Psych · General adult psychiatry — mood disorders
Major depressive disorder
Also known as MDD · Unipolar depression · Clinical depression · Major depression · Depressive episode · Treatment-resistant depression · Psychotic depression · Melancholic depression
Exam-exhaustive fellowship reference on major depressive disorder — DSM-5-TR and ICD-11 criteria and specifiers; epidemiology and suicide risk; monoamine and circuit models; differentials including bipolar and medical mimics; PHQ-9 and HAM-D in measurement-based care; STAR*D, antidepressant NMA, psychotherapy and ECT evidence; stepped care (RANZCP/NICE/APA/CANMAT); special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Major depressive disorder (MDD) is the high-volume backbone of general adult psychiatry examinations. A FRANZCP MEQ will demand a structured assessment, bipolar screen, named drug with dose and monitoring, and a safety plan. An MRCPsych CASC will test risk communication and explanation of antidepressants to a patient or relative. An ABPN item will test STAR*D stepwise logic, specifier definitions, and augmentation evidence. This topic is written so a candidate who has read nothing else can answer those questions at consultant depth.[1][6][17]
Overview and definition
MDD is a syndrome of persistent low mood and/or anhedonia plus a cluster of cognitive, neurovegetative and behavioural features lasting long enough and severe enough to impair function, after bipolar spectrum illness, substance effects and medical mimics have been reasonably excluded. It is not "feeling sad" and it is not diagnosed by a blood test. The modern exam stance is operational criteria plus formulation: criteria gate the diagnosis; formulation explains vulnerability, precipitants, maintaining factors and the recovery plan.[9][17]
DSM-5-TR structure you must reproduce. Criterion A requires five or more symptoms present during the same 2-week period, representing a change from previous functioning; at least one symptom is either depressed mood or markedly diminished interest or pleasure. The remaining list: significant weight or appetite change; insomnia or hypersomnia; psychomotor agitation or retardation (observable); fatigue or loss of energy; worthlessness or excessive guilt; diminished concentration or indecisiveness; recurrent thoughts of death, suicidal ideation, or suicide attempt/plan. Symptoms cause clinically significant distress or impairment. The episode is not attributable to a substance or another medical condition, and is not better explained by a schizophrenia-spectrum or other psychotic disorder. There has never been a manic or hypomanic episode (or such episodes were substance-induced or secondary to medical illness). [17]
ICD-11. Depressive episode and depressive disorder use a similar symptom menu with severity grading and course descriptors. Duration is typically at least 2 weeks for a depressive episode. State which manual you are using when duration or specifier language is examined. [17]
Classification and specifiers
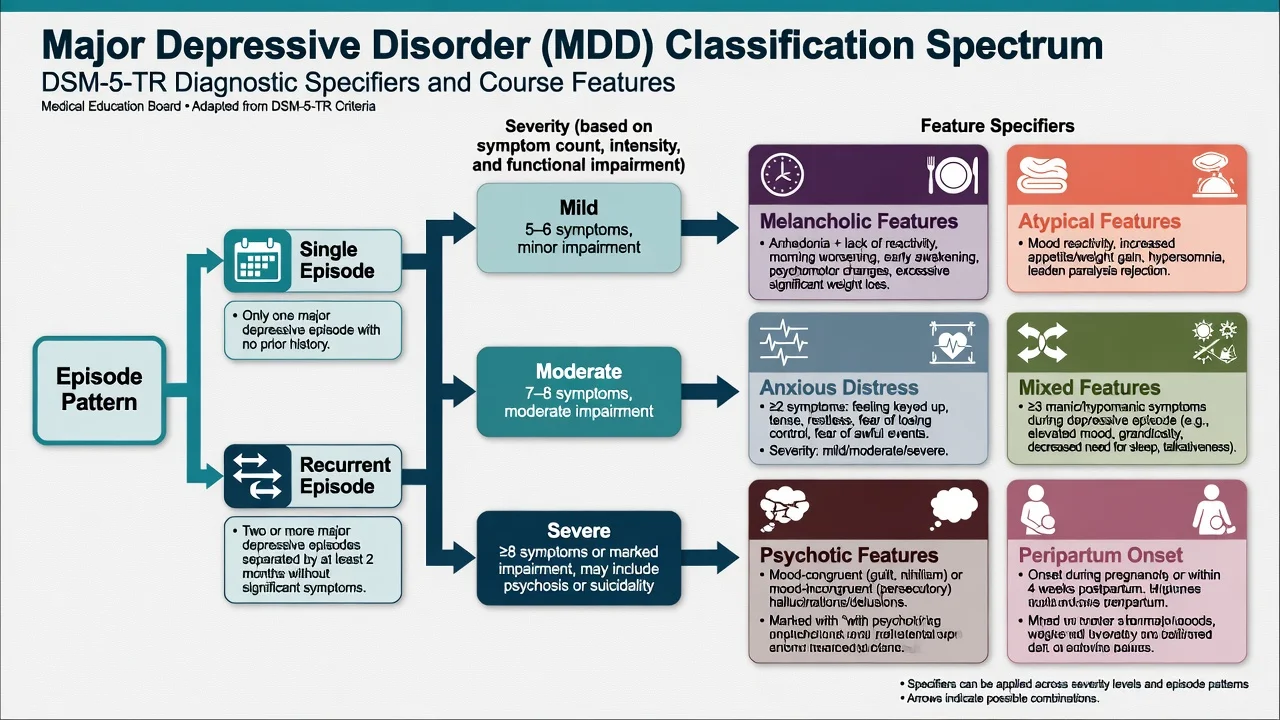
Severity
- Mild: fewer symptoms, manageable distress, limited functional loss
- Moderate: between mild and severe
- Severe: most symptoms, marked impairment; may include psychosis or high suicide risk
