Psych · General adult psychiatry — impulse control
Kleptomania and pyromania
Also known as Pathological stealing · Pathological fire-setting · Impulse-control disorder theft · Impulse-control disorder arson · Kleptomanic stealing · Pyromaniac fire-setting
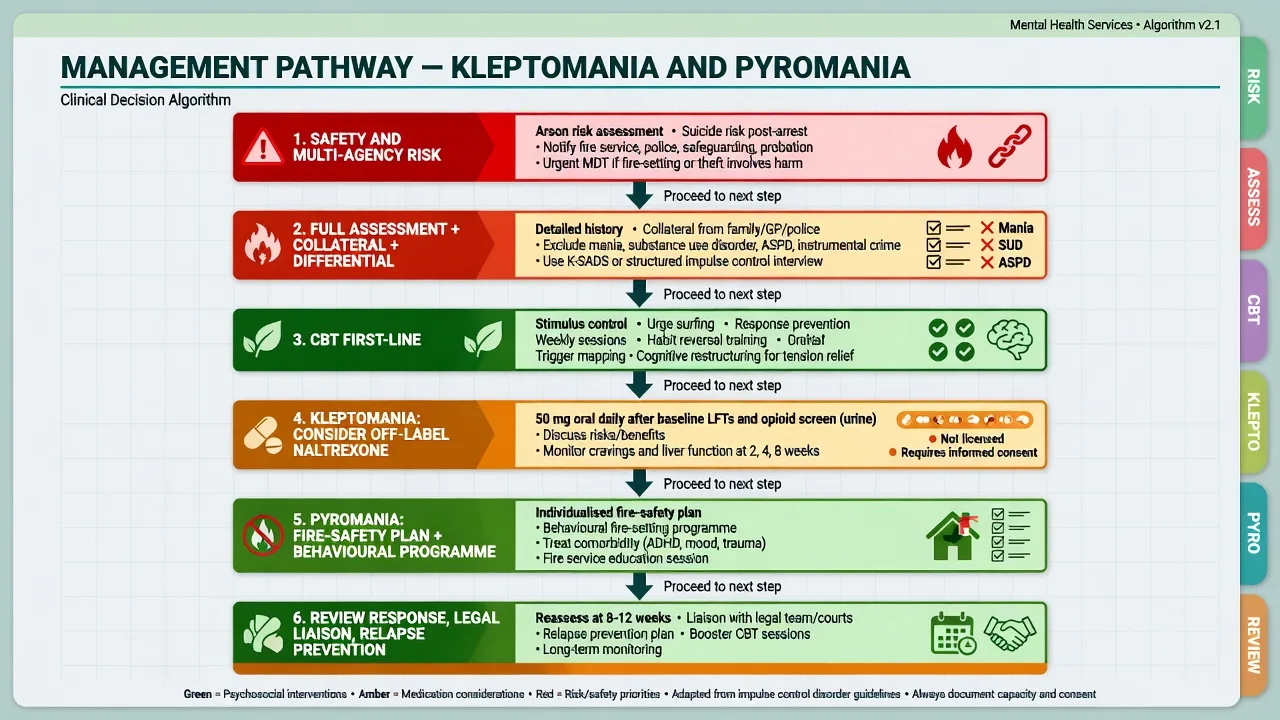
Exam-exhaustive fellowship reference on kleptomania and pyromania — DSM-5-TR and ICD-11 criteria, urge–act–aftermath phenomenology, epidemiology and comorbidity, differentials from instrumental theft/arson mania SUD CD/ASPD, assessment and MIDI concept, CBT and stimulus control, Grant naltrexone RCT with LFT/opioid counselling, Koran escitalopram nuance, multi-agency arson risk and post-arrest suicide assessment. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Kleptomania and pyromania are low-prevalence but high-yield general-adult and forensic-interface topics. Examiners test strict operational criteria, the urge–act–aftermath cycle, the hard truth that most shoplifting and most arson are not these diagnoses, comorbidity (mood, SUD, other ICDs), post-arrest suicide risk, and a treatment story that is evidence-limited yet not empty: CBT skills, Grant’s naltrexone RCT in kleptomania, failed SSRI maintenance signal after open-label response, and multi-agency arson risk management.[1][2][3][5][11]
Overview and definition
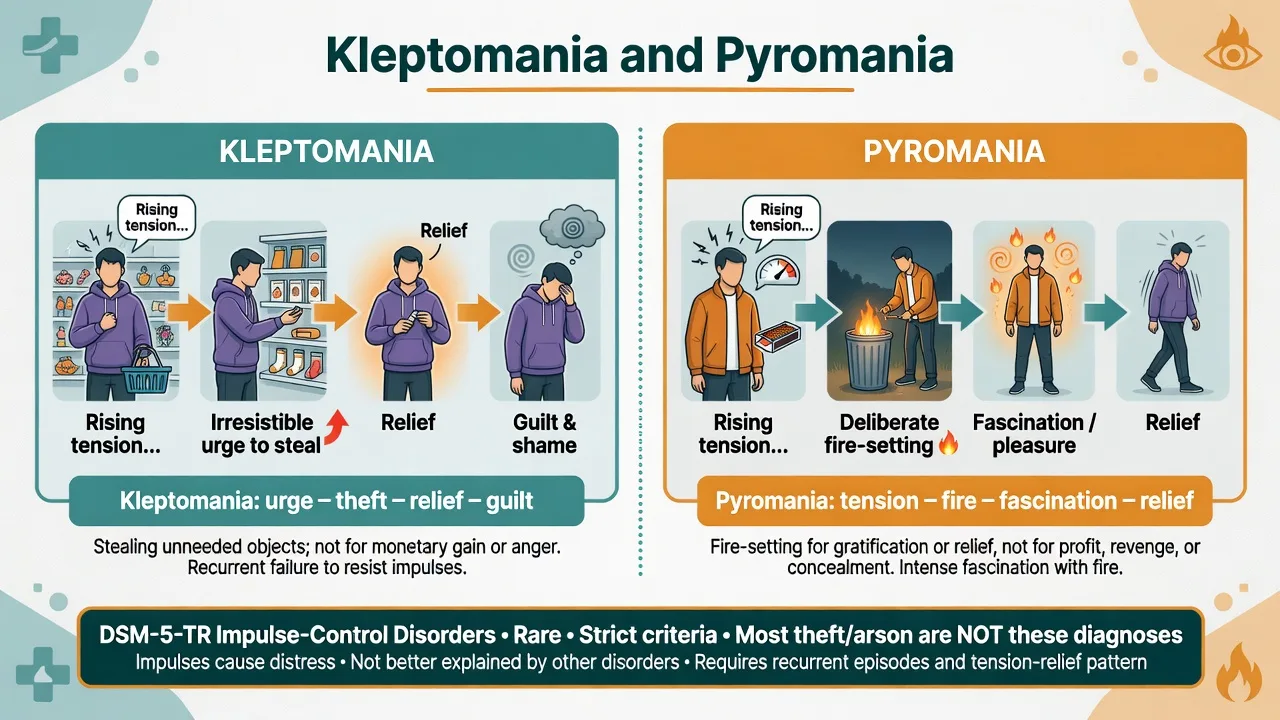
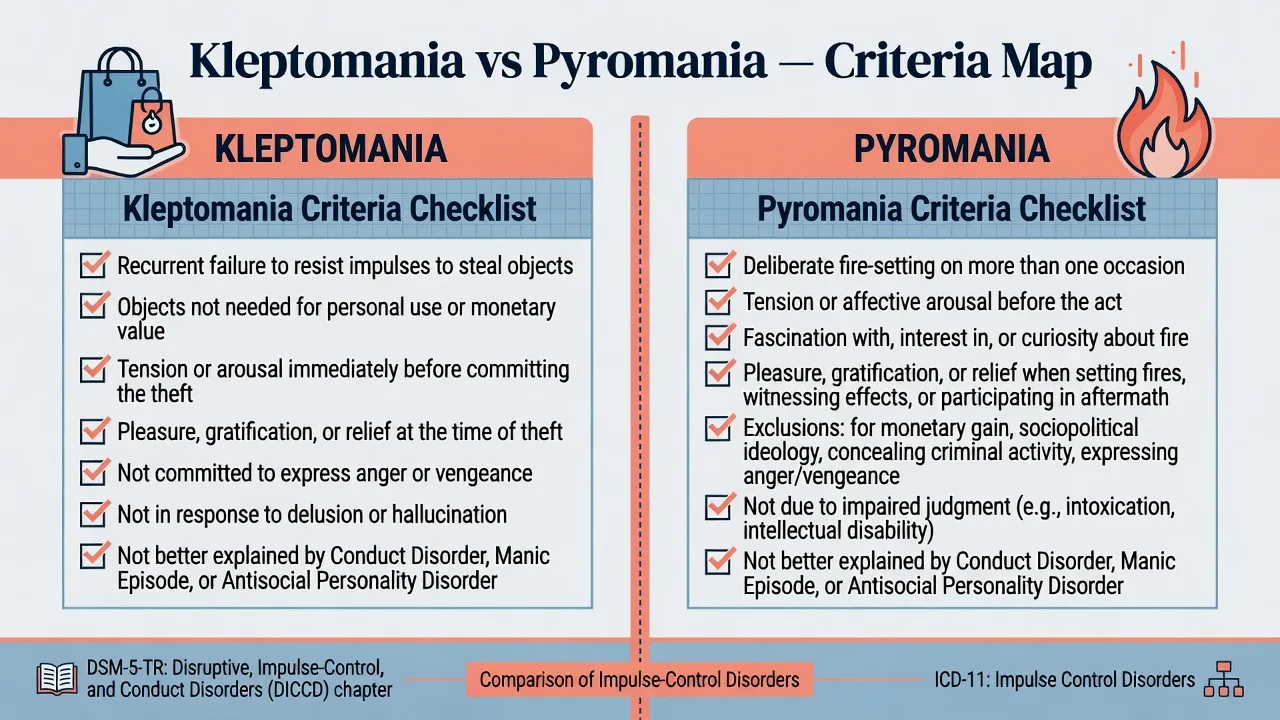
Kleptomania is recurrent failure to resist impulses to steal objects that are not needed for personal use or for their monetary value, with increasing sense of tension immediately before committing the theft and pleasure, gratification, or relief at the time of committing the theft. The stealing is not committed to express anger or vengeance and is not in response to a delusion or a hallucination; it is not better explained by conduct disorder, a manic episode, or antisocial personality disorder.[3][4][8]
Pyromania is deliberate and purposeful fire-setting on more than one occasion, tension or affective arousal before the act, fascination with, interest in, curiosity about, or attraction to fire and its situational contexts, and pleasure, gratification, or relief when setting fires, witnessing their effects, or participating in their aftermath. Fire-setting is not done for monetary gain, as an expression of sociopolitical ideology, to conceal criminal activity, to express anger or vengeance, or in response to delusion/hallucination, and is not better explained by impaired judgment (for example intoxication, neurocognitive disorder, intellectual disability) or by conduct disorder, mania, or ASPD.[2][11]
