Psych · General adult psychiatry — OCRD
Hoarding and related disorders
Also known as Hoarding disorder · Compulsive hoarding · Pathological hoarding · Animal hoarding · Diogenes syndrome · Severe domestic squalor · OCRD · SI-R · Clutter Image Rating
Exam-exhaustive fellowship reference on hoarding disorder — DSM-5-TR/ICD-11 OCRD criteria; vs OCD, ADHD, dementia and squalor; Frost–Hartl model; SI-R/CIR/ADL assessment; specialised CBT (waitlist RCT, meta-analysis); limited pharmacotherapy signals (paroxetine, venlafaxine XR); capacity, multiagency risk and forced-cleanout pitfalls. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Hoarding disorder (HD) is a high-yield OCRD discriminator topic at FRANZCP, MRCPsych, and ABPN level. Examiners test DSM-5-TR separation from OCD, Frost–Hartl maintaining mechanisms, home-based assessment tools, specialised CBT components, the limits of pharmacotherapy, and the interface with capacity, squalor, animal welfare, and multiagency risk. A candidate who reads only this topic should defend diagnosis, differential, and stepped care at consultant depth.[2][4][9]
Overview and definition
HD is defined by persistent difficulty discarding or parting with possessions, regardless of actual value, due to a perceived need to save items and distress associated with discarding. Accumulation produces clutter that congests and substantially compromises the intended use of living areas (or living areas would be unusable without third-party intervention). Distress or impairment is required; the picture is not better explained by another medical condition or mental disorder.[2][9]
Clinical essence for viva. The core problem is the discarding decision and attachment to possessions, not mere messiness. Acquisition (free items, buying) is common and is specified when present. Insight ranges from good to delusional-level conviction that saving is necessary.[2][9]
DSM-5-TR. HD sits in the obsessive-compulsive and related disorders (OCRD) chapter. Specifiers: insight (good/fair; poor; absent insight/delusional beliefs) and with excessive acquisition.[2]
ICD-11. Hoarding disorder is classified among obsessive-compulsive or related disorders with analogous core features; state which manual you are using when boundaries with OCD are examined.[2][4]
