Psych · General adult psychiatry — impulse-control disorders
Impulse-control disorders overview
Also known as Impulse control disorders · Disruptive impulse-control and conduct disorders · Intermittent explosive disorder overview · Kleptomania overview · Pyromania overview · Behavioural impulsivity disorders · DICCD · CSBD impulse control
Exam-exhaustive fellowship atlas on impulse-control disorders as a group — DSM-5-TR Disruptive/Impulse-Control/Conduct chapter versus ICD-11 Impulse control disorders, major reclassifications (gambling, OCRD, CSBD), shared urge phenomenology, IED epidemiology, kleptomania and pyromania, dopamine-agonist ICDs, assessment (MIDI/QUIP concepts), CBT-first care, fluoxetine and naltrexone evidence, forensic and risk interfaces. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
This atlas leaf is the group overview for impulse-control problems in general adult psychiatry. Leaf topics on gambling, ODD/CD, ASPD, OCRD body-focused behaviours, and sexual/paraphilic disorders deepen individual syndromes; examiners still expect a clean map of what sits where, what was reclassified, and how assessment and treatment differ by disorder.[1][2][12]
Overview and definition
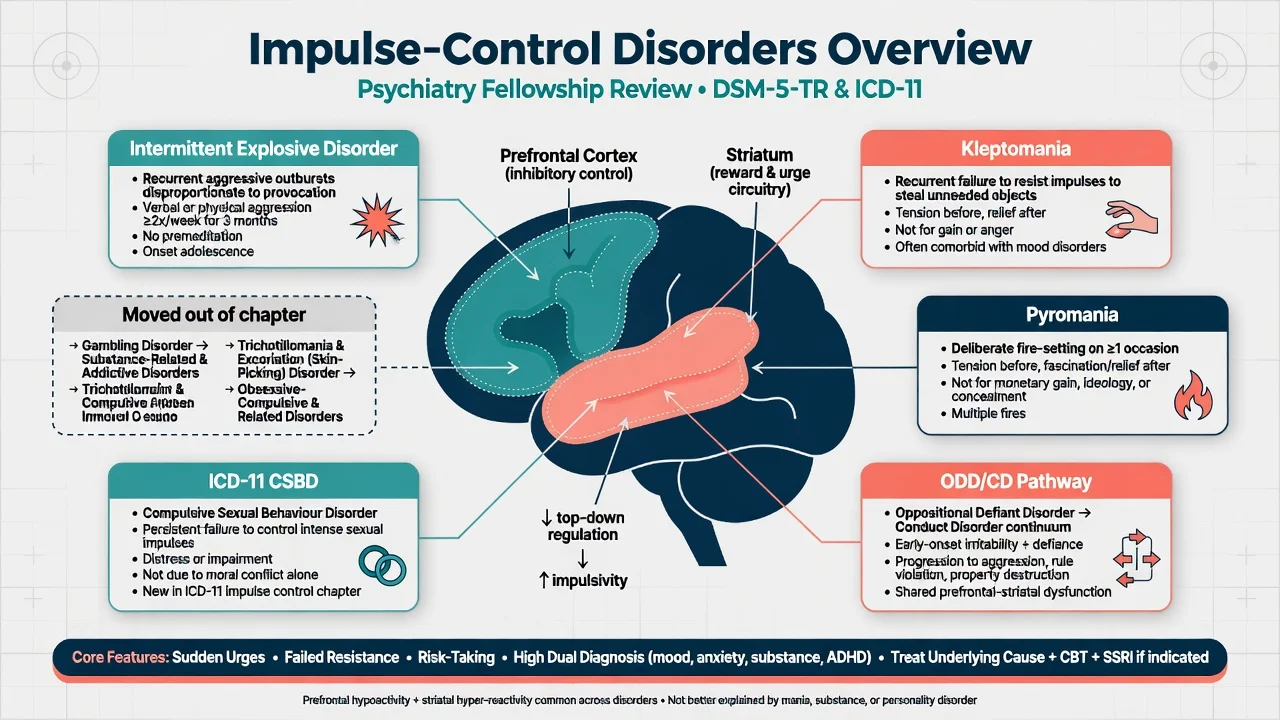
Historically, impulse-control disorders (ICDs) described recurrent failure to resist an impulse, drive, or temptation to perform an act harmful to self or others, often with rising tension before the act, gratification or relief during it, and variable guilt afterward.[1][2] That template still helps viva language for kleptomania, pyromania, and many urge-driven presentations, but it is not a single mechanism diagnosis and does not fit every DSM-5-TR Disruptive, Impulse-Control, and Conduct Disorder (DICCD) equally well (for example developmental ODD/CD pathways).[1][5]
Impulsivity versus compulsivity. Impulsivity emphasises rapid, poorly planned action with inadequate regard to consequences. Compulsivity emphasises repetitive acts aimed at reducing distress or preventing a feared outcome. Many clinical behaviours sit on a continuum or share cortico-striatal circuit themes; do not force every patient into one pole.[1][2]
Classification — the exam map
DSM-5-TR: Disruptive, Impulse-Control, and Conduct Disorders
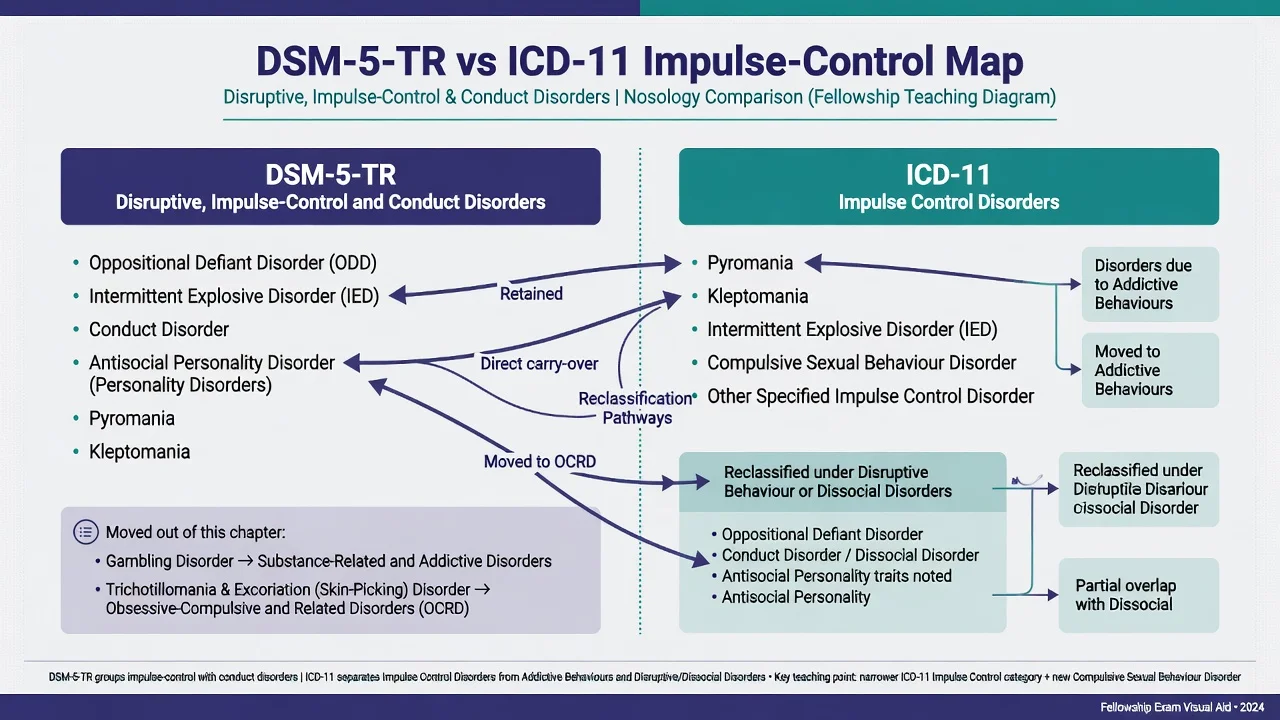
