Psych · General adult psychiatry — trauma and stressor-related disorders
Grief and prolonged grief disorder
Also known as Prolonged grief disorder · Complicated grief · Persistent complex bereavement disorder · Pathological grief · Traumatic grief · Bereavement
Exam-exhaustive fellowship reference on normal grief versus prolonged grief disorder (DSM-5-TR and ICD-11), differential from major depression, dual-process and cognitive-behavioural mechanisms, suicide risk, Complicated Grief Treatment and grief-focused CBT evidence, selective pharmacotherapy for comorbidity, and cultural care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Grief and bereavement sit at the junction of everyday human experience and formal psychiatric nosology. Fellowship examiners test whether you can protect adaptive mourning from medicalisation, still detect treatable PGD and comorbid MDD/PTSD, and deliver evidence-based grief-focused care rather than reflexive sedatives or unsupported stage-of-grief dogma.[4][8][15][17]
Overview and definition
Grief is the multidimensional reaction to loss — emotional (yearning, sorrow, anger, guilt), cognitive (preoccupation, disbelief), behavioural (searching, social withdrawal), somatic (sleep, appetite, emptiness), social, and spiritual. Mourning is the culturally patterned expression of grief through ritual, roles, and community practice. Bereavement is the state of having lost someone close through death.[4][15]
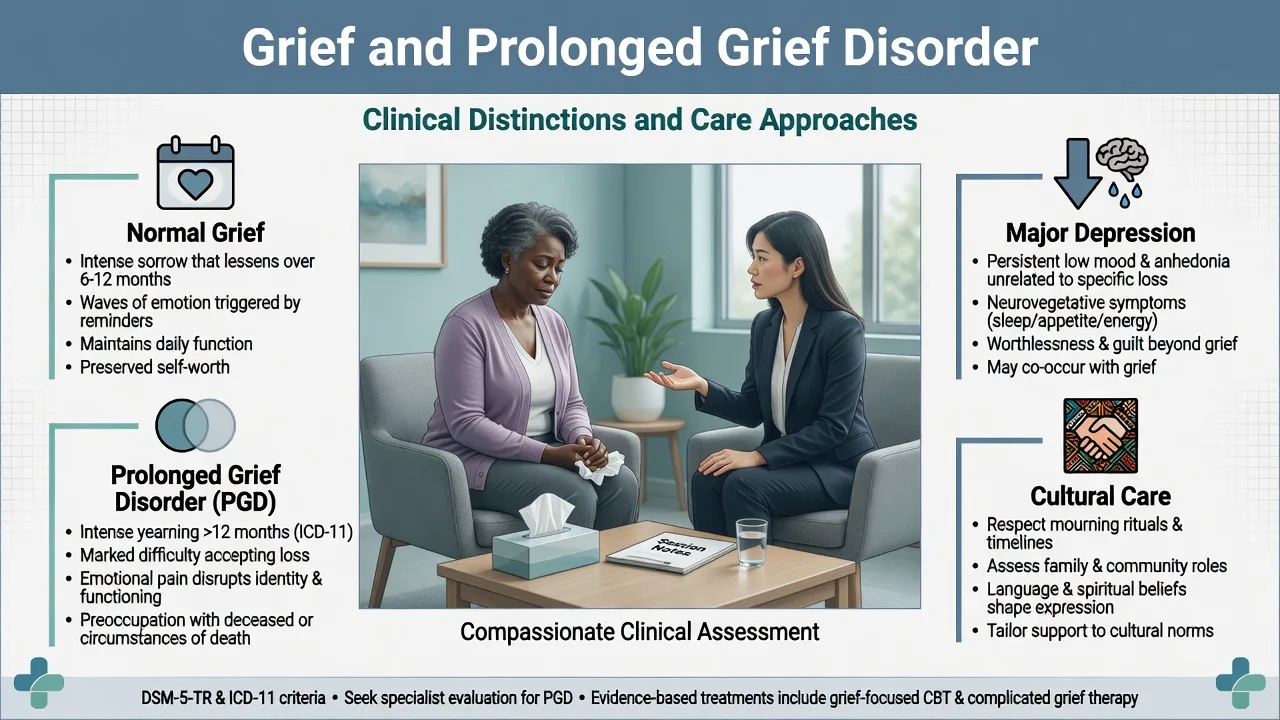
Adaptive (normal) grief is intense and often oscillating; it typically softens in intensity over time and permits progressive re-engagement with life, even when love and continuing bonds endure. Adaptive grief is not a DSM/ICD mental disorder.[4][8][15]
Prolonged grief disorder (PGD) is a freestanding diagnosis in DSM-5-TR and ICD-11 for a minority of bereaved people whose grief remains intense, persistent beyond duration and cultural norms, and functionally impairing, with yearning/preoccupation as the core.[4][7][8]
Historical and research labels still appear in viva stems: complicated grief (Shear clinical research package and trials), persistent complex bereavement disorder (DSM-5 Section III), and traumatic grief. Analysis of Yale Bereavement Study data indicated that PGD and PCBD criteria largely identify the same entity, whereas the older complicated-grief item set is not identical.[6][8]
Classification and diagnostic criteria
DSM-5-TR Prolonged Grief Disorder (reproduce in viva)
Anchor answers to operational criteria rather than vibes.[4][8]
- Death of a person close to the bereaved, with the death having occurred at least 12 months ago for adults (or at least 6 months ago for children and adolescents).
