Psych · General adult psychiatry — somatic symptom and related
Illness anxiety disorder
Also known as Health anxiety · Hypochondriasis · Hypochondriacal disorder · Illness anxiety · Cyberchondria · Disease phobia · IAD
Exam-exhaustive fellowship reference on illness anxiety disorder — DSM-5-TR criteria and care-seeking/care-avoidant subtypes; DSM-IV hypochondriasis reorganisation vs somatic symptom disorder; ICD-11 hypochondriasis framing; Warwick–Salkovskis CBT model; epidemiology and mortality risk; differentials; CL interface; CBT evidence (Barsky, Greeven, CHAMP, meta-analyses, internet CBT); SSRI evidence (paroxetine, fluoxetine). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Illness anxiety disorder (IAD) is a high-yield general adult and consultation-liaison topic at the FRANZCP, MRCPsych, and ABPN interface. Examiners test the DSM-5-TR reorganisation of hypochondriasis, the SSD vs IAD discriminator (symptom load), the cognitive-behavioural maintaining cycle, CBT and SSRI trial names, and the CL interface with high-utilising medical patients who are neither “faking” nor always medically free of disease.[3][9][14]
Overview and definition
IAD is defined by preoccupation with having or acquiring a serious illness. Somatic symptoms are not present or, if present, are only mild in intensity. There is a high level of anxiety about health, and the individual performs excessive health-related behaviours (e.g. repeatedly checking the body for signs of illness) or exhibits maladaptive avoidance (e.g. avoiding doctor appointments and hospitals). Illness preoccupation has been present for at least 6 months, though the specific illness that is feared may change over that period. The illness-related preoccupation is not better explained by another mental disorder (e.g. SSD, panic, GAD, OCD, delusional disorder, BDD).[14][15][16]
Clinical essence for viva. The core process is health anxiety with catastrophic misinterpretation of benign cues, safety behaviours that prevent disconfirmation, and often a doctor-shopping or care-avoiding medical pathway — not “imagining symptoms for secondary gain.” Patients may have real medical disease and still meet criteria for pathological health anxiety about severity, progression, or additional illness.[9][10][12]
Classification: DSM-5-TR, legacy hypochondriasis, ICD-11
DSM-5 / DSM-5-TR placement. IAD sits in the somatic symptom and related disorders chapter with SSD, conversion (functional neurological symptom) disorder, psychological factors affecting other medical conditions, factitious disorder, and other specified / unspecified somatic symptom and related disorders.[14][15]
