Psych · General adult psychiatry — personality disorders
Histrionic personality disorder
Also known as HPD · Histrionic PD · Cluster B histrionic · Dramatic personality disorder (historical teaching) · Hysterical personality (historical)
Exam-exhaustive fellowship reference on histrionic personality disorder — DSM-5-TR and ICD-11 criteria, construct-validity controversies, epidemiology, interpersonal mechanisms, differentials (BPD, NPD, mania, somatization, ASPD pathways), assessment, frame-based psychotherapy, comorbidity-only pharmacotherapy, countertransference. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Histrionic personality disorder (HPD) is a low-weight but high-trap Cluster B topic. FRANZCP MEQs and vivas test criteria accuracy, sex-bias awareness, differentials with BPD/mania/NPD, and honest management limits. MRCPsych CASC tests non-stigmatising explanation and boundary language. ABPN items test DSM thresholds, the HPD–ASPD–somatization pathway hypothesis, and construct-validity debates. A candidate who overclaims validity or under-assesses risk after theatrical self-harm fails at consultant standard.[1][3][5]
Overview and definition
HPD is an enduring, inflexible pattern of excessive emotionality and attention-seeking that begins by early adulthood, is present across contexts, and causes distress or impairment — not better explained solely by another mental disorder, substance, or medical condition. The person is often uncomfortable when not the centre of attention, may use appearance or seductive behaviour to secure an audience, shows rapidly shifting shallow affect, and forms relationships that feel more intimate than the mutual history supports.[1][5]
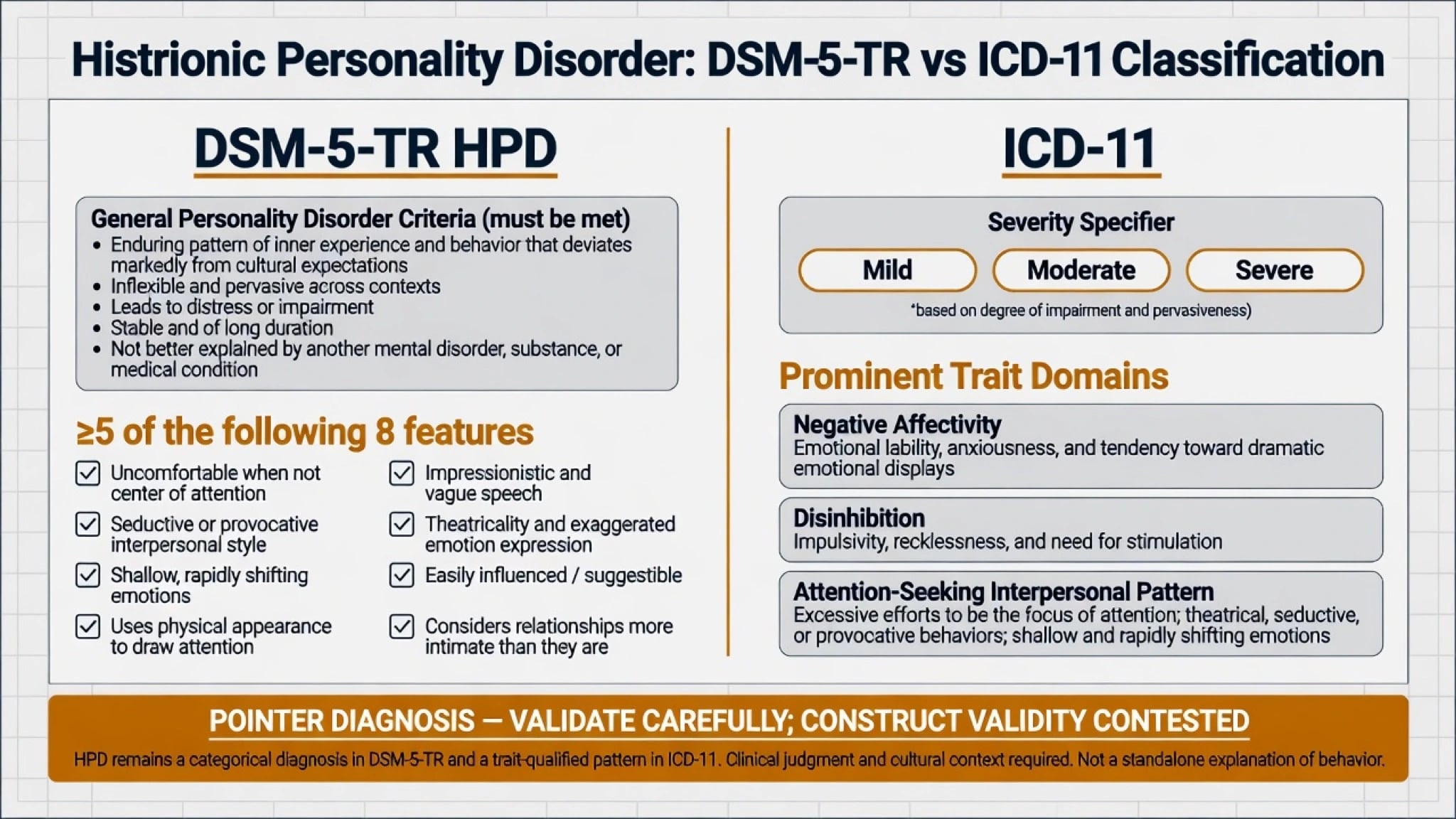
DSM-5-TR structure you must reproduce. After general personality disorder criteria are met, HPD requires five or more of eight features: (1) is uncomfortable in situations in which he or she is not the centre of attention; (2) interaction with others is often characterised by inappropriate sexually seductive or provocative behaviour; (3) displays rapidly shifting and shallow expression of emotions; (4) consistently uses physical appearance to draw attention to self; (5) has a style of speech that is excessively impressionistic and lacking in detail; (6) shows self-dramatisation, theatricality, and exaggerated expression of emotion; (7) is suggestible (easily influenced by others or circumstances); (8) considers relationships to be more intimate than they actually are.[1][5]
ICD-11 framing. Personality disorder is graded by severity of self and interpersonal dysfunction (mild, moderate, severe), then qualified with trait domain descriptors. HPD-like presentations often map to negative affectivity (emotional lability) and disinhibition, with interpersonal attention-seeking as a clinical pattern rather than a proven biological taxon. Name which system you are applying in viva answers.[1][2]
