; epidemiology and burden; neurobiology and worry models; differentials; GAD-7 and HAM-A; CBT; SSRI/SNRI dosing; pregabalin and buspirone; benzodiazepine cautions; depression comorbidity; NICE/Canadian/WFSBP/ANZ stepped care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Generalised anxiety disorder (GAD) is a high-volume general adult topic that appears as “worried well” stems, primary-care somatisation, and comorbidity with depression. FRANZCP MEQs demand criteria, organic exclusion, a named drug with dose, and CBT ingredients. MRCPsych CASC tests explanation of diagnosis and medication without colluding with endless benzodiazepines. ABPN items test GAD-7 bands, SSRI versus pregabalin evidence, and duration thresholds. This topic is written so a candidate who has read nothing else can answer those questions at consultant depth.[1][3][18]
Overview and definition
GAD is a syndrome of excessive anxiety and worry occurring more days than not for a prolonged period, about multiple events or activities, that the person finds difficult to control, accompanied by a cluster of associated symptoms and clinically significant distress or impairment — after substance effects, medical mimics and competing mental disorders have been reasonably excluded. It is not ordinary situational worry, and it is not diagnosed by a blood test or a single panic attack.[3]
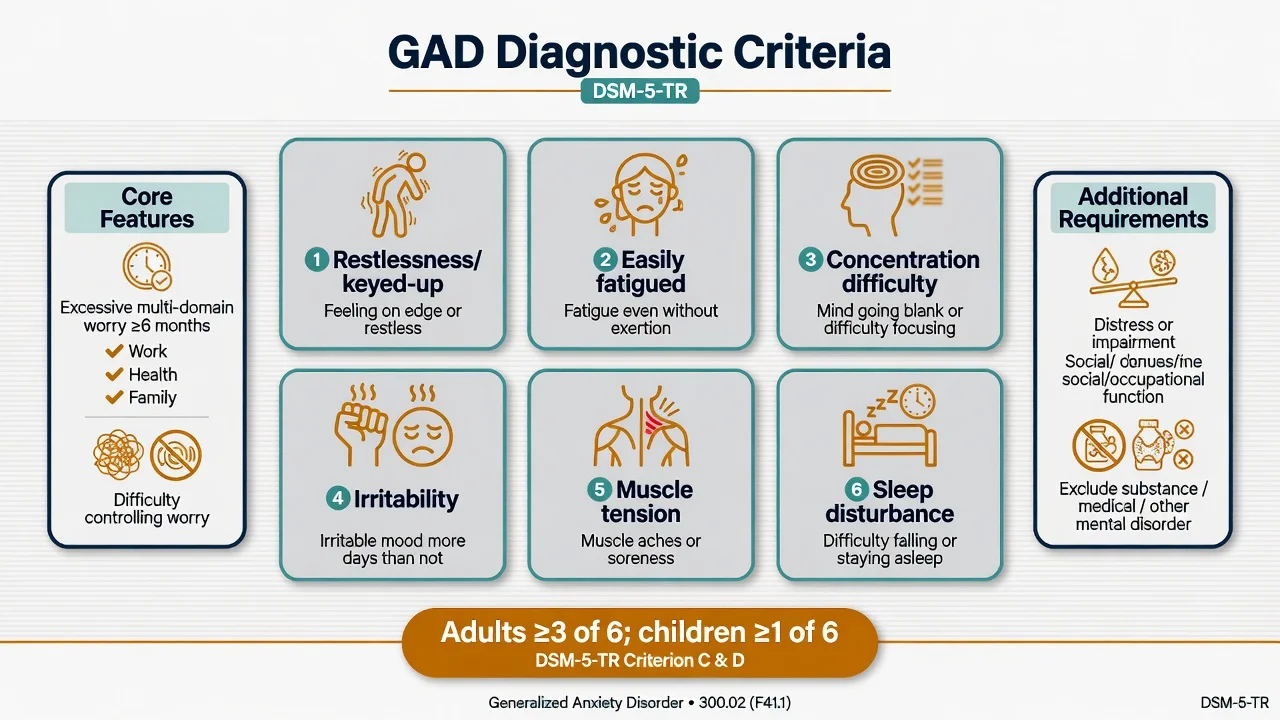
DSM-5-TR structure you must reproduce. Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (for example work or school performance). The individual finds it difficult to control the worry. The anxiety and worry are associated with three (or more) of the following six symptoms (with at least some symptoms present more days than not for the past 6 months); only one item is required in children: (1) restlessness or feeling keyed up or on edge; (2) being easily fatigued; (3) difficulty concentrating or mind going blank; (4) irritability; (5) muscle tension; (6) sleep disturbance (difficulty falling or staying asleep, or restless unsatisfying sleep). Symptoms cause clinically significant distress or impairment. The disturbance is not attributable to a substance or another medical condition, and is not better explained by another mental disorder (for example panic disorder only during panic, social anxiety only about scrutiny, OCD obsessions, separation anxiety, PTSD, anorexia body image, somatic symptom disorder, illness anxiety, schizophrenia-spectrum, or bipolar/depressive disorder mood episodes alone).[3][17]
ICD-11. Generalised anxiety disorder emphasises free-floating anxiety or worry focused on multiple everyday events, with associated symptoms such as muscular tension, autonomic overactivity, and subjective nervousness, with duration and impairment thresholds stated in the manual you are using. When duration language is examined, name which system you are applying — DSM-5-TR’s 6-month threshold is the classic exam anchor, while epidemiological work has debated shorter duration cut-points and their effect on prevalence.[3][17]
Classification
Core criteria spine
- Excessive multi-domain worry more days than not