Clinical essence for viva. Both are disorders of irresistible impulse with tension-relief phenomenology, not moral labels and not synonyms for “any thief” or “any arsonist.” Between acts the person may function, conceal, or present only for depression/anxiety. Guilt and shame after acts are common but not pathognomonic of safety.[3][4][14]
DSM-5-TR placement. Both sit in Disruptive, Impulse-Control, and Conduct Disorders alongside ODD, IED, CD, and related categories. ICD-11 frames them among impulse control disorders. State which manual you are using when coding or defending thresholds.[7][8]
Terminology trap (forensic gold). Fire-setting is the behaviour; arson is a legal charge; pyromania is a rare psychiatric diagnosis. Confusing the three fails viva and court credibility.[11]
Classification and criterion map
Kleptomania core
- Irresistible impulse to steal
- Objects not needed for use/value
- Tension before; pleasure/relief at theft
- Not anger, delusion, CD/mania/ASPD
Pyromania core
- Deliberate fires more than once
- Tension/arousal before act
- Fascination with fire and contexts
- Pleasure/relief at setting or aftermath
Shared ICD features
- Urge–act–aftermath cycle
- Distress, impairment, or legal cost
- High psychiatric comorbidity
- DSM-5-TR DICCD / ICD-11 impulse control
Hard exclusions
- Need-based or profit theft
- Revenge/fraud/protest arson
- Mania or psychosis-driven acts
- Substance-only or CD/ASPD pattern alone
Conceptual models place kleptomania on an impulsive–compulsive spectrum with possible OCD-like, addictive, and affective subtypes — useful for formulation, not a substitute for operational criteria.[14][8]
Epidemiology and risk factors
Headline epidemiology (exam numbers)
Community prevalence of kleptomania is low; teaching figures in the region of 0.3–0.6% are widely quoted, with higher rates among some shoplifting samples and structured college screening detecting a small percentage meeting criteria.[7][8][10] Clinical series (McElroy; Grant) show female predominance, adolescent or early-adult onset for many, frequent prior apprehension, and substantial mood and substance comorbidity; stolen items are often hoarded, discarded, gifted, or returned rather than used for need.[3][4][6]