Why separated from OCD. Phenomenology (ego-syntonic attachment vs ego-dystonic obsessions), comorbidity patterns, heritability signals, neural decision-making findings, and poorer response to standard OCD ERP/SSRI packages support a distinct syndrome — while secondary hoarding as an OCD symptom still exists and must be formulated separately.[2][3][4]
Classification and related constructs
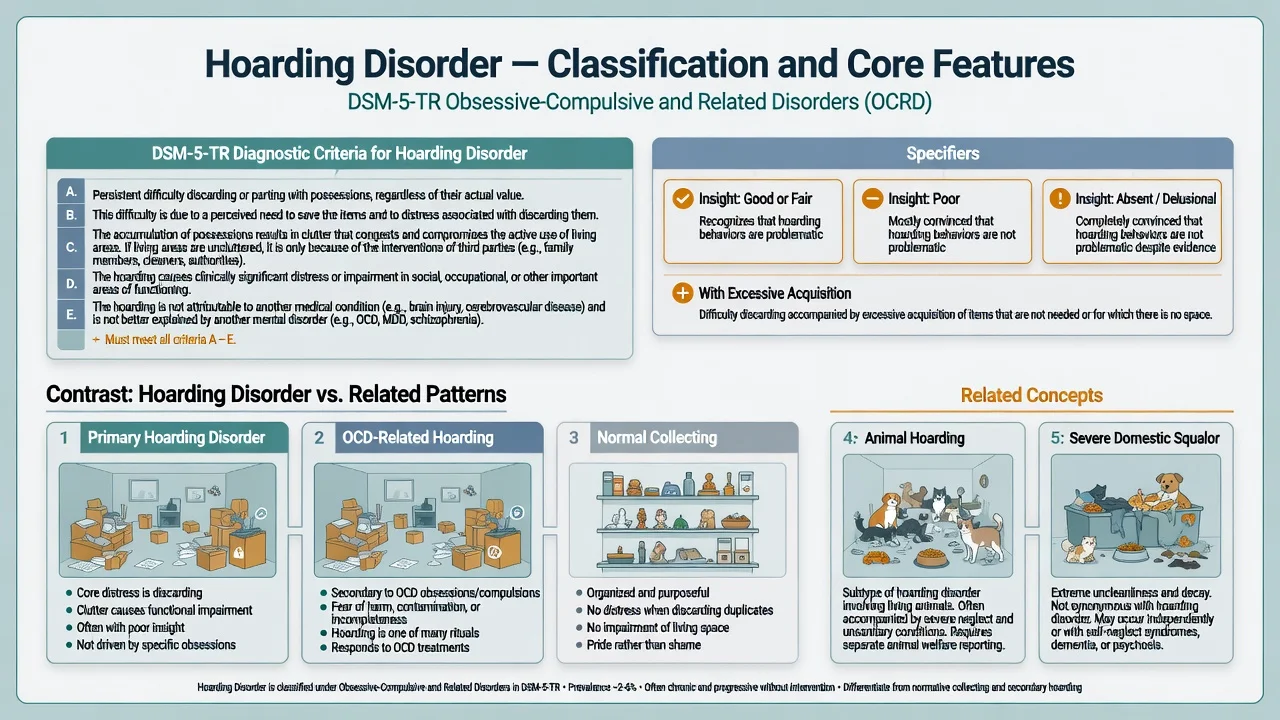
Primary HD
- Distress centered on discarding
- Emotional/identity attachment to items
- Living areas unusable for intended purpose
- Often limited insight; acquisition common
OCD-related saving
- Saving driven by contamination, harm, or symmetry obsessions
- Items kept to prevent catastrophe or ritual incompleteness
- Other OCD themes usually present
- May improve with OCD-targeted ERP/SSRI
Normal collecting
- Organised, prideful display
- Space remains usable
- Pleasure rather than shame dominates
- Discarding duplicates is tolerable
Squalor / Diogenes-type
- Filth, decay, self-neglect prominent
- Not a DSM diagnosis; descriptive cluster
- May occur with or without true HD
- Old-age psychiatry multiagency picture
Animal hoarding is a severe related phenotype: accumulation of animals with failure to provide minimal nutrition, sanitation, and veterinary care, often with denial of suffering. It carries animal-welfare reporting duties and is not managed as “pets plus mild clutter.” Severe domestic squalor is reviewed extensively in old-age psychiatry literature and is not synonymous with HD.[16][17]
Epidemiology and burden
Headline epidemiology (exam numbers)
Systematic review and meta-analysis place point prevalence of HD in the low single-digit percent range in community samples; field studies refine case-finding and service-use implications.[5][6] Twin data support substantial heritability of compulsive hoarding symptoms.[7] Economic and social burden — family conflict, work impairment, housing threats — is well documented.[15]
Comorbidities commonly include major depression, anxiety disorders, ADHD traits/inattention, OCD, trauma history, and personality vulnerability. Formulate each stream; do not collapse everything into “OCD.”[4][9]