- Since the death, development of a persistent grief response characterised by one or both of: intense yearning/longing for the deceased person, or preoccupation with thoughts or memories of the deceased (in children, preoccupation may focus on circumstances of the death). These are present most days to a clinically significant degree for at least the past month.
- As a result of the death, at least three of eight additional symptoms present most days for at least the past month to a clinically significant degree (examples include identity disruption, marked sense of disbelief, avoidance of reminders, intense emotional pain related to the death, difficulty reintegrating into relationships and activities, emotional numbness, sense that life is meaningless, intense loneliness).
- The disturbance causes clinically significant distress or impairment.
- The duration and severity of the bereavement reaction clearly exceed expected social, cultural, or religious norms for the individual's culture and context.
- The symptoms are not better explained by another mental disorder (for example MDD, PTSD) and are not attributable to substances or another medical condition.[4][7][8]
ICD-11 Prolonged Grief Disorder (exam delta)
ICD-11 PGD emphasises persistent and pervasive longing for the deceased or persistent preoccupation, accompanied by intense emotional pain (for example sadness, guilt, anger, denial, blame), with the grief response persisting for an atypically long period after the loss (more than 6 months) and exceeding expected social, cultural or religious norms, plus significant impairment. Clinical utility work supports that ICD-11 guidelines can be applied reliably in clinical samples when operationalised carefully.[7][8]
When an examiner asks for a number, name which system you are using. Do not invent a hybrid "9-month" rule.[7][8]
Two separate classification moves candidates confuse
- DSM-5 removed the bereavement exclusion for major depressive episode — meaning MDD can be diagnosed during bereavement when full criteria are met; evidence reviews argued bereavement-related depression is not categorically unique.[9][10][11]
- DSM-5-TR formalised PGD as its own diagnosis after decades of complicated grief / PCBD research — this is not the same as "turning all grief into depression."[4][8]
Adjustment disorder criteria exclude normal bereavement and should not be used when PGD better accounts for the presentation.[4][8]
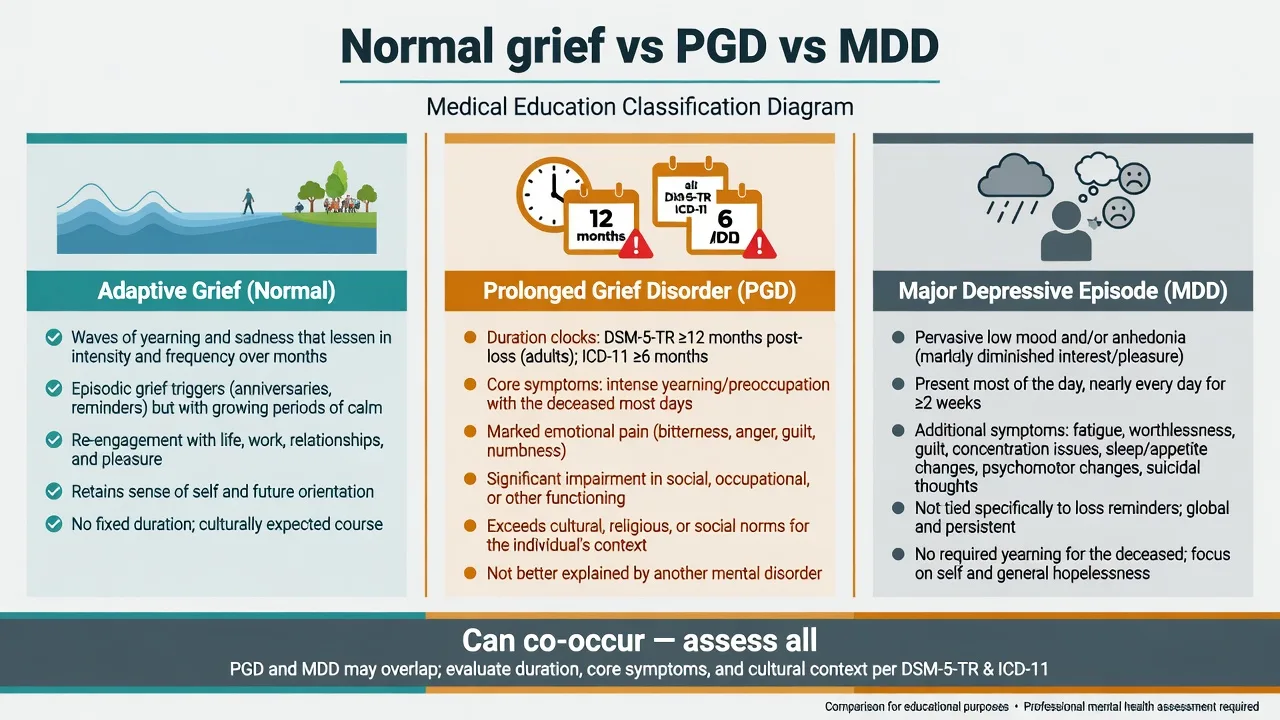
Adaptive grief
- Expected after death
- Yearning waves that typically soften
- Continuing bonds may be healthy
- Not a mental disorder
DSM-5-TR PGD
- ≥12 months adult / ≥6 months youth
- Yearning or preoccupation ≥1 month
- ≥3 additional symptoms
- Impairment + exceeds cultural norms
ICD-11 PGD
- ≥6 months after loss
- Longing or preoccupation
- Intense emotional pain
- Exceeds norms + impairment
MDD in bereavement
- Full episode criteria can be met
