Psych · General adult psychiatry — bipolar and related disorders
Mixed features and rapid cycling
Also known as Mixed episode · Mixed features specifier · Dysphoric mania · Mixed depression · Rapid cycling bipolar · Ultra-rapid cycling · Ultradian cycling
Exam-exhaustive fellowship reference on DSM-5-TR mixed features specifier versus historical mixed episode, ICD-11 framing, rapid cycling (≥4 episodes in 12 months), suicide risk in mixed states, antidepressant monotherapy prohibition, lithium/valproate/SGA algorithms, thyroid and substance drivers, STEP-BD and olanzapine mixed-features evidence, and RANZCP/NICE/CANMAT/BAP deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Mixed features and rapid cycling are the two bipolar course modifiers examiners use to test whether you think in polarity, not unipolar templates. A FRANZCP MEQ will demand operational criteria, a suicide-focused risk plan, and named agents with doses; an MRCPsych item will punish antidepressant monotherapy; an ABPN stem will bury mixed symptoms inside an “agitated depression” vignette. This topic is the specialist layer on top of bipolar I/II — read it as the high-risk phenotype chapter.[13][14][15][19]
Overview and definition
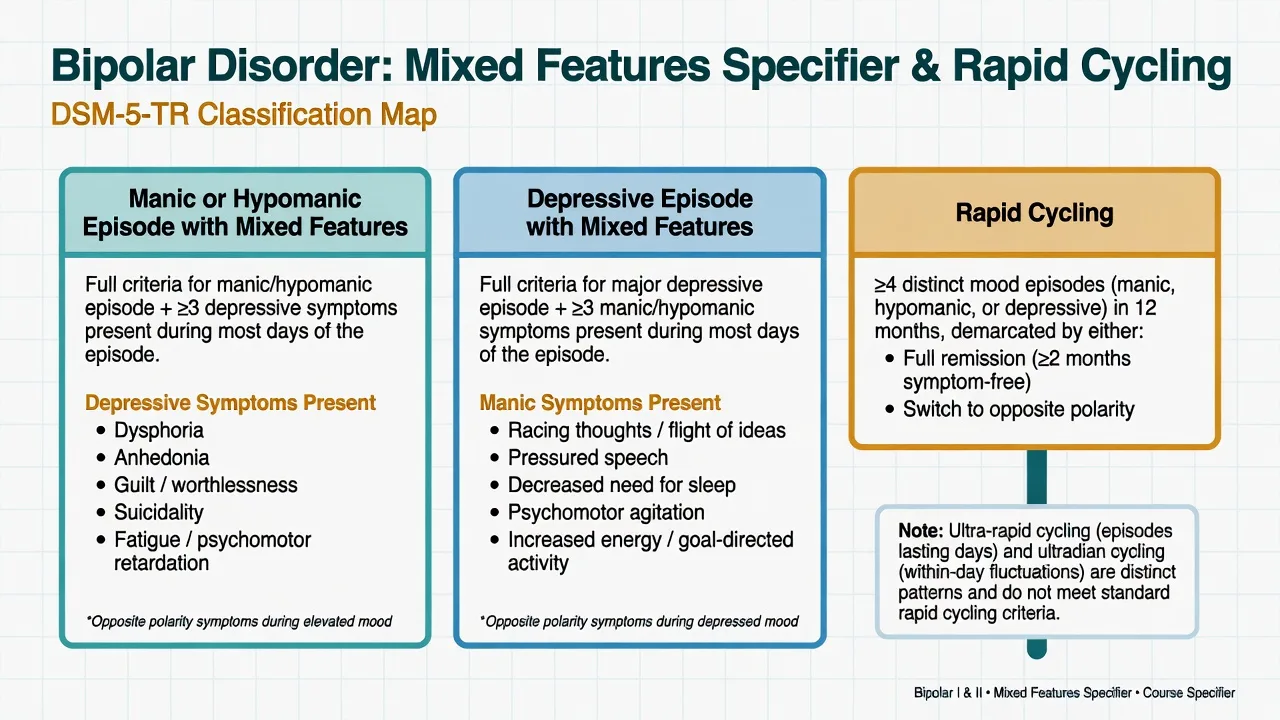
Mixed features (DSM-5-TR specifier). Applied when a full manic, hypomanic, or major depressive episode is accompanied by opposite-pole symptoms present during most days of the episode. It is not a free-standing diagnosis. It replaces the older requirement, for many exam purposes, that a patient must meet full mania and full depression at the same time (the historical mixed episode construct).[2][19]
Operational framing candidates must own these two poles of the mixed features specifier.[2][19]
- Manic or hypomanic episode with mixed features: full manic or hypomanic criteria plus at least three depressive symptoms (for example dysphoria, anhedonia, guilt or worthlessness, suicidality, fatigue or psychomotor retardation) present most days of the episode. Symptoms that can count for both poles (irritability, distractibility, insomnia/agitation) need careful attribution — do not double-count casually.[2][19]