Core chapter members candidates must list: oppositional defiant disorder (ODD); intermittent explosive disorder (IED); conduct disorder (CD); antisocial personality disorder (ASPD) (also in the personality chapter); pyromania; kleptomania; plus other specified and unspecified disruptive, impulse-control, and conduct disorders.[1][5]
High-yield reclassifications out of the old impulse-control basket
- Gambling disorder moved into Substance-Related and Addictive Disorders (behavioural addiction framing; criteria reworked versus DSM-IV pathological gambling).[12]
- Trichotillomania and excoriation (skin-picking) disorder moved into Obsessive-Compulsive and Related Disorders.[1][2]
- Pathological shopping, non-paraphilic hypersexuality, and internet use problems are not free-standing DSM-5-TR ICD diagnoses in the same way; formulate carefully and use other specified categories only when justified.[2][11]
ICD-11: Impulse control disorders
ICD-11 groups pyromania, kleptomania, intermittent explosive disorder, and compulsive sexual behaviour disorder (CSBD) among impulse control disorders (with residual other/unspecified codes). Gambling disorder and gaming disorder sit under disorders due to addictive behaviours. ODD/CD-type presentations live under disruptive behaviour or dissocial disorders. State which system you are coding when an examiner asks “where does CSBD sit?” — ICD-11 impulse control, not automatically a paraphilic disorder.[11][12]
DSM-5-TR DICCD
- ODD, IED, CD, ASPD cross-list
- Pyromania, kleptomania
- Other/unspecified DICCD
- Gambling NOT here
ICD-11 Impulse control
- Pyromania, kleptomania, IED
- CSBD included
- Other/unspecified ICD
- Gambling/gaming are addictive behaviours
Moved out (DSM)
- Gambling → addictive disorders
- Trichotillomania → OCRD
- Excoriation → OCRD
- Know the history for MCQs
Formulation axes
- Urge–act–aftermath sequence
- Instrumental vs impulsive
- Comorbidity load
- Iatrogenic agonist pathway
Epidemiology and risk
Headline facts for viva
NCS-R data showed intermittent explosive disorder is far from exotic: lifetime prevalence in the several-percent range depending on narrow versus broad definitions, with substantial role impairment and comorbidity.[4][5] Kleptomania and pyromania remain uncommon in general community samples but appear in specialised clinical and forensic streams; pyromania clinical series document heavy psychiatric comorbidity rather than pure “fire fascination” alone.[8][13] Structured screening of adult psychiatric inpatients finds impulse-control problems more often than unaided clinical detection implies.[3]