- No bereavement exclusion (DSM-5+)
- Pervasive low mood/anhedonia
- May co-occur with PGD
Epidemiology and risk factors
Numbers and settings candidates should own
Among bereaved adults, a systematic review and meta-analysis estimated pooled PGD prevalence in the order of about one in ten, with substantial heterogeneity reflecting criteria sets, sampling, and culture.[5] Cross-national analyses confirm that prevalence estimates move with methodology and context — quote ranges carefully rather than a single global constant.[16]
Risk factors cluster as: nature of the death (violent, sudden, suicide, multiple losses); relationship to the deceased (child loss, highly dependent or conflicted attachment); personal vulnerability (prior depression, anxiety, PTSD, insecure attachment, limited support); and context (poverty, concurrent stressors, blocked rituals, social stigma).[5][12][16][19] COVID-related deaths added isolation, disrupted funerals, and mass bereavement as public-mental-health stressors.[19]
Complicated grief samples show medical comorbidity burden and elevated clinical complexity; suicide-bereaved people are a priority subgroup for both grief-focused care and risk surveillance.[12]
Pathophysiology and maintaining mechanisms
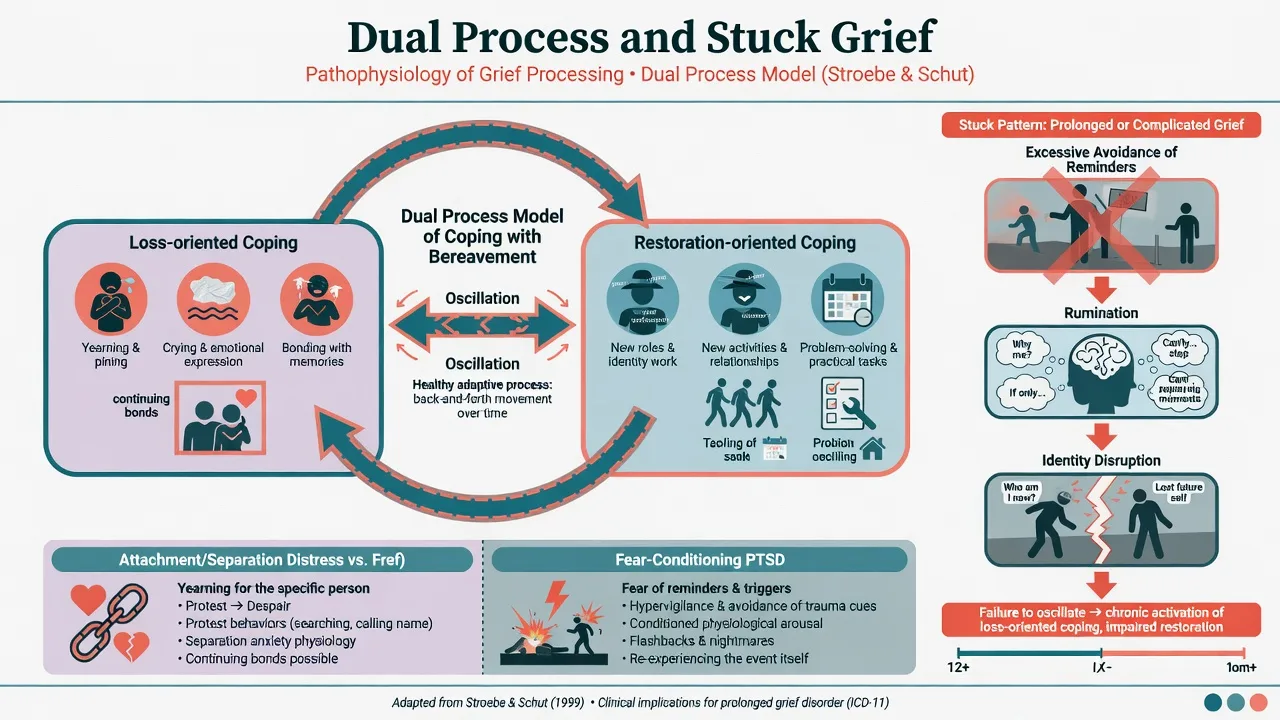
Dual process model (Stroebe and Schut). Adaptive coping oscillates between loss-oriented processes (yearning, crying, bonding memories, grief work) and restoration-oriented processes (new roles, practical tasks, distraction, new activities). Pathology is framed less as failure to complete a fixed sequence of stages and more as stuck oscillation — excessive avoidance of loss material, or relentless rumination without restoration, or inability to re-engage life tasks.[15]
Attachment and yearning. Separation distress (yearning, searching, proximity-seeking to reminders) is core. This is phenomenologically distinct from the pervasive anhedonia and self-reproach that dominate many major depressive episodes, although both can coexist.[4][8]
Cognitive-behavioural maintaining factors. Catastrophic beliefs ("I cannot live without them"; "Moving on betrays them"), rumination, and avoidance of people/places/objects linked to the death maintain severity. Complicated Grief Treatment outcome research supports that change in avoidance and maladaptive grief-related beliefs mediates improvement.[14][20]
Contrast models. PTSD after traumatic death emphasises fear conditioning, intrusive re-experiencing of the manner of death, and threat-related arousal. MDD emphasises pervasive mood, neurovegetative load, and global self-worth collapse. PGD emphasises separation distress about the person lost. Formulations can include more than one mechanism when comorbidity is present.[8][12]
Clinical presentation