- Duration ≥6 months (DSM-5-TR)
- Difficulty controlling the worry
- Distress or functional impairment
Associated symptoms (adults ≥3)
- Restlessness / keyed up
- Fatigue
- Concentration blankness
- Irritability, muscle tension, sleep disturbance
Exclusions
- Substance-induced (caffeine, stimulants, alcohol withdrawal)
- Medical (e.g. hyperthyroidism)
- Better explained by another anxiety, OCD, trauma, mood, or psychotic disorder
Related constructs
- Adjustment disorder with anxiety (stressor-linked, milder threshold)
- Anxious temperament / high neuroticism (trait, not diagnosis alone)
- Mixed anxiety-depression presentations in primary care
- Illness anxiety / somatic symptom overlap
Severity in practice is graded by symptom load, disability, comorbidity and risk rather than by a single laboratory value. Stepped-care pathways use severity and complexity to match intensity of psychological and pharmacological treatment.[5][6]
Epidemiology and risk factors
Headline numbers every candidate must own
GAD contributes substantial disability days and economic cost through lost productivity, primary-care utilisation and comorbidity. Prevalence estimates are sensitive to the duration criterion and to whether subthreshold free-floating anxiety is counted — examiners may ask why rates differ across surveys.[17][18]
Risk factors include female sex, high trait neuroticism, family history of anxiety or mood disorder, childhood adversity, chronic psychosocial stress, and comorbid depressive or other anxiety disorders. Suicide risk is not zero in “pure” GAD and rises sharply with depression, substance use and hopelessness — never discharge on the assumption that worry alone is safe.[3][18]
Pathophysiology
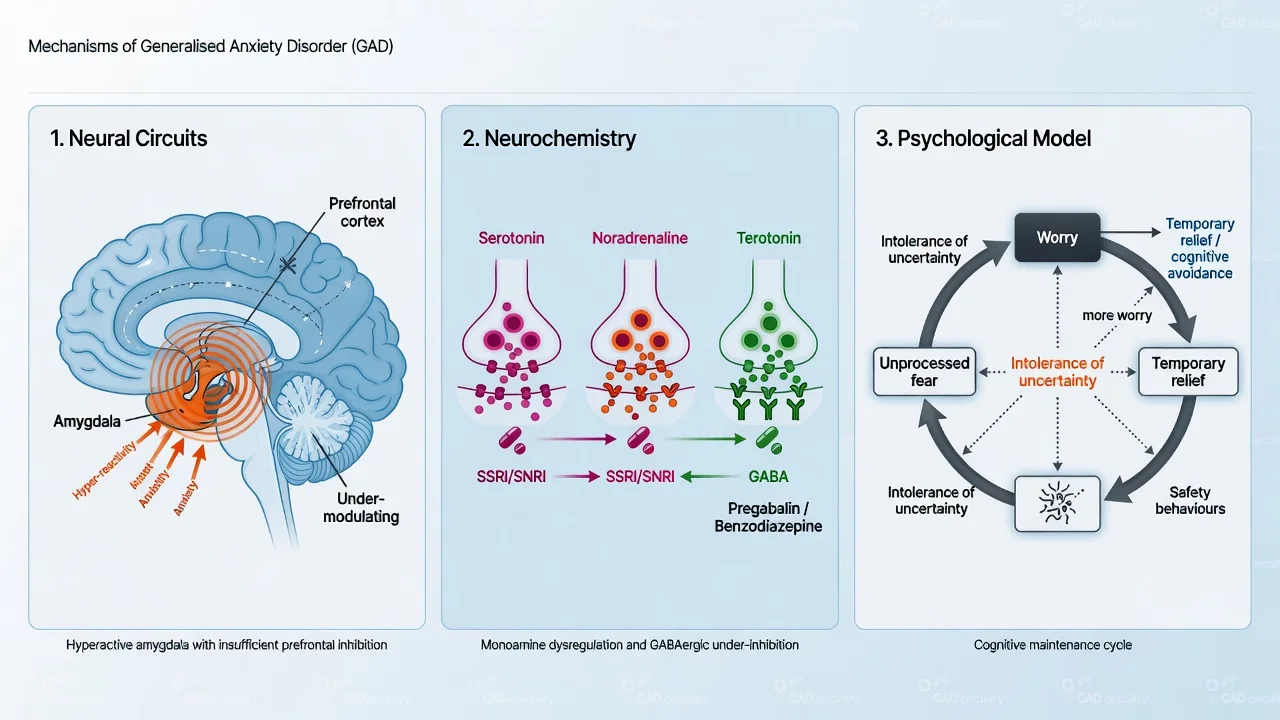
Circuit framing (viva depth, not diagnostic imaging). Group-level models emphasise limbic (including amygdala) hyper-reactivity with insufficient prefrontal top-down regulation of threat appraisal. Imaging is not an individual diagnostic test for GAD.[3]
Transmitter pharmacology that changes prescribing. Serotonergic and noradrenergic systems are the targets of SSRIs and SNRIs. GABAergic facilitation underlies benzodiazepine anxiolysis (rapid, dependence-prone). Pregabalin binds the α2δ subunit of voltage-gated calcium channels, reducing excitatory neurotransmitter release — clinically anxiolytic with a different risk profile from classical benzos, but still with misuse potential in vulnerable patients.[4][10][16]
Psychological models that change therapy choice. Cognitive avoidance (Borkovec-type) frames worry as predominantly verbal thought that suppresses imagery and emotional processing, producing short-term distress reduction and long-term maintenance. Intolerance of uncertainty drives checking, reassurance and perpetual planning when ambiguous outcomes feel intolerable. Metacognitive models highlight positive beliefs (“worrying helps me prepare”) and negative beliefs (“my worry is uncontrollable and dangerous”). Safety behaviours and muscle tension maintain threat expectation and somatic feedback loops.[13][14]
Clinical presentation