- Major depressive episode with mixed features: full major depressive criteria plus at least three manic or hypomanic symptoms (racing thoughts or flight of ideas, pressured speech, decreased need for sleep, psychomotor agitation, increased energy or goal-directed activity, elevated or expansive mood, grandiosity). Decreased sleep need (energy preserved) is not the same as insomnia with exhaustion.[3][19]
Historical mixed episode. DSM-IV mixed episode required simultaneous full mania and full major depression for at least 1 week. That phenotype still exists clinically (severe dysphoric mania) but is now captured more broadly by the mixed features specifier, which also includes subtler opposite-pole loading that predicts severity and suicide risk.[2][19]
Rapid cycling. At least four distinct mood episodes meeting full criteria (manic, hypomanic, or major depressive) within a 12-month period, demarcated by full or partial remission of at least 2 months or by a switch to the opposite polarity. It is a course specifier, not a separate disease. Ultra-rapid (episodes lasting days to weeks) and ultradian (within-day mood shifts) patterns are descriptive clinical language and usually do not meet formal rapid-cycling criteria by themselves — examiners fail candidates who call every affective storm “rapid cycling.”[4][6][20]
ICD-11. Retains a mixed episode / mixed features clinical logic with polarity-based episode construction. State which manual you are using in the answer; do not invent hybrid criteria.[19]
Classification
Mixed features (episode specifier)
- Opposite-pole symptoms during a full manic, hypomanic, or depressive episode
- Typically ≥3 opposite-pole symptoms most days of the episode
- High suicide and severity signal
- Changes acute pharmacotherapy away from AD monotherapy
Historical mixed episode
- Full mania + full major depression simultaneously
- Narrower construct than DSM-5-TR mixed features
- Still useful language for severe dysphoric mania
- Do not require this bar to withhold antidepressants
Rapid cycling (course specifier)
- ≥4 full mood episodes in 12 months
- Demarcated by remission or polarity switch
- Often state-like and driver-linked
- Hunt AD, thyroid, substances, sleep chaos
Ultra-rapid / ultradian
- Days–weeks (ultra-rapid) or within-day (ultradian) shifts
