Psych · General adult psychiatry — impulse control
Intermittent explosive disorder
Also known as IED · Impulse-control disorder aggression · Explosive anger attacks · Impulsive aggression disorder · Rage attacks (clinical IED)
Exam-exhaustive fellowship reference on intermittent explosive disorder — DSM-5-TR A1/A2 frequency criteria, impulsive vs instrumental aggression, NCS-R and WMH epidemiology, serotonergic and SEIP mechanisms, differentials vs ASPD/BPD/bipolar/substance/organic, OAS-M assessment, CBT and fluoxetine RCT evidence, AED adjuncts, risk and forensic interface. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Intermittent explosive disorder (IED) is a high-yield general-adult and forensic-interface topic at FRANZCP, MRCPsych, and ABPN level. Examiners test operational criteria (especially A1 vs A2 frequency traps), the impulsive-versus-instrumental aggression distinction, differentials from ASPD, BPD, bipolar mania, and substance/organic causes, epidemiology that is more common than older textbooks implied, and a treatment story that is evidence-limited but not nihilistic: multicomponent CBT, fluoxetine, and cautious AED use while treating comorbidity and protecting victims.[1][2][3]
Overview and definition
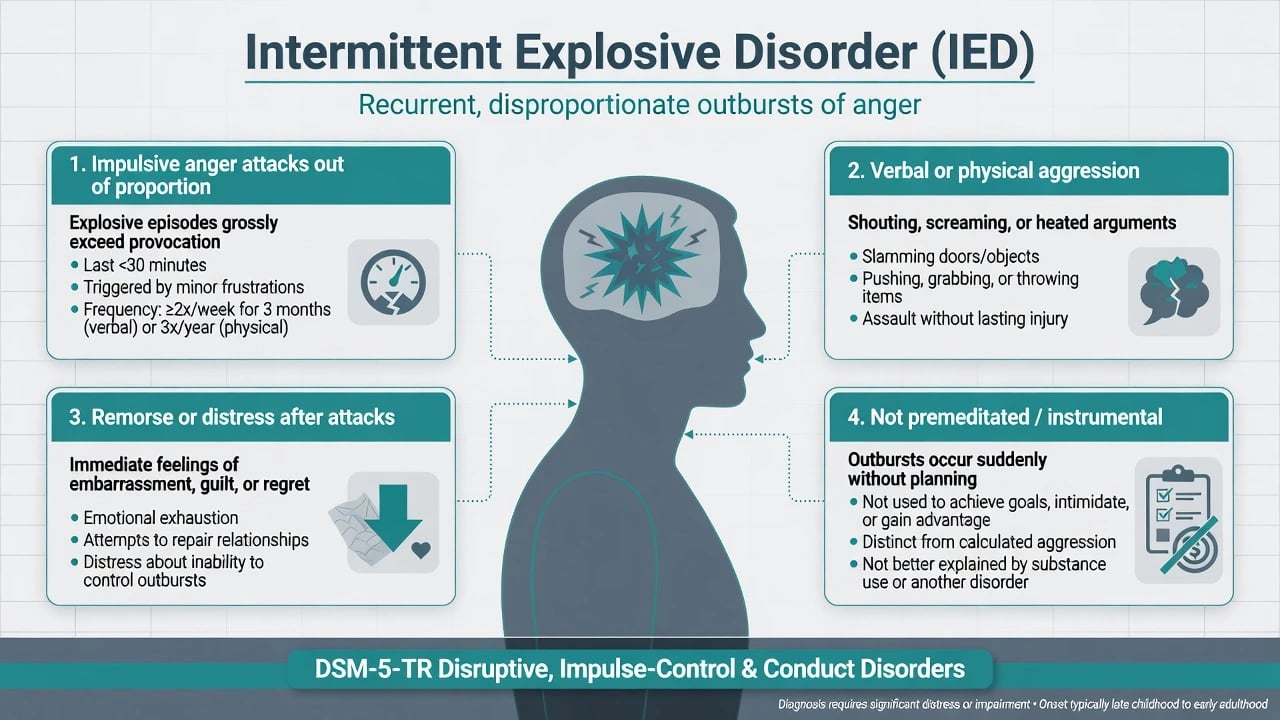
IED is defined by recurrent behavioural outbursts representing a failure to control aggressive impulses, where the aggression is grossly out of proportion to any precipitating psychosocial stressors, is impulsive and/or anger-based rather than premeditated, is not aimed primarily at tangible objectives (money, intimidation as planned instrument), causes marked distress or impairment (or legal/financial consequences), occurs at chronological age ≥6 years (or equivalent developmental level), and is not better explained by another mental disorder, medical condition, or the physiological effects of a substance.[2]
Clinical essence for viva. Think reactive, affective aggression in discrete “attacks,” often followed by remorse, embarrassment, or relief — not the remorseless instrumental pattern that characterises classic ASPD narratives. Between attacks the person may function well or show residual irritability; the diagnosis still requires frequency/severity thresholds and exclusion logic.[2]
DSM-5-TR placement. IED sits in Disruptive, Impulse-Control, and Conduct Disorders alongside ODD, CD, pyromania, kleptomania, and related categories. This is not a personality disorder diagnosis, though Cluster B comorbidity is common and must be formulated separately.[2]