Pathophysiology and maintaining model
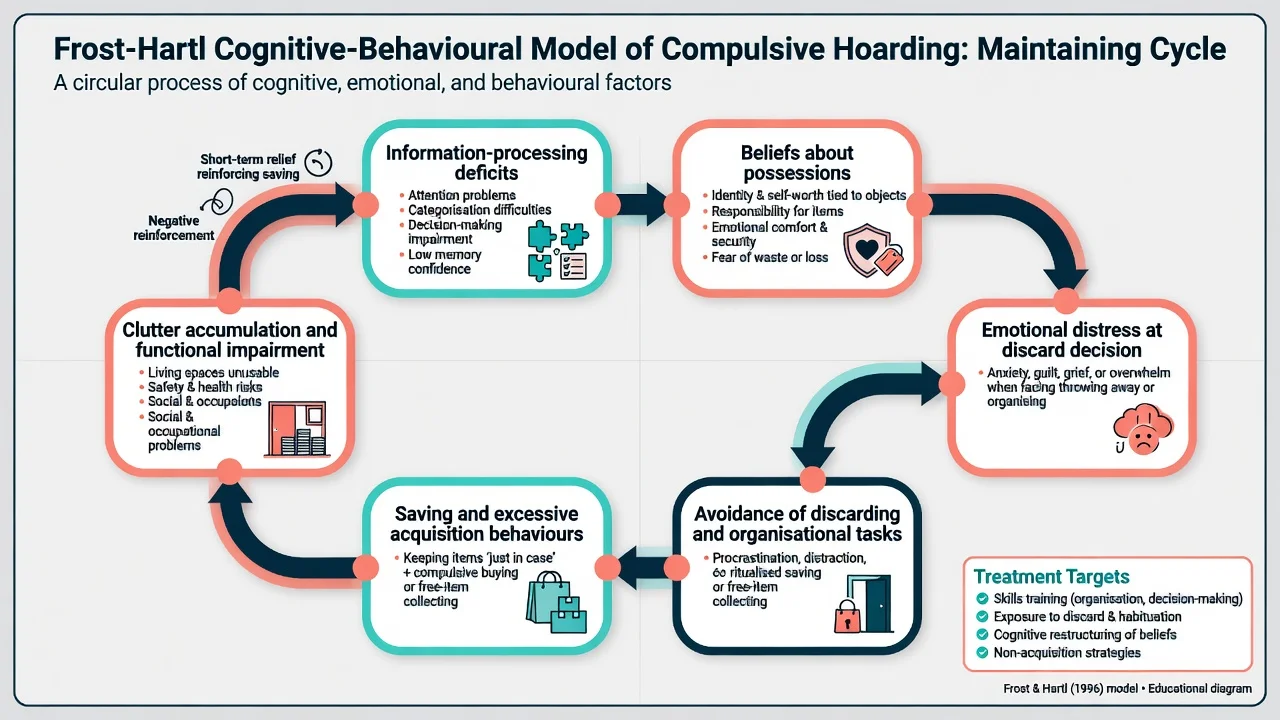
Frost–Hartl model (viva-ready). Compulsive hoarding is maintained by: (1) information-processing problems (attention, categorisation, decision-making, memory confidence); (2) beliefs and emotional attachments to possessions (identity, responsibility, comfort, fear of waste); (3) emotional distress at discard or organisation tasks; (4) avoidance and (5) saving/acquiring behaviours that provide short-term relief while worsening clutter and impairment.[1]
Treatment targets map directly onto the model: skills training, exposure to discarding with habituation, cognitive restructuring of possession beliefs, and non-acquisition practice.[1][10]
Neural studies of decision-making during discarding tasks show different engagement patterns in HD versus controls — useful for viva framing of “why discarding feels impossible,” not for individual diagnosis.[9]
Clinical presentation
Patients present after family conflict, landlord/fire service referral, eviction threat, or medical admission revealing unsafe housing. Living rooms, kitchens, bathrooms, and exits may be impassable. Sleeping surfaces, cooking, and hygiene are compromised. Shame and social isolation are common; insight is often incomplete.[9][15]
MSE language. Overvalued (or occasionally delusional-level) beliefs about the necessity of saving; indecisiveness; anxiety or grief when discard is proposed; variable mood; cognition usually intact in primary adult HD — if not, rethink organic differentials. Risk formulation includes environmental harm and neglect more often than acute interpersonal violence, but depression and suicidality still require assessment.[9]
Atypical traps. Sudden late-life onset, language change, disinhibition, or rapid accumulation — screen for dementia/FTD and other organic causes. Adolescent saving without household compromise may be developmental; still assess trajectory and family accommodation.[4][9]
Differential diagnosis
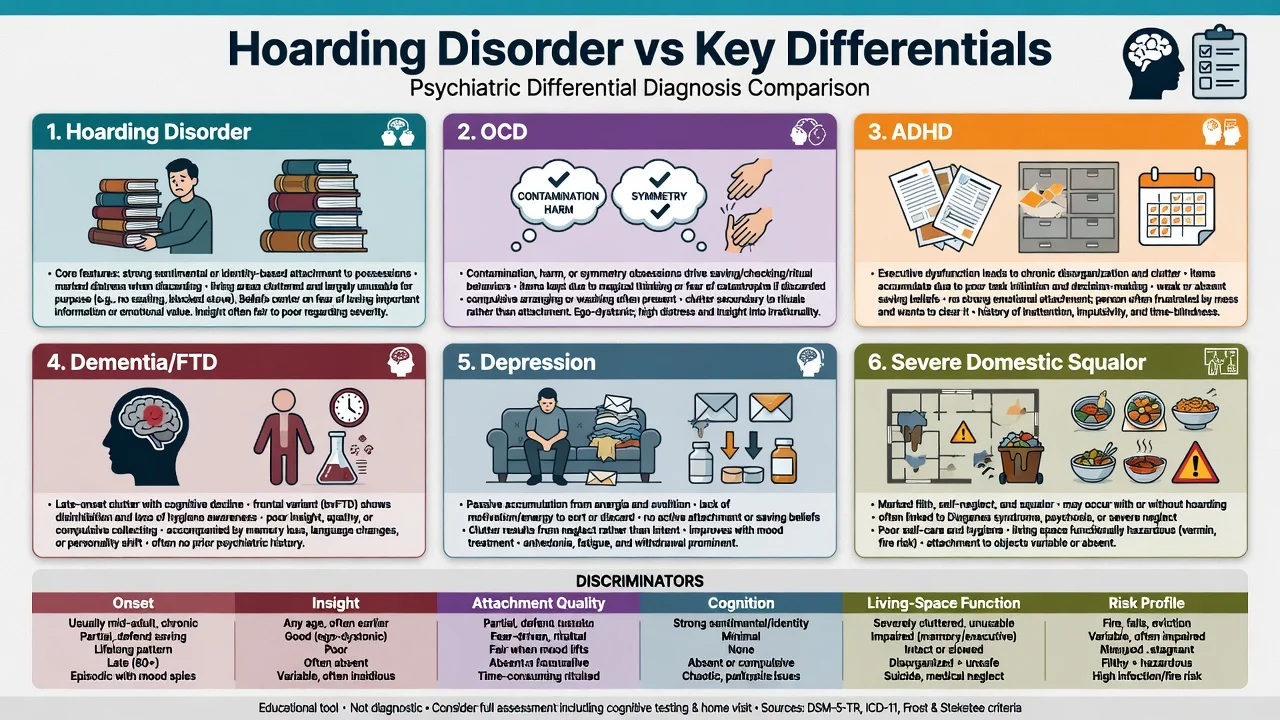
OCD
- Obsessions/compulsions beyond possessions
- Saving to prevent harm/contamination/incompleteness
- Ego-dystonic quality more typical