- Usually not formal DSM rapid cycling alone
- Differential includes BPD, ADHD, substance use
- Still warrants careful polarity charting
Epidemiology and risk factors
Headline numbers
Prospective outpatient data comparing rapid-cycling and non-rapid-cycling bipolar illness show more overall morbidity, more depressive burden in many samples, and a phenotype that is clinically meaningful but not always permanent.[4] Systematic reviews estimate rapid cycling in roughly one in five bipolar patients depending on method, with associations to earlier onset, more severe course, and treatment complexity.[6][20]
STEP-BD analyses demonstrated that manic symptoms during bipolar depressive episodes are common and clinically important — not rare curiosities.[3] Depressive features during mania increase severity and influence treatment outcomes under DSM-5 mixed-specifier analyses.[2]
Risk associations for rapid cycling and mixed states. Female sex (many series), antidepressant exposure, thyroid dysfunction (including lithium-related hypothyroidism), substance use (stimulants, cannabis, alcohol), sleep disruption, and earlier onset. Wehr’s classic series emphasised antidepressants and other reversible factors among contributors to rapid cycling.[5][6]
Pathophysiology
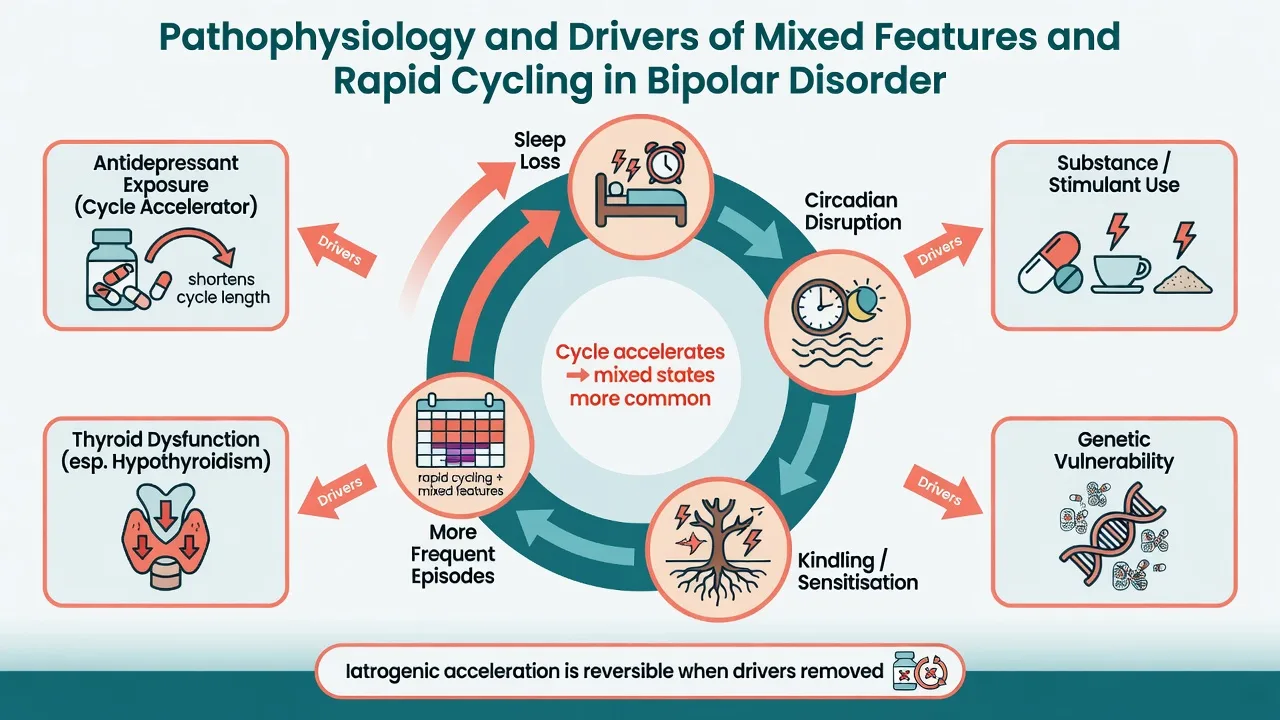
Think multi-level, not single-transmitter dogma. Circadian instability and sleep loss both trigger and maintain polarity instability. Kindling or sensitisation language (earlier episodes more stress-triggered, later more autonomous and frequent) is useful at viva depth if you avoid overclaiming it as proven in every patient.[19][6]
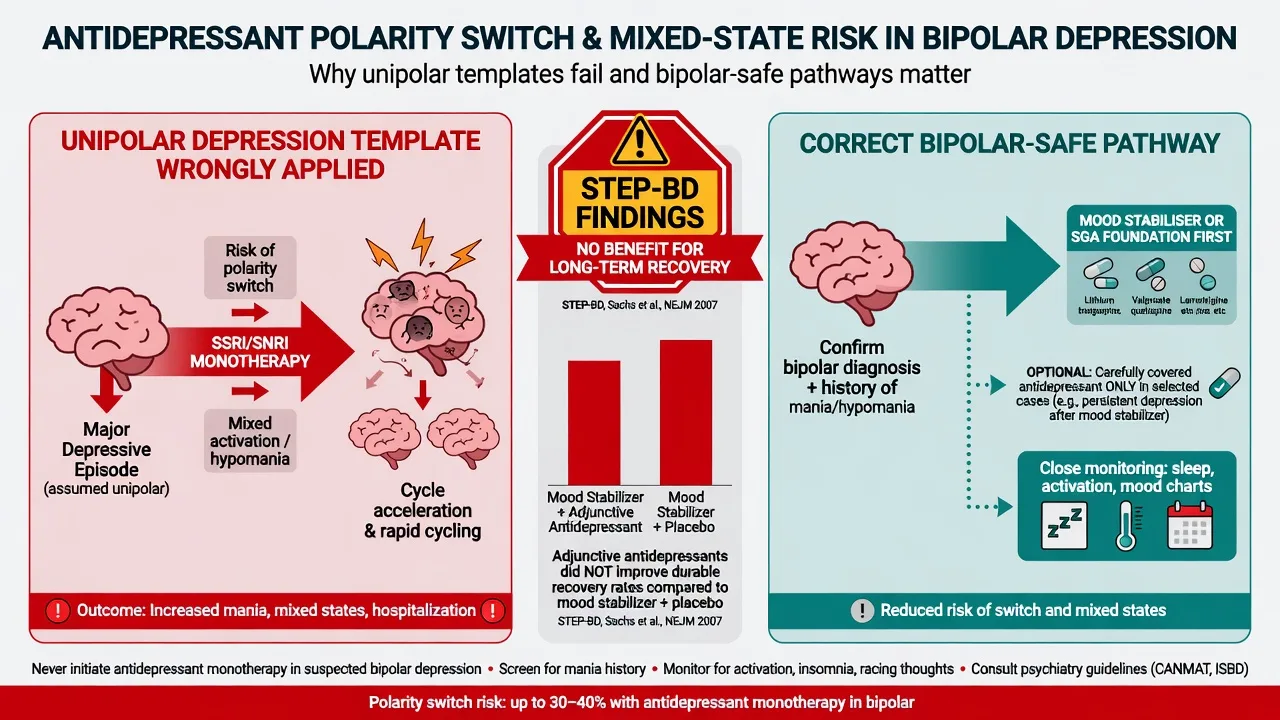
Iatrogenic pathophysiology. Antidepressants can precipitate switch into mania or mixed states and may accelerate cycling in vulnerable patients; transition-to-mania data from bipolar depression treatment cohorts support vigilance for activation.[8][9] Thyroid axis disruption, including subclinical hypothyroidism, is a reversible contributor that must be screened rather than mythologised.[5][6]
Mixed phenomenology can be framed as concurrent activation of arousal or approach systems (energy, pressure, decreased sleep need) and negative valence systems (dysphoria, guilt, suicidality). That framing explains why the high-risk phenotype is depression plus energy, not depression plus retardation alone.[2][3]