ICD-11. Expect impulse-control disorder framing with recurrent failure to control aggressive impulses and clinically significant distress/impairment; always state which manual you are using when criteria thresholds are examined.[2]
Classification and criterion map
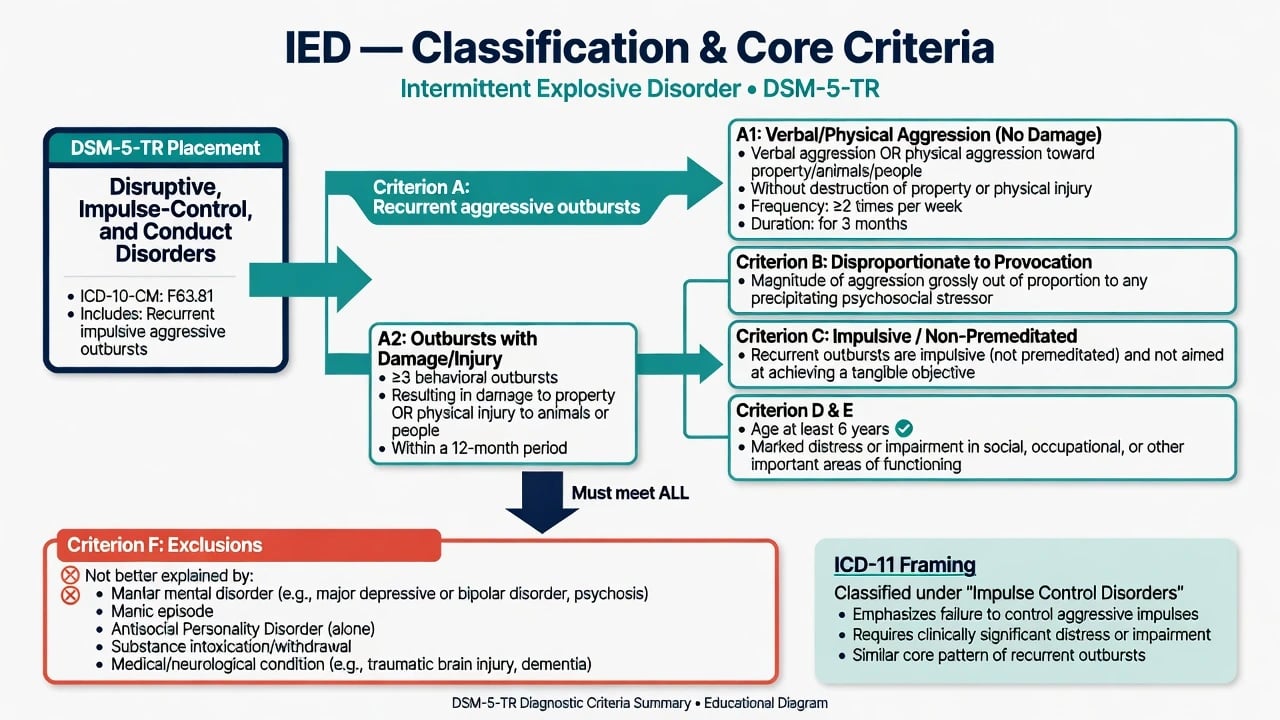
Criterion A1 path
- Verbal aggression and/or physical aggression without damage
- Toward property, animals, or other individuals
- Average ≥ twice weekly for 3 months
- Does not require injury or destruction
Criterion A2 path
- Three behavioural outbursts within 12 months
- Involve damage/destruction of property and/or
- Physical assault causing injury to animals/people
- Higher severity threshold, lower frequency
Shared required features
- Grossly disproportionate to provocation
- Impulsive/anger-based, not premeditated
- Not primarily for tangible gain
- Age ≥6; distress/impairment/consequences
Key exclusions
- Not better explained by mania/bipolar
- Not better explained by psychosis
- Not solely substance intoxication/withdrawal
- Not better explained by ASPD/CD alone or medical
Research criteria (IED-IR and Coccaro’s programme of work) tightened frequency, impairment, and exclusion rules and underpinned the DSM-5 reconceptualisation of IED as a disorder of impulsive aggression rather than only rare catastrophic assaults.[2]
Epidemiology and risk factors
Headline epidemiology (exam numbers)
US NCS-R data found lifetime and 12-month DSM-IV IED prevalence of approximately 7.3% and 3.9%, with numerous lifetime attacks and meaningful property damage costs — examiners use these figures to counter the myth that IED is vanishingly rare.[1] Cross-national World Mental Health analyses yield a lower average lifetime prevalence (~0.8%) with wide between-country variation; quote the dataset you mean.[9] Adolescent NCS-A work shows early onset, high persistence, and substantial comorbidity, reinforcing early recognition.[8]
Risk and developmental correlates. Childhood maltreatment is associated with IED and with suicidal behaviour pathways; formulate trauma without collapsing IED into PTSD alone.[10] Family loading for aggression/impulse-control problems, modelling of explosive coping, and comorbid externalising disorders raise risk. Self-harm and suicide attempts are elevated especially when IED co-occurs with personality disorder or PTSD.[11][12]
Pathophysiology and maintaining model