Pyromania is rare in general samples. Clinical series document heavy psychiatric comorbidity rather than pure isolated “fire fascination,” and forensic teaching emphasises that the large majority of arson cases fail pyromania criteria once motives and exclusions are applied.[2][11] Systematic screening of adult psychiatric inpatients finds impulse-control problems more often than unaided detection implies — ask, do not wait for confession.[9][12]
Pathophysiology and maintaining model
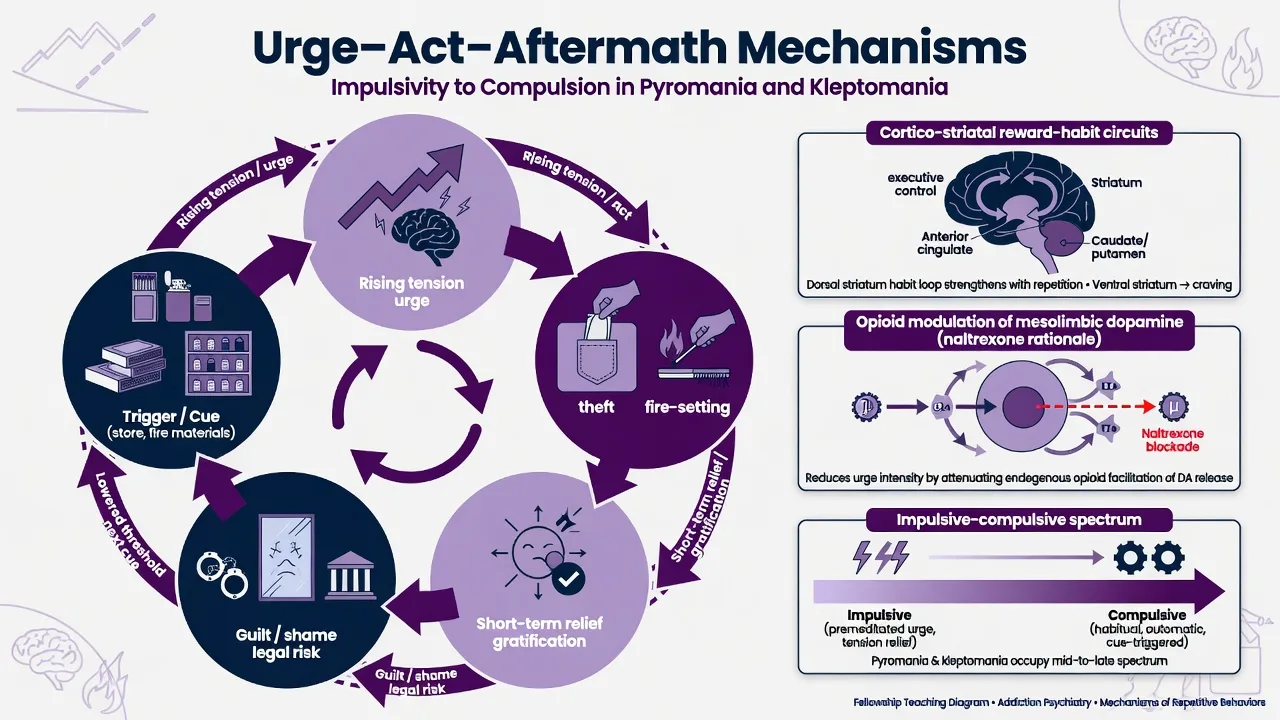
Behavioural cycle. Cue (retail environment; matches/accelerants/fire interest contexts) → rising tension/urge → act → short-term relief or thrill → guilt, shame, and legal threat → lowered threshold for the next cue. Treatment targets cue control, urge tolerance, and aftermath meaning-making — not moral lectures alone.[8][14]
Neurobiological teaching frame. Cortico-striatal reward and habit circuits and opioid modulation of mesolimbic dopamine provide a coherent rationale for testing opioid antagonists in urge-driven stealing; they are not diagnostic tests.[1][8][14] Mood and serotonergic comorbidity pathways explain historical SSRI interest; RCT maintenance data temper enthusiasm.[5][7]
Clinical presentation
Kleptomania. Rising tension in shops or other opportunities; stealing of small, redundant, or unneeded items; relief during or immediately after the act; later guilt and concealment; sometimes returning goods or self-punishing behaviour. Help-seeking is often delayed until legal crisis or comorbid depression surfaces.[3][4][6]
Pyromania. Deliberate fires for tension relief and fascination; interest in fire paraphernalia, fire services, or watching aftermath; repeated episodes. Instrumental motives (money, revenge, protest, hiding evidence) argue against the diagnosis.[2][11]
MSE language. Reality testing usually intact absent comorbidity; thought form intact; insight into harmfulness variable; urge intensity and ability to delay should be documented; risk domains include legal exposure, public fire safety, secondary victims, and suicide after shame or arrest.[2][4][11]
