Psych · General adult psychiatry — mood disorders
Melancholic and atypical depression specifiers
Also known as Melancholic features · Atypical features · Melancholia · Atypical depression · Reverse vegetative depression · Endogenous depression · Depression with melancholic features · Depression with atypical features
Exam-exhaustive fellowship reference on DSM-5-TR melancholic features and atypical features as depressive episode specifiers — operational criteria, epidemiology, HPA and reverse-vegetative mechanisms, differentials, assessment, biological intensity including ECT and historical MAOI preferential response, psychotherapy, RANZCP/NICE/APA/CANMAT deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
These two specifiers are high-yield because they force operational criteria, vegetative polarity, and treatment-intensity thinking rather than vague "type of depression" folklore. FRANZCP MEQs reward exact criterion lists, ECT thresholds for melancholia, and MAOI safety when atypical pathways escalate. MRCPsych papers love reactivity versus nonreactivity and leaden paralysis. CASC stations often ask you to explain why one patient needs urgent inpatient/ECT discussion while another needs interpersonal work plus careful antidepressant choice.[4][6][10]
Definition and classification

Neither specifier is a freestanding DSM-5-TR disorder. Both attach to a full major depressive episode (or a depressive episode in bipolar disorder). You still document severity, course (single versus recurrent), and other applicable specifiers (psychotic features, seasonal pattern, peripartum onset, anxious distress, mixed features).[5][7][10]
Melancholic features (DSM-5-TR — reproduce for exams)
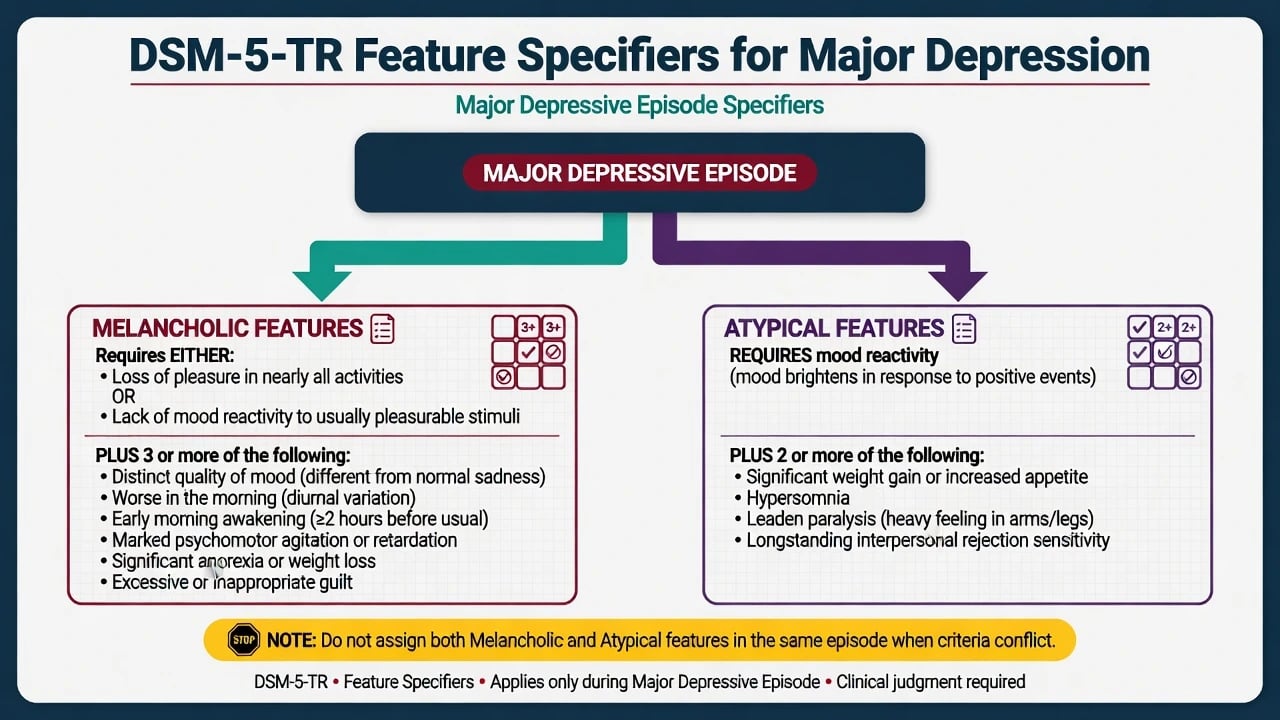
During the most severe period of the current episode, require either loss of pleasure in all or almost all activities or lack of reactivity to usually pleasurable stimuli (does not feel much better, even temporarily, when something good happens), plus three or more of: distinct quality of depressed mood (different from grief-like sadness); depression regularly worse in the morning; early-morning awakening (at least two hours before usual); marked