AMPD language (exam polish). Criterion A: impairment in identity (externalised self-worth), self-direction, empathy (shallow attunement), and intimacy (provisional intensity). Criterion B traits often include attention-seeking and emotional lability. Use this language even when services code categorical DSM.[1][12]
Pointer diagnosis. Empirical work questions whether HPD is a coherent, discrete category versus a mixture of borderline-spectrum and “hysterical” personality features; Bakkevig and Karterud challenge construct validity, and Blagov and Westen describe borderline and hysterical subtypes that reorganise many cases labelled histrionic. Mature answers keep the criteria fluent and refuse naive reification.[1][2]
Classification and nosology
DSM-5-TR categorical
- General PD criteria + ≥5 of 8 features
- Cluster B (dramatic/erratic) teaching scaffold
- Impressionistic speech and provisional intimacy are high-yield
- Must begin by early adulthood and be pervasive
ICD-11 dimensional
- Severity of personality dysfunction first
- Traits: negative affectivity, disinhibition, attention-seeking pattern
- Optional pattern language varies by service
- Better for intensity and stepped-care decisions
Validity controversy
- Coherence of pure HPD category challenged
- Borderline vs hysterical subtype reorganisation proposed
- High overlap with other Cluster B traits
- Pointer diagnosis: re-map when formulation deepens
Normal expressiveness
- Culture and temperament are not HPD
- Single-episode theatricality under stress is not PD
- Impairment and pervasiveness required
- Sex stereotypes must not drive diagnosis
Historical “hysteria” roots still shape stigma and sex bias; Novais and colleagues summarise how modern HPD criteria inherit older constructs. Examiners reward candidates who can state criteria without moralising language and who name the validity debate without discarding clinical utility of recognising attention-seeking interpersonal strategies that cause harm.[5][1][2]
Epidemiology and risk factors
Headline epidemiology candidates must own
Community surveys establish that personality disorders as a class are common enough to matter in every general adult clinic, with substantial disability and comorbidity; HPD specifically is less frequent than several other PD categories and shows method-dependent prevalence. Revised NESARC analyses refine gender patterns and substance comorbidity across PD diagnoses — dual diagnosis is expected, not exceptional.[7][8][9]
Sex and pathway hypotheses. Clinical samples often show female predominance for HPD labels. Cale and Lilienfeld examine whether HPD and ASPD can function as sex-differentiated manifestations related to psychopathic propensities; Lilienfeld and colleagues classically linked HPD pathways toward ASPD (more often coded in men) and somatization (more often coded in women) in some formulations. Use these as exam hypotheses, not crude biological sex essentialism — diagnostic bias is real.[3][4]