- Severity guides intensity of care and ECT consideration
Course
- Single episode vs recurrent (two or more episodes)
- Partial vs full remission
- Persistent depressive disorder if chronic low-grade depression for years (dysthymia pathway)
- Residual symptoms drive relapse risk
Feature specifiers
- Anxious distress, mixed features, melancholic, atypical
- Psychotic features (mood-congruent or incongruent)
- Catatonia, peripartum onset, seasonal pattern
- Mixed features flag bipolar spectrum risk
Related diagnoses
- Persistent depressive disorder (dysthymia)
- Premenstrual dysphoric disorder
- Substance/medication-induced depressive disorder
- Depressive disorder due to another medical condition
Specifiers and related diagnoses sit on separate axes from severity and course.[17]
Melancholic features. Near-complete anhedonia or lack of reactivity, plus features such as distinct quality of mood, morning worsening, early-morning awakening, marked psychomotor change, significant anorexia or weight loss, and excessive guilt. Melancholia often responds well to biological treatments including ECT.[8][17]
Atypical features. Mood reactivity plus two or more of: significant weight gain or increased appetite, hypersomnia, leaden paralysis, long-standing interpersonal rejection sensitivity. Historically linked to monoamine oxidase inhibitor (MAOI) responsiveness in classic teaching; modern practice still uses the specifier for formulation and sometimes treatment choice.[16]
Psychotic features. Delusions or hallucinations during the episode; often mood-congruent (guilt, nihilism, deserved punishment) but mood-incongruent psychosis still occurs. Management is not "SSRI alone."[17]
Mixed features. Manic/hypomanic symptoms during a major depressive episode without meeting full mania criteria — a critical discriminator that changes the pharmacological plan and bipolar risk framing.[17]
Epidemiology and risk factors
Headline numbers every candidate must own
The National Comorbidity Survey Replication estimated substantial 12-month and lifetime prevalence of MDD in US adults, with earlier onset cohorts accumulating higher lifetime risk and with treatment contact often delayed after first onset.[9]
Risk factors include family history of mood disorder, early adversity and trauma, chronic medical illness, substance use, major life events, loneliness and social defeat, and prior depressive episodes. Female sex associates with higher community prevalence; male sex associates with higher completed suicide rates in many jurisdictions — both statements can be true simultaneously.[9][17]
Pathophysiology
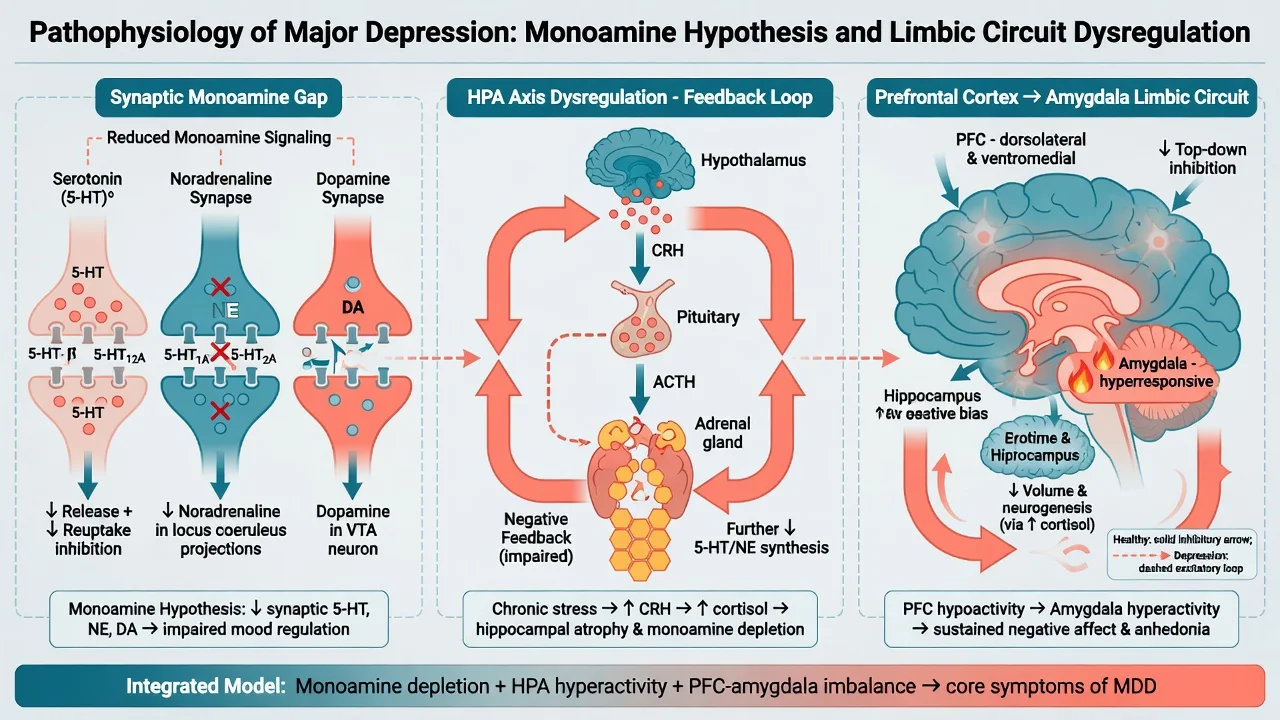
Monoamine hypothesis (working clinical model). Reduced synaptic availability or altered signalling of serotonin (5-HT), noradrenaline and/or dopamine contributes to mood, drive, sleep and appetite dysregulation. SSRIs, SNRIs, TCAs and MAOIs act primarily here. Limits you must state: delayed clinical response despite rapid reuptake blockade; incomplete response rates; and the fact that monoamines are necessary but not sufficient to explain the syndrome.[6][16]
HPA axis and stress biology. Chronic stress can dysregulate CRH–ACTH–cortisol feedback, with downstream effects on hippocampus, sleep and monoamine systems. Useful for viva framing of severe melancholia and medical comorbidity — not for ordering a diagnostic cortisol test on every patient.[17]