Adaptive grief. Waves of yearning and sorrow triggered by reminders; preserved capacity for moments of pleasure or connection; gradual reorganisation of identity and routine; cultural mourning practices engaged. Sleep and appetite disturbance are common early and usually improve.[4][15]
PGD. Persistent intense yearning or mental preoccupation with the deceased long after cultural peers have begun to re-engage; identity disruption ("part of me died with them"); disbelief that feels frozen; avoidance of graves, photographs, the hospital corridor, the empty chair; emotional numbness; sense that life is empty or meaningless; intense loneliness; stalled work and relationships. MSE should quote the loss link and the stalled restoration: "Every day I wait for her key in the door; I still set two places; I cannot go into our bedroom."[4][7][8]
Special stems. Suicide loss: guilt, stigma, anger, trauma imagery of discovery, family contagion concerns — CGT remains relevant and HEAL analyses inform this subgroup.[12] COVID/disrupted mourning: unfinished goodbyes, virtual funerals, isolation amplify risk pathways.[19] Cultural presentations may emphasise somatic distress, ritual obligations, or experiences of the deceased's presence that are culturally intelligible — formulate before pathologising.[17][18]
Differential diagnosis
Key discriminators for fellowship stems are as follows.[4][8]
- Normal grief vs PGD: duration thresholds (system-specific), cultural-norm criterion, persistence of yearning/preoccupation cluster, and impairment that does not progressively allow life re-engagement.[4][7][8]
- PGD vs MDD: person-linked yearning and identity disruption vs pervasive low mood/anhedonia, self-critical worthlessness not solely loss-linked, marked psychomotor change, and full symptom count; Kendler and colleagues found bereavement-related major depression substantially similar to other stressor-related MDD — so do not withhold MDD diagnosis when criteria are met.[8][11]
- PGD vs PTSD: separation distress about the deceased vs trauma clusters about how they died; both after violent death.[8][12]
- Adjustment disorder: not normal bereavement; not used when PGD better fits.[4][8]
- Culturally expected mourning: long rituals or anniversary practices that fit cultural norms and do not meet the "exceeds norms + impairment" threshold are not PGD.[17][18]
- Grief-related sensing of the deceased vs psychosis: form, insight, cultural congruence, other psychotic features.[8][17]
- Substances and medical mimics when course is atypical.[8]
Do not dual-code soft labels when full criteria for MDD or PTSD are met — treat those fully while still addressing grief mechanisms if present.[8][9][10]
Clinical and bedside assessment
Structure the interview as a bereavement-focused assessment with mandatory risk and cultural formulation.[7][8][17]
- Loss map — who died, relationship quality, circumstances (natural/unnatural/suicide/homicide), date, notification experience, body viewing, rituals completed or blocked, secondary losses (home, income, status).