Care-seeking vs care-avoidant. Specifiers capture opposite behavioural poles that both maintain anxiety: relentless investigation and reassurance versus avoidance of care that can delay detection of real disease. Both are examinable.[14]
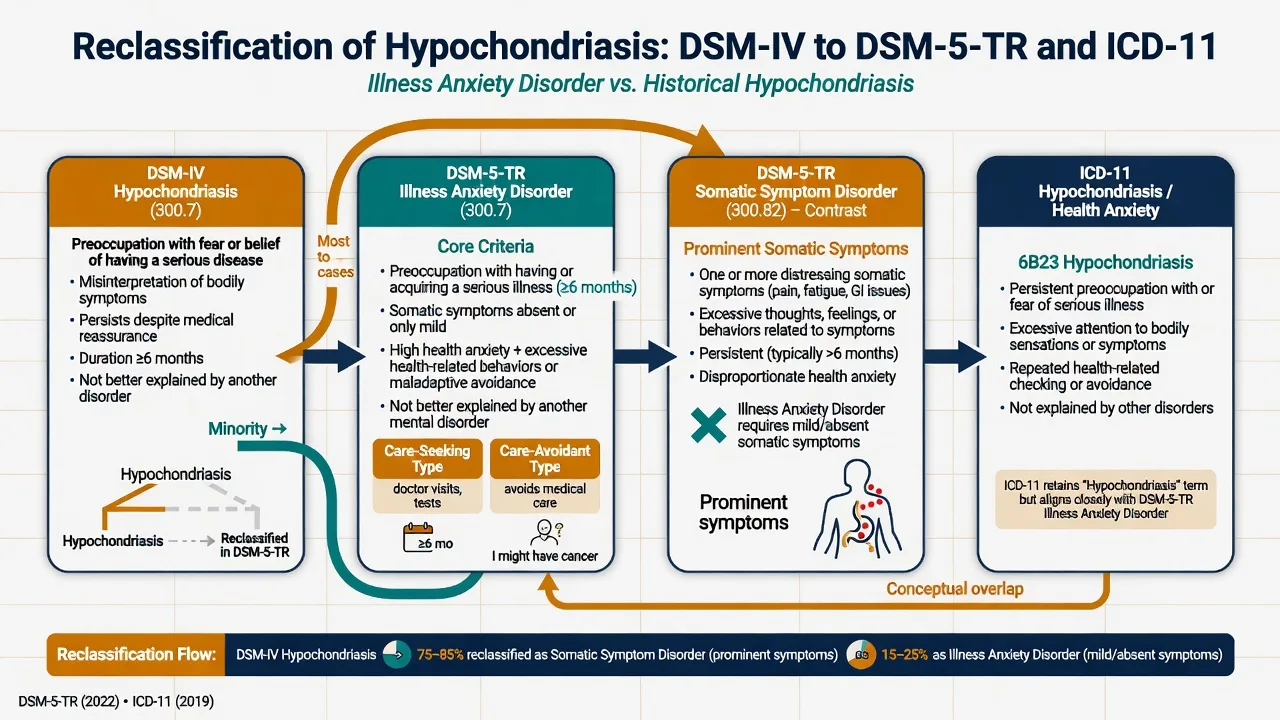
Historical hypochondriasis (DSM-IV and earlier). DSM-IV hypochondriasis required preoccupation with fears of having a serious disease based on misinterpretation of bodily symptoms, persisting despite medical evaluation and reassurance, for at least 6 months. In the DSM-5 reorganisation, individuals with prominent somatic symptoms plus disproportionate responses largely meet somatic symptom disorder, whereas individuals with high health anxiety and minimal somatic symptoms meet illness anxiety disorder.[14][15][16]
Exam pearl: do not claim that “hypochondriasis simply became IAD.” The bulk of the old construct maps to SSD; IAD is the cleaner “health anxiety with little somatic load” phenotype.[14][15][16]
ICD-11. ICD-11 retains hypochondriasis (excessive health anxiety / preoccupation with having a serious disease) among obsessive-compulsive or related disorders in some teaching maps, while bodily distress disorder captures multi-system distressing bodily symptoms with excessive attention — closer to European “bodily distress” traditions. Always state which manual you are using when classification is scored.[14][16]
Illness anxiety disorder
- Minimal or absent somatic symptoms
- Core = fear of serious disease
- Care-seeking or care-avoidant behaviours
- ≥6 months preoccupation typical
Somatic symptom disorder
- One or more distressing somatic symptoms
- Disproportionate thoughts, feelings, behaviours about symptoms
- Not defined by 'medically unexplained'
- May include health anxiety with high symptom load
Legacy hypochondriasis
- DSM-IV disease fear + misinterpretation
- Required persistence despite evaluation
- Most reclassified as SSD in DSM-5
- Minority pure IAD pathway
ICD-11 neighbours
- Hypochondriasis / health anxiety framing
- Bodily distress disorder for multi-symptom clusters
- Declare manual in viva answers
- Regional coding may lag DSM wording
Epidemiology and risk
Headline epidemiology (exam numbers)
Australian population data place lifetime health anxiety around 5.7% and current around 3.4%, with substantial comorbidity, disability, and service use — figures higher than older narrow hypochondriasis prevalence estimates that required strict criteria.[11] In general hospital medical clinics, significant health anxiety is common (order of one in five attenders across specialties in Tyrer and colleagues’ survey), with neurology among the highest — a direct rationale for CL and medical-clinic CBT programmes such as CHAMP.[12]