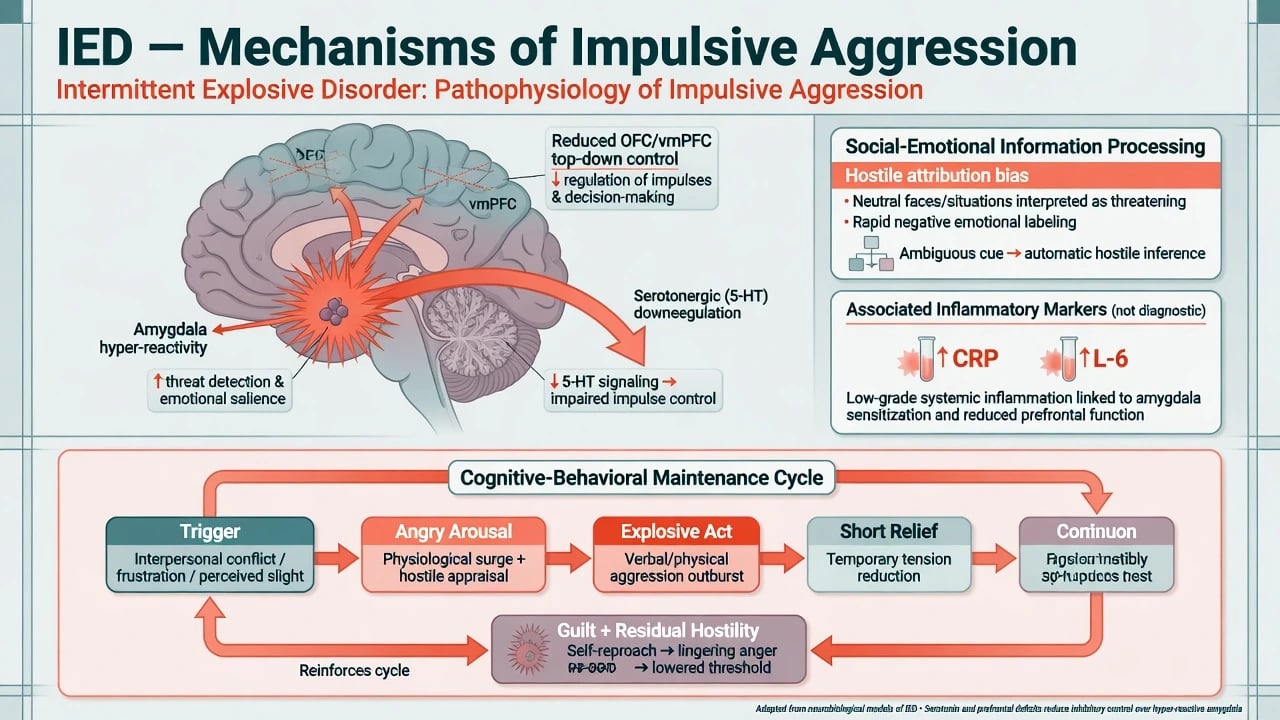
Serotonergic model. Indices of reduced central 5-HT function associate with impulsive aggression; fluoxetine’s anti-aggressive effects in impulsive-aggressive personality-disordered subjects and in IED RCTs provide clinical pharmacological support without proving a single-cause biology.[3][5]
Circuit and social cognition. Teaching-level framing emphasises amygdala threat hyper-reactivity with insufficient orbitofrontal/ventromedial prefrontal top-down control, plus hostile attribution bias and impaired social-emotional information processing on ambiguous interpersonal cues.[16] Inflammatory markers (e.g. CRP, IL-6) can be elevated at group level in IED and correlate with aggression measures — research correlate only, not a clinic test.[13]
CBT maintaining cycle (viva-ready). Trigger (perceived slight) → physiological arousal + hostile appraisal → explosive act → short tension reduction → guilt/residual hostility → lowered threshold for next trigger. Treatment targets arousal regulation, reappraisal, and problem-solving — not “anger venting” as catharsis.[4][16]
Clinical presentation
Attacks often escalate within minutes after minor frustration (traffic, criticism, queues, partner disagreement): raised voice, threats, throwing/breaking objects, pushing/hitting, then rapid de-escalation over minutes to hours. Patients frequently report later remorse, amnesia for parts of the peak, or shame — useful but not pathognomonic.[2]
MSE language. Affect may be irritable or euthymic between episodes; thought form usually intact; no primary delusions of persecution required (ideas of unfairness are common); insight into harmfulness of attacks is often partial; risk assessment must cover others (partners, children, co-workers) and self.[2][11]
Settings. ED after assault or property damage; couple/family clinic after domestic incidents; forensic/court-mandated “anger management”; occupational health after workplace outbursts; adolescent services after school fights. Always ask about weapons, substance proximity, and victim safety.[1][12]
Differential diagnosis
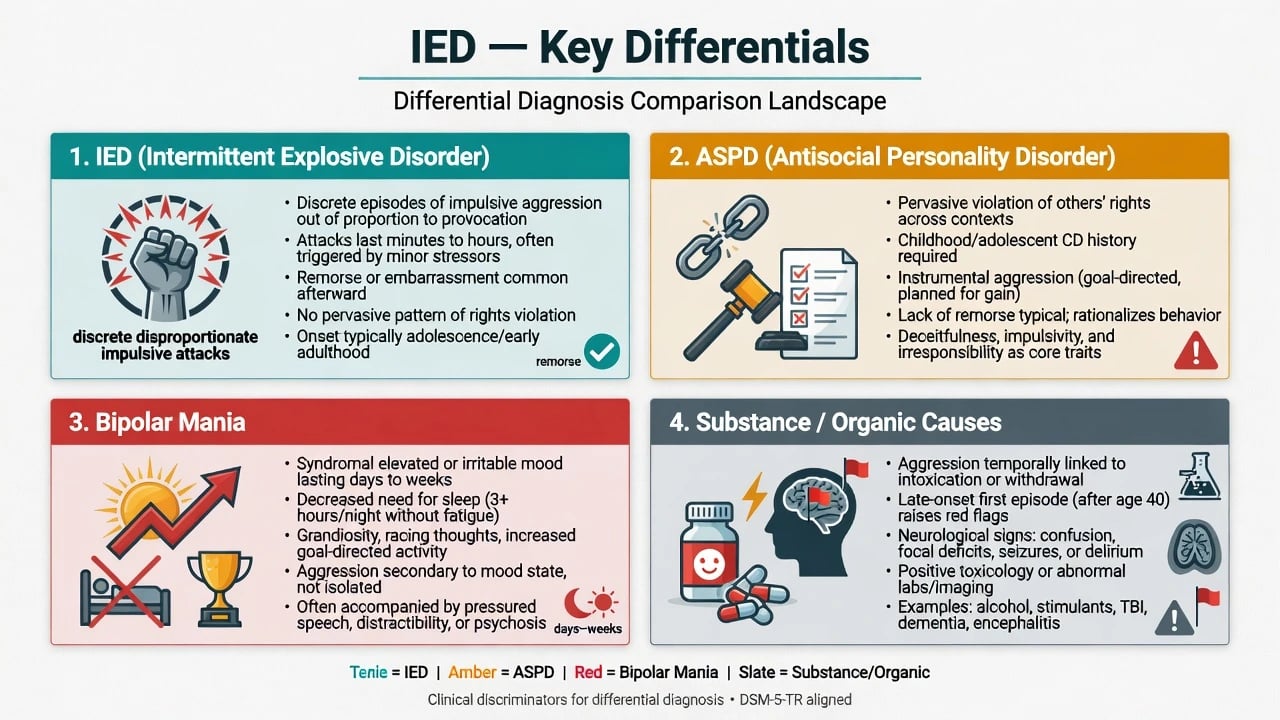
ASPD
- Pervasive rights violation since adolescence
- Conduct disorder onset before 15 required for DSM ASPD
- Instrumental aggression and lack of remorse common
- IED attacks can co-occur — formulate both if criteria met
BPD
- Affective instability, abandonment fear, identity disturbance
- Self-harm often for affect regulation
- Anger is one facet of broader PD pattern