- Timeline — apply the system you are using (DSM-5-TR 12 months adult / 6 months youth; ICD-11 ≥6 months).
- PGD symptom inventory — yearning, preoccupation, identity, disbelief, avoidance, pain, reintegration failure, numbness, meaninglessness, loneliness.
- Full syndrome screen — MDD, bipolar, PTSD/ASD, panic, substances, psychosis.
- Risk — passive death wish, desire for reunion, intent, plan, means, prior attempts, impulsivity, alcohol/drugs, protective factors (other children, faith, duty).
- Function and supports — work/school, caregiving, isolation, cultural community.
- Cultural formulation — expected mourning period, rituals, family hierarchy, language, spiritual meanings of continuing bonds.[7][8][17]
Scales. Historical Inventory of Complicated Grief / PG-13 lineage and modern Traumatic Grief Inventory variants map to DSM-5-TR and ICD-11 constructs; use them to measure severity and response. PHQ-9 and GAD-7 monitor comorbidity but do not diagnose PGD.[4][7]
Investigations
There is no laboratory or imaging test for grief or PGD. Investigate to exclude differentials and to baseline pharmacotherapy when treating comorbid depression: TSH when indicated, metabolic panel, pregnancy test, urine drug screen if substances contribute, ECG before selected antidepressants in cardiac risk. Neuroimaging only for neurological red flags, not to "prove" grief.[8]
Management — acute risk and crisis
Priorities: physical safety; substance intoxication; safeguarding other survivors after suicide/homicide; decide home with plan versus crisis team versus inpatient care. Short-term hypnotics for severe acute insomnia are occasional bridges only (for example temazepam 10 mg orally at night for a few nights in a carefully selected adult, or local non-benzodiazepine alternatives) with an exit plan — never convert grief into chronic sedative dependence.[8]
Do not pathologise the first weeks to months after an expected death when functioning and cultural fit remain acceptable; offer support, information, and review triggers.[4][15]
Management — definitive stepped care
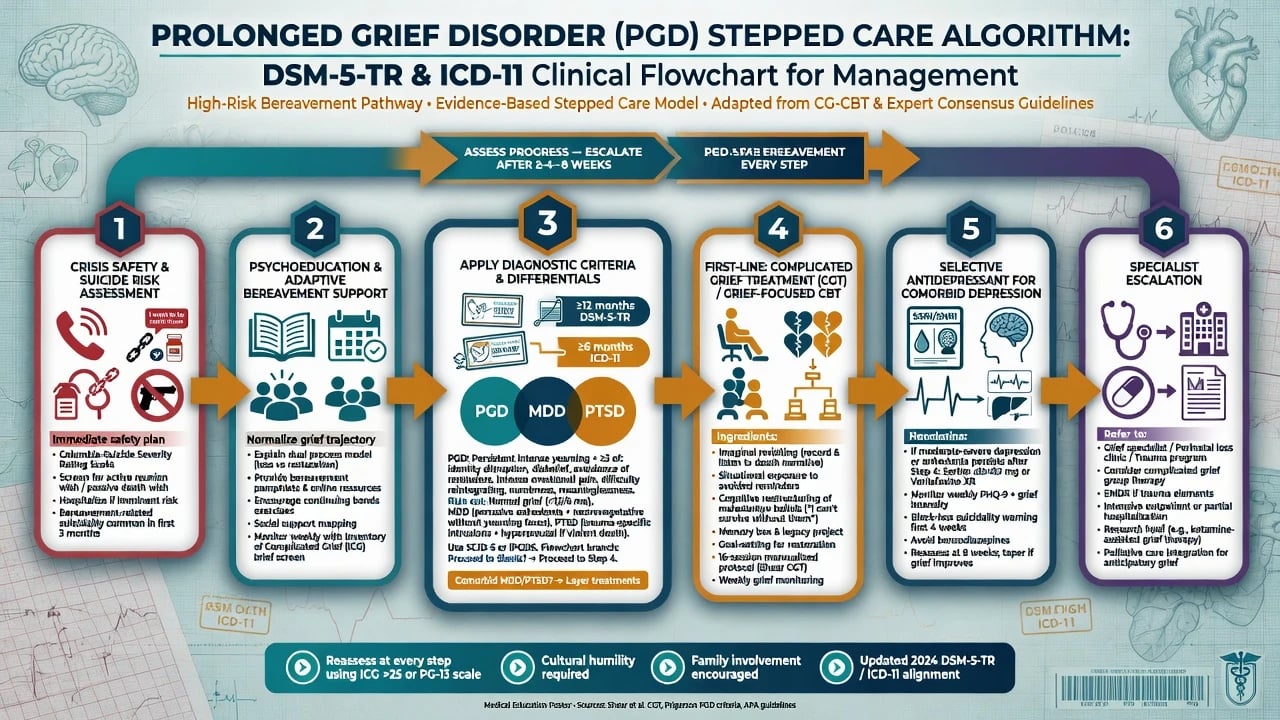
Step 0 — Safety and practical needs
Risk management, housing, finances after death, childcare, and legal/administrative secondary losses. Practical help is clinical care, not "non-medical."[15][19]
Step 1 — Psychoeducation and supportive bereavement care
Explain oscillation of grief, continuing bonds, and when to seek help. Community bereavement services, peer support, and culturally congruent rituals are appropriate for adaptive grief. Avoid forced "closure" rhetoric that shames ongoing love.[15][17]
Step 2 — Grief-focused psychotherapy (first-line for PGD / complicated grief)
Complicated Grief Treatment (CGT) is the landmark named package. The original randomised trial showed CGT superior to interpersonal psychotherapy for complicated grief.[1] A later RCT supported CGT efficacy in older adults.[3] The optimising trial examined CGT with or without citalopram and remains the key modern reference for combined treatment questions.[2]
Name CGT ingredients in MEQs: grief psychoeducation; aspirational goals for a life of meaning after loss; revisiting the story of the death (imaginal work); reconnecting with the deceased in adaptive ways (for example imaginal conversation); graded work on avoided situations; behavioural activation toward restoration; and addressing guilt, anger, and self-blame carefully. Mediator analyses support reduction of avoidance and maladaptive beliefs as change mechanisms.[1][2][20]