- Can co-occur with primary HD — dual formulation
ADHD
- Clutter from executive dysfunction
- Weak emotional need to save specific items
- Person often wants order but cannot initiate
- Treat ADHD and skills in parallel when comorbid
Dementia / FTD
- Late new onset with cognitive decline
- Frontal change, hygiene unawareness
- Collecting or utilising behaviour possible
- Neurocognitive work-up first
Depression / squalor
- Passive accumulation from anergia
- Squalor = filth/self-neglect cluster
- May coexist with HD or replace it
- Snowdon old-age series inform multiagency care
Also discriminate psychosis (delusional object significance beyond HD usefulness beliefs), autism-related collecting, and substance-related neglect of the home.[3][4][16]
Assessment
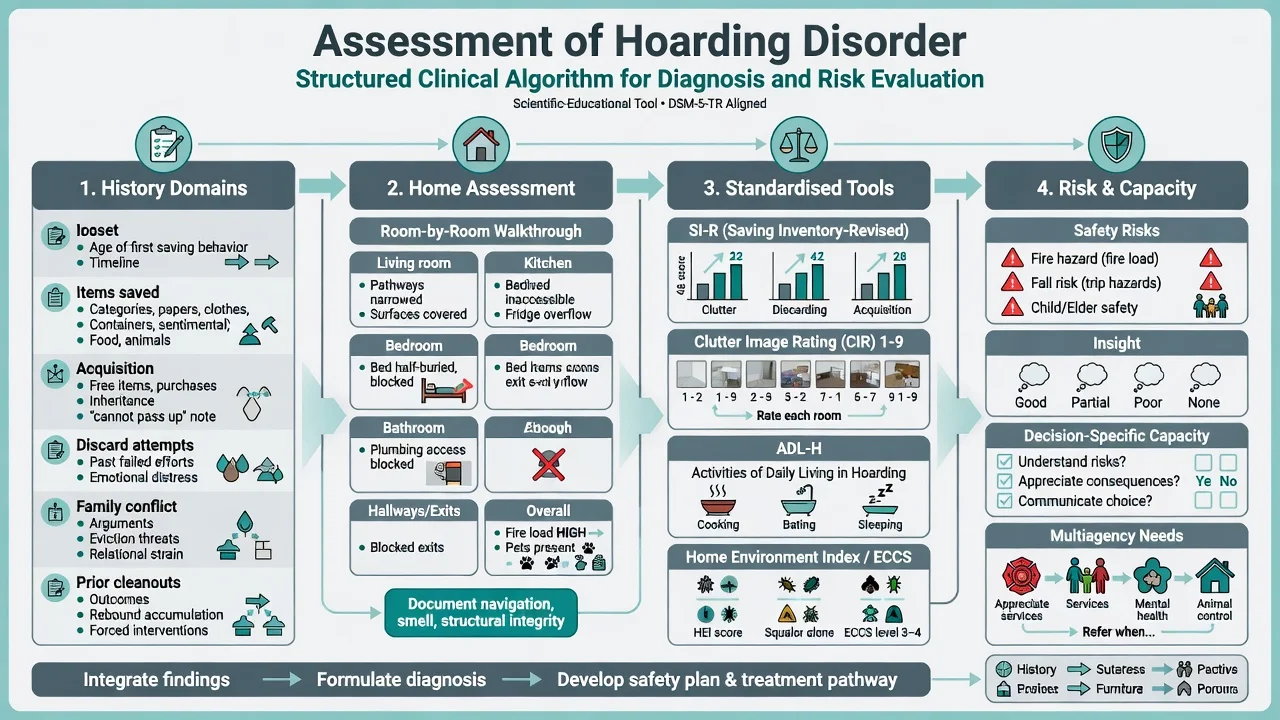
History. Onset of saving; item categories; rooms affected; acquisition pathways; prior discard attempts and forced cleanouts; insight; functional impact; family accommodation or conflict; prior therapy fidelity (was it specialised HD CBT or generic “declutter advice?”).[9]
Home visit. Whenever safe and feasible, assess room-by-room function, pathways, exits, fire load, sanitation, food safety, and animals. Photographs (with consent) and pictorial scales aid documentation and serial review.[9]
Key measures structure severity and response: SI-R (clutter, difficulty discarding, acquisition subscales — severity and treatment response), Clutter Image Rating (pictorial room clutter 1–9 as a rapid visual anchor), ADL-H (functional impact on daily activities), and Home Environment Index / ECCS when squalor and environmental cleanliness are in question.[8][9][19][20]
SI-R is a core self-report instrument for compulsive hoarding severity.[8] Diagnosis and multi-method assessment are reviewed in standard HD assessment syntheses; ADL-H and the Home Environment Index extend functional and squalor measurement.[9][19][20]
Capacity. Capacity is decision-specific (e.g. accepting a fire-safety cleanout of exits vs total property clearance). Assess understanding, appreciation, reasoning, and communication for the decision at hand. Statutes and guardianship pathways are jurisdiction-specific — state principles of least restrictive care without inventing section numbers across countries.[9][16]