Risk and aetiology. Developmental overvaluation of appearance or performance, inconsistent attention, insecure attachment, modelling of dramatic affect regulation, and trauma can feed externalised self-worth. None alone makes the diagnosis. Late-onset dramatic personality change is organic and affective until proven otherwise.[5][1]
Pathophysiology and mechanisms
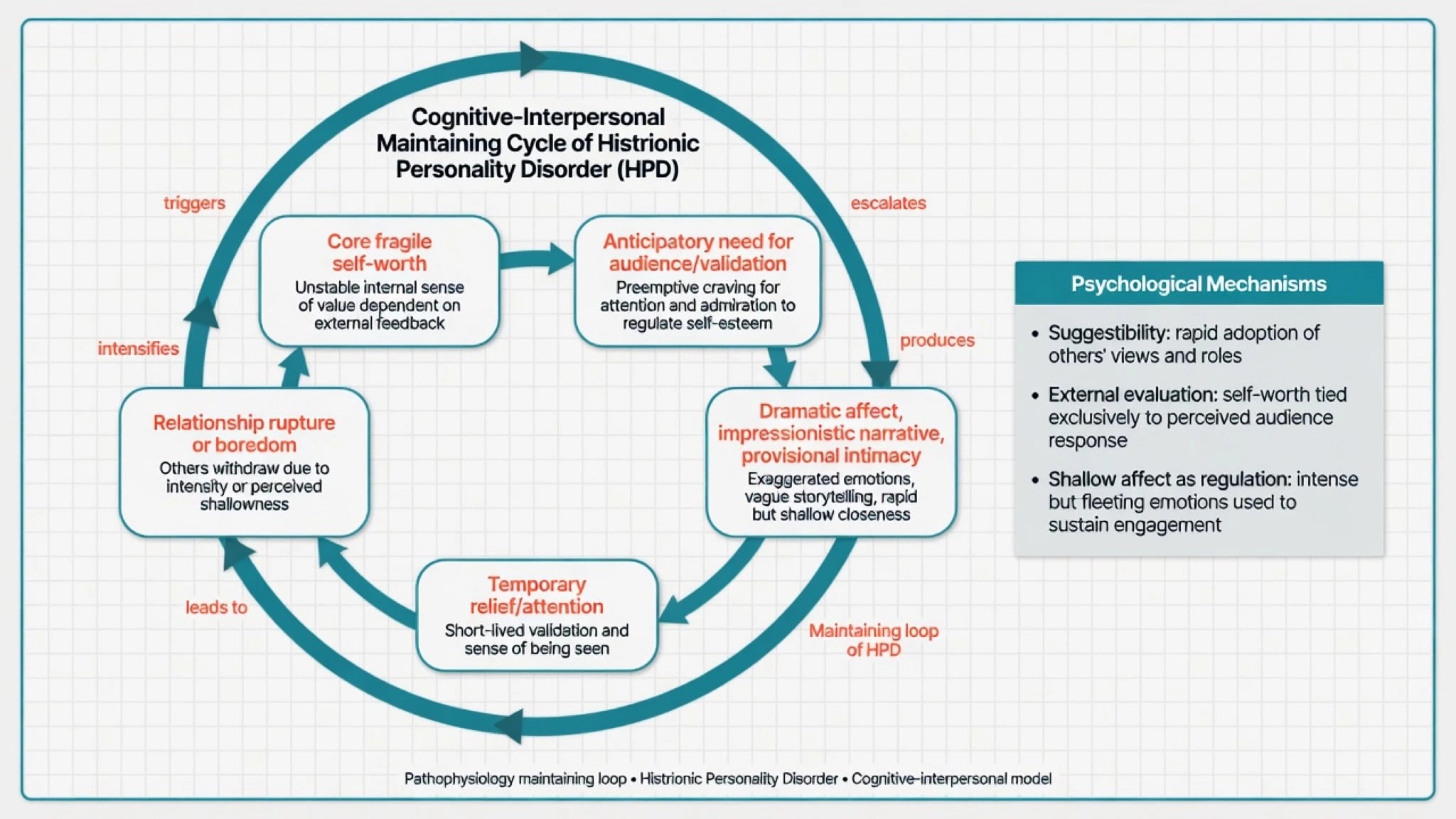
Interpersonal maintaining loop. Core fragility of self-worth generates a need for external validation. Dramatic affect, impressionistic storytelling, seductive or provisional intimacy, and appearance-focused bids produce short-term connection or care. When depth, consistency, or mutuality is required, relationships rupture or cool — confirming the need for the next performance. Suggestibility amplifies influence by charismatic others and by clinical teams who over- or under-respond.[1][2][6]
Affect and cognition. Emotions are vivid but may lack depth and endurance; speech is colourful and detail-poor; evaluation of self is external. This is a formulation for therapy targets (building internal self-representation, affect differentiation, realistic intimacy), not a claim of a diagnostic brain scan.[1][6]
Overlap mechanisms with BPD and NPD. Emotion dysregulation and identity instability pull toward BPD; status/admiration regulation and envy pull toward pathological narcissism. HPD sits in the attention-seeking theatrical zone; many patients meet mixed criteria — dual diagnosis when operational thresholds are met is better than forced purity.[2][12][13][14]
Clinical presentation
Core picture. Patients may present after a relationship rupture, public embarrassment, medical crisis, or workplace conflict. History reveals a pattern of intense but short-lived relationships, discomfort when ignored, and use of charm, crisis, or appearance to recruit care. MSE: theatrical affect, impressionistic narrative, possible seductive or overly familiar style, suggestibility, variable insight, and rapid shifts when attention is withdrawn or shared.[1][5]
Healthcare utilisation. High medical contact, dramatic symptom reports, and frustration among teams are common. Discriminate carefully from somatic symptom disorder, factitious presentations, and genuine medical disease — all can co-exist with personality patterns.[4][1]
Crisis presentation. After rejection or loss of audience, depressive collapse, suicidal ideation, or self-harm of variable lethality may occur. Communicative or interpersonal functions of self-harm do not make risk low. Assess intent, plan, means, depression, substances, and protective factors fully.[1][14]