CBT approaches targeting exposure to avoided reminders plus behavioural activation and anti-rumination strategies have randomised support, including internet-delivered formats.[14] Network meta-analysis of psychotherapies for adult PGD supports psychological treatment efficacy as a class — quote direction of effect and name specific packages when possible.[13] Suicide-loss HEAL analyses support that complicated grief treatments are relevant in this high-stigma subgroup.[12]
Step 3 — Pharmacotherapy (selective)
Antidepressants are not first-line monotherapy for pure PGD when grief-focused therapy is available and indicated.[2][8][13]
Treat comorbid major depression or severe anxiety with standard regimens, in parallel with grief-focused therapy when possible. Example adult regimen for comorbid MDD: sertraline 25–50 mg orally each morning, early review in 1–2 weeks for activation/suicidality (especially under 25 years), titrate toward 50–100 mg as tolerated, measurement-based PHQ-9 plus grief scale monitoring, several weeks at therapeutic dose. The optimising CGT trial informs examiners' questions about citalopram combined with CGT — know the trial exists and that therapy remains central rather than claiming a unique "PGD dose" separate from depression practice.[2][8]
Avoid routine long-term benzodiazepines. Avoid antipsychotics for ordinary grief without psychotic indications.[8]
Step 4 — Specialist escalation
Escalate for high suicide risk, diagnostic uncertainty (bipolar, psychosis, organic disease), failed adequate grief-focused therapy, heavy substance comorbidity, homicide/disaster mass-casualty contexts, or complex child protection issues after parental death.[8][12]
ANZ practice maps onto GP shared care, public and private psychology for grief-focused CBT/CGT-informed work, bereavement services, and secondary mental health for risk or comorbidity. Apply cultural safety for Māori, Aboriginal and Torres Strait Islander peoples; partner with community and spiritual supports rather than imposing purely Western timelines. Prescribe within PBS/PHARMAC constraints.[8][17]
Specific subtypes and scenarios
Widow(er)hood after chronic illness. Caregiver exhaustion, anticipatory grief, and relief-guilt mixtures; assess medical self-neglect in the survivor.[5]
Child and perinatal loss. High PGD risk; disenfranchised grief when social networks minimise the loss; partner discord common.[5][16]
Suicide bereavement. Stigma, guilt, trauma, and elevated complicated grief load — HEAL treatment data are examinable.[12]
Homicide, disaster, war, refugee multiple losses. Trauma–grief comorbidity is the rule; sequence safety, trauma care, and grief work thoughtfully.[16]
COVID-disrupted funerals. Unfinished leave-taking and isolation are maintaining factors; validate ritual repair where possible.[19]
Older adults. High loss exposure and loneliness; CGT RCT evidence specifically includes elderly samples; start any medication low and slow.[3]
Children and adolescents. DSM duration threshold ≥6 months; developmental presentations (regression, school failure, play); caregiver systems are part of treatment.[4][8]