Investigations
No lab or scan diagnoses primary HD. Obtain cognitive screening and targeted investigations when late onset, focal neurology, rapid change, or suspected medical drivers of self-neglect are present. Medical review of falls, infection risk, respiratory exposure, and malnutrition is part of severe squalor care.[16][17]
Acute risk and environmental emergency
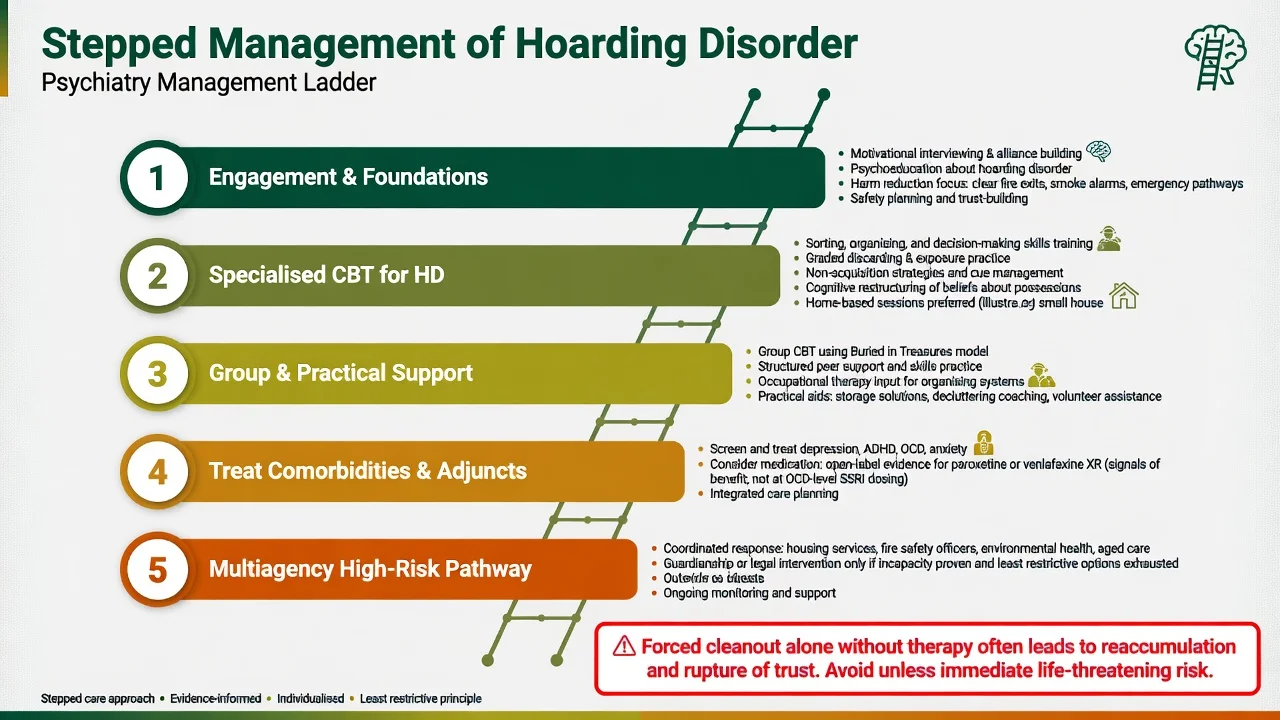
Forced cleanout alone without engagement and a therapy plan commonly produces severe distress, rupture of trust, and rapid reaccumulation — reserve emergency clearance for life-threatening risk and plan follow-up care.[9][16]
Definitive management
First-line — specialised CBT for HD
Specialised CBT is the evidence-based psychological cornerstone. Core components map to the Frost–Hartl model and trial protocols: motivational enhancement and collaborative goal-setting (often partial decluttering and safety first); skills training (sorting, categorising, decision-making); graded exposure to discarding with response prevention of saving rituals; non-acquisition practice and cue management; cognitive work on beliefs about waste, identity, responsibility, and memory distrust; and home-based sessions whenever possible — clinic-only talk therapy is insufficient for severe clutter.[1][10][11]
Evidence. A waitlist-controlled trial of CBT for HD demonstrated clinically meaningful gains versus waitlist.[10] Meta-analysis supports CBT as an effective intervention for HD symptoms, though residual clutter is common and effect sizes are modest relative to some other OCRDs.[11] Group CBT and bibliotherapy formats show pilot promise as access extenders.[18]
Geriatric note. Standard CBT protocols yield more limited gains in older adults with compulsive hoarding; adapted, longer, or more practical OT-augmented approaches are often required.[14]
Generic supportive counselling, one-off professional “blitz cleans,” or pure contamination ERP designed for OCD without discarding/acquisition targets are exam failure modes for primary HD.[10][11]
Pharmacotherapy — adjunctive, not gold-standard monotherapy