Parkinson disease / restless legs. Large cross-sectional work associates dopamine agonist treatment with impulse-control disorders (gambling, hypersexuality, compulsive shopping, binge eating), with clinically important prevalence in treated cohorts; case–control data reinforce the association beyond disease alone.[9][10][16]
Pathophysiology
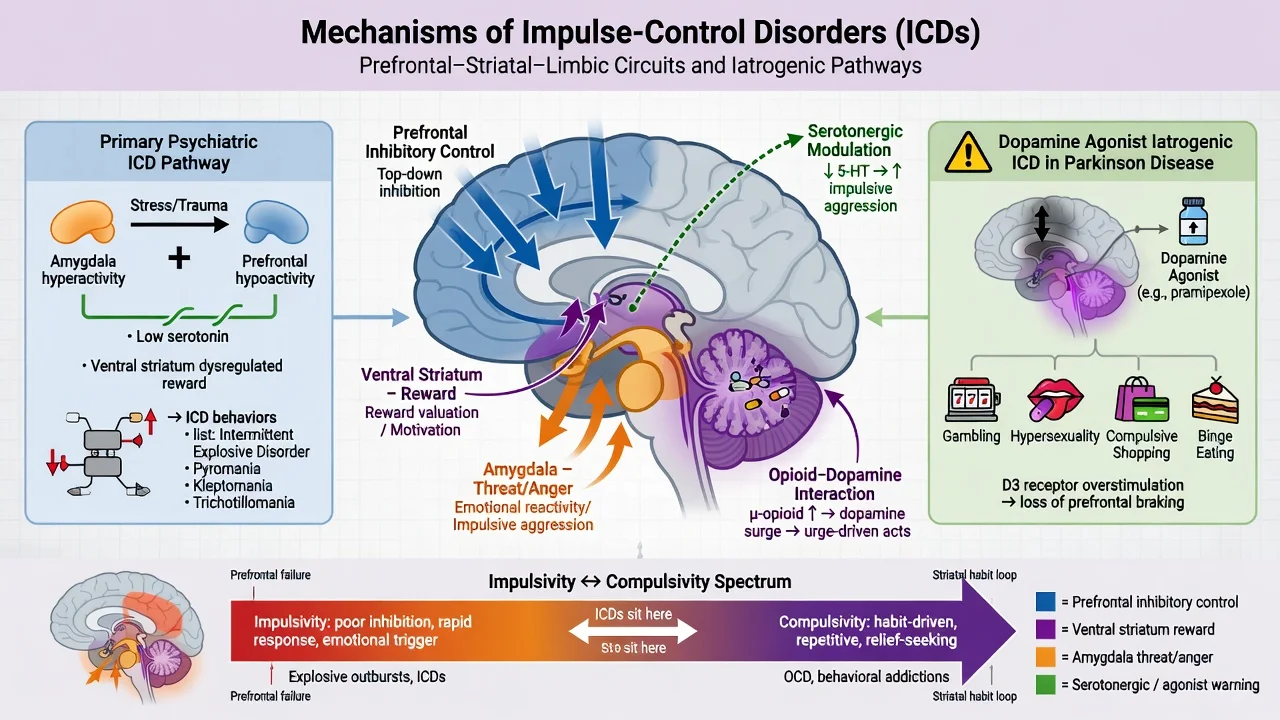
Impulsive aggression (IED-leaning models). Reduced serotonergic tone, impaired prefrontal top-down control, and heightened limbic/amygdala reactivity provide a coherent framework for reactive outbursts and for why SSRIs were tested in IED.[5][6]
Urge-driven “behavioural addiction-adjacent” acts (kleptomania, historical gambling, CSBD). Cortico-striatal reward and habit learning, cue reactivity, and opioid modulation of mesolimbic dopamine underpin both craving phenomenology and the trial rationale for opioid antagonists.[2][7][12]
Iatrogenic pathway. D2/D3-preferring dopamine agonists can unmask ICDs in Parkinson disease and RLS; this is a drug-effect formulation until the medication is reviewed, not a moral failure.[9][10][16]
Clinical presentation by core disorders
Intermittent explosive disorder
Recurrent behavioural outbursts representing a failure to control aggressive impulses, manifested as verbal aggression or physical aggression toward property, animals, or people. DSM-5 emphasises frequency criteria: frequent lower-intensity outbursts (A1) and/or less frequent high-intensity outbursts causing damage or injury (A2); aggression is grossly out of proportion to provocation and is not premeditated for tangible objectives such as money, power, or intimidation (those point toward instrumental aggression/ASPD pathways).[5][15] Age, developmental, and exclusion rules (not better explained by another mental disorder, medical condition, or substance) must be applied.[5]
Kleptomania
Recurrent failure to resist impulses to steal objects that are not needed for personal use or monetary value. Tension before theft; pleasure, gratification, or relief at the time of committing the theft; stealing not committed to express anger or vengeance and not in response to delusion or hallucination; not better explained by CD, mania, or ASPD.[2][13] Clinical samples show high rates of mood and substance comorbidity and substantial shame/concealment.[13]
Pyromania