Differential diagnosis
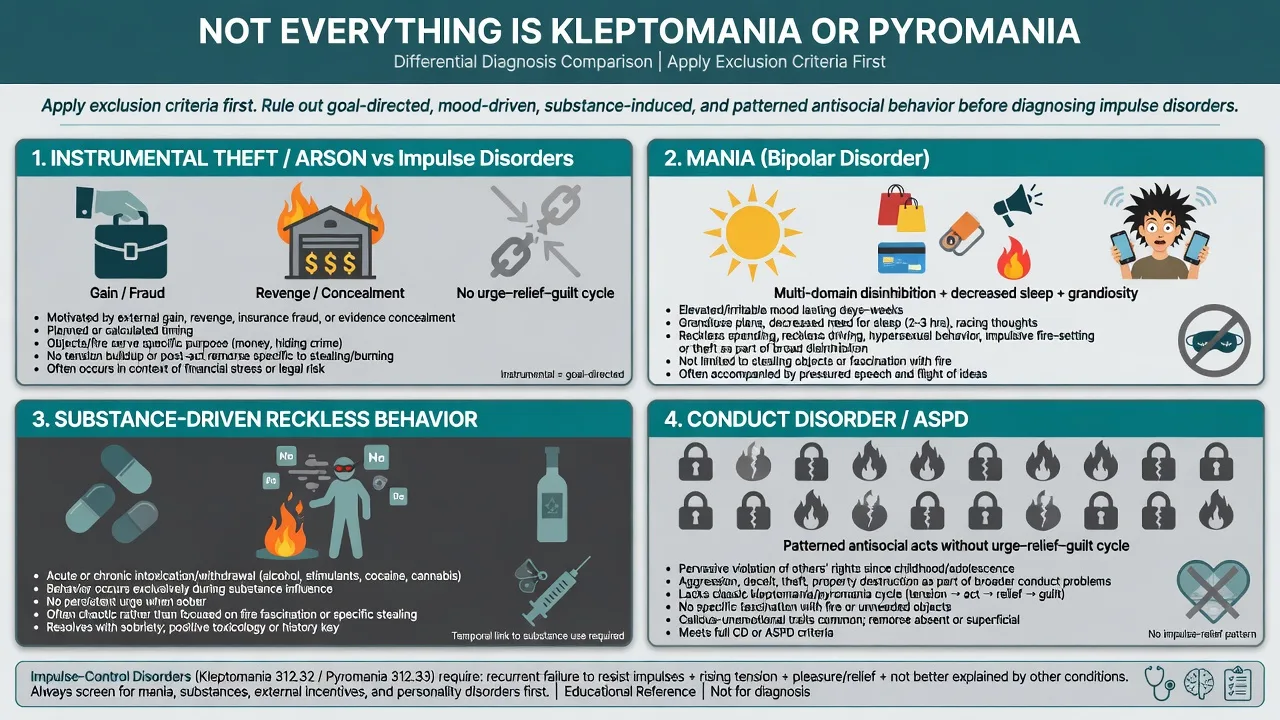
Instrumental crime
- Need, profit, revenge, fraud, concealment
- Planning and tangible objectives
- No classic unneeded-object or fire-fascination frame
- Legal formulation primary
Mania / mixed
- Days–weeks elevated/irritable mood
- Decreased need for sleep, grandiosity
- Multi-domain disinhibition
- Stabilise mood then reassess
Substance-driven
- Acts tightly linked to intoxication
- Assess sober-period urges separately
- Integrated dual-diagnosis care
- UDS and timeline critical
CD / ASPD
- Pervasive rights violation pattern
- Conduct history rules for ASPD
- Remorse may be shallow or absent
- Do not force rare ICD labels
Also exclude psychotic motives, organic frontal syndromes when onset is late or atypical, and dopamine-agonist-related impulsivity when PD/RLS drugs are present (more classically gambling/hypersexuality/shopping, but still reconciling medication effects matters).[7][8][11]
Assessment
Structure: (1) urge–act–aftermath narrative; (2) object value/need or fire motives and exclusions; (3) frequency, planning versus impulse, ability to delay; (4) substances and medications; (5) mood, psychosis, OCD spectrum, ADHD, trauma, personality; (6) legal chronology and current charges; (7) collateral (family, retailers, police, fire service); (8) suicide and public-safety risk; (9) capacity for justice processes.[4][9][11][12]
Tools. The Minnesota Impulse Disorders Interview (MIDI) is a validated structured clinical interview concept for systematic ICD enquiry — know the name even if your service uses local forms.[10][12]
Risk. Static factors (prior arrests, early onset, prior fire-setting, male sex for many arson samples) versus dynamic factors (acute grievance, substance use, access to accelerants, untreated depression, non-engagement) and protective factors (engagement, cue control, supports, supervised conditions). Structured professional judgement humility applies; tools do not perfectly predict individual acts.[2][11]
Investigations
Clinical diagnoses. Obtain UDS when substances may drive behaviour; baseline LFTs (and pregnancy test when relevant) before naltrexone; exclude current opioid use (precipitated withdrawal risk); metabolic panel and ECG if starting other psychotropics. Imaging or EEG only for neurological red flags (late abrupt onset, focal signs, cognitive decline, seizures).[1][8][13]