Clinical presentation
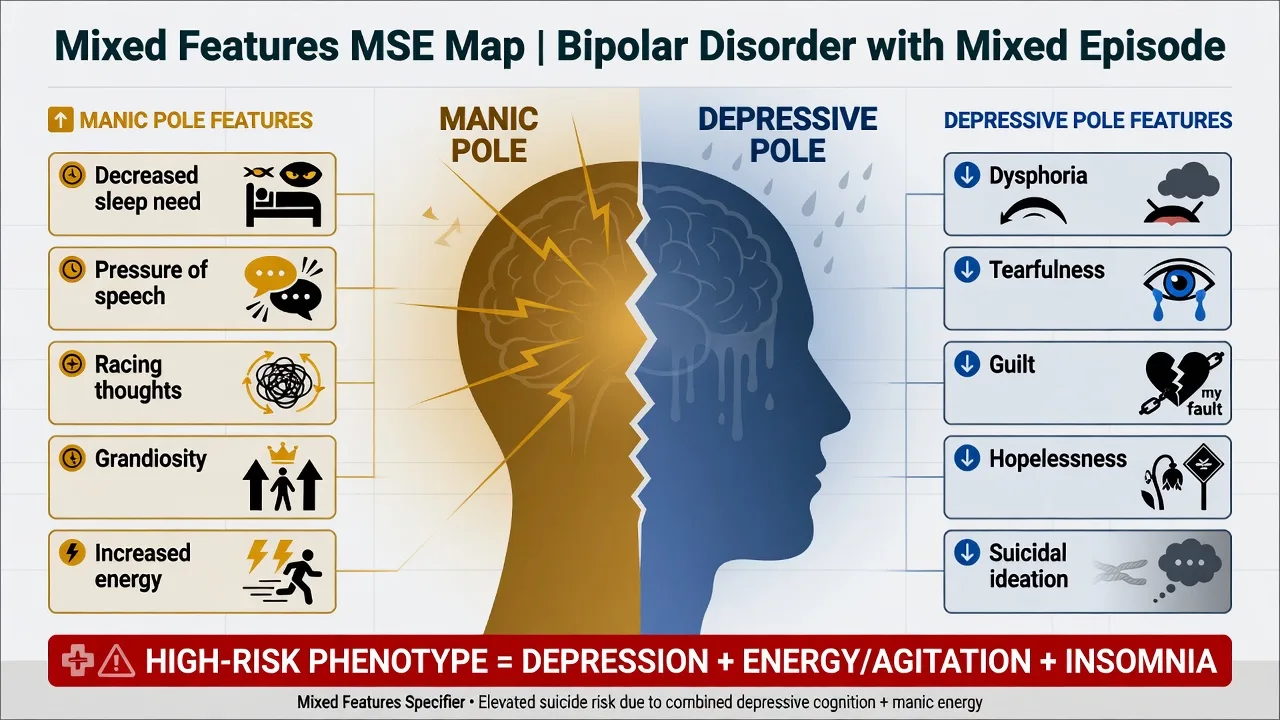
Mania or hypomania with mixed features. Mood may be irritable more than euphoric. Speech remains pressured; thought form accelerated; sleep need falls. Simultaneously the patient reports tearfulness, self-reproach, anhedonia, or active suicidal ideation. Families describe “wired and weeping.” Insight is often poor for the manic pole even when depressive cognitions are loudly present.[2][19]
Depression with mixed features. Core depressive syndrome with racing thoughts, pressure, restlessness, goal-directed bursts, or decreased sleep need. STEP-BD quantified how frequently manic symptoms ride along with bipolar depression.[3] This is the classic setup for misdiagnosis as “agitated unipolar depression” and unsafe antidepressant monotherapy.[8][14]
Rapid cycling course. Patients and collaterals report a year of repeated poles with incomplete recovery. Mood charts beat retrospective guesswork. Incomplete inter-episode recovery, residual anxiety, and substance use are common companions.[4][6]
Atypical and special presentations. Late-onset first mixed picture demands organic rethink. Perinatal mixed states combine sleep deprivation and high suicide risk. Cultural expression of dysphoric activation must be interpreted with formulation skill, not dismissed as “personality.”[14][19]
Differential diagnosis
Discriminators matter more than lists.[14][19]
| Mimic | Points toward mimic | Points toward mixed features / rapid cycling |
|---|---|---|
| Borderline PD affective instability | Minutes–hours shifts, interpersonal triggers, identity disturbance | Days–weeks syndromal poles; decreased sleep need; autonomous polarity |
| ADHD | Trait childhood onset, continuous inattention | Episodic poles with clear euthymic intervals |
| Stimulant intoxication | Timeline locked to drug; resolves with abstinence | Symptoms persist weeks after abstinence; lifetime polarity |
| Akathisia / AD activation | Starts after dose increase; restlessness without true decreased sleep need | Full opposite-pole cluster meeting specifier counts |