Mortality is not a joke diagnosis. A large Swedish cohort of individuals with clinical hypochondriasis diagnoses showed increased all-cause mortality, including from suicide and other unnatural causes, as well as natural causes — reframing IAD away from “worried well” caricature toward a condition requiring serious risk assessment and treatment access.[13]
Comorbid depression, GAD, panic, and OCD-spectrum conditions are common; formulate each and treat the health-anxiety cycle specifically rather than assuming generic anxiety care will suffice.[11][18]
Pathophysiology and maintaining model
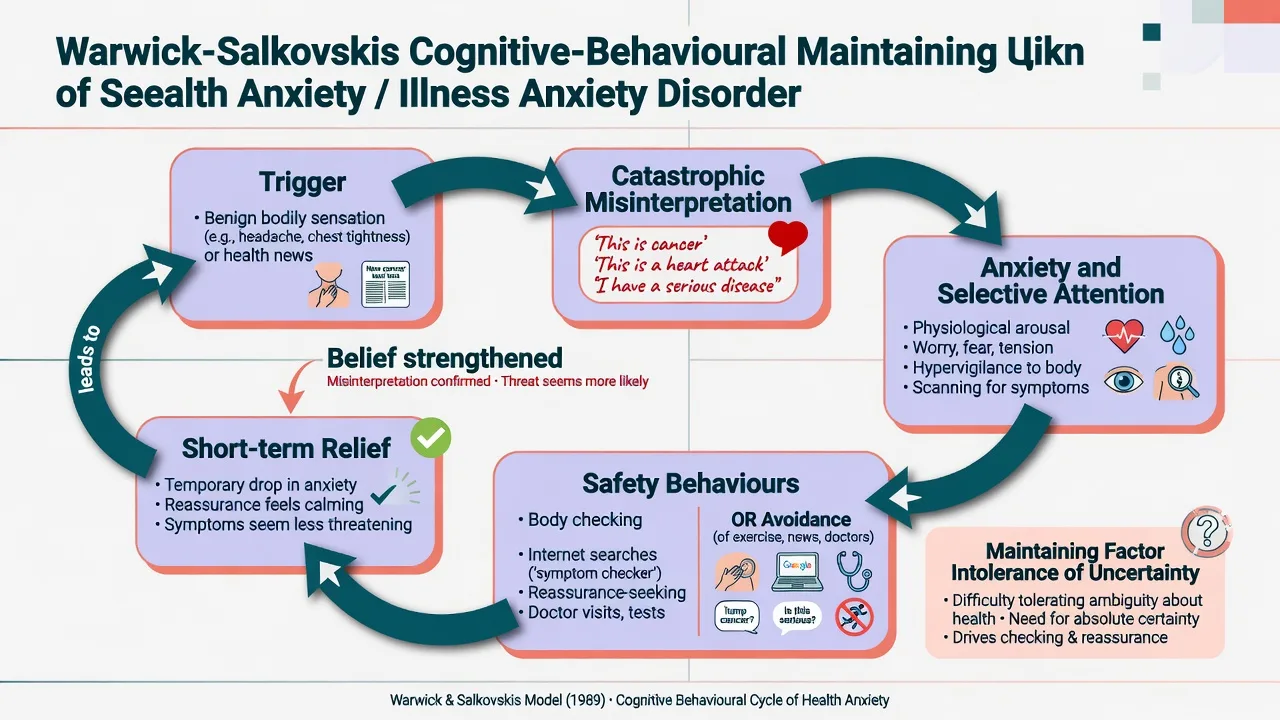
Cognitive-behavioural model (viva-ready). Benign bodily sensations, medical information, family illness histories, or media cues are catastrophically misinterpreted as evidence of serious disease. Anxiety rises; selective attention amplifies interoception; safety behaviours (body checking, pulse monitoring, internet “research,” seeking multiple medical opinions, or avoiding hospitals and tests) reduce anxiety briefly but prevent disconfirmation and strengthen the illness belief. Reassurance from doctors or relatives functions as a compulsion-like behaviour that wears off, driving further seeking.[9][10]
Intolerance of uncertainty is a high-yield psychological mechanism: incomplete medical certainty after normal tests is intolerable, so patients escalate investigations. Cyberchondria (escalating health-related internet searching that increases anxiety) is a modern amplifier, not a separate disease entity.[9][18]
Pharmacology signal. SSRI responsiveness in hypochondriasis/health-anxiety trials supports an anxiety-spectrum serotonergic treatment model without implying a diagnostic biomarker.[2][4][5]
Clinical presentation
Typical feared diseases: cancer, cardiac sudden death, neurological degeneration (MS, motor neuron disease), HIV/serious infection. Hours may be spent checking moles, pulses, stools, or online symptom checkers. Care-seeking patients cycle through GPs, ED, and specialists with “negative” work-ups and transient relief. Care-avoidant patients refuse colonoscopy, mammography, or follow-up bloods despite risk factors — real disease can be missed.[12][14]
MSE. Anxious affect; health-focused overvalued ideas ranging to near-delusional conviction; preserved reality testing outside the health domain; no primary formal thought disorder or multimodal hallucinations when the formulation is pure IAD. Insight fluctuates — many accept a psychological contribution only after alliance and a both–and explanation.[9][14]
Differential diagnosis
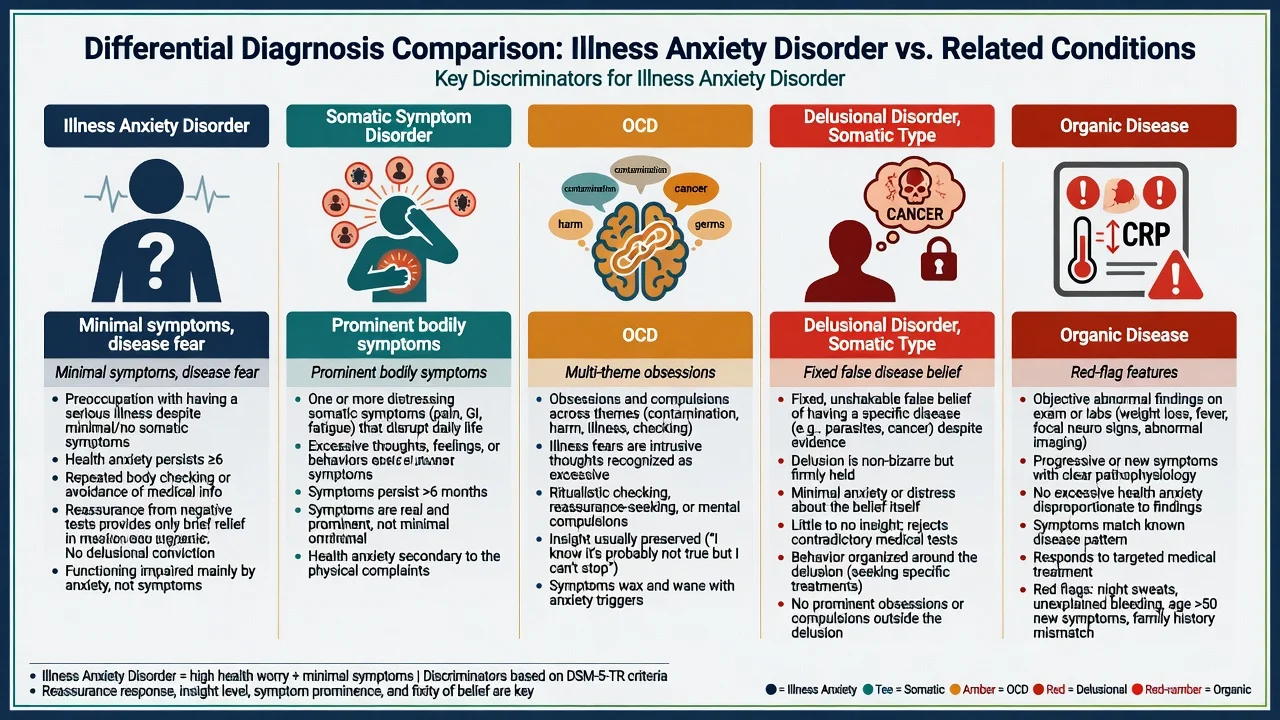