Male and non-stereotyped presentations. Attention-seeking via risk-taking, status performance, or antisocial behaviour may be mislabelled as pure ASPD/NPD; do not require a caricature of seductive theatricality to consider HPD features.[3][4]
Differential diagnosis
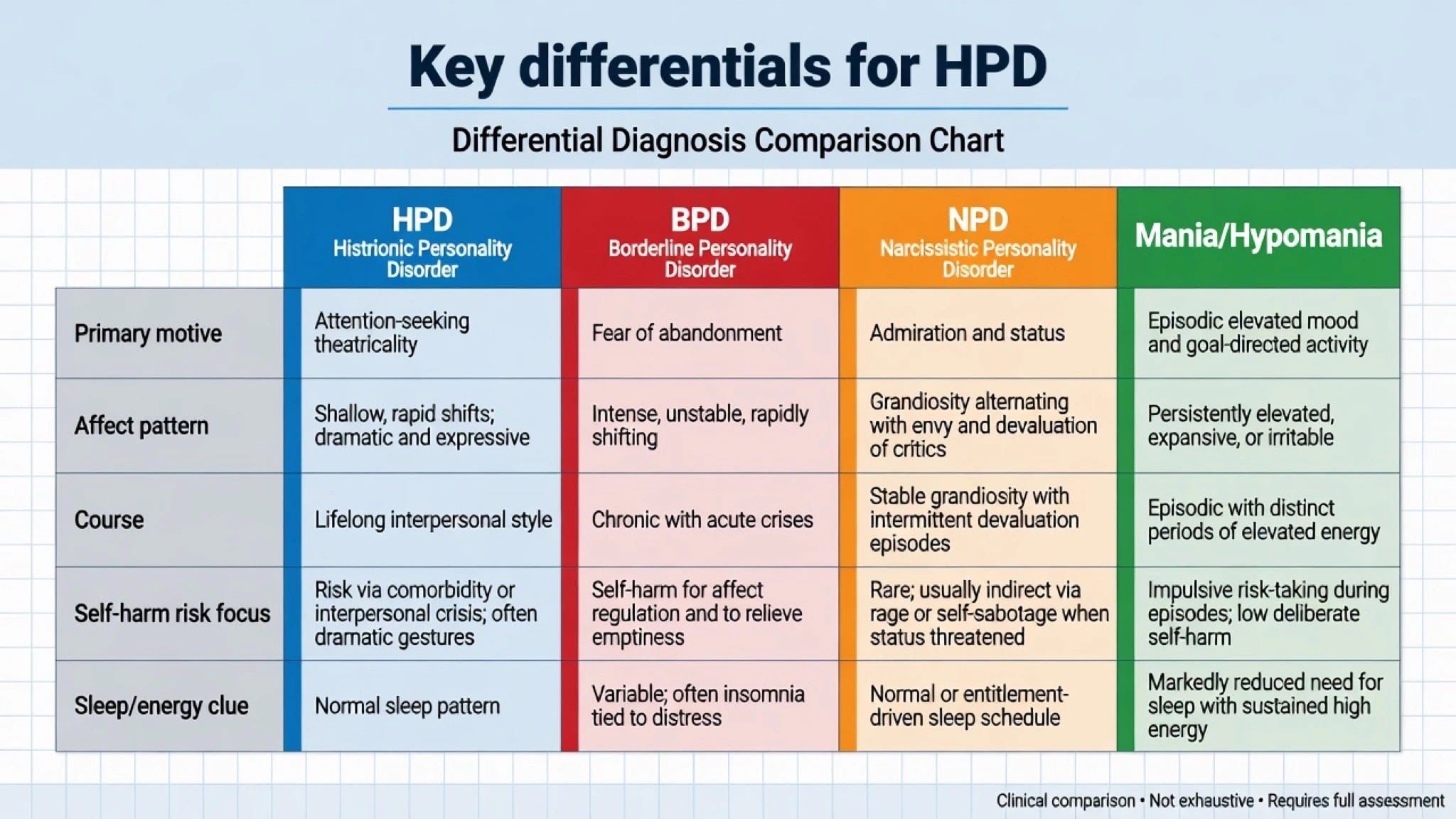
HPD vs BPD
- BPD: abandonment fear, emptiness, self-harm as regulation, identity diffusion
- HPD: attention-seeking theatricality, shallower rapid affect shifts
- Overlap common — dual diagnosis when both criteria met
- Do not use HPD to avoid offering BPD-informed care
HPD vs NPD
- NPD: admiration/status, entitlement, envy, devaluation of critics
- HPD: attention for its own sake, suggestibility, provisional intimacy
- Both may charm and exploit; motive differs
- Pathological narcissism includes vulnerable poles
HPD vs mania
- Mania/hypomania: days–weeks, reduced sleep need, energy, goal-direction
- HPD: lifelong interpersonal style
- Substance-induced disinhibition mimics both
- Never lock PD during untreated mania
Somatic / other
- Somatic symptom disorder: health anxiety and care-seeking focus
- Factitious/malingering: conscious production for sick role or secondary gain
- Organic late-onset change: TBI, FTD, endocrine
- PTSD and dissociation can produce dramatic affect
The classic HPD–ASPD–somatization pathway hypothesis remains examinable as history of ideas and sex-bias discussion, not as a mandatory clinical algorithm.[3][4][12]
Clinical and bedside assessment
History structure. Developmental attention patterns and attachment; school and peer reputation for drama or seduction; relationship chronology (idealisation, rapid intimacy claims, serial rupture); occupational performance under evaluation; substance use; medical care-seeking; prior therapy dropouts; current crisis trigger; what help is sought today. Obtain collateral — self-report is often impressionistic.[1][5]
MSE focus. Rapport (charm, familiarity, flirtation, or rage when not preferred), affect theatricality versus depth, speech impressionism, thought content (rejection, abandonment, envy), insight, judgement, and in-session attention bids. Document boundary tests early.[1][11]
Risk. Suicide and self-harm with full formulation; intimate partner violence (victim or perpetrator); sexual exploitation; child safeguarding; public behavioural risk when disinhibited. Capacity is decision-specific. Use local Mental Health Act principles when statutory criteria are met — do not invent section numbers.[1][14]
Tools (conceptual). SCID-5-PD / IPDE for categorical PD diagnosis; depression and anxiety scales; BPD screens when indicated; substance screens. Tools support longitudinal clinical diagnosis.[7][14]
Investigations