| Unipolar agitated depression | No lifetime hypo/mania after careful collateral | Any clear hypomania/mania or mixed symptom cluster in bipolar context |
| Delirium | Fluctuating attention, medical illness | Clear polarity without clouded sensorium |
| PTSD hyperarousal | Trauma cues, nightmares, avoidance | Sustained polarity with energy and sleep-need change |
| Hyperthyroidism | Heat intolerance, tremor, weight loss, abnormal TFT | Polarity persists after endocrine correction |
Organic and secondary causes of mixed or manic pictures include steroids, stimulant misuse, autoimmune encephalitis, frontal lesions, epilepsy, and Cushing syndrome. First mixed presentation after mid-life is a classic organic prompt.[19]
Clinical and bedside assessment
Structure assessment as polarity chart + opposite-pole screen + risk + medical exclusion + capacity.[13][14]
- 12-month episode chart: list every full manic, hypomanic, and major depressive episode with start/stop dates, hospitalisations, psychosis, and switches — this is how rapid cycling is diagnosed or refuted.
- Opposite-pole symptom inventory during the index episode (do not assume pure poles).
- MSE with quoted examples — “I am worthless and I need to fix the company tonight.”
- Suicide and violence risk: intent, plan, means, mixed energy, alcohol, agitation, protective factors. Mixed states demand higher intensity of risk management.
- Capacity and legal status using least-restrictive local statute principles (do not invent foreign section numbers).
- Collateral on sleep hours, spending, irritability, and day-to-day polarity.
- Scales conceptually: YMRS plus MADRS together for mixed severity; CGI; prospective mood charts and sleep diaries.[13][14]
Investigations
Before lithium, valproate, or an SGA, complete a safety baseline.[14][18]
- Bloods: FBC, U&E/eGFR, calcium, TFT (non-negotiable in rapid cycling), LFT, fasting glucose or HbA1c, lipids.
- ECG if cardiac risk, older age, or QT-relevant polypharmacy.
- Weight/BMI, BP, waist metabolic baseline.
- Pregnancy test when relevant.
- Urine drug screen (supports formulation; does not exclude primary bipolar).
- Imaging/EEG/autoimmune work-up for first atypical mixed presentations, focal neurology, seizure, or encephalitis features.[14][18]