Key discriminators: SSD has prominent distressing somatic symptoms; OCD has multi-theme obsessions/compulsions beyond illness; GAD has multi-domain real-life worry; panic has discrete unexpected clusters rather than enduring disease conviction alone; delusional disorder somatic type has fixed false disease belief with psychotic process features; organic disease shows progressive red flags and objective signs needing action; factitious/malingering involve intentional production for sick role or external gain rather than anxiety-driven checking without deception.[14][15][16]
Never diagnose IAD only because tests are negative. Use positive psychiatric features (checking, reassurance, catastrophic appraisals, functional pattern) and maintain a low threshold to re-evaluate when the clinical picture changes.[14][15][16]
If somatic symptom burden is high, score PHQ-15 conceptually and consider SSD as the primary frame while still treating health-anxiety behaviours.[19]
Clinical and bedside assessment
History structure. Feared disease hierarchy; duration (6-month threshold teaching); hours per day on checking/internet; care-seeking vs avoidance; list of prior investigations and who ordered them; response to reassurance; family illness models and accommodation; depression and panic symptoms; substance use; trauma related to medical events; functional impact.[9][11]
Risk. Structured suicide assessment is mandatory — elevated mortality and suicide in hypochondriasis cohorts refute the “benign worry” narrative. Also assess medical risk from care-avoidance (delayed cancer detection, untreated cardiac symptoms).[13]
Measurement. Health-anxiety inventories / Whiteley Index concept for tracking; PHQ-9 and GAD-7 for comorbidity; PHQ-15 if multi-symptom load suggests SSD pathway.[11][19]
Collateral. GP utilisation data and family reports of night-time checking or request for endless reassurance are high-yield.[12]
Investigations and proportionate medicine
No lab diagnoses idiopathic IAD. Obtain proportionate medical evaluation for red flags and age-appropriate screening; then stop uncoordinated re-testing without new clinical change. Agree a single medical home (named GP or specialty clinic) and a written plan for when new symptoms warrant re-assessment. Baseline metabolic profile, ECG, and pregnancy testing as indicated before SSRI.[3][12][14]
Management — acute risk and resuscitation
Manage SSRI-related activation, hyponatraemia (especially older adults), and serotonin syndrome risk with polypharmacy on standard medical pathways.[4][5]
Management — definitive and stepwise
Engagement and CL interface (do this first)
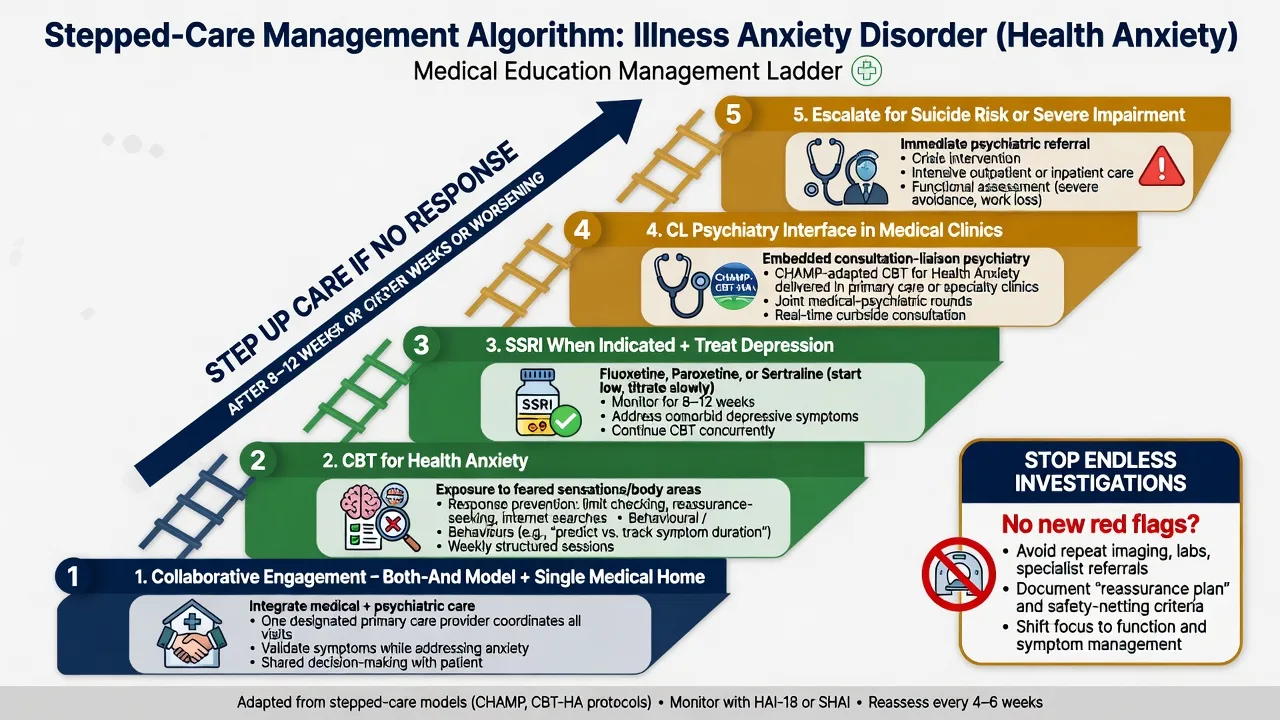