Core features combine psychic anxiety (apprehensive expectation, irritability, concentration difficulty, mind going blank) with somatic tension (muscle tightness, restlessness, sleep disruption) and variable autonomic symptoms (palpitations, sweating, GI upset). Tempo is chronic with fluctuations; patients often say “I have always been a worrier” but functional collapse is more recent.[3]
Primary-care and somatic presentations. Headache, chest tightness, IBS-like symptoms, fatigue and insomnia may dominate. The exam trap is either over-medicalising every symptom indefinitely or missing a real medical mimic. Quote the patient’s words in the MSE (e.g. “If I stop worrying, something terrible will happen”).[18]
Atypical presentations examiners test. Late first onset; perinatal exacerbation; older adults with health-focused worry overlapping illness anxiety; cultural idioms emphasising bodily heat, spirit or heart distress rather than “anxiety”; adolescents where irritability and school performance worry predominate.[3]
Differential diagnosis
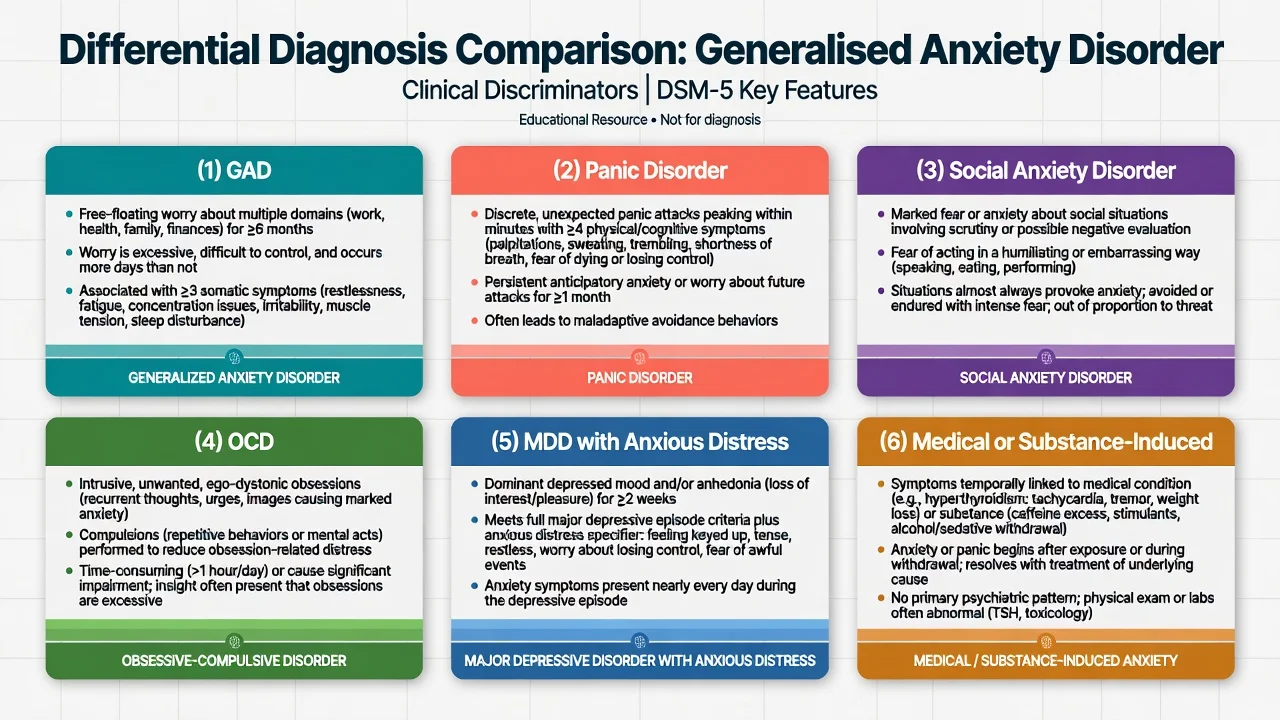
Panic disorder
- Discrete unexpected panic attacks
- Anticipatory anxiety about next attack
- Avoidance of attack cues
- Worry is attack-centred, not multi-domain free-floating
Social anxiety
- Fear of scrutiny, embarrassment, performance
- Situationally bound
- Safety behaviours (rehearsal, alcohol)
- Not primarily multi-theme life worry
OCD
- Intrusive ego-dystonic obsessions
- Compulsions / mental rituals
- Content often bizarre or forbidden
- GAD worry is real-life themes without true rituals
MDD / bipolar / trauma / medical
- MDD: low mood/anhedonia dominate; anxious distress specifier
- PTSD: trauma-linked re-experiencing
- Substance: caffeine, stimulants, alcohol withdrawal
- Medical: hyperthyroid, arrhythmia, hypoglycaemia, phaeo rare
Also keep illness anxiety disorder, somatic symptom disorder, adjustment disorder, ADHD with secondary worry, and anxious-avoidant personality traits on the board — traits do not cancel a syndromal GAD diagnosis when criteria are met.[3][5]
Clinical and bedside assessment
Structure the interview: worry domains and controllability; duration; associated six symptoms; avoidance and reassurance; caffeine, nicotine, alcohol and other substances; depression and suicide risk; bipolar screen (antidepressant planning); trauma screen; medical and medication history; perinatal status; function at work and relationships; prior treatments and adequacy (therapy type, drug, dose, duration, adherence).[5]
Document a full Mental State Examination. Risk is mandatory when depression, hopelessness, substance use or agitation is present. Capacity is decision-specific. Involuntary care uses local Mental Health Act principles — least restrictive, statute-bound; do not invent section numbers for the wrong jurisdiction.[5]
Investigations and measurement-based care
Baseline before pharmacotherapy (typical adult set). TSH when clinically indicated; full blood count; urea and electrolytes; liver function as indicated; ECG when cardiac risk or QT-active agents; pregnancy test when relevant; urine drug screen when substance contribution is plausible. Neuroimaging is for neurological red flags — not routine for classic young-adult GAD.[5][6]