Circuit model. Prefrontal under-engagement and limbic (including amygdala) over-reactivity is a group-level research framing for negative bias, rumination and anhedonia. Imaging is not an individual diagnostic test for MDD.[17]
Glutamate / NMDA. Subanaesthetic ketamine produces rapid antidepressant effects in treatment-resistant major depression, supporting glutamatergic and synaptic plasticity models beyond classical monoamines.[12]
Psychological models that change treatment. Cognitive triad (self, world, future), behavioural inactivation, and interpersonal role disputes map directly onto CBT, behavioural activation and IPT respectively.[18][20]
Clinical presentation
Core features: depressed mood; anhedonia; guilt/worthlessness; impaired concentration; psychomotor change; sleep and appetite disruption; fatigue; suicidal ideation. Tempo is usually days to weeks for a discrete episode, though prodromal dysphoria may be longer. Quote the patient's words in the MSE (e.g. "I am a burden"; "nothing gives pleasure").[10][17]
Atypical presentations examiners test. Late-life depression may present with apathy, cognitive complaints ("pseudodementia" language is outdated — assess both depression and cognition), and somatisation. Adolescents may show irritability more than sad mood. Cultural idioms may emphasise bodily pain, heat, or spirit rather than "depression." Somatic presentations in primary care are common — screen actively.[9][17]
Psychotic and catatonic depression. Nihilistic delusions, deserved punishment, auditory hallucinations with depressive content, refusal of food, and catatonic signs escalate urgency and often favour ECT.[8]
Differential diagnosis
Bipolar depression
- Prior mania/hypomania is decisive when present
- Family history of bipolar; postpartum mania; early onset
- Mixed features, highly recurrent course, antidepressant switching
- Treat as bipolar spectrum — not unipolar monotherapy
Grief / adjustment
- Grief: waves of yearning, preserved self-worth often, tied to loss
- MDD: pervasive anhedonia, worthlessness, functional collapse
- Adjustment: identifiable stressor, milder threshold, time-limited
- Do not force a false dichotomy — grief can co-occur with MDD
Substance / medication
- Alcohol, cannabis, stimulants, sedatives
- Steroids, interferon, isotretinoin, some antihypertensives
- Timeline locked to exposure strengthens attribution
- Treat substance and mood in parallel
Medical / organic
- Hypothyroidism, B12 deficiency, anaemia, OSA
- Neurological disease, stroke, Parkinson disease
- Delirium with dysphoria — attention and fluctuation
- Late first episode or focal signs → investigate
Also keep primary anxiety disorders with secondary demoralisation, ADHD with chronic underachievement, personality (borderline affective instability), and schizophrenia with depressive features on the board. [17]
Clinical and bedside assessment
Structure the interview: episode chronology; prior episodes and treatment adequacy (drug, dose, duration, adherence, response); bipolar screen (elated/irritable periods, reduced sleep need, grandiosity, risky behaviour); substance use; trauma; medical and medication history; perinatal status; family history; function and supports.[2][17]