Acute / emergency management
There is no classic autonomic detox protocol for pure kleptomania or pyromania. Crisis care is risk containment, dual-diagnosis treatment, legal liaison, and safety planning — not “urge detox theatre.”[8][11]
Definitive management
Psychological therapy
CBT packages are first-line across both disorders in specialist teaching: psychoeducation, stimulus control (shopping plans, accompaniment, avoid high-risk aisles/times; fire-material access control), urge surfing, cognitive restructuring of justifications (“I deserve this,” “no one is hurt”), response prevention alternatives, emotional regulation, and relapse prevention. Motivational interviewing addresses ambivalence and shame without collusion. Family work must not create secrecy that endangers the public.[8][14]
Pharmacotherapy — kleptomania
There is no TGA/FDA-approved drug labelled specifically for kleptomania. The best-known randomised evidence is naltrexone: in an 8-week double-blind placebo-controlled trial, oral naltrexone reduced stealing urges and behaviour versus placebo in adults with kleptomania.[1] Earlier open-label work supported feasibility and symptomatic improvement signals.[13]
Practical fellowship regimen (individualise; off-label counselling mandatory): confirm no current opioid dependence or recent opioid use; obtain baseline LFTs and exclude acute hepatitis; discuss hepatotoxicity risk, pregnancy considerations, and that this is not a licensed indication. A common starting approach is naltrexone 50 mg orally daily, with clinical review of urges, stealing behaviour, adherence, and LFTs at follow-up (for example early review within 2–4 weeks and interval labs per local protocol), dose individualisation only under specialist supervision if higher trial-range doses are considered, and continuation only with clear benefit and ongoing psychosocial care. Do not use naltrexone as monotherapy without CBT/risk work.[1][8][13]
SSRI nuance (exam favourite). Escitalopram showed open-label improvement in some patients with kleptomania, but double-blind discontinuation failed to demonstrate maintenance superiority over placebo — do not overclaim SSRIs as proven disease-modifying monotherapy for the stealing drive itself; still treat comorbid depression/anxiety aggressively.[5][8]