Use a both–and formulation: bodily sensations are real; the threat and attention systems amplify danger appraisals and disability. Avoid “nothing is wrong with you” (invalidating) and avoid endless collusive testing (reinforcing). Schedule regular, time-limited medical reviews rather than only crisis-driven visits; reduce on-demand reassurance; involve family to stop accommodation of checking rituals.[3][9][10]
CHAMP (Cognitive behaviour therapy for Health Anxiety in Medical Patients) is the flagship CL-relevant trial: adapted CBT-HA delivered to high health-anxiety medical outpatients improved outcomes and was cost-effective, with sustained benefit in longer follow-up analyses — cite for FRANZCP/MRCPsych medical-setting stems.[3][17]
First-line psychological treatment — CBT for health anxiety
Specialised CBT includes: psychoeducation on the maintaining cycle; cognitive work on catastrophic misinterpretations; exposure to bodily sensations and health-related cues; response prevention for checking, reassurance-seeking, and internet searching; behavioural experiments testing feared outcomes; attention training away from body scanning.[1][9][18]
Landmark evidence candidates must name: Barsky and Ahern (2004) CBT versus usual care reduces hypochondriacal symptoms and health anxiety at follow-up;[1] Greeven et al. (2007) CBT versus paroxetine versus control — both active arms outperform control;[2] Greeven et al. (2009) naturalistic follow-up supports durability of CBT and paroxetine benefits;[20] Tyrer CHAMP (2014) multicentre CBT-HA in medical clinics is clinically effective and cost-effective;[3] Tyrer et al. (2017) HTA reports lasting benefit to 5 years;[17] Olatunji (2014) and Cooper (2017) meta-analyses support CBT efficacy for hypochondriasis/health anxiety;[6][18] Hedman (2011) internet CBT and Axelsson (2020) internet versus face-to-face noninferiority support ICBT access pathways.[7][8]
Generic supportive counselling without exposure and response-prevention elements is an exam failure mode.[1][6][18]
Pharmacotherapy — SSRI evidence
SSRIs are appropriate for IAD/health anxiety especially with comorbid depression or anxiety, inadequate CBT access/response, or patient preference after informed discussion.[2][4][5]
Exam dose anchors (adult oral starts; titrate and monitor). Paroxetine often 10–20 mg daily with titration (Greeven RCT versus CBT; sexual/withdrawal effects and interactions matter; not first-choice in pregnancy discussions).[2] Fluoxetine often 20 mg daily, titrate as tolerated (Fallon placebo-controlled 2008 and multi-arm 2017; long half-life).[4][5] Sertraline often 25–50 mg daily start as a pragmatic comorbidity-friendly SSRI with activation monitoring.[4]