psychomotor agitation or retardation; significant anorexia or weight loss; excessive or inappropriate guilt. Parker frames melancholia as a historically rich construct that DSM retains as a specifier rather than a separate coded disorder — know the operational list for scoring, and know the debate that melancholia may deserve stronger biological identity than a checkbox alone implies.[7][10]
Atypical features (DSM-5-TR — reproduce for exams)
Mood reactivity is mandatory (mood brightens in response to actual or potential positive events), plus two or more of: significant weight gain or increase in appetite; hypersomnia; leaden paralysis (heavy, leaden feelings in arms or legs); a long-standing pattern of interpersonal rejection sensitivity (not limited only to mood episodes) that results in significant social or occupational impairment. Criteria must predominate during the majority of days of the current or most recent major depressive episode (rejection sensitivity may be trait-like). Do not apply atypical features if the episode also meets melancholic features when the constructs conflict on reactivity — examiners treat simultaneous dual coding as a conceptual fail.[1][4][5]
ICD-11. Use depressive episode/disorder with symptom and course qualifiers rather than assuming DSM specifier names transfer unchanged. State which manual you are applying when asked "is this melancholia a diagnosis?" in viva.[10]
Historical language. "Endogenous depression," "vital depression," and "delusional melancholia" map imperfectly onto modern melancholic and psychotic-feature coding. "Atypical depression" in Columbia criteria historically emphasised mood reactivity and reverse vegetative signs with MAOI preferential response — the modern DSM atypical specifier is the descendant you must operationalise.[1][2][5]
Melancholic features
- Nonreactive mood / near-total anhedonia
- Early waking, anorexia, morning worsening
- Psychomotor change and excessive guilt
- Often higher biological intensity and ECT
Atypical features
- Mood reactivity required
- Hypersomnia, hyperphagia, leaden paralysis
- Rejection sensitivity (can be trait-like)
- Historical MAOI preferential response