Document a full Mental State Examination. Risk is mandatory: ideation, intent, plan, means, prior attempts, hopelessness, protective factors, command content if psychotic, access to firearms/medications, dependents. Capacity is decision-specific. Involuntary care uses local Mental Health Act principles — least restrictive, statute-bound; do not invent section numbers for the wrong jurisdiction.[17]
Investigations and measurement-based care
Baseline before antidepressants (typical adult set). TSH; full blood count; urea and electrolytes; liver function; consider glucose/lipids and BMI (especially if using mirtazapine, quetiapine or other metabolic agents); ECG when cardiac risk, older age, TCA planned, or high-dose citalopram/escitalopram; pregnancy test when relevant; B12/folate if indicated; urine drug screen when substance contribution is plausible. Neuroimaging when late first onset, focal neurology or cognitive red flags fire — not routinely for every young adult with classic MDD.[16][17]
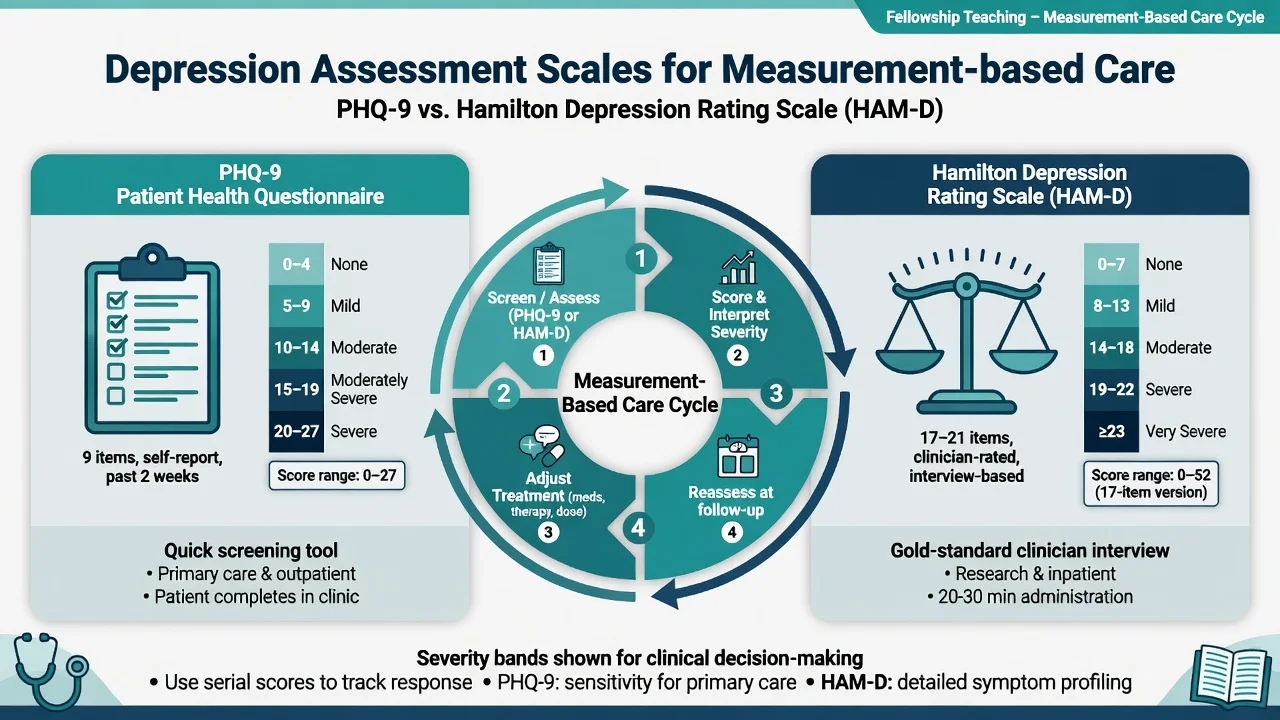
PHQ-9. Nine self-report items aligned to DSM symptom domains over the past 2 weeks; score range 0–27. Common severity bands used in practice: 0–4 none/minimal; 5–9 mild; 10–14 moderate; 15–19 moderately severe; 20–27 severe. Item 9 screens suicidal thoughts but is not a complete risk assessment.[10]
HAM-D (HDRS). Clinician-rated scale (classic 17-item version widely used in trials); foundational severity instrument in research.[11]
Measurement-based care. STAR*D used systematic measurement and dose adjustment; serial PHQ-9 or equivalent plus side-effect review is now expected practice, not optional paperwork.[2]
Management — acute risk and resuscitation
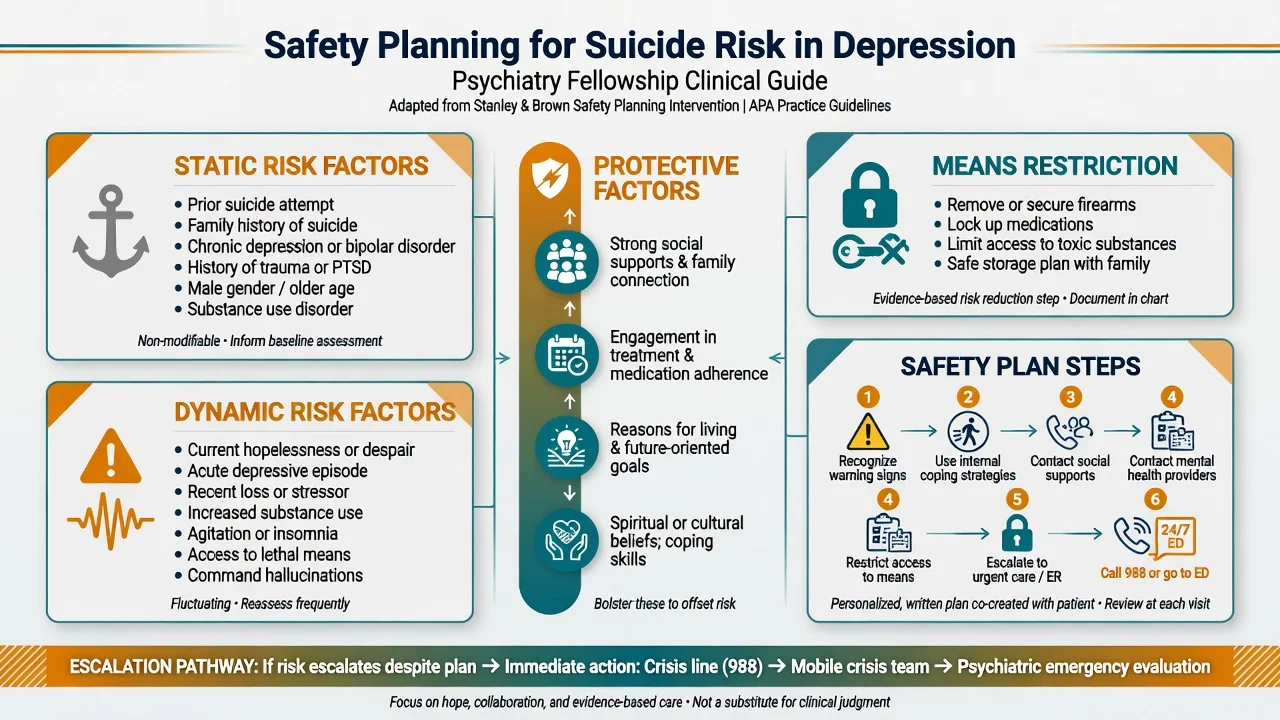
Safety planning (collaborative). Warning signs; internal coping; social contacts; professional contacts; means restriction; reasons for living. Reassess after starting antidepressants, after relationship rupture, substance relapse, or discharge.[17]
Medical emergencies of treatment. Serotonin syndrome (stop serotonergic agents; supportive care; cyproheptadine in selected protocols under medical care); TCA overdose (sodium bicarbonate for wide-complex arrhythmia; critical care); SSRI-related symptomatic hyponatraemia in the elderly (stop agent; fluid management). [16]
Management — definitive and stepwise
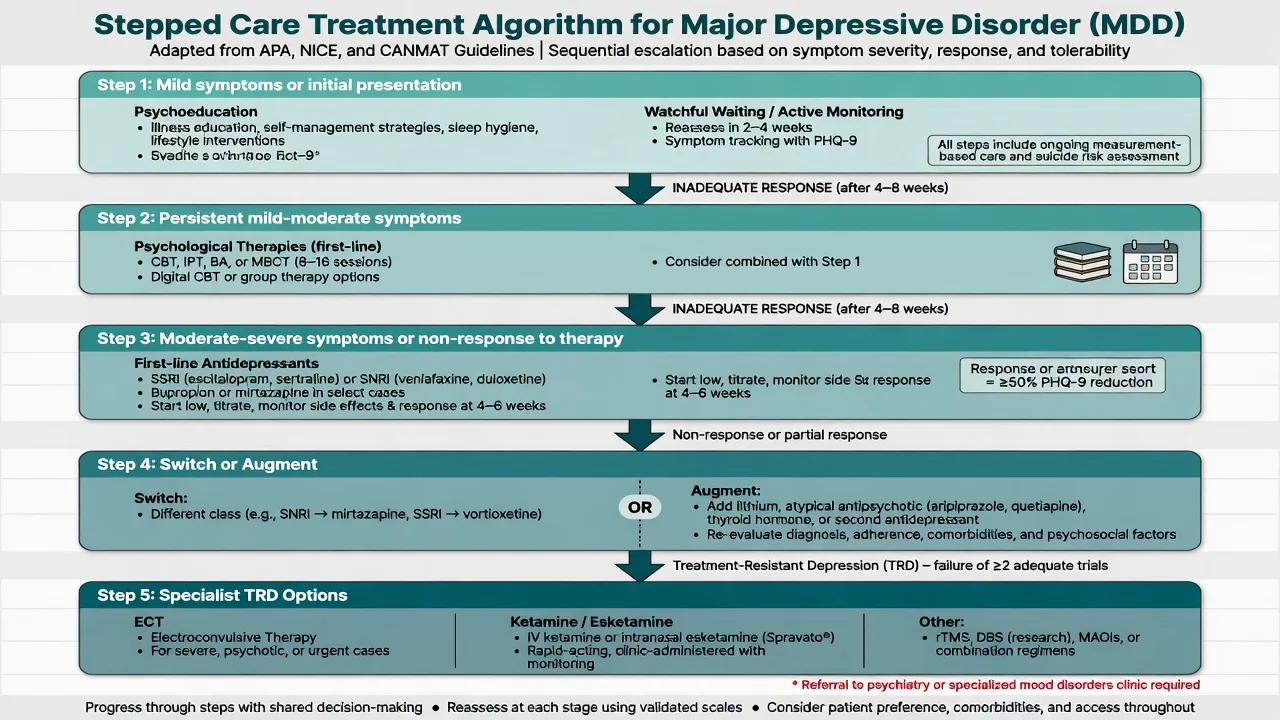
Stepped care principles
Match intensity to severity, risk and preference. Mild depression may start with psychoeducation, structured self-help, behavioural activation or brief psychological therapy with active monitoring. Moderate-to-severe depression typically warrants a formal evidence-based psychotherapy and/or antidepressant, often in combination when severity or chronicity is high. Specialist escalation is for high risk, psychosis, catatonia, diagnostic complexity, or non-response.[16][17][18]
RANZCP mood disorder guidelines emphasise formulation-driven care, careful bipolar exclusion, shared decision-making, and staged pharmacological and psychological treatment within Australian and New Zealand service models.[17]
First-line antidepressants — agent, dose, monitoring