Pharmacotherapy — pyromania
No medicine is labelled as disease-modifying for pyromania. Prioritise specialised behavioural programmes, individualised fire-safety planning, multi-agency liaison (mental health, fire service, police/probation as indicated), and treatment of mood, SUD, trauma, ADHD, or other drivers. Psychotropics target comorbidity, not a mythical “anti-fire receptor.”[2][11]
Comorbidity and social interventions
Mood disorders, SUD, other ICDs, and personality pathology often drive impairment more than the rare ICD label alone — integrated care beats sequential ping-pong.[2][4][6][9] Legal advocacy, vocational support, and realistic court-report language (base rates, exclusions, treatability limits) complete the plan.[11]
Subtypes and clinical scenarios
- Retail kleptomania with discarded/returned goods versus organised theft rings for gain.[3][4]
- Kleptomania + major depression or bipolar spectrum — treat the mood syndrome; reassess stealing when euthymic.[3][6]
- Kleptomania + SUD — dual formulation when sober-period urges persist.[6]
- Adolescent fire interest versus meeting full pyromania criteria after exclusions.[2][11]
- Forensic arson evaluation where pyromania is the uncommon answer.[11]
- Court-mandated “anger/theft programme” with mixed motives — clarify criteria honestly.[8][11]
Complications and pitfalls
Other pitfalls: pure moralising without CBT offer; missing mania; therapeutic nihilism; colluding with secrecy; labelling ASPD patterned theft as kleptomania without urge phenomenology.[8][11][14]
Prognosis and disposition
Course is often chronic-relapsing when cues and comorbidity persist; engagement, stimulus control, treated dual diagnosis, and legal stabilisation improve outlook; naltrexone responders in trial data show reduced urges and stealing behaviour over the study window.[1][4][8] Most care is outpatient specialist/shared care with a written risk plan. Step up to forensic pathways or inpatient care for uncontainable arson risk, severe dual diagnosis, or acute suicide risk — not for symbolic “urge detox.”[2][11]
Special populations
Adolescents. Prefer developmental CD/ODD frameworks first for patterned antisocial acts; family and school interventions; child protection when fire-setting endangers others.[7][11]