Deliberate and purposeful fire-setting on more than one occasion; tension or affective arousal before the act; fascination with fire and its contexts; pleasure/relief when setting fires or witnessing aftermath; not done for monetary gain, ideology, concealment of crime, expression of anger/vengeance, better explained by impaired judgment (e.g. neurocognitive disorder, intoxication), or accounted for by CD, mania, or ASPD.[8] Most people charged with arson do not meet pyromania — that is a classic exam discriminator.[8]
CSBD (ICD-11 framing)
Persistent pattern of failure to control intense, repetitive sexual impulses or urges resulting in repetitive sexual behaviour, with marked distress or impairment, continued despite little satisfaction or adverse consequences. CSBD is not a licence to pathologise high consensual desire alone, and it is not automatically a paraphilic disorder (paraphilic disorders retain harm/consent/distress framing of atypical arousal targets).[11]
Developmental disruptive pathway
ODD and CD are developmental disruptive disorders with their own criteria, trajectories into ASPD for a subset, and dedicated atlas leaves — mention them in the group map without replacing those topics.[1]
MSE language. Document triggers, prodromal tension, urge intensity, ability to delay, insight, regret versus ego-syntonic pride, concealment, substance use around episodes, and multi-domain risk (violence, arson, sexual harm, legal, financial, suicide).[2][3]
Differential diagnosis
Mania / mixed
- Decreased need for sleep, grandiosity
- Multi-domain disinhibition
- Episode timeline
- Stabilise mood then reassess ICD
Substance-driven
- Alcohol/stimulant-linked aggression or theft
- Still screen independent ICD when sober
- Withdrawal can worsen irritability
- Integrated dual-diagnosis care
Personality / CD
- Instrumental aggression or theft for gain
- Cross-context enduring pattern
- ASPD requires conduct history rules
- Do not force kleptomania label
Organic / iatrogenic
- Dopamine agonist ICDs
- Frontal injury, bvFTD red flags
- Seizures, encephalitis when atypical
- Drug review before new labels stick
Also separate OCRD body-focused repetitive behaviours from kleptomania/pyromania, and separate CSBD from paraphilias and from non-pathological sexual diversity.[2][11]
Clinical and bedside assessment
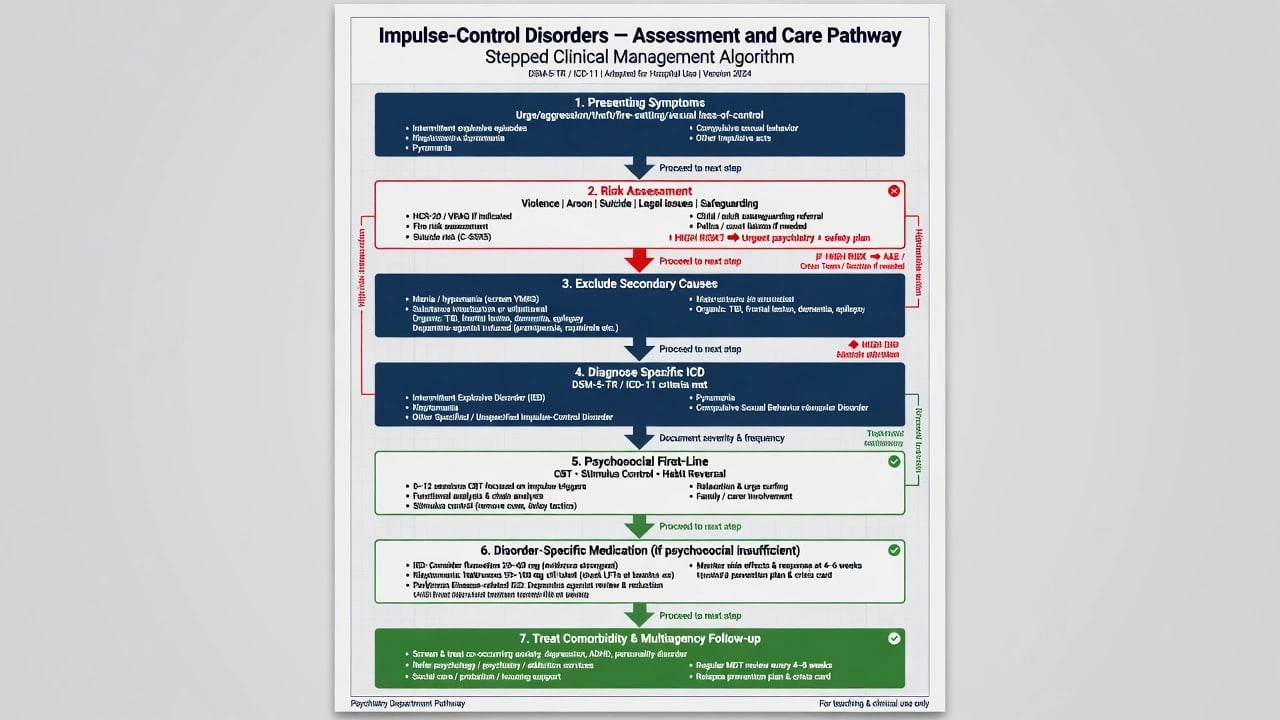
Structure the interview around: (1) urge–act–aftermath narrative; (2) frequency, severity, weapons/fire/sexual risk details; (3) instrumental motives versus impulsive loss of control; (4) full psychiatric review of systems (mood, psychosis, trauma, ADHD, personality); (5) substances; (6) medications (dopamine agonists, stimulants); (7) legal history and current charges; (8) collateral; (9) capacity when decisions or justice processes are live.[2][3][14]