Seasonal pattern
- Course specifier, not feature polarity
- Often winter reverse vegetative overlap
- Two-year seasonal rule
- Light therapy pathway separate
Psychotic features
- Delusions/hallucinations in MDE
- Common with severe melancholia
- Combination AD+AP or ECT
- Not the same as atypical
Epidemiology and risk
Numbers candidates should own
Population and clinical rates of atypical features vary with instrument and sample; reviews place substantial minorities of depressed patients in the atypical band in many outpatient settings, with lower pure rates in some research samples and higher rates when reverse vegetative symptoms are common.[5][6] Melancholic features concentrate in more severe, inpatient, older, and psychotic presentations. Female predominance and earlier onset are classic for atypical pathways; anxiety comorbidity and bipolar-spectrum risk also rise in the reverse vegetative and rejection-sensitivity phenotype.[4][6]
Base major depression epidemiology (NCS-R and related surveys) reminds candidates that depression is common and recurrent — specifier work sits on top of full episode diagnosis, not instead of it.[12]
Risk. Specifier labels do not imply mild illness. Severe melancholia carries high suicide and self-neglect risk; atypical presentations can be chronic, interpersonally destabilising, and still lethal. Risk assessment tracks intent, plan, means, protective factors, and previous attempts — not whether appetite went up or down.[10][12]
Pathophysiology and mechanisms
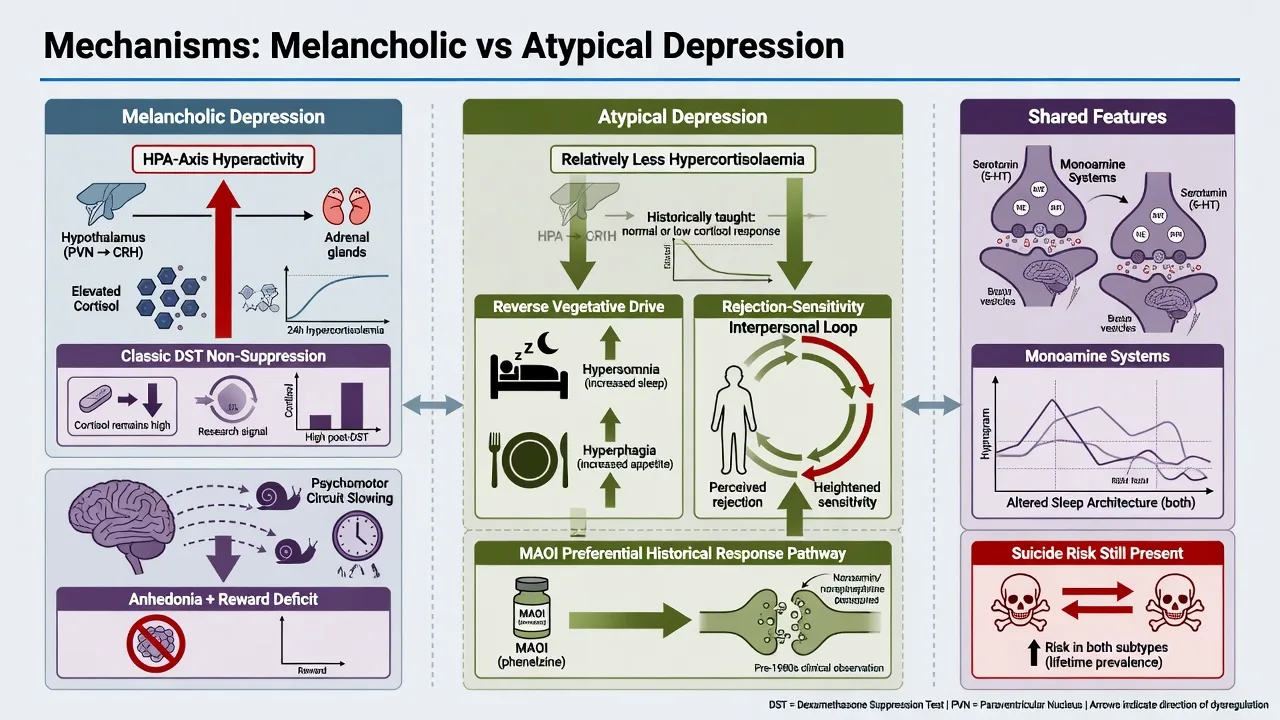
Melancholia — HPA and psychomotor biology. Melancholic presentations are more consistently linked in research to HPA-axis hyperactivity and cortisol dysregulation. Historical dexamethasone suppression test (DST) non-suppression literature is examinable as a research story, not as a test you order to "prove" melancholia in routine general adult practice.[7][8] Cortisol trajectory work has mapped onto melancholic symptoms and, in selected samples, ECT response — useful viva nuance without turning cortisol into a diagnostic gate.[8] Psychomotor retardation/agitation, early waking, and near-total anhedonia organise the clinical phenotype.