- Comorbidity frequent; primary problem may be BPD
Bipolar mania/mixed
- Elevated/expansive/irritable mood days–weeks
- Decreased need for sleep, grandiosity, racing thoughts
- Aggression secondary to syndromal mood episode
- Do not call manic rage 'IED'
Substance / organic
- Aggression tightly linked to alcohol/stimulants
- Late-onset change → TBI, FTD, seizure, delirium
- UDS, neuro exam, imaging/EEG when indicated
- Treat the driver first
Also discriminate ADHD impulsivity without explosive attack criteria, ODD/CD developmental patterns in youth, autism-related meltdowns in sensory overload contexts, psychotic aggression under command delusions, and deliberate planned violence for gain (criminal instrumental aggression ≠ IED).[2]
Assessment
Structure the aggression history: frequency, duration, triggers, peak behaviours, weapons, injury, remorse, premeditation, substance timing, childhood conduct, legal chronology, trauma, and current goals. Collateral from partners, family, workplace, and records is essential; self-report alone may minimise or externalise.[1][2]
Risk. Separate static (prior assaults, male sex, early onset, prior weapons use) from dynamic (intoxication, acute grievance, weapon access, sleep deprivation, non-adherence, recent escalation) and protective factors (engagement, substance remission, prosocial supports, supervised living). Structured tools inform professional judgement; they do not perfectly predict individual violence.[11][12]
Scales. The Overt Aggression Scale–Modified (OAS-M) is widely used in impulsive-aggression trials to track verbal aggression, aggression against objects, and aggression against others — useful for measurement-based care, not stand-alone diagnosis.[3][7]
Investigations. Clinical diagnosis. Obtain UDS when relevant; baseline labs and ECG before selected pharmacotherapy; neuroimaging/EEG for late onset, focal neurology, seizures, cognitive decline, or significant TBI history. Screen mood, PTSD, SUD, ADHD, and personality pathology systematically.[2][10]
Acute / emergency management
Acute care targets imminent harm, not personality remoulding. Document capacity for decisions, duty-to-protect reasoning without inventing statute numbers, and early dual-diagnosis liaison when substances drive attacks.[2]
Definitive management
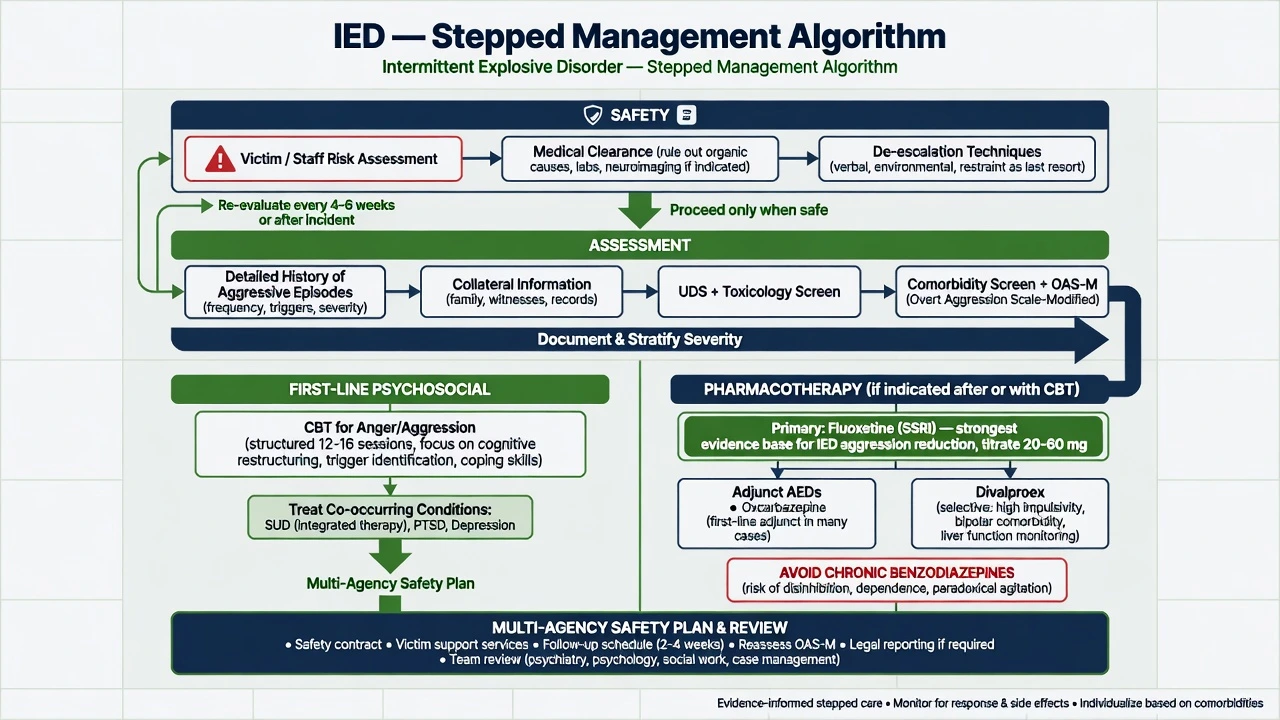
Psychological therapy