HPD has no laboratory gold standard. Investigate to exclude mimics and prepare for medication when used: TSH, FBC, U&E, LFT, glucose/lipids, pregnancy test when relevant, urine drug screen when substances may explain behaviour, ECG when cardiac risk or QTc-risk drugs are planned. Neuroimaging or EEG only when late-onset change, focal neurology, seizures, or cognitive decline fire. Screen systematically for BPD, bipolar spectrum, major depression, PTSD, substance use, and somatic symptom presentations because they change the map more than the HPD label alone.[1][12][14]
Management — acute / emergency
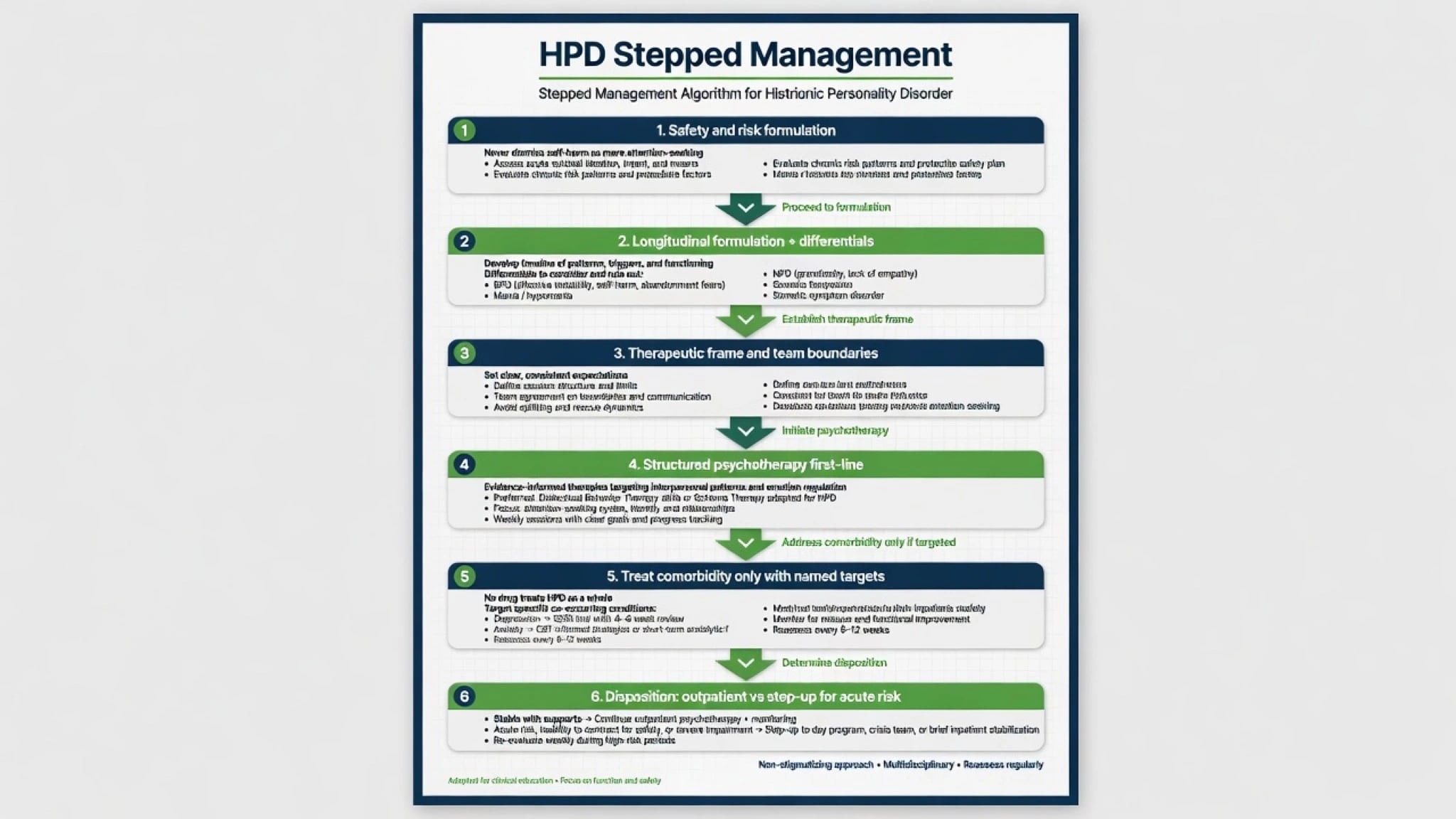
Acute principles. Validate emotional pain without rewarding dangerous theatre with special privileges that split the team. Clear consistent frame across nursing, medical, and community staff. De-escalation first for behavioural crisis; if pharmacological restraint is required for imminent safety, use local rapid-tranquillisation protocols with monitoring — not a long-term “personality sedative.” Assess alcohol and other substances. Jurisdiction-specific legal options only when criteria met.[1][11]
Management — definitive and stepwise
Psychotherapy and frame first-line
Structured psychological care with a firm, predictable frame is the core of definitive management. Goals: increase affective depth and differentiation, reduce reliance on external validation, build realistic intimacy, and interrupt crisis-as-communication when safer alternatives exist. Change-process research in psychotherapy for patients presenting with HPD examines session-level mechanisms of improvement — the fellowship takeaway is that HPD is treatable as an interpersonal pattern, not a moral sentence, even though HPD-specific RCT density is thinner than for BPD specialised programmes.[6][1]
Schema therapy and broader PD evidence. When global self-concept and interpersonal patterns dominate, schema therapy has multicentre RCT support for personality disorders (Bamelis and colleagues), including samples beyond BPD-only pathways — name the trial honestly without claiming an HPD-only miracle protocol.[10]
Alliance stance. Warmth with limits. Predict idealisation, seduction, and devaluation. Team consistency prevents splitting. Supervision is part of competence when eroticised, rescuing, or hostile countertransference arises — Betan and colleagues provide empirical mapping of countertransference patterns to personality pathology that examiners still respect.[11][12]
Pharmacotherapy — comorbidity only
No medication treats HPD as a whole disorder. Prescribe for comorbid major depression, anxiety disorders, or other clear targets, with measurement and stop/review dates. Avoid chronic benzodiazepines as personality treatment and avoid antipsychotic polypharmacy without psychotic phenomena or another indication.[1][10]