GAD-7. Seven self-report items over the past 2 weeks; score range 0–21. Common severity bands used in practice and research: 5 mild, 10 moderate, 15 severe. Excellent screening and monitoring tool — not a stand-alone diagnosis and not a full suicide risk assessment.[1]
HAM-A (Hamilton Anxiety Rating Scale). Classic clinician-rated scale (14 items spanning psychic and somatic anxiety) used as a primary endpoint in many pharmacological RCTs. Know that trial “response” definitions often use percentage HAM-A reduction — quote the scale’s role, not fabricated cut-offs you cannot defend.[2][7][10]
Serial GAD-7 or equivalent plus side-effect and risk review is expected measurement-based care.[1][5]
Management — acute risk and resuscitation
Acute severe anxiety. Calm environment, clear explanation, exclude medical emergency, offer low-stimulus setting. A short course of a benzodiazepine may be used for severe distress with a documented indication, short duration (days, not months as default), no automatic repeats, and a plan to establish SSRI/SNRI and/or CBT. Example exam-level short-term agents: diazepam 2–5 mg orally as needed with strict limits, or lorazepam 0.5–1 mg orally — always individualise for age, respiratory disease, and substance history.[5][6]
Suicidal crisis with comorbid depression. Safety plan, means restriction, intensify setting, treat both syndromes — an SSRI/SNRI may cover both anxiety and depression once acute safety is addressed.[3][5]
Management — definitive and stepwise
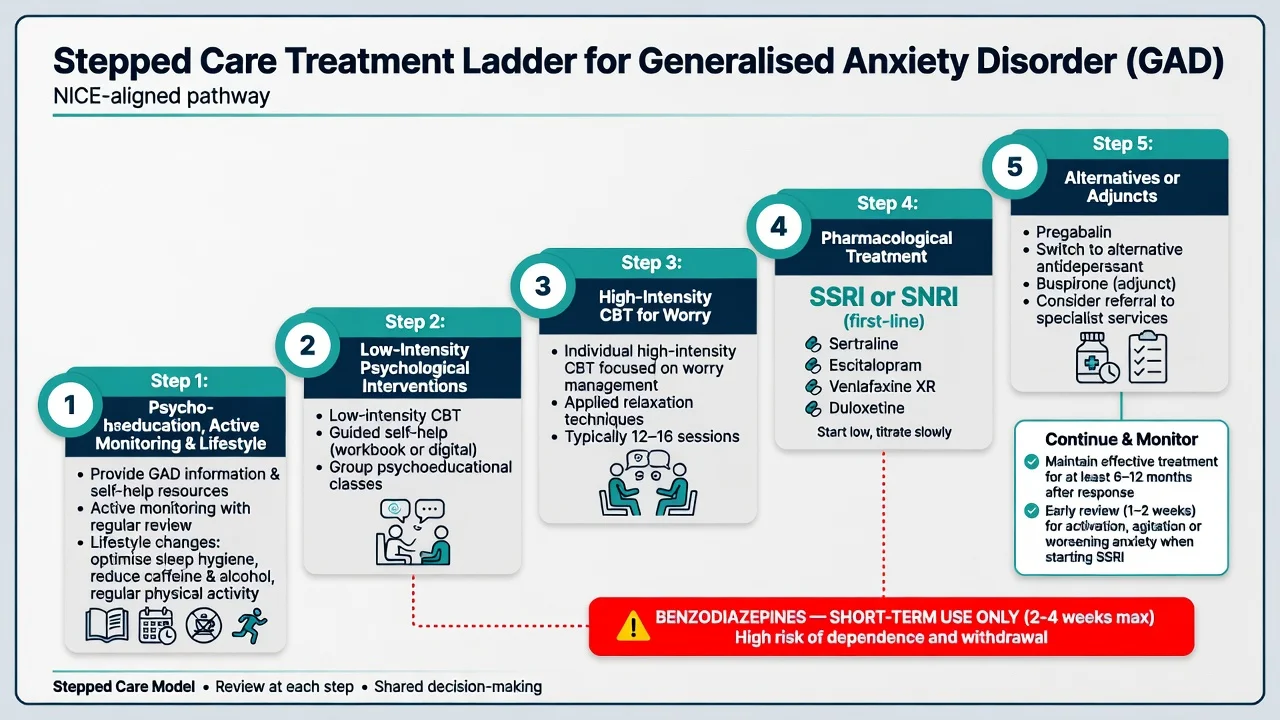
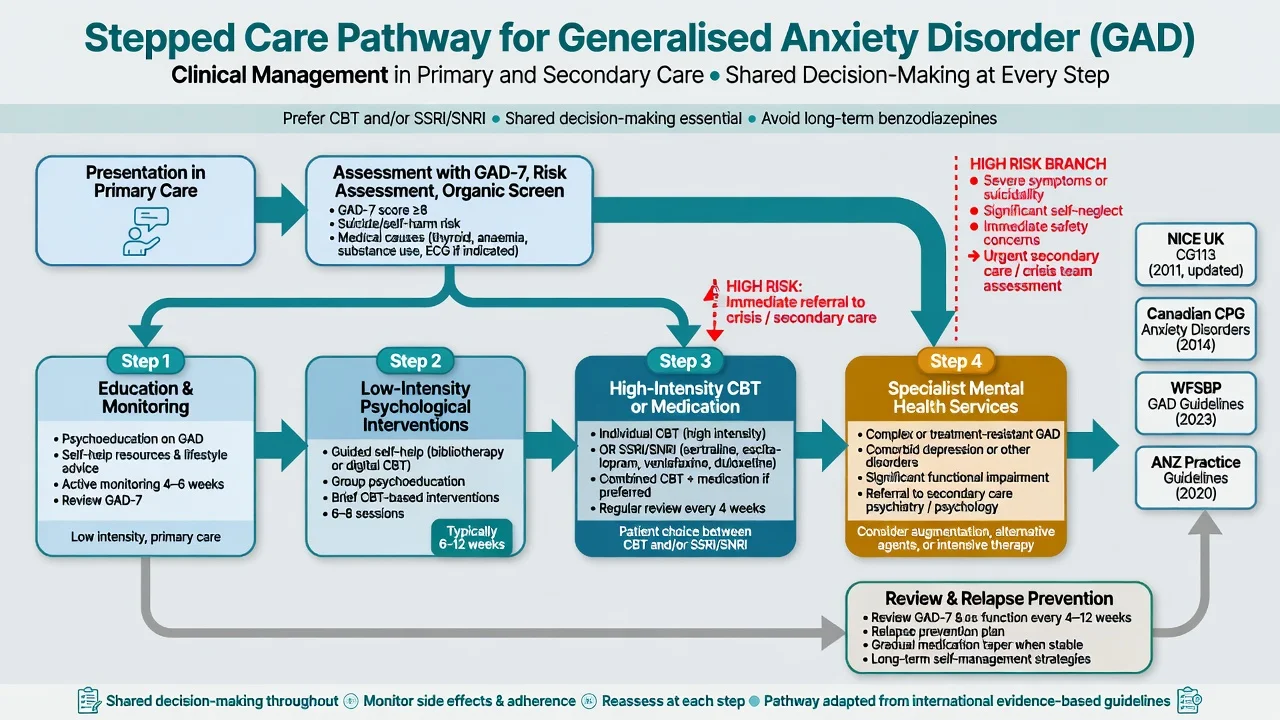
Stepped care principles
Match intensity to severity, disability, preference and comorbidity. Low-intensity interventions and active monitoring suit mild presentations. Moderate-to-severe GAD typically warrants high-intensity CBT and/or an antidepressant (SSRI or SNRI). Combination treatment is reasonable when severity, chronicity or partial response supports it. Specialist escalation is for high risk, diagnostic complexity, treatment resistance, or heavy substance comorbidity.[5][6][14]
Australian and New Zealand practice aligns with evidence-based CBT access (public and private pathways), first-line SSRI/SNRI prescribing, and cautious benzodiazepine stewardship within local formulary and PBS/PHARMAC constraints. Formulate culturally, including for Māori, Aboriginal and Torres Strait Islander peoples, using local cultural safety frameworks rather than stereotype checklists.[5][6]
First-line psychological therapy — CBT for GAD
CBT for GAD is not generic “talk about feelings.” High-yield ingredients: psychoeducation; self-monitoring of worry episodes; cognitive restructuring of probability overestimation and catastrophising; worry postponement / worry time; imaginal exposure to feared outcomes; problem-solving training; intolerance of uncertainty experiments; reduction of safety behaviours and reassurance-seeking; applied relaxation / progressive muscle relaxation; relapse prevention. Meta-analytic and Cochrane-level evidence supports psychological therapies, with CBT the dominant evidence-based model examiners expect you to name with components.[13][14]