Complications and pitfalls
Classic pitfalls: inventing hybrid duration numbers; using only antidepressants without grief-focused therapy for PGD; chronic benzodiazepines; forced "moving on" shaming of continuing bonds; missing suicide risk and reunion planning; ignoring cultural-norm criterion in DSM/ICD; soft-labelling full MDD as grief alone.[2][8][9][17]
Prognosis and disposition
Most bereaved people adapt without meeting PGD criteria. A clinically important minority develop persistent impairing grief; risk is higher after unnatural death and in those with prior vulnerability.[5][16] Grief-focused psychotherapies improve complicated/prolonged grief severity; comorbid depression trajectories influence response and should be treated when present.[1][2][13]
Disposition ladder: primary care and bereavement services → specialist psychology/psychiatry for PGD, high risk, or comorbidity → crisis/inpatient care when safety requires it. Expect anniversary and birthday flares; plan proactive review around those dates.[8][15]
Special populations and cultural care
Cultural formulation is diagnostic, not optional colour. Both DSM-5-TR and ICD-11 require that the reaction exceed expected cultural and religious norms — meaning the clinician must know something about those norms or consult cultural brokers.[7][17] Qualitative work from New Delhi and mixed-methods reviews of East and Southeast Asian mourning rituals show that ritual participation, family roles, and meaning systems shape both distress and recovery pathways; pathologising culturally coherent practices is a formulation error.[17][18]
Indigenous and migrant care in ANZ requires interpreter use, family inclusion as appropriate, and respect for spiritual continuing bonds. Intellectual disability needs concrete language and carer-system support after a carer's death.[17][18]
Evidence, guidelines and controversies
Therapy landmarks. Shear 2005 JAMA CGT RCT; Shear 2014 elderly CGT RCT; Shear 2016 optimising CGT ± citalopram; Eisma/Boelen internet exposure and behavioural activation RCT; Hao 2024 network meta-analysis of psychotherapies for adult PGD.[1][2][3][13][14]
Nosology landmarks. Prigerson 2009 psychometric validation of proposed PGD criteria; Maciejewski 2016 PGD≈PCBD convergence; Mauro 2019 ICD-11 clinical utility; Simon 2020 commentary supporting a grief-related DSM diagnosis.[4][6][7][8]
Depression interface. Removal of bereavement exclusion literature (Zisook/Iglewicz) and Kendler 2008 comparison of bereavement-related and other stressor-related MDD.[9][10][11]
Mechanisms and context. Dual process model decade review; COVID mental-health framing of related deaths; cultural validity challenges to DSM-5-TR criteria.[15][17][19]
Controversies examiners love: 6 versus 12 month duration thresholds; risk of medicalising love and mourning; whether antidepressants help pure PGD; continuing bonds versus older detachment models; cultural validity of symptom lists.[7][8][17]
Exam pearls
GRIEVED
Self-test: high-yield traps
- DSM-5-TR adult duration? At least 12 months after the death.
- ICD-11 duration? More than 6 months (atypically long for the culture).
- Core features? Yearning/longing or preoccupation with the deceased.
- Is normal grief a disorder? No.