Medication evidence is weaker than for OCD. Open-label paroxetine was associated with improvement in compulsive hoarding symptoms in a treatment study; dosing followed SSRI/SRI principles with specialist monitoring rather than a single universal fixed dose for all patients.[12] An open trial of venlafaxine extended-release also reported improvement in HD symptoms.[13]
Fellowship teaching rank-order: specialised CBT with home sessions is first-line for core HD; treat MDD/ADHD/OCD comorbidity with standard agents to aid engagement; open-label paroxetine or venlafaxine XR may be considered as adjuncts after discussion of limited evidence; antipsychotic monotherapy is not first-line for primary HD and is reserved for true psychosis comorbidity.[10][12][13]
Individualise agent, start low, titrate, monitor suicide risk when depressed, sexual/GI effects, hyponatraemia in older adults, and interactions. Do not claim a large multi-site SSRI RCT evidence base equivalent to OCD or BDD fluoxetine data.[12][13]
Multiagency and social interventions
Psychiatry alone rarely remediates severe environmental risk. Coordinate psychology/CBT therapists, occupational therapy, housing, fire prevention, environmental health, aged-care supports, and — when capacity is lacking and least restrictive options fail — guardianship or equivalent statutory pathways under local law.[15][16][17]
Family work: reduce accommodation of acquiring, stop hostile surprise cleanouts when possible, and share a safety-focused plan.[15]
Special populations and scenarios
Older adults. Falls, fire, squalor, and cognitive differentials dominate; Ayers data temper expectations for standard CBT alone.[14][16][17]
Animal hoarding. Parallel psychiatric care, animal welfare authority involvement, and public-health hygiene measures; do not prioritise “keeping the animals together” over welfare standards.[16]
Comorbid OCD + HD. Map which saving is obsession-driven versus attachment-driven; treat both content streams (OCD ERP/SSRI package plus HD discarding/acquisition protocol).[3][4]
Prognosis and disposition