Typical high-intensity course concepts: about 12–20 sessions (local protocols vary); homework is essential; family accommodation of reassurance may need addressing.[14]
First-line pharmacotherapy — agent, dose, monitoring
Doses below are typical adult oral starting and common therapeutic ranges for exam answers; individualise for age, hepatic/renal function, interactions and pregnancy. Cite local product information for legal prescribing.[4][5][16]
| Agent (class) | Typical start | Common therapeutic range | Key monitoring / notes |
|---|---|---|---|
| Sertraline (SSRI) | 25–50 mg daily | 50–200 mg daily | RCT efficacy in GAD; GI and sexual side-effects; relatively flexible cardiac/perinatal discussions |
| Escitalopram (SSRI) | 5–10 mg daily | 10–20 mg daily | Flexible-dose RCT evidence; QTc caution at higher doses; hyponatraemia in elderly |
| Paroxetine (SSRI) | 10–20 mg daily | 20–50 mg daily | Flexible-dose RCT evidence; higher discontinuation syndrome risk; anticholinergic load |
| Venlafaxine XR (SNRI) | 37.5–75 mg daily | 75–225 mg daily | 6-month RCT in nondepressed GAD; BP monitoring; discontinuation symptoms |
| Duloxetine (SNRI) | 30 mg daily | 60–120 mg daily | Pooled RCT evidence; useful if pain comorbidity; LFTs; avoid significant liver disease |
| Typical adult oral ranges for exam use; individualise and check local product information.[7][8][9][11][12] |
Start low when anxiety is severe (initial activation/jitteriness is a classic early adverse effect), review within 1–2 weeks for activation, akathisia and suicidality (especially under 25 years and with depression), then titrate. Declare an adequate trial only after about 4–6 weeks at a therapeutic dose with adherence checked — not after 10 days of half-dose.[7][8][9][11][12]
Network meta-analysis of pharmacological treatments for GAD supports clinically meaningful benefits for several agents versus placebo, with differences in acceptability; use NMA as a comparative map, not as a single “best drug for everyone.”[4]
Pregabalin
Pregabalin has robust RCT evidence in GAD, including comparison arms with alprazolam for psychic and somatic symptoms, and evidence as adjunct in partial SSRI/SNRI responders.[10][19]
Exam-level dosing concept (adult, normal renal function): often start 75 mg twice daily (or lower in frailty), titrate toward 150–600 mg/day in divided doses as tolerated — exact titration per product information and renal function. Monitor dizziness, sedation, weight gain, oedema; counsel on misuse/dependence risk and avoid combining carelessly with opioids or alcohol. Reduce dose in renal impairment.[4][10][19]
Buspirone (azapirone)
Buspirone is a 5-HT1A partial agonist with anxiolytic effect, delayed onset (often 2+ weeks), and little euphoria compared with benzodiazepines. Cochrane-level review supports azapirones versus placebo in GAD, with methodological caveats you should acknowledge.[15]