Named adult example when an examiner forces a plan (individualise; check local product information). For comorbid major depression without bipolarity: sertraline 50 mg orally once daily, review in 1–2 weeks for activation, anxiety increase and suicidality (especially under age 25), titrate toward a commonly used therapeutic range of 50–150 mg daily as tolerated, with response review at 6–12 weeks at an adequate dose and limited early supply if overdose risk is elevated. Pair with psychotherapy and frame work; counsel sexual side effects and discontinuation syndrome. This is comorbidity treatment, not a cure of personality.[1][10][14]
Care system and disposition
Most patients are managed in outpatient psychotherapy and general adult pathways. Step up for acute suicide risk, severe depression, mania, or unsafe behaviour. Step down when interpersonal strategies stabilise and crises reduce. Primary care liaison matters when somatic presentations dominate healthcare use.[1][6][7]
Australian and New Zealand practice emphasises stepped mental health care, access to psychological therapies where available, trauma-informed engagement, and culturally safe practice. Local Mental Health Act provisions govern involuntary care — name least-restrictive principles, not invented foreign section numbers. Coordinate with primary care for SSRI prescribing and monitoring when specialist waitlists are long.[1][10]
Specific subtypes and scenarios
HPD with BPD-spectrum overlap. Prioritise emotion dysregulation, self-harm pathways, and structured BPD-informed care when criteria are met; do not use HPD as a reason to withhold evidence-based approaches used in BPD services.[2][14]
HPD-like presentation in mania. Treat bipolarity first; reassess personality only after euthymia and substance clearance.[12]
High medical utilisation / somatic focus. Parallel medical work-up and psychiatric formulation; avoid either pure psychologising of disease or pure medicalisation of interpersonal distress.[4]
Substance use as facilitator. Dual-diagnosis pathway; substances amplify disinhibition and relationship risk.[9]
Male attention-seeking via risk/status. Avoid sex-stereotyped underdiagnosis; use criteria and collateral, not caricature.[3][4]
Ward splitting and boundary testing. Unified team plan, predictable visits, no secret special exceptions, supervision for staff countertransference.[11]
Complications and pitfalls
Classic pitfalls: dismissing all self-harm as attention-seeking; sex-biased overdiagnosis in women and underdiagnosis in men; collapsing HPD into BPD or NPD without discriminators; boundary violations (special treatment, sexual dual relationships, punitive discharge); chronic benzodiazepines or polypharmacy as personality treatment; missing mania, organic change, or severe depression; diagnosing PD from a single dramatic interview; pejorative “drama queen” language in the record.[1][2][3][11]
Prognosis and disposition