Doses below are typical adult oral starting and common therapeutic ranges used in exam answers; always individualise for age, hepatic/renal function, interactions and pregnancy. Cite local product information for legal prescribing.[6][16]
| Agent (class) | Typical start | Common therapeutic range | Key monitoring / notes |
|---|---|---|---|
| Sertraline (SSRI) | 50 mg daily | 50–200 mg daily | Sexual dysfunction, GI effects; relatively favourable in cardiac and perinatal discussions |
| Escitalopram (SSRI) | 10 mg daily | 10–20 mg daily | QTc caution at higher doses; hyponatraemia in elderly |
| Citalopram (SSRI) | 20 mg daily | 20–40 mg daily (lower max in elderly) | QTc dose ceiling; measurement-based care exemplar in STAR*D |
| Fluoxetine (SSRI) | 20 mg daily | 20–60 mg daily | Long half-life; activating; TADS adolescent evidence |
| Venlafaxine XR (SNRI) | 75 mg daily | 75–225 mg daily | BP monitoring; discontinuation symptoms; noradrenergic at higher doses |
| Duloxetine (SNRI) | 30–60 mg daily | 60–120 mg daily | Pain comorbidity; LFTs; avoid in significant liver disease |
| Mirtazapine | 15 mg at night | 15–45 mg at night | Sedation, weight gain; useful if insomnia/anorexia |
| Bupropion XL (NDRI; availability varies) | 150 mg daily | 150–300 mg daily | Seizure risk (contraindications); less sexual dysfunction; not for bulimia/anorexia |
| Typical adult ranges for exam use; individualise and check local product information.[16][6] |
Adequate trial definition (exam mantra). Right drug, therapeutic dose, about 4–6 weeks at that dose (longer if partial slow response), verified adherence, addressed substance use and psychotherapy access, before declaring failure.[2][16]
STAR*D — the numbers examiners want
STAR*D was a large, real-world sequential treatment programme in outpatients with MDD using measurement-based care.[1][2]
- Level 1 (citalopram): roughly one-third remitted with first-line SSRI under measurement-based care.[2]
- Level 2 switch (e.g. bupropion-SR, sertraline, or venlafaxine-XR after SSRI failure): similar remission rates across switch options in the published comparison — choice is guided by side-effect profile and residual symptoms more than a single "best" switch agent.[3]
- Augmentation options later in the algorithm included lithium or T3 after two failed medication steps, with clinically meaningful though limited absolute remission rates.[4]
- Level 4 compared tranylcypromine versus venlafaxine plus mirtazapine after three failed trials — both difficult, modest remission, high intolerance risk for MAOI pathway.[5]
- Cumulative lesson: remission probability falls with each failed step; residual symptoms are common; measurement and sequential planning beat random polypharmacy.[1]
Switch vs augment
After non-response: confirm diagnosis (especially bipolarity), adherence, dose, substance use, and psychotherapy engagement. Switch within or across class when intolerance or zero response. Augment when partial response is present and tolerability allows. Evidence-based augmenters include lithium, T3, and atypical antipsychotics (e.g. aripiprazole, quetiapine XR, olanzapine–fluoxetine in selected protocols) with metabolic and EPS/akathisia monitoring.[4][16][19]