Atypical features — reverse vegetative and interpersonal biology. Classical teaching contrasts atypical depression with more hypercortisolaemic melancholia and notes preferential historical response to MAOIs versus TCAs in the Columbia programme — a treatment-response clue, not a pathognomonic biomarker.[1][2][4] Hypersomnia, hyperphagia, and leaden heaviness form the reverse vegetative cluster; rejection sensitivity maintains interpersonal crises that feed recurrent mood destabilisation.[4][6]
Shared monoamine framing. Both phenotypes remain within major depression biology; monoamine systems, sleep architecture, and reward circuits are relevant across the board. Do not invent a single neurotransmitter story that uniquely "explains" either specifier.[10][11]
Clinical presentation
Melancholia at the bedside. Near-total anhedonia, nonreactive affect, morning worsening, early waking, marked guilt, anorexia or weight loss, and observable psychomotor change. Speech may be sparse; latency lengthens; self-care collapses. When psychosis co-occurs, guilt and nihilistic themes are common — treat that pathway as psychotic depression intensity, not as "a bit more melancholic."[7][10]
Atypical features at the bedside. Mood can brighten temporarily to good news or interpersonal warmth, yet the episode remains impairing across weeks. Patients describe heavy leaden limbs, long sleeps, increased appetite or carbohydrate craving, and lifelong sensitivity to perceived rejection that damages work and relationships. Chronicity and partial inter-episode recovery are common teaching points.[4][5][6]
Overlap with seasonal winter depression. Winter major depression often shows reverse vegetative features and can meet atypical criteria — assess both the feature axis and the seasonal pattern course axis; they are related but not identical constructs.[4][6]
Differential diagnosis
Bipolar depression
- Prior hypo/mania decisive
- Atypical features common in bipolar depression
- Family history and postpartum mania clues
- Stabiliser-first when bipolar
Psychotic depression / catatonia
- Delusions/hallucinations or catatonic signs
- Often melancholic neurovegetative change
- Combination AD+AP or ECT
- Not coded as atypical
Medical / sleep mimics
- Hypothyroidism, anaemia
- OSA with hypersomnia and weight
- Steroids and other drugs
- Investigate when history suggests
Personality / anxiety overlap
- Rejection sensitivity can be trait-like
- Borderline affective instability vs full MDE
- Social anxiety comorbidity
- Formulate both axes when comorbid
Also discriminate primary hypersomnia syndromes, delayed sleep-phase disorder, anorexia nervosa weight trajectory, grief/demoralisation without full MDE, and substance-related mood change.[6][10]
Assessment
Structure the interview: (1) confirm full MDE criteria and impairment; (2) probe mood reactivity with concrete recent examples; (3) map vegetative polarity (sleep and appetite direction, weight change); (4) diurnal variation and early waking; (5) observe psychomotor state; (6) guilt quality and anhedonia breadth; (7) leaden paralysis and rejection-sensitivity history when atypical is possible; (8) bipolar screen every time; (9) substances, medical list, perinatal status; (10) suicide risk with means; (11) collateral for intake and interpersonal crises.[4][10]
Scales. PHQ-9 tracks severity but under-samples specifier criteria — ask leaden paralysis, rejection sensitivity, reactivity, and early waking explicitly. HAM-D and MADRS are useful clinician-rated anchors in secondary care.[10][13]