Tools. The Minnesota Impulse Disorders Interview (MIDI) is a structured clinical interview validated for impulse-control disorder enquiry in research and specialty settings — know the concept even if your service uses local forms.[14] In Parkinson disease, QUIP / QUIP-RS family questionnaires support systematic ICD screening with patient and informant input.[9][16]
Risk domains (non-optional). Violence to others; intimate-partner violence; arson and public safety; sexual harm; child protection; financial collapse; suicide after shame or legal crisis.[4][8]
Investigations
No blood test diagnoses primary ICDs. Use urine drug screen when substances may drive or mimic episodes; LFTs (and pregnancy test when relevant) before naltrexone; metabolic panel and ECG if starting SSRIs or other psychotropics in at-risk patients; medication reconciliation for agonists. Imaging or EEG only for neurological red flags (late abrupt onset, focal signs, cognitive decline, seizures).[2][7][9]
Acute / crisis management
There is no classic autonomic detox protocol for pure kleptomania, pyromania, or IED. Crisis care is risk containment, treatment of intoxication/withdrawal, urgent agonist review when relevant, and suicide assessment after legal or interpersonal catastrophe.[2][9]
Definitive management
Shared psychosocial pillars
Motivational interviewing for ambivalence; CBT packages targeting triggers, cognitive justifications, urge surfing, stimulus control, problem-solving, and relapse prevention; contingency management where ethical and feasible; family psychoeducation without collusive secrecy; vocational and legal advocacy as indicated.[2][1]
Disorder-specific medical notes (exam-level)
IED. Psychological anger-regulation/CBT approaches are foundational. Fluoxetine has double-blind RCT support for reducing aggression in IED compared with placebo; practical adult framing often starts around fluoxetine 20 mg orally daily, with review for activation, akathisia, sexual side effects, and suicidality risk (especially younger adults), titration toward trial-range doses under specialist supervision when tolerated, and parallel psychosocial care. Individualise using local product information; treat alcohol and other SUD aggressively because they fuel outbursts.[6][5]