Example augmentation doses (adult, exam-level). Aripiprazole often start 2–5 mg orally daily, titrate toward 5–15 mg as tolerated; quetiapine XR often 50 mg at night building toward 150–300 mg for augmentation ranges used in trials/guidelines — always monitor weight, glucose, lipids, sedation and QTc risk context.[16][19]
Psychotherapy evidence
CBT and interpersonal psychotherapy (IPT) have robust efficacy; behavioural activation is efficient and scalable; multiple bona fide psychotherapies show benefit in network meta-analysis, with differences often modest once effective therapies are compared.[18] CBT can match medication in moderate-to-severe depression in skilled delivery settings, and combination treatment is often preferred when severity, chronicity or preference supports it.[20] Mindfulness-based cognitive therapy is particularly discussed for relapse prevention in recurrent depression.[18]
Maintenance and relapse prevention
Continuing antidepressant after remission reduces relapse substantially versus stop — classic meta-analytic framing from Geddes and colleagues remains a cornerstone teaching point.[7] Practical rule of thumb used in guidelines: continue at least 6–12 months after first-episode remission; longer (2 years or indefinite) after recurrent, severe, or highly impairing illness, individualised with the patient.[7][16][17]
ECT pathway
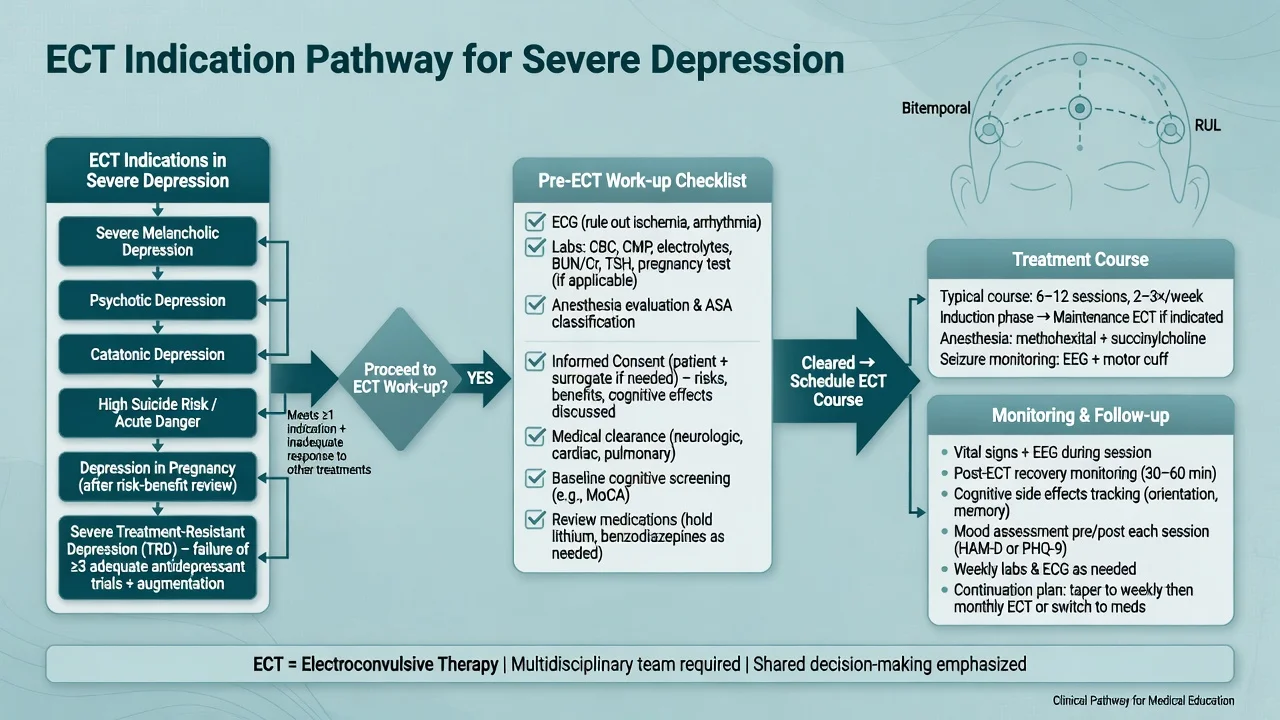
ECT has the strongest short-term efficacy signal among somatic treatments for severe depressive disorders in systematic review.[8] Indications examiners expect: severe melancholic or psychotic depression; catatonia; urgent high suicide risk; poor oral intake; prior excellent ECT response; pregnancy with severe depression when risks favour ECT; and treatment resistance after adequate trials. Work-up includes consent, medical and anaesthetic review, ECG and labs as indicated, medication review (e.g. lithium, anticonvulsants, benzodiazepines), and cognitive baseline. Typical acute course is multiple sessions over weeks with electrode placement (right unilateral vs bitemporal) balancing efficacy and cognitive adverse effects.[8][17]
Ketamine and esketamine (TRD pointer)
Subanaesthetic ketamine showed rapid antidepressant effects in treatment-resistant major depression in a landmark RCT.[12] Intranasal esketamine combined with a newly initiated oral antidepressant improved outcomes in TRD and has relapse-prevention data when continued with oral antidepressant in responders.[13][14] These sit in specialist pathways with monitoring for dissociation, BP, misuse potential and access constraints — see the dedicated treatment-resistant depression topic for full algorithms.[13]
Specific subtypes and scenarios
Psychotic depression. Antidepressant plus antipsychotic, or ECT as a primary option depending on severity and speed required.[8][17]
Seasonal pattern. Recurrent seasonal onset/remission; light therapy is a guideline-supported option in appropriate patients alongside standard care.[16]
Perinatal (brief — pointer). Screen in pregnancy and postpartum; untreated depression harms parent and infant; sertraline is commonly discussed as a first-line pharmacological option when medication is needed; psychotherapy should be offered; escalate urgently for postpartum psychosis differential. Full detail belongs in perinatal psychiatry.[17]