Exam-level dosing concept: often 5 mg two to three times daily, titrate toward 20–30 mg/day in divided doses (maximum per label commonly 60 mg/day). Less effective historically in patients with recent chronic benzodiazepine exposure; not ideal as sole rescue for acute panic-level distress.[15][20]
Benzodiazepines — limited role, major exam trap
Benzodiazepines reduce anxiety rapidly and performed well on some short-term endpoints historically, but dependence, tolerance, cognitive and psychomotor impairment, falls in the elderly, and rebound anxiety make them unsuitable as routine long-term monotherapy for GAD in modern guidelines.[5][6][16]
Use only: short-term bridging while an SSRI starts; severe acute distress with a clear stop date; specialist contexts with documented rationale. Prefer long half-life agents for taper of dependent patients rather than abrupt cessation. When discontinuing long-term benzodiazepines, structured taper plus consideration of alternative anxiolysis (including evidence-informed antidepressant pathways studied in discontinuation contexts) is safer than abrupt stop.[20]
Partial response, switching and augmentation
After non-response: re-check diagnosis (depression, OCD, substances, medical), adherence, dose, and CBT quality. Switch SSRI↔SNRI or to another first-line agent when zero response or intolerance. Augment with pregabalin when partial response to SSRI/SNRI is documented.[4][19] Second-generation antipsychotics are not routine first-line anxiolytics — reserve for specialist formulation with metabolic monitoring if used at all.[5][6]
Duration after response
Continue an effective antidepressant for a substantial period after response — practical teaching often at least 6–12 months, longer when illness is highly recurrent, chronic, or severely disabling — then taper slowly with relapse monitoring. Stopping the week the patient “feels a bit better” is a classic error.[5][6]
Specific subtypes and scenarios
GAD with major depression. Extremely common. Treat both; SSRI/SNRI often covers both domains; suicide risk assessment is mandatory; do not minimise depression because worry is loud.[3][5]
GAD with alcohol or sedative use. Alcohol is a frequent self-medication; benzos compound dependence risk. Address substance use in parallel; avoid simply replacing alcohol with unsupervised diazepam.[5]
Chronic / treatment-resistant GAD. Re-formulate; ensure genuine CBT for worry (not unstructured support); optimise dose; consider pregabalin pathway; specialist psychology; occupational rehabilitation.[4][14]
Primary care versus specialist. Specialist psychiatry for high suicide risk, diagnostic uncertainty, treatment resistance, complex personality or trauma comorbidity, or failed adequate primary-care trials.[5]
Complications and pitfalls
Classic pitfalls: chronic benzo monotherapy; under-dosed SSRI trials; missing depression or bipolarity; ignoring caffeine/thyroid; sexual side-effects silently destroying adherence; venlafaxine/paroxetine discontinuation syndromes from abrupt stop; pregabalin diversion; endless reassurance without exposure-based CBT; diagnostic overshadowing of medical disease.[5][12][16]
Prognosis and disposition