Investigations
As for major depression: FBC, U&E, LFT, TSH; glucose/lipids/BMI when metabolic risk or atypical weight gain; pregnancy test when relevant; ECG when TCAs or other QTc-risk agents are planned; consider sleep study if OSA is plausible for hypersomnia and weight gain. Do not order routine DST or specialised cortisol panels to confirm melancholia in general adult clinics — HPA literature informs viva framing, not day-to-day diagnosis.[8][10][11] Pre-ECT work-up follows standard medical/anaesthetic pathways when severity demands neurostimulation.[9]
Acute and emergency management
Stabilise medical risk (hydration, electrolytes, pressure care in profound retardation). Manage agitation with least-restrictive safe options while locking a definitive depression plan. Legal status follows jurisdiction-specific capacity and risk thresholds — never invent section numbers. Watch for serotonin toxicity when serotonergic load is high, NMS if antipsychotics are added for psychosis/agitation, and severe hyponatraemia in older adults on SSRIs.[10][16]
Definitive management
Melancholic pathway
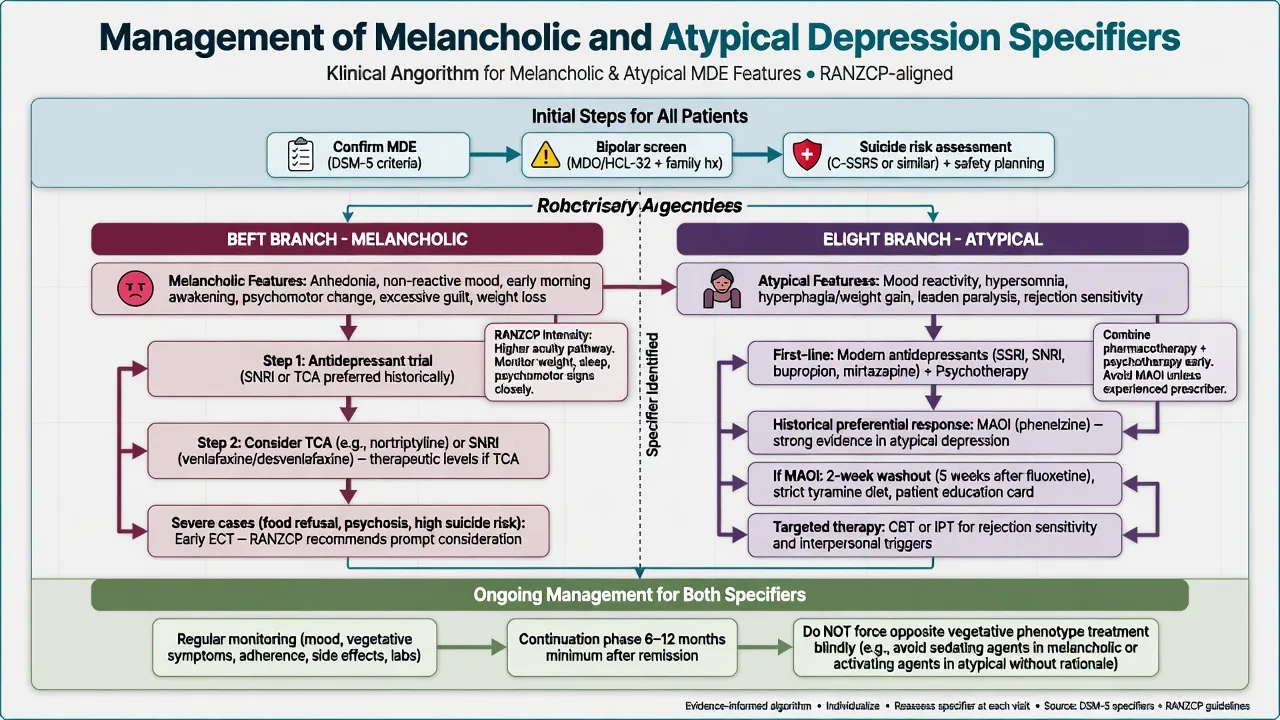
Measurement-based care remains mandatory. For moderate–severe melancholic major depression, start or optimise an evidence-based antidepressant at adequate dose and duration, with early specialist intensity. Teaching adult oral anchors (individualise; confirm product information): venlafaxine XR often start 75 mg orally daily, titrate toward 150–225 mg (sometimes higher under specialist BP monitoring); sertraline 50 mg orally daily toward 150–200 mg as tolerated; nortriptyline when TCA chosen — start low (e.g. 25 mg orally at night), titrate with plasma levels where available, ECG and anticholinergic risk review, typical antidepressant ranges often land near 50–150 mg daily depending on level and tolerance. Monitor response, activation, sodium in older adults, BP on SNRIs, and cardiac risk on TCAs.[10][11][13]
ECT has strong short-term efficacy in severe depressive disorders and is first-line or early when melancholia is severe, psychotic, catatonic, food-refusing, highly suicidal, previously ECT-responsive, or too slow on medicines.[9][10] Cortisol trajectory research is a scientific footnote, not a gate to ECT consent.[8]
Atypical pathway
Modern first-line care still uses evidence-based antidepressants and/or psychotherapy rather than leaping to MAOI for every reverse vegetative outpatient. SSRIs, SNRIs, and bupropion are commonly used; bupropion SR switch logic after SSRI nonresponse is examinable from STAR*D (e.g. start 150 mg orally daily, increase toward 300–400 mg daily in divided SR dosing as tolerated; seizure-risk exclusions apply).[11][13]
Historical preferential response. Columbia programme RCTs showed phenelzine superior to imipramine and placebo patterns in atypical depression defined by reactivity and associated features — this is the classic paper set every viva expects by name (Liebowitz 1988; Quitkin 1988).[1][2] Jarrett 1999 showed cognitive therapy and phenelzine both superior to placebo in atypical depression, supporting psychotherapy as a real option, not a soft afterthought.[3] Stewart’s clinical synthesis remains a practical examination map for treating atypical features in contemporary systems.[4]