Multicomponent CBT for IED (group and individual formats) showed reductions in aggressive behaviour in a pilot randomised trial versus wait-list, adapting anger-focused CBT elements (arousal reduction, cognitive restructuring of hostile appraisals, problem-solving, relapse prevention).[4] In practice, offer structured CBT-informed anger/aggression work, couples/family sessions when safe, and integrated substance treatment when alcohol or stimulants lower the threshold for attacks.[4]
Pharmacotherapy
There is no TGA/FDA-approved drug labelled specifically for IED. Evidence-based teaching still has a clear hierarchy based on randomised trials of impulsive aggression and IED rather than marketing labels.[3][14]
Fluoxetine (best-known IED SSRI RCT). In a double-blind placebo-controlled trial in IED, fluoxetine produced sustained reductions in OAS-M aggression and irritability scores.[3] Earlier work in impulsive-aggressive personality-disordered subjects also supported anti-aggressive effects of fluoxetine versus placebo.[5] A practical fellowship regimen (individualise): start fluoxetine 20 mg orally daily, review response and adverse effects at 2–4 weeks, titrate toward the 20–60 mg daily range used in aggression literature as tolerated, continue an adequate trial (often ≥8–12 weeks) before declaring failure, monitor for activation/akathisia, sexual side-effects, hyponatraemia risk in older adults, and suicide risk early in treatment, especially if comorbid depression is present.[3][5]
AED adjuncts for impulsive aggression. Oxcarbazepine reduced impulsive aggression versus placebo in a double-blind trial of adults with clinically significant impulsive aggression.[6] Divalproex showed benefit for impulsive aggression particularly in Cluster B personality disorder subgroups in a multicentre RCT; it is not a blanket first drug for all IED and requires LFTs, FBC, weight/metabolic review, and strict pregnancy avoidance counselling (teratogenicity).[7] Cochrane and meta-analytic work on antiepileptics/mood stabilisers for aggression suggests possible benefit for selected agents with heterogeneous methods — interpret cautiously and prioritise safety labs and informed consent.[14][15]
What to avoid as “anti-aggression defaults.” Chronic benzodiazepines risk dependence, disinhibition, and paradoxical agitation. Long-term antipsychotic “chemical restraint” without a clear target symptom, time limit, and metabolic/EPS monitoring is poor practice. Lithium and other agents appear in broader aggression literature but are not automatic IED first-line without comorbidity-driven rationale.[14][15]