Women with kleptomania. Clinical series enrichment; shame barriers delay help; perinatal medication counselling if treating with naltrexone or psychotropics.[3][4]
Older adults. New theft or fire impulsivity triggers organic, mood, and medication review rather than de novo classic ICD assumptions.[8]
Intellectual disability. Capacity, positive behaviour support, and developmental context — avoid dumping all challenging behaviour into rare ICD labels.[11]
Forensic populations. Strict criteria, multi-agency risk, honest base rates that pyromania is uncommon among arson defendants.[11]
Evidence and regional notes
ANZ (FRANZCP / RANZCP context). No single RANZCP clinical practice guideline titled solely for kleptomania or pyromania. Apply DSM-5-TR criteria, structured risk assessment, dual-diagnosis competence, least-restrictive emergency care, child/family safeguarding, and explicit off-label pharmacotherapy counselling for naltrexone. Justice liaison and fire-service partnerships matter for arson risk.[1][8][11]
UK (MRCPsych / NICE-adjacent). Use ICD-11/DSM operational knowledge for Paper A/B; map management to violence/arson risk principles and common mental health psychosocial pathways rather than inventing a kleptomania-specific NICE CG number.[8][11]
US (ABPN / APA). DSM-5-TR criteria are primary; Grant naltrexone RCT and Koran escitalopram discontinuation design are high-yield evidence names; forensic firesetting reviews emphasise behaviour versus charge versus diagnosis.[1][5][11]
Landmark anchors: McElroy 1991 series, Grant 2002 characteristics, Grant 2009 naltrexone RCT, Koran 2007 escitalopram OL+DB discontinuation, Grant 2007 pyromania comorbidity, Odlaug/Grant college MIDI screen, Burton 2012 forensic firesetting review, Dell'Osso/Schreiber ICD reviews, MIDI validation.[1][2][3][4][5][7][8][10][11][12]
Exam pearls
- Most arson is not pyromania — exclusions first.[2][11]
- Naltrexone ~50 mg oral daily after LFTs and opioid check is the best-known RCT pharmacotherapy teaching point for kleptomania (off-label).[1]
- Escitalopram: open-label signal, failed double-blind discontinuation — know the nuance.[5]
- Urge–tension–relief cycle is the viva phenomenology language for both disorders.[8][14]
- Always assess self-harm/suicide after arrest and multi-agency public fire safety.[11]