Without structured care, patterns of unstable relationships, crises, and healthcare friction often persist. Categorical HPD is frequently longitudinally less stable than BPD; many patients re-map diagnostically as formulation deepens. With alliance, frame consistency, psychotherapy engagement, and treatment of comorbidity, interpersonal strategies and crisis frequency can improve. Disposition is usually outpatient; hospitalisation is for risk or severe illness, not for the PD label alone.[1][2][6][10]
Special populations
Youth. Dramatic affect and identity experimentation are common in adolescence. Do not casually assign permanent HPD labels without longitudinal evidence of pervasive impairment beginning by early adulthood patterns.[2][5]
Older adults. Lifelong patterns may decompensate after bereavement or loss of audience/role. New late-life dramatic change is organic/mood until proven otherwise.[1]
Pregnancy and parenting. Treat depression carefully; minimise unnecessary polypharmacy; support attachment, safety, and partner/family dynamics that may include IPV risk.[1][10]
Cultural formulation. Expressive cultural communication styles are not HPD. Sex-role stereotypes must not drive diagnosis. In ANZ practice, Indigenous cultural safety and family-inclusive care are competencies.[5][1]
Evidence, guidelines and controversies
Construct validity anchors: Bakkevig and Karterud 2010; Blagov and Westen 2008; Novais historical roots 2015.[1][2][5]
Sex and pathway literature: Cale and Lilienfeld 2002; Lilienfeld and colleagues 1986 on HPD, ASPD, and somatization relationships.[3][4]
Epidemiology: Grant NESARC; Lenzenweger NCS-R; Trull revised NESARC PD; Tomko community BPD characteristics for comorbidity and utilisation context on the Cluster B spectrum.[7][8][9][14]
Treatment and process: Babl psychotherapy change processes 2023; Bamelis schema therapy RCT; Betan countertransference; Caligor and Pincus work for NPD differentials and pathological narcissism framing.[6][10][11][12][13]
Mature controversies. Whether HPD should remain a freestanding category; how far ICD-11 severity should replace Cluster B labels; how to resource long-term psychotherapy outside specialist clinics; and how to name sex bias without erasing genuine clinical patterns of attention-seeking interpersonal harm.[1][2][5]
Exam pearls
HISTRIONIC — viva checklist
HISTRION
≥5 of 8 DSM features after general PD criteria
Impressionistic speech; intimacy claims exceed reality
Shallowness of rapidly shifting affect
Theatricality and need to be centre of attention
Re-map to BPD/mania/NPD — pointer diagnosis
Investigate late-onset change; no lab gold standard
Only comorbidity meds; no drug cures HPD
Never dismiss self-harm as mere attention-seeking
60-second oral summary