Kleptomania. CBT and stimulus control (shopping triggers, accompaniment strategies) first. Naltrexone showed benefit versus placebo for kleptomania urges/behaviour in a double-blind trial — counsel as off-label, obtain baseline LFTs, exclude acute hepatitis and current opioid use (precipitated withdrawal), and typically discuss oral naltrexone starting about 50 mg daily with monitoring rather than as a solo “cure.”[7][13]
Pyromania. Specialised behavioural programmes, fire-safety planning, and multiagency risk management; pharmacotherapy is not primary and should target comorbidity.[8]
CSBD. CBT-based control and values work, relationship interventions, treat depression/SUD/trauma; avoid moral panic and avoid missing paraphilic harm patterns that need a different risk frame.[11]
Parkinson/RLS agonist ICDs. Primary intervention is agonist dose reduction, cessation, or switch with neurology liaison; add psychosocial support; do not leave the agonist unchanged while only starting an SSRI or naltrexone.[9][10][16]
Comorbidity
Mood disorders, SUD, ADHD, trauma-related disorders, and personality pathology are common and often drive impairment more than the ICD label alone — integrated care beats sequential ping-pong.[3][4][13]
FRANZCP-aligned practice expects structured risk assessment, dual diagnosis competence, culturally safe care for Aboriginal and Torres Strait Islander and Māori peoples, and realistic off-label pharmacotherapy counselling. Justice liaison, child protection, and gambling-help pathways may all interface depending on the act type. Dopamine-agonist ICDs require neurology co-management in PD/RLS clinics.[2][9]
Subtypes and scenarios
Community IED after minor provocations with relationship and occupational collapse. Forensic aggression requiring instrumental-versus-impulsive formulation. Retail kleptomania versus organised theft rings. Arson assessment where pyromania is the uncommon answer. PD multi-ICD cluster (gambling + hypersexuality + shopping). Youth ODD/CD evolving toward adult externalising disorders. CSBD with pornography escalation and partner distress without paraphilic targets.[5][8][9][11]
Complications and pitfalls
Other pitfalls: moralising without CBT offer; missing mania or SUD; missing agonists; naltrexone without LFTs; ignoring post-offence suicide risk; confusing ASPD instrumental violence with IED; pathologising consensual sexuality as CSBD without loss-of-control and impairment criteria.[2][5][7][11]