When MAOI is chosen (specialist). Example teaching: phenelzine start 15 mg orally daily, build toward often 45–90 mg/day in divided doses as tolerated with postural BP checks; absolute tyramine diet education; pharmacy flag; written crisis plan for severe headache after restricted foods; never combine with SSRI/SNRI/clomipramine/tramadol/pethidine; about 2-week washout from most serotonergic antidepressants and about 5 weeks after fluoxetine before irreversible MAOI. STAR*D level-4 tranylcypromine data show late-pathway MAOI is hard and low-yield after multiple failures — specialist intensity, not casual improvisation.[14][16]
Psychotherapy and social interventions
Network meta-analysis supports multiple evidence-based psychotherapies for depression; choose modality to fit residual maintaining factors.[15] For atypical presentations, target behavioural withdrawal, interpersonal rejection sensitivity, and rumination with CBT or IPT-informed work. For melancholia, therapy is adjunctive once biological intensity has secured enough engagement — not a substitute for ECT when the patient is not eating.[3][10][15]
Regional guideline deltas
RANZCP mood disorder guidelines emphasise formulation-driven care, bipolar exclusion, staged pharmacological and psychological treatment, and early ECT for severe melancholic and psychotic presentations within Australian and New Zealand service models.[10]
Subtypes and scenarios
Melancholia with psychotic features. Treat as psychotic depression intensity: combination antidepressant plus antipsychotic or ECT — not SSRI alone.[9][10]
Atypical features plus seasonal pattern. Assess both axes; winter light therapy may apply when seasonal pattern criteria are met (see seasonal topic) without dropping suicide-risk and bipolar screens.[4][6]
Atypical features in bipolar depression. Stabiliser-first framing; antidepressants only with care after elevation risk is managed.[10]
Late-life melancholia. Medical comorbidity, higher psychotic-feature rates in severe episodes, ECT often highly effective, start medicines low, monitor sodium and falls.[9][10]
Treatment-resistant atypical depression. After adequate first-line trials, specialist review for MAOI pathway, augmentation, or neuromodulation — exclude pseudo-resistance first.[13][14][16]
Complications and pitfalls
Prognosis and disposition
Melancholic episodes often show strong response signals to biological treatments including ECT when severity is high; incomplete recovery and residual symptoms still predict relapse.[8][9] Atypical presentations may run a more chronic course with anxiety comorbidity and interpersonal relapse triggers; psychotherapy and long-term relapse prevention matter.[4][6][15] Disposition ladder: measurement-based community care → intensive community → voluntary inpatient → involuntary care when risk/capacity thresholds met under local law → ECT suite. STARD sequential remission decrements apply mainly to outpatient non-psychotic MDD sequencing — do not use STARD alone as the algorithm for near-terminal melancholia.[13]
Special populations
Older adults
- More melancholic/psychotic severe episodes
- ECT often highly effective
- Lower start doses; Na and falls vigilance
- Medical comorbidity review
Youth
- Atypical features and rejection sensitivity common
- Bipolar and trauma differentials
- Family involvement
- Specialist CAMHS when severe
Pregnancy
- Untreated severe melancholia is not zero-harm
- ECT may be preferred in high-risk illness
- MAOI generally avoided
- Perinatal specialist liaison
Cultural safety
- Guilt and rejection content with cultural formulation
- Interpreter and family decision styles