In the Fallon 2017 randomised trial, fluoxetine (with medical management) was efficacious for hypochondriasis; joint CBT plus fluoxetine offered incremental benefit over monotherapy pathways in the study’s responder framework — know the design (placebo, CBT, fluoxetine, joint) without overstating universal superiority of combination for every patient.[2][4][5][20]
Adequate trial teaching. Use depression/anxiety-range titration, monitor early activation and suicidality (especially under 25 years where local warnings apply), allow several weeks at a therapeutic dose before declaring non-response, and combine with CBT when feasible.[4][5]
What not to do
- Endless specialist referrals without a coordinating plan.[3][12]
- Pure benzodiazepine long-term for health anxiety (dependence, no disease-conviction extinction).[18]
- Antipsychotic monotherapy for non-psychotic IAD.[14]
- Dismissive discharge that ruptures alliance and multiplies ED visits.[9]
Subtypes and high-yield scenarios
Post-negative cancer or cardiac work-up. Classic stem: normal investigations, rising checking and internet use — start CBT-HA and coordinated primary care, not another CT “for peace of mind” without indication.[1][3]
IAD with real chronic disease. Health anxiety about progression can coexist with diabetes, IBD, or treated cancer — treat the anxiety process without denying the medical diagnosis.[12][14]
Care-avoidant subtype. Safety-net for red flags; graded exposure to medical settings is part of CBT.[14]
Cyberchondria-dominant. Explicit response prevention for online searching; schedule limited, structured information sources.[9][18]
Complications and pitfalls
Missing organic disease by over-psychiatricising new red flags; iatrogenic maintenance via uncoordinated testing; missing suicide/depression; mislabeling severe conviction as schizophrenia and withholding CBT/SSRI; treating only panic attacks while leaving illness beliefs and checking intact.[13][14][16]
Prognosis and disposition
Untreated course is often chronic and fluctuating. Specialised CBT produces moderate-to-large benefits in meta-analyses, with durability signals from CHAMP and Greeven follow-up. Disposition is usually outpatient CBT ± SSRI; embed CL pathways in high-utilising medical clinics; step up for suicide risk or severe functional collapse. Continue effective SSRI and offer CBT boosters when residual checking or comorbidity persists.[3][6][17][18][20]
Special populations
Older adults. Lower threshold to re-evaluate organic disease at late first onset; SSRI hyponatraemia and polypharmacy risk.[4][13]
Perinatal. Collaborative obstetric–psychiatry risk–benefit discussion of untreated health anxiety versus SSRI (sertraline often discussed as pragmatic); avoid paroxetine first-line in pregnancy discussions where local guidance discourages it.[2][4]