Without specialised intervention, HD is typically chronic and progressive as clutter accumulates. With CBT, many patients improve on SI-R and functional measures, but full clearance is uncommon — set realistic goals (exits clear, bed usable, kitchen functional, reduced acquisition). Poorer insight, severe baseline clutter, cognitive impairment, and lack of home access predict harder courses.[10][11][14]
Step up intensity for high environmental risk, incapacity, or failure of outpatient engagement; step down when safety goals hold and skills generalise.[10][14][16]
Regional practice notes
ANZ (FRANZCP). Frame as OCRD with specialised psychological treatment and multiagency risk (fire, housing, aged care, guardianship under state/territory law). Mental Health Act use is for mental illness criteria and risk as defined locally — severe clutter alone is not automatically “treatable under the Act” without meeting statutory thresholds; capacity and adult safeguarding frameworks often matter more.[2][9][16]
UK (MRCPsych). Guideline pathways are historically stronger for OCD/BDD than standalone HD; still offer evidence-based specialised CBT for HD and multiagency safeguarding. CASC stations often test explanation of HD vs OCD and engagement around home-based work.[2][10][11]
US (ABPN). DSM-5-TR OCRD criteria, SI-R/CIR language, and CBT-first teaching; adult protective services and fire codes interface in severe cases.[2][8][9]
India (MD/DNB, NEET-SS). Same nosology and CBT principles; emphasise family accommodation, limited specialist CBT access, and practical harm reduction plus treatable comorbidity.[5][10][15]
Exam pearls
Related disorders in one line
BDD is appearance OCRD; OCD is multi-theme obsessions/compulsions; HD is discarding/attachment/clutter OCRD — shared chapter, different protocols.[2][4]
References
- [1]Frost RO, Hartl TL A cognitive-behavioral model of compulsive hoarding Behav Res Ther, 1996.PMID 8871366
- [2]Mataix-Cols D, Frost RO, Pertusa A, et al. Hoarding disorder: a new diagnosis for DSM-V? Depress Anxiety, 2010.PMID 20336805
- [3]Pertusa A, Fullana MA, Singh S, et al. Compulsive hoarding: OCD symptom, distinct clinical syndrome, or both? Am J Psychiatry, 2008.PMID 18483134
- [4]Pertusa A, Frost RO, Fullana MA, et al. Refining the diagnostic boundaries of compulsive hoarding: a critical review Clin Psychol Rev, 2010.PMID 20189280