Adolescents. TADS found fluoxetine and especially combination fluoxetine plus CBT superior to placebo for adolescent depression; CBT alone was less effective than fluoxetine on primary endpoints in the acute phase of that trial.[15] Monitor activation and suicidality closely after starting SSRIs; involve family; use developmentally adapted therapy.[15]
Late-life. Medical comorbidity, polypharmacy, hyponatraemia, falls, and cognitive overlap dominate. "Start low, go slow" with SSRIs often preferred over TCAs; ECT remains highly effective in severe late-life depression.[8][17]
Complications and pitfalls
Common traps: diagnosing unipolar MDD without bipolar screen; calling treatment failure after days; ignoring sexual side-effects that drive covert non-adherence; missing SSRI hyponatraemia; combining multiple serotonergic agents carelessly; treating akathisia as anxiety with more SSRI; discontinuing antidepressants abruptly (flu-like discontinuation syndrome, especially short half-life agents).[16][17]
Prognosis and disposition
Most episodes remit with treatment, but residual symptoms and recurrence are common — especially after multiple prior episodes.[1][7] Disposition ladder: primary care with collaborative care; secondary community mental health; intensive community/crisis; day programmes; voluntary inpatient; involuntary inpatient when risk and capacity thresholds are met under local law. Functional recovery (work, relationships, self-care) is the outcome that matters beyond a PHQ-9 score alone.[17]
Special populations
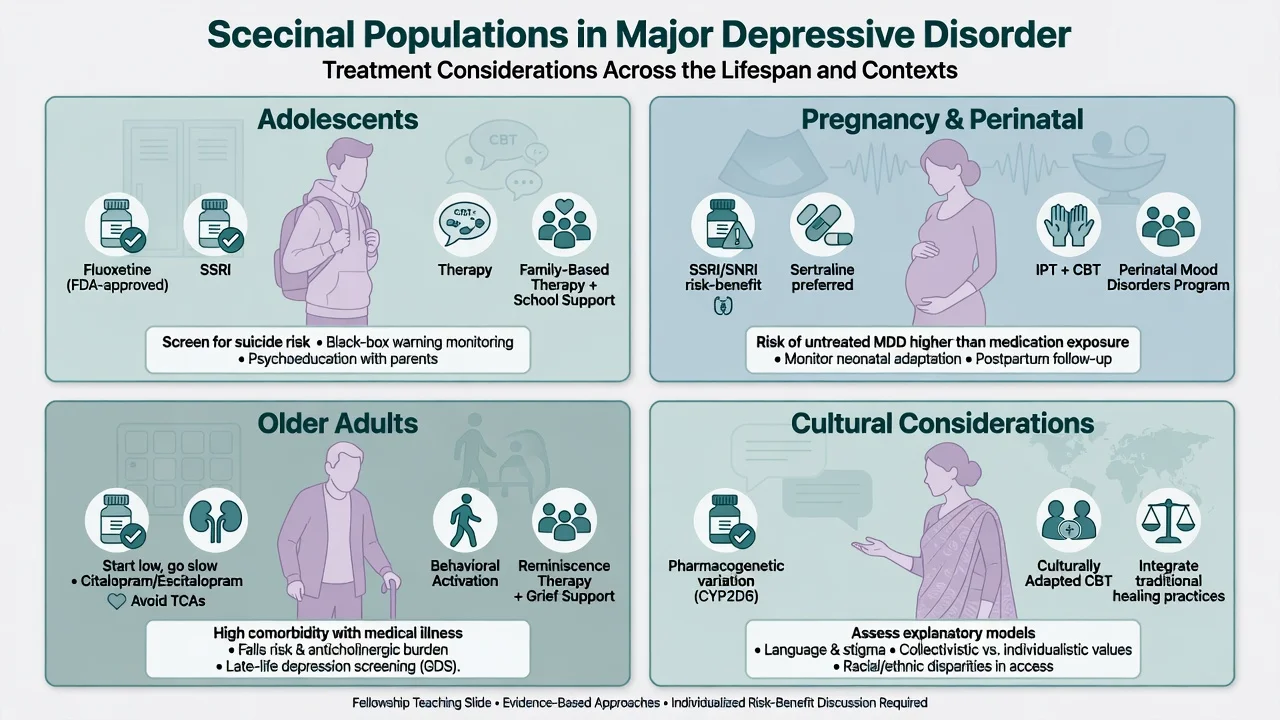
Adolescents
- Family involvement and school function
- Fluoxetine best-studied SSRI (TADS)
- Activation and suicidality monitoring
- Therapy access is non-optional ideal
Perinatal
- Risk of untreated MDD is not zero-harm
- Prefer agents with more reproductive data (e.g. sertraline)
- Screen partner/supports; infant bonding
- Urgent pathway if psychosis or high suicide risk
Older adults
- Medical work-up intensity higher
- Hyponatraemia, falls, QTc, interactions
- Avoid highly anticholinergic TCAs first-line
- ECT often excellent in severe illness
Cultural safety
- Explanatory models and stigma
- Interpreter use; family decision styles
- FRANZCP cultural safety expectations
- Do not pathologise culturally normative grief
Population-specific monitoring and first-line choices must be stated explicitly at viva.[15][17]
Evidence, guidelines and regional differences
Landmark pillars for exams: STAR*D sequential real-world remission and measurement-based care;[1][2] Cipriani 2018 network meta-analysis of 21 antidepressants (all more effective than placebo; differences in efficacy and acceptability are mostly modest — choose with tolerability and patient factors);[6] Geddes 2003 relapse prevention with continued antidepressants;[7] UK ECT Review Group 2003 efficacy of ECT;[8] Zarate ketamine and esketamine TRD programmes;[12][13][14] TADS adolescent treatment;[15] CANMAT 2016 pharmacological ranking;[16] RANZCP 2020 mood disorder guidelines;[17] psychotherapy network evidence and CBT–medication comparisons.[18][20]