Without treatment, GAD is often chronic and fluctuating with high disability. With adequate CBT and/or SSRI/SNRI, many patients achieve meaningful response; residual worry predicts relapse, so relapse-prevention skills and adequate medication duration matter.[3][13][18]
Disposition ladder: GP shared care and primary psychological services; secondary community mental health for complex cases; inpatient care uncommon unless high risk, severe comorbidity, or medical complications of withdrawal. Functional recovery (work, relationships, sleep) is an outcome alongside GAD-7 change.[5]
Special populations
Children and adolescents. Associated-symptom threshold differs (one of six in DSM). Family work and school function are central. If medication is used, SSRI choice and activation/suicidality monitoring are mandatory; specialist CAMHS pathways preferred.[3][5]
Older adults. Prefer non-benzo strategies; watch hyponatraemia on SSRIs, falls, polypharmacy, and medical mimics. Start low, go slow.[5][6]
Pregnancy and lactation. Untreated severe anxiety has maternal and fetal stress correlates; discuss risks and benefits. Sertraline is frequently discussed as a pragmatic SSRI option when medication is needed; avoid benzodiazepines where possible, especially late pregnancy (floppy infant/withdrawal concerns). Coordinate with obstetric care.[5]
Intellectual disability and cultural formulation. Adapt communication; carers as collateral; cultural expressions of distress; FRANZCP cultural safety expectations in ANZ practice.[5]
Evidence, guidelines and regional differences
Landmark synthesis. Tyrer and Baldwin’s Lancet seminar remains a compact clinical overview of concept, burden and treatment framing.[3] Slee and colleagues’ Lancet network meta-analysis maps comparative efficacy and acceptability of pharmacological options — use it to justify class choices, not to invent league-table dogma for an individual patient.[4] Wittchen’s burden paper anchors disability and cost arguments.[18]
Key RCTs to name. Venlafaxine XR six-month nondepressed GAD trial (Gelenberg); sertraline 12-week trial (Allgulander); escitalopram flexible-dose (Davidson); paroxetine flexible-dose (Pollack); duloxetine pooled analyses (Allgulander); pregabalin versus placebo and alprazolam (Rickels); pregabalin adjunctive after SSRI/SNRI partial response (Rickels).[7][8][9][10][11][12][19]
Psychotherapy evidence. Mitte’s meta-analysis comparing CBT with pharmacotherapy; Hunot Cochrane review of psychological therapies for GAD.[13][14]
Guidelines. Canadian CPG (Katzman et al.) and WFSBP Version 3 Part I (Bandelow et al.) are high-yield international anchors; NICE stepped care shapes UK exams; ANZ practice maps onto these with local formulary and cultural safety overlays.[5][6]
Controversies. Optimal duration criterion; role of pregabalin given misuse; whether combination CBT+meds is default in moderate severity; how aggressively to avoid all benzodiazepines versus time-limited bridging.[4][6][17]
Exam pearls
WORRIED
Self-test: one-liner viva traps
- Duration? 6 months more days than not (DSM-5-TR).
- Adult symptom count? At least 3 of 6 associated symptoms.