- [5]Postlethwaite A, Kellett S, Mataix-Cols D Prevalence of Hoarding Disorder: A systematic review and meta-analysis J Affect Disord, 2019.PMID 31200169
- [6]Nordsletten AE, Reichenberg A, Hatch SL, et al. Epidemiology of hoarding disorder Br J Psychiatry, 2013.PMID 24158881
- [7]Iervolino AC, Perroud N, Fullana MA, et al. Prevalence and heritability of compulsive hoarding: a twin study Am J Psychiatry, 2009.PMID 19687130
- [8]Frost RO, Steketee G, Grisham J Measurement of compulsive hoarding: saving inventory-revised Behav Res Ther, 2004.PMID 15350856
- [9]Frost RO, Steketee G, Tolin DF Diagnosis and assessment of hoarding disorder Annu Rev Clin Psychol, 2012.PMID 22035242
- [10]Steketee G, Frost RO, Tolin DF, et al. Waitlist-controlled trial of cognitive behavior therapy for hoarding disorder Depress Anxiety, 2010.PMID 20336804
- [11]Tolin DF, Frost RO, Steketee G, et al. Cognitive behavioral therapy for hoarding disorder: a meta-analysis Depress Anxiety, 2015.PMID 25639467
- [12]Saxena S, Brody AL, Maidment KM, et al. Paroxetine treatment of compulsive hoarding J Psychiatr Res, 2007.PMID 16790250
- [13]Saxena S, Sumner J Venlafaxine extended-release treatment of hoarding disorder Int Clin Psychopharmacol, 2014.PMID 24722633
- [14]Ayers CR, Wetherell JL, Golshan S, et al. Cognitive-behavioral therapy for geriatric compulsive hoarding Behav Res Ther, 2011.PMID 21784412
- [15]Tolin DF, Frost RO, Steketee G, et al. The economic and social burden of compulsive hoarding Psychiatry Res, 2008.PMID 18597855
- [16]Snowdon J, Shah A, Halliday G Severe domestic squalor: a review Int Psychogeriatr, 2007.PMID 16973099
- [17]Snowdon J, Halliday G A study of severe domestic squalor: 173 cases referred to an old age psychiatry service Int Psychogeriatr, 2011.PMID 20678298
- [18]Muroff J, Steketee G, Bratiotis C, et al. Group cognitive and behavioral therapy and bibliotherapy for hoarding: a pilot trial Depress Anxiety, 2012.PMID 22447579
- [19]Frost RO, Hristova V, Steketee G, et al. Activities of Daily Living Scale in Hoarding Disorder J Obsessive Compuls Relat Disord, 2013.PMID 23482436
- [20]Rasmussen JL, Steketee G, Frost RO, et al. Assessing squalor in hoarding: the Home Environment Index Community Ment Health J, 2014.PMID 24292497