Comorbidity and social interventions
Treating alcohol/stimulant use, PTSD, depression, and ADHD (carefully) is often higher-yield for risk reduction than chasing pure “anger chemistry.” Psychoeducation (attack diary, early-warning signs, time-out plans that do not abandon partners unsafely), occupational/legal liaison, and multi-agency risk meetings when domestic violence is present complete the plan.[10][12]
Subtypes and clinical scenarios
- A1-predominant verbal/aggression-without-damage vs A2 damage/injury patterns — same disorder concept, different frequency/severity doors.[2]
- IED + SUD — aggression often clusters around intoxication; still assess sober-period attacks.[1]
- IED + PTSD — higher suicidal behaviour burden; integrate trauma-focused care and dual risk formulation.[12]
- IED + Cluster B PD — formulate primary longitudinal pattern; divalproex evidence partly cluster-B enriched.[7][11]
- Adolescent pathway — early onset, school impairment, family conflict; differentiate ODD/CD; family-based behavioural work primary.[8]
- Forensic/court-mandated anger programme — clarify whether criteria for IED are met or whether ASPD/substance pathology dominates; honest prognosis for engagement.[2]
Complications and pitfalls
Misdiagnosis traps include labelling all domestic violence as IED (misses coercive control and ASPD), missing mania, and therapeutic nihilism (“nothing works”) that withholds CBT, SUD care, and fluoxetine trials with evidence signals.[2][3][4]
Prognosis and disposition
Without intervention, course is often persistent from early onset through adulthood, with recurrent relational, occupational, legal, and injury costs.[1][8] Better trajectories associate with treatment engagement, substance remission, stable supports, and treated comorbidity. Most care is outpatient with a written risk plan; step up to crisis admission or forensic pathways when imminent harm cannot be contained, weapons are active risks, or multi-agency thresholds for public protection are met.[2][12]
Special populations
Children/adolescents. Diagnostic age floor ≥6 years; tantrums, ODD, CD, autism, and family violence exposure require careful discrimination; prioritise behavioural parent training/family interventions and school plans before adult-style polypharmacy.[8]
Women. Under-recognised; more verbal/relational patterns possible; assess bidirectional IPV risk and safeguarding of children.[1]
Older adults. New explosive aggression is a neurocognitive/medical red flag, not de novo classic IED.[2]