HPD is DSM ≥5/8 excessive emotionality and attention-seeking with general PD criteria — a Cluster B pointer diagnosis with contested construct validity (Bakkevig, Blagov). Discriminate BPD (abandonment/self-harm regulation), NPD (admiration/status), mania (episodic energy and reduced sleep), and somatization pathways; dual diagnosis is common. Assess risk fully after theatrical crises. Treat with firm frame and structured psychotherapy (process evidence; schema therapy PD RCT support); medicate comorbidity only (e.g. sertraline for depression with dose and review). Watch sex bias and countertransference. No drug cures HPD as a whole; hope is realistic change in interpersonal strategies.[1][2][6][10][11]
References
- [1]Bakkevig JF, Karterud S Is the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, histrionic personality disorder category a valid construct? Compr Psychiatry, 2010.PMID 20728002
- [2]Blagov PS, Westen D Questioning the coherence of histrionic personality disorder: borderline and hysterical personality subtypes in adults and adolescents J Nerv Ment Dis, 2008.PMID 19008729
- [3]Cale EM, Lilienfeld SO Histrionic personality disorder and antisocial personality disorder: sex-differentiated manifestations of psychopathy? J Pers Disord, 2002.PMID 11881161
- [4]Lilienfeld SO, Van Valkenburg C, Larntz K, Akiskal HS The relationship of histrionic personality disorder to antisocial personality and somatization disorders Am J Psychiatry, 1986.PMID 3717392
- [5]Novais F, Araújo A, Godinho P Historical roots of histrionic personality disorder Front Psychol, 2015.PMID 26441812
- [6]Babl A, Gómez Penedo JM, Berger T, Schneider N, Sachse R, Kramer U Change processes in psychotherapy for patients presenting with histrionic personality disorder Clin Psychol Psychother, 2023.PMID 35776063
- [7]Grant BF, Hasin DS, Stinson FS, Dawson DA, et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions J Clin Psychiatry, 2004.PMID 15291684
- [8]Lenzenweger MF, Lane MC, Loranger AW, Kessler RC DSM-IV personality disorders in the National Comorbidity Survey Replication Biol Psychiatry, 2007.PMID 17217923
- [9]Trull TJ, Jahng S, Tomko RL, Wood PK, Sher KJ Revised NESARC personality disorder diagnoses: gender, prevalence, and comorbidity with substance dependence disorders J Pers Disord, 2010.PMID 20695803
- [10]Bamelis LL, Evers SM, Spinhoven P, Arntz A Results of a multicenter randomized controlled trial of the clinical effectiveness of schema therapy for personality disorders Am J Psychiatry, 2014.PMID 24322378
- [11]Betan E, Heim AK, Zittel Conklin C, Westen D Countertransference phenomena and personality pathology in clinical practice: an empirical investigation Am J Psychiatry, 2005.PMID 15863790
- [12]Caligor E, Levy KN, Yeomans FE Narcissistic personality disorder: diagnostic and clinical challenges Am J Psychiatry, 2015.PMID 25930131
- [13]Pincus AL, Lukowitsky MR Pathological narcissism and narcissistic personality disorder Annu Rev Clin Psychol, 2010.PMID 20001728
- [14]Tomko RL, Trull TJ, Wood PK, Sher KJ Characteristics of borderline personality disorder in a community sample: comorbidity, treatment utilization, and general functioning J Pers Disord, 2014.PMID 25248122