- GAD-7 severe band? 15 and above commonly used.
- First-line drugs? SSRI or SNRI (sertraline, escitalopram, paroxetine, venlafaxine XR, duloxetine).
- Pregabalin role? Evidence-based alternative/adjunct; misuse caution.
- Buspirone pearl? Delayed onset; weaker after chronic benzo use.
- Benzos? Short-term bridge only, not maintenance first-line.[1][4][5][15]
References
- [1]Spitzer RL, Kroenke K, Williams JB, Löwe B A brief measure for assessing generalized anxiety disorder: the GAD-7 Arch Intern Med, 2006.PMID 16717171
- [2]Hamilton M The assessment of anxiety states by rating Br J Med Psychol, 1959.PMID 13638508
- [3]Tyrer P, Baldwin D Generalised anxiety disorder Lancet, 2006.PMID 17174708
- [4]Slee A, Nazareth I, Bondaronek P, Liu Y, Cheng Z, Freemantle N Pharmacological treatments for generalised anxiety disorder: a systematic review and network meta-analysis Lancet, 2019.PMID 30712879
- [5]Katzman MA, Bleau P, Blier P, Chokka P, Kjernisted K, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders BMC Psychiatry, 2014.PMID 25081580
- [6]Bandelow B, Allgulander C, Baldwin DS, Costa DLDC, Denys D, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for treatment of anxiety, obsessive-compulsive and posttraumatic stress disorders - Version 3. Part I: Anxiety disorders World J Biol Psychiatry, 2023.PMID 35900161
- [7]Gelenberg AJ, Lydiard RB, Rudolph RL, Aguiar L, Haskins JT, Salinas E Efficacy of venlafaxine extended-release capsules in nondepressed outpatients with generalized anxiety disorder: A 6-month randomized controlled trial JAMA, 2000.PMID 10865302
- [8]Allgulander C, Dahl AA, Austin C, Morris PL, Sogaard JA, Fayyad R, et al. Efficacy of sertraline in a 12-week trial for generalized anxiety disorder Am J Psychiatry, 2004.PMID 15337655
- [9]Davidson JR, Bose A, Korotzer A, Zheng H Escitalopram in the treatment of generalized anxiety disorder: double-blind, placebo controlled, flexible-dose study Depress Anxiety, 2004.PMID 15274172
- [10]Rickels K, Pollack MH, Feltner DE, Lydiard RB, Zimbroff DL, Bielski RJ, et al. Pregabalin for treatment of generalized anxiety disorder: a 4-week, multicenter, double-blind, placebo-controlled trial of pregabalin and alprazolam Arch Gen Psychiatry, 2005.PMID 16143734
- [11]Allgulander C, Hartford J, Russell J, Ball S, Erickson J, Raskin J, et al. Pharmacotherapy of generalized anxiety disorder: results of duloxetine treatment from a pooled analysis of three clinical trials Curr Med Res Opin, 2007.PMID 17559726
- [12]Pollack MH, Zaninelli R, Goddard A, McCafferty JP, Bellew KM, Burnham DB, et al. Paroxetine in the treatment of generalized anxiety disorder: results of a placebo-controlled, flexible-dosage trial J Clin Psychiatry, 2001.PMID 11411817
- [13]Mitte K Meta-analysis of cognitive-behavioral treatments for generalized anxiety disorder: a comparison with pharmacotherapy Psychol Bull, 2005.PMID 16187860
- [14]Hunot V, Churchill R, Silva de Lima M, Teixeira V Psychological therapies for generalised anxiety disorder Cochrane Database Syst Rev, 2007.PMID 17253466
- [15]Chessick CA, Allen MH, Thase M, Batista Miralha da Cunha AB, Kapczinski FF, de Lima MS, et al. Azapirones for generalized anxiety disorder Cochrane Database Syst Rev, 2006.PMID 16856115
- [16]Hidalgo RB, Tupler LA, Davidson JR An effect-size analysis of pharmacologic treatments for generalized anxiety disorder J Psychopharmacol, 2007.PMID 17984162
- [17]Kessler RC, Brandenburg N, Lane M, Roy-Byrne P, Stang PD, Stein DJ, et al. Rethinking the duration requirement for generalized anxiety disorder: evidence from the National Comorbidity Survey Replication Psychol Med, 2005.PMID 16045073
- [18]Wittchen HU Generalized anxiety disorder: prevalence, burden, and cost to society Depress Anxiety, 2002.PMID 12497648
- [19]Rickels K, Shiovitz TM, Ramey TS, Weaver JJ, Knapp LE, Miceli JJ Adjunctive therapy with pregabalin in generalized anxiety disorder patients with partial response to SSRI or SNRI treatment Int Clin Psychopharmacol, 2012.PMID 22302014
- [20]Rickels K, DeMartinis N, García-España F, Greenblatt DJ, Mandos LA, Rynn M Imipramine and buspirone in treatment of patients with generalized anxiety disorder who are discontinuing long-term benzodiazepine therapy Am J Psychiatry, 2000.PMID 11097963