- FRANZCP cultural safety expectations
- Do not pathologise normative beliefs
Population-specific monitoring changes first steps — state them explicitly at viva.[9][10]
Evidence, guidelines and controversies
Landmark pillars: Liebowitz 1988 and Quitkin 1988 Columbia atypical MAOI specificity;[1][2] Jarrett 1999 cognitive therapy versus phenelzine;[3] Stewart 2007 treating atypical features synthesis;[4] Quitkin 2002 and Łojko 2017 validity and prevalence reviews;[5][6] Parker 2015 melancholia as specifier versus disorder debate;[7] Mickey 2018 cortisol trajectory, melancholia, and ECT response;[8] UK ECT Review Group;[9] RANZCP 2020 and CANMAT pharmacological framing;[10][11] STAR*D multi-step and late MAOI pathway context;[13][14] Cuijpers psychotherapy network meta-analysis;[15] contemporary MAOI prescriber guides for safe late-pathway use.[16]
Controversies to handle calmly: whether melancholia should be a freestanding disorder; how strongly MAOI preferential response survives in the SSRI era; how often pure atypical versus mixed reverse vegetative presentations occur; metabolic and safety trade-offs of late-pathway strategies. Answer with named criteria, named trials, and patient-specific risk.[4][6][7]
Exam pearls
REACTIVE
REACTIVE is a memory scaffold for viva sequence — still apply full formulation, local legal standards, and measurement-based care.[1][3][9][10]
References
- [1]Quitkin FM, Stewart JW, McGrath PJ, et al. Phenelzine versus imipramine in the treatment of probable atypical depression: defining syndrome boundaries of selective MAOI responders Am J Psychiatry, 1988.PMID 3278631
- [2]Liebowitz MR, Quitkin FM, Stewart JW, et al. Antidepressant specificity in atypical depression Arch Gen Psychiatry, 1988.PMID 3276282
- [3]Jarrett RB, Schaffer M, McIntire D, et al. Treatment of atypical depression with cognitive therapy or phenelzine: a double-blind, placebo-controlled trial Arch Gen Psychiatry, 1999.PMID 10232298
- [4]Stewart JW Treating depression with atypical features J Clin Psychiatry, 2007.PMID 17348764
- [5]Quitkin FM Depression with atypical features: diagnostic validity, prevalence, and treatment Prim Care Companion J Clin Psychiatry, 2002.PMID 15014736
- [6]Łojko D, Rybakowski JK Atypical depression: current perspectives Neuropsychiatr Dis Treat, 2017.PMID 29033570
- [7]Parker G Melancholia and catatonia: disorders or specifiers? Curr Psychiatry Rep, 2015.PMID 25417594
- [8]Mickey BJ, Ginsburg Y, Sitzmann AF, et al. Cortisol trajectory, melancholia, and response to electroconvulsive therapy J Psychiatr Res, 2018.PMID 29775916
- [9]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045
- [10]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [11]Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [12]Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R) JAMA, 2003.PMID 12813115
- [13]Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report Am J Psychiatry, 2006.PMID 17074942
- [14]McGrath PJ, Stewart JW, Fava M, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946177
- [15]Cuijpers P, Quero S, Noma H, et al. Psychotherapies for depression: a network meta-analysis covering efficacy, acceptability and long-term outcomes of all main treatment types World Psychiatry, 2021.PMID 34002502
- [16]Van den Eynde V, Abdelmoemin WR, Abraham MM, et al. The prescriber's guide to classic MAO inhibitors (phenelzine, tranylcypromine, isocarboxazid) for treatment-resistant depression CNS Spectr, 2023.PMID 35837681