Adolescents. Family accommodation, school avoidance, social media health content — family-inclusive CBT framing.[18]
Cultural formulation. Validate explanatory models (spirit, heat, karma) while still offering CBT-compatible behavioural change when impairment meets criteria.[11]
Regional practice deltas
ANZ (FRANZCP): Frame collaborative primary care and C-L pathways; use TGA-local formulary for SSRIs; cite Sunderland Australian epidemiology in local stems; CHAMP is UK-origin but highly examinable for medical-clinic CBT. UK (MRCPsych): NICE stepped-care anxiety pathways and CHAMP cost-effectiveness are high-yield CASC/MEQ anchors. US (ABPN): DSM-5-TR SSD/IAD wording and Fallon/Barsky trial names dominate. MD/DNB/NEET-SS: Expect definitions, hypochondriasis history, CBT cycle, named SSRI trials, and differential from delusional disorder.[1][3][4][11]
Evidence and guidelines — named anchors
Deploy: Dimsdale (DSM-5 SSD/IAD nosology), Mayou (critical appraisal of the chapter), Warwick and Salkovskis (CBT model), Barsky, Greeven, Tyrer CHAMP, Fallon, Olatunji / Cooper meta-analyses, Hedman / Axelsson internet CBT, Sunderland, Tyrer clinic prevalence, Mataix-Cols mortality.[1][2][3][4][6][9][11][13][14]
There is no single RANZCP “IAD-only” clinical practice guideline equivalent to some mood-disorder CPGs; exam answers rest on trial evidence + stepped collaborative care principles and local anxiety/depression guidance for SSRI and psychological therapy access.[3][18]
Exam pearls
Classic stems: post-negative oncology work-up with escalating checking; neurology clinic high utilizer; care-avoidant patient missing screening; near-delusional cancer conviction without psychosis; combination CBT + SSRI discussion after partial response.[3][4][12]
Landmark names to deploy under pressure: Warwick–Salkovskis, Barsky, Greeven, Tyrer CHAMP, Fallon, Olatunji, Hedman/Axelsson, Sunderland, Mataix-Cols, Dimsdale.[1][3][4][9][11][13][14]
References
- [1]Barsky AJ, Ahern DK Cognitive behavior therapy for hypochondriasis: a randomized controlled trial JAMA, 2004.PMID 15039413
- [2]Greeven A, van Balkom AJ, Visser S, et al. Cognitive behavior therapy and paroxetine in the treatment of hypochondriasis: a randomized controlled trial Am J Psychiatry, 2007.PMID 17202549
- [3]Tyrer P, Cooper S, Salkovskis P, et al. Clinical and cost-effectiveness of cognitive behaviour therapy for health anxiety in medical patients: a multicentre randomised controlled trial Lancet, 2014.PMID 24139977