- DSM-5-TR DICCD chapter; ICD-11 impulse control — name the manual.[7][8]
STEAL FIRE checklist
References
- [1]Grant JE, Kim SW, Odlaug BL A double-blind, placebo-controlled study of the opiate antagonist, naltrexone, in the treatment of kleptomania Biol Psychiatry, 2009.PMID 19217077
- [2]Grant JE, Won Kim S Clinical characteristics and psychiatric comorbidity of pyromania J Clin Psychiatry, 2007.PMID 18052565
- [3]McElroy SL, Pope HG Jr, Hudson JI, et al. Kleptomania: a report of 20 cases Am J Psychiatry, 1991.PMID 2018170
- [4]Grant JE, Kim SW Clinical characteristics and associated psychopathology of 22 patients with kleptomania Compr Psychiatry, 2002.PMID 12216013
- [5]Koran LM, Aboujaoude EN, Gamel NN Escitalopram treatment of kleptomania: an open-label trial followed by double-blind discontinuation J Clin Psychiatry, 2007.PMID 17388713
- [6]Grant JE, Odlaug BL, Kim SW Kleptomania: clinical characteristics and relationship to substance use disorders Am J Drug Alcohol Abuse, 2010.PMID 20575650
- [7]Dell'Osso B, Altamura AC, Allen A, Marazziti D, Hollander E Epidemiologic and clinical updates on impulse control disorders: a critical review Eur Arch Psychiatry Clin Neurosci, 2006.PMID 16960655
- [8]Schreiber L, Odlaug BL, Grant JE Impulse control disorders: updated review of clinical characteristics and pharmacological management Front Psychiatry, 2011.PMID 21556272
- [9]Grant JE, Levine L, Kim D, Potenza MN Impulse control disorders in adult psychiatric inpatients Am J Psychiatry, 2005.PMID 16263865
- [10]Odlaug BL, Grant JE Impulse-control disorders in a college sample: results from the self-administered Minnesota Impulse Disorders Interview (MIDI) Prim Care Companion J Clin Psychiatry, 2010.PMID 20694115
- [11]Burton PRS, McNiel DE, Binder RL Firesetting, arson, pyromania, and the forensic mental health expert J Am Acad Psychiatry Law, 2012.PMID 22960918
- [12]Chamberlain SR, Grant JE Minnesota Impulse Disorders Interview (MIDI): Validation of a structured diagnostic clinical interview for impulse control disorders Psychiatry Res, 2018.PMID 29772488
- [13]Grant JE, Kim SW An open-label study of naltrexone in the treatment of kleptomania J Clin Psychiatry, 2002.PMID 12000210
- [14]Grant JE Understanding and treating kleptomania: new models and new treatments Isr J Psychiatry Relat Sci, 2006.PMID 16910369