Prognosis and disposition
Course is often chronic-relapsing when comorbidity and environmental triggers persist; engagement with therapy, reduced cue access, legal/social stabilisation, and treated dual diagnosis improve outlook.[1][2] Agonist-related ICDs frequently improve after drug adjustment.[9][16] Disposition ladder: GP/shared care and psychology → specialist psychiatry/addiction/sexual health as relevant → forensic services for high violence/arson risk → inpatient only for acute risk or severe dual diagnosis, not for “urge detox” theatre.[2]
Special populations
Adolescents. Prefer ODD/CD frameworks first; family and school interventions; child protection when aggression or fire-setting endangers others.[1] Women with kleptomania. Clinical samples often female-predominant; shame barriers delay help.[13] Older adults. New impulsivity triggers organic and medication review (including dopamine agonists).[9] Intellectual disability. Behavioural phenotypes, capacity, and positive behaviour support — avoid dumping all challenging behaviour into “ICD.” Cultural safety. Justice over-representation and stigma require non-racist formulation and advocacy, not stereotype-based risk inflation.[2]
Evidence and guidelines
Name at viva: Dell'Osso 2006 and Schreiber/Grant 2011 ICD reviews; Grant 2005 inpatient screening; Kessler NCS-R IED 2006; Coccaro DSM-5 IED framing and A1/A2 validity work; Coccaro fluoxetine RCT 2009; Grant naltrexone kleptomania RCT 2009; Grant pyromania comorbidity series; Weintraub 2006/2010 and Voon 2011 agonist ICD studies; Chamberlain MIDI validation; Kraus CSBD ICD-11; Potenza gambling primer for reclassification context.[1][2][3][4][5][6][7][8][9][10][11][12][14][15][16]
Exam pearls
IMPULSE
Self-test: chapter map and two drug facts
List DSM-5-TR DICCD members and two disorders that left the old impulse-control basket. State ICD-11 placement of CSBD. Quote IED as a several-percent lifetime disorder in NCS-R-type data. Name fluoxetine RCT evidence for IED and naltrexone RCT evidence for kleptomania with LFT counselling. Name Weintraub-level dopamine-agonist ICD association.[4][5][6][7][9][11]
References
- [1]Dell'Osso B, Altamura AC, Allen A, Marazziti D, Hollander E Epidemiologic and clinical updates on impulse control disorders: a critical review Eur Arch Psychiatry Clin Neurosci, 2006.PMID 16960655
- [2]Schreiber L, Odlaug BL, Grant JE Impulse control disorders: updated review of clinical characteristics and pharmacological management Front Psychiatry, 2011.PMID 21556272