- [4]Fallon BA, Ahern DK, Pavlicova M, et al. A Randomized Controlled Trial of Medication and Cognitive-Behavioral Therapy for Hypochondriasis Am J Psychiatry, 2017.PMID 28659038
- [5]Fallon BA, Petkova E, Skritskaya N, et al. A double-masked, placebo-controlled study of fluoxetine for hypochondriasis J Clin Psychopharmacol, 2008.PMID 19011432
- [6]Olatunji BO, Kauffman BY, Meltzer S, et al. Cognitive-behavioral therapy for hypochondriasis/health anxiety: a meta-analysis of treatment outcome and moderators Behav Res Ther, 2014.PMID 24954212
- [7]Hedman E, Andersson G, Andersson E, et al. Internet-based cognitive-behavioural therapy for severe health anxiety: randomised controlled trial Br J Psychiatry, 2011.PMID 21357882
- [8]Axelsson E, Andersson E, Ljótsson B, et al. Effect of Internet vs Face-to-Face Cognitive Behavior Therapy for Health Anxiety: A Randomized Noninferiority Clinical Trial JAMA Psychiatry, 2020.PMID 32401286
- [9]Warwick HM, Salkovskis PM Hypochondriasis Behav Res Ther, 1990.PMID 2183757
- [10]Salkovskis PM, Warwick HM Morbid preoccupations, health anxiety and reassurance: a cognitive-behavioural approach to hypochondriasis Behav Res Ther, 1986.PMID 3753387
- [11]Sunderland M, Newby JM, Andrews G Health anxiety in Australia: prevalence, comorbidity, disability and service use Br J Psychiatry, 2013.PMID 22500013
- [12]Tyrer P, Cooper S, Crawford M, et al. Prevalence of health anxiety problems in medical clinics J Psychosom Res, 2011.PMID 22118381
- [13]Mataix-Cols D, Isomura K, Sidorchuk A, et al. All-Cause and Cause-Specific Mortality Among Individuals With Hypochondriasis JAMA Psychiatry, 2024.PMID 38091000
- [14]Dimsdale JE, Creed F, Escobar J, et al. Somatic symptom disorder: an important change in DSM J Psychosom Res, 2013.PMID 23972410
- [15]Dimsdale JE, Levenson J What's next for somatic symptom disorder? Am J Psychiatry, 2013.PMID 24306336
- [16]Mayou R Is the DSM-5 chapter on somatic symptom disorder any better than DSM-IV somatoform disorder? Br J Psychiatry, 2014.PMID 25029686
- [17]Tyrer P, Salkovskis P, Tyrer H, et al. Cognitive-behaviour therapy for health anxiety in medical patients (CHAMP): a randomised controlled trial with outcomes to 5 years Health Technol Assess, 2017.PMID 28877841
- [18]Cooper K, Gregory JD, Walker I, et al. Cognitive Behaviour Therapy for Health Anxiety: A Systematic Review and Meta-Analysis Behav Cogn Psychother, 2017.PMID 28229805
- [19]Kroenke K, Spitzer RL, Williams JB The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms Psychosom Med, 2002.PMID 11914441
- [20]Greeven A, van Balkom AJ, van der Leeden R, et al. Cognitive behavioral therapy versus paroxetine in the treatment of hypochondriasis: an 18-month naturalistic follow-up J Behav Ther Exp Psychiatry, 2009.PMID 19616195