Controversies to handle calmly at viva: antidepressant effect sizes in mild depression; long-term maintenance vs deprescribing; early use of ketamine/esketamine versus traditional augmentation; and the ethics of involuntary treatment for high-risk depression.[12][17]
Exam pearls
SIGECAPS
SIGECAPS is a memory scaffold for Criterion A domains — still apply full operational criteria and exclusions.[17]
Self-test: what is an adequate antidepressant trial?
References
- [1]Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report Am J Psychiatry, 2006.PMID 17074942
- [2]Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice Am J Psychiatry, 2006.PMID 16390886
- [3]Rush AJ, Trivedi MH, Wisniewski SR, Stewart JW, Nierenberg AA, Thase ME, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression N Engl J Med, 2006.PMID 16554525
- [4]Nierenberg AA, Fava M, Trivedi MH, Wisniewski SR, Thase ME, McGrath PJ, et al. A comparison of lithium and T(3) augmentation following two failed medication treatments for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946176
- [5]McGrath PJ, Stewart JW, Fava M, Trivedi MH, Wisniewski SR, Nierenberg AA, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946177
- [6]Cipriani A, Furukawa TA, Salanti G, Chaimani A, Atkinson LZ, Ogawa Y, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis Lancet, 2018.PMID 29477251
- [7]Geddes JR, Carney SM, Davies C, Furukawa TA, Kupfer DJ, Frank E, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review Lancet, 2003.PMID 12606176
- [8]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045
- [9]Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R) JAMA, 2003.PMID 12813115
- [10]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941
- [11]Hamilton M A rating scale for depression J Neurol Neurosurg Psychiatry, 1960.PMID 14399272
- [12]Zarate CA Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression Arch Gen Psychiatry, 2006.PMID 16894061
- [13]Popova V, Daly EJ, Trivedi M, Cooper K, Lane R, Lim P, et al. Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study Am J Psychiatry, 2019.PMID 31109201
- [14]Daly EJ, Trivedi MH, Janik A, Li H, Zhang Y, Li X, et al. Efficacy of Esketamine Nasal Spray Plus Oral Antidepressant Treatment for Relapse Prevention in Patients With Treatment-Resistant Depression: A Randomized Clinical Trial JAMA Psychiatry, 2019.PMID 31166571
- [15]March J, Silva S, Petrycki S, Curry J, Wells K, Fairbank J, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents With Depression Study (TADS) randomized controlled trial JAMA, 2004.PMID 15315995
- [16]Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [17]Malhi GS, Bell E, Bassett D, Boyce P, Bryant R, Hazell P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [18]Cuijpers P, Quero S, Noma H, Ciharova M, Miguel C, Karyotaki E, et al. Psychotherapies for depression: a network meta-analysis covering efficacy, acceptability and long-term outcomes of all main treatment types World Psychiatry, 2021.PMID 34002502
- [19]Nelson JC, Papakostas GI Atypical antipsychotic augmentation in major depressive disorder: a meta-analysis of placebo-controlled randomized trials Am J Psychiatry, 2009.PMID 19687129
- [20]DeRubeis RJ, Hollon SD, Amsterdam JD, Shelton RC, Young PR, Salomon RM, et al. Cognitive therapy vs medications in the treatment of moderate to severe depression Arch Gen Psychiatry, 2005.PMID 15809408