Pregnancy/lactation. Prefer psychotherapy and non-teratogenic strategies; avoid valproate; if an SSRI is used, document risk–benefit and perinatal monitoring; safety planning for partner/infant is mandatory.[7]
Intellectual disability. Diagnose only with developmental contextualisation; positive behaviour support first; psychotropics target defined symptoms with review dates.[2]
Evidence and regional notes
ANZ (FRANZCP / RANZCP context). No single RANZCP clinical practice guideline titled solely for IED. Apply DSM-5-TR criteria, general principles of violence risk assessment, least-restrictive emergency care, dual-diagnosis integration, and child/family safeguarding frameworks used in Australian and New Zealand public mental health. Prescribe within local formulary and pregnancy safety standards (valproate restrictions).[2][7]
UK (MRCPsych / NICE-adjacent). Use ICD-11/DSM operational knowledge for Paper A/B; for management, map to NICE-related guidance on violence and aggression, personality disorder, and substance misuse services rather than inventing an IED-specific NICE CG number.[2][14]
US (ABPN / APA). DSM-5-TR criteria are primary; APA resources on aggression and impulse-control disorders; fluoxetine and CBT teaching as above; forensic interfaces vary by state duty-to-protect statutes — do not invent section numbers.[2][3][4]
Landmark anchors to name in viva: Kessler NCS-R epidemiology, Coccaro DSM-5 impulsive-aggression review, Coccaro fluoxetine IED RCT, McCloskey CBT RCT, Mattes oxcarbazepine, Hollander divalproex (Cluster B signal), plus maltreatment/suicidality comorbidity papers.[1][2][3][4][6][7]
Exam pearls
- Impulsive/anger-based ≠ instrumental planned violence.[2]
- Age ≥6; not better explained by other disorders — hierarchy matters.[2]
- Fluoxetine has dedicated IED RCT data; start 20 mg oral daily, titrate in the 20–60 mg range with monitoring as above.[3]
- CBT for anger/aggression is first-line psychosocial, not unstructured “venting.”[4]
- Always assess self-harm and partner/child safety, especially with PTSD/PD comorbidity.[11][12]
- Late onset → organic work-up before IED label.[2]
IED ATTACK checklist
References
- [1]Kessler RC, Coccaro EF, Fava M, et al. The prevalence and correlates of DSM-IV intermittent explosive disorder in the National Comorbidity Survey Replication Arch Gen Psychiatry, 2006.PMID 16754840
- [2]Coccaro EF Intermittent explosive disorder as a disorder of impulsive aggression for DSM-5 Am J Psychiatry, 2012.PMID 22535310