- Can MDD be diagnosed while grieving? Yes, if full criteria met (no bereavement exclusion).
- First-line for PGD? Grief-focused psychotherapy (CGT/CBT), not automatic SSRI.
- Named CGT trial? Shear 2005 JAMA; later elderly and optimising trials.
- Cultural criterion? Reaction must exceed expected social/cultural/religious norms.[1][2][3][4][7][8][9]
References
- [1]Shear K, Frank E, Houck PR, Reynolds CF 3rd Treatment of complicated grief: a randomized controlled trial JAMA, 2005.PMID 15928281
- [2]Shear MK, Reynolds CF 3rd, Simon NM, Zisook S, et al. Optimizing Treatment of Complicated Grief: A Randomized Clinical Trial JAMA Psychiatry, 2016.PMID 27276373
- [3]Shear MK, Wang Y, Skritskaya N, Duan N, et al. Treatment of complicated grief in elderly persons: a randomized clinical trial JAMA Psychiatry, 2014.PMID 25250737
- [4]Prigerson HG, Horowitz MJ, Jacobs SC, Parkes CM, et al. Prolonged grief disorder: Psychometric validation of criteria proposed for DSM-V and ICD-11 PLoS Med, 2009.PMID 19652695
- [5]Lundorff M, Holmgren H, Zachariae R, Farver-Vestergaard I, et al. Prevalence of prolonged grief disorder in adult bereavement: A systematic review and meta-analysis J Affect Disord, 2017.PMID 28167398
- [6]Maciejewski PK, Maercker A, Boelen PA, Prigerson HG "Prolonged grief disorder" and "persistent complex bereavement disorder", but not "complicated grief", are one and the same diagnostic entity World Psychiatry, 2016.PMID 27717273
- [7]Mauro C, Reynolds CF, Maercker A, Skritskaya N, et al. Prolonged grief disorder: clinical utility of ICD-11 diagnostic guidelines Psychol Med, 2019.PMID 29909789
- [8]Simon NM, Shear MK, Reynolds CF, Cozza SJ, et al. Commentary on evidence in support of a grief-related condition as a DSM diagnosis Depress Anxiety, 2020.PMID 31916663
- [9]Iglewicz A, Seay K, Zetumer SD, Zisook S The removal of the bereavement exclusion in the DSM-5: exploring the evidence Curr Psychiatry Rep, 2013.PMID 24136623
- [10]Zisook S, Corruble E, Duan N, Iglewicz A, et al. The bereavement exclusion and DSM-5 Depress Anxiety, 2012.PMID 22495967
- [11]Kendler KS, Myers J, Zisook S Does bereavement-related major depression differ from major depression associated with other stressful life events? Am J Psychiatry, 2008.PMID 18708488
- [12]Zisook S, Shear MK, Reynolds CF, Simon NM, et al. Treatment of Complicated Grief in Survivors of Suicide Loss: A HEAL Report J Clin Psychiatry, 2018.PMID 29617064
- [13]Hao F, Qiu F, Liang Z, Li P Psychotherapies for prolonged grief disorder in adults: A systematic review and network meta-analysis Asian J Psychiatr, 2024.PMID 38970900
- [14]Eisma MC, Boelen PA, van den Bout J, Stroebe W, et al. Internet-Based Exposure and Behavioral Activation for Complicated Grief and Rumination: A Randomized Controlled Trial Behav Ther, 2015.PMID 26520217
- [15]Stroebe M, Schut H The dual process model of coping with bereavement: a decade on Omega (Westport), 2010.PMID 21058610
- [16]Comtesse H, Smid GE, Rummel AM, Spreeuwenberg P, et al. Cross-national analysis of the prevalence of prolonged grief disorder J Affect Disord, 2024.PMID 38220101
- [17]Moore BS, da Silva JP, Farias M Diagnosing Prolonged Grief Disorder: Cultural Challenges to the DSM-5-TR Criteria Cult Med Psychiatry, 2025.PMID 40830691
- [18]Sarkar S, Gupta P, Sahu A, Anwar N, et al. A qualitative phenomenological exploration of prolonged grief in New Delhi, India Transcult Psychiatry, 2023.PMID 37993997
- [19]Simon NM, Saxe GN, Marmar CR Mental Health Disorders Related to COVID-19-Related Deaths JAMA, 2020.PMID 33044510
- [20]Glickman K, Shear MK, Wall MM Mediators of Outcome in Complicated Grief Treatment J Clin Psychol, 2017.PMID 27755654