- [3]Grant JE, Levine L, Kim D, Potenza MN Impulse control disorders in adult psychiatric inpatients Am J Psychiatry, 2005.PMID 16263865
- [4]Kessler RC, Coccaro EF, Fava M, Jaeger S, Jin R, Walters E The prevalence and correlates of DSM-IV intermittent explosive disorder in the National Comorbidity Survey Replication Arch Gen Psychiatry, 2006.PMID 16754840
- [5]Coccaro EF Intermittent explosive disorder as a disorder of impulsive aggression for DSM-5 Am J Psychiatry, 2012.PMID 22535310
- [6]Coccaro EF, Lee RJ, Kavoussi RJ A double-blind, randomized, placebo-controlled trial of fluoxetine in patients with intermittent explosive disorder J Clin Psychiatry, 2009.PMID 19389333
- [7]Grant JE, Kim SW, Odlaug BL A double-blind, placebo-controlled study of the opiate antagonist, naltrexone, in the treatment of kleptomania Biol Psychiatry, 2009.PMID 19217077
- [8]Grant JE, Won Kim S Clinical characteristics and psychiatric comorbidity of pyromania J Clin Psychiatry, 2007.PMID 18052565
- [9]Weintraub D, Koester J, Potenza MN, Siderowf AD, Stacy M, Voon V, et al. Impulse control disorders in Parkinson disease: a cross-sectional study of 3090 patients Arch Neurol, 2010.PMID 20457959
- [10]Weintraub D, Siderowf AD, Potenza MN, Goveas J, Morales KH, Duda JE, et al. Association of dopamine agonist use with impulse control disorders in Parkinson disease Arch Neurol, 2006.PMID 16831966
- [11]Kraus SW, Krueger RB, Briken P, First MB, Stein DJ, Kaplan MS, et al. Compulsive sexual behaviour disorder in the ICD-11 World Psychiatry, 2018.PMID 29352554
- [12]Potenza MN, Balodis IM, Derevensky J, Grant JE, Petry NM, Verdejo-Garcia A, et al. Gambling disorder Nat Rev Dis Primers, 2019.PMID 31346179
- [13]Grant JE, Odlaug BL, Kim SW Kleptomania: clinical characteristics and relationship to substance use disorders Am J Drug Alcohol Abuse, 2010.PMID 20575650
- [14]Chamberlain SR, Grant JE Minnesota Impulse Disorders Interview (MIDI): Validation of a structured diagnostic clinical interview for impulse control disorders Psychiatry Res, 2018.PMID 29772488
- [15]Coccaro EF, Lee R, McCloskey MS Validity of the new A1 and A2 criteria for DSM-5 intermittent explosive disorder Compr Psychiatry, 2014.PMID 24321204
- [16]Voon V, Sohr M, Lang AE, Potenza MN, Siderowf AD, Whetteckey J, et al. Impulse control disorders in Parkinson disease: a multicenter case--control study Ann Neurol, 2011.PMID 21416496