- [3]Coccaro EF, Lee RJ, Kavoussi RJ A double-blind, randomized, placebo-controlled trial of fluoxetine in patients with intermittent explosive disorder J Clin Psychiatry, 2009.PMID 19389333
- [4]McCloskey MS, Noblett KL, Deffenbacher JL, et al. Cognitive-behavioral therapy for intermittent explosive disorder: a pilot randomized clinical trial J Consult Clin Psychol, 2008.PMID 18837604
- [5]Coccaro EF, Kavoussi RJ Fluoxetine and impulsive aggressive behavior in personality-disordered subjects Arch Gen Psychiatry, 1997.PMID 9400343
- [6]Mattes JA Oxcarbazepine in patients with impulsive aggression: a double-blind, placebo-controlled trial J Clin Psychopharmacol, 2005.PMID 16282841
- [7]Hollander E, Tracy KA, Swann AC, et al. Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders Neuropsychopharmacology, 2003.PMID 12700713
- [8]McLaughlin KA, Green JG, Hwang I, et al. Intermittent explosive disorder in the National Comorbidity Survey Replication Adolescent Supplement Arch Gen Psychiatry, 2012.PMID 22752056
- [9]Scott KM, Lim CCW, Hwang I, et al. The cross-national epidemiology of DSM-IV intermittent explosive disorder Psychol Med, 2016.PMID 27572872
- [10]Fanning JR, Meyerhoff JJ, Lee R, Coccaro EF History of childhood maltreatment in intermittent explosive disorder and suicidal behavior J Psychiatr Res, 2014.PMID 24935900
- [11]Jenkins AL, McCloskey MS, Kulper D, et al. Self-harm behavior among individuals with intermittent explosive disorder and personality disorders J Psychiatr Res, 2015.PMID 25300440
- [12]Fanning JR, Lee R, Coccaro EF Comorbid intermittent explosive disorder and posttraumatic stress disorder: Clinical correlates and relationship to suicidal behavior Compr Psychiatry, 2016.PMID 27624432
- [13]Coccaro EF, Lee R, Coussons-Read M Elevated plasma inflammatory markers in individuals with intermittent explosive disorder and correlation with aggression in humans JAMA Psychiatry, 2014.PMID 24352431
- [14]Huband N, Ferriter M, Nathan R, Jones H Antiepileptics for aggression and associated impulsivity Cochrane Database Syst Rev, 2010.PMID 20166067
- [15]Jones RM, Arlidge J, Gillham R, et al. Efficacy of mood stabilisers in the treatment of impulsive or repetitive aggression: systematic review and meta-analysis Br J Psychiatry, 2011.PMID 21282779
- [16]Coccaro EF, Fanning JR, Keedy SK, Lee RJ Social cognition in Intermittent Explosive Disorder and aggression J Psychiatr Res, 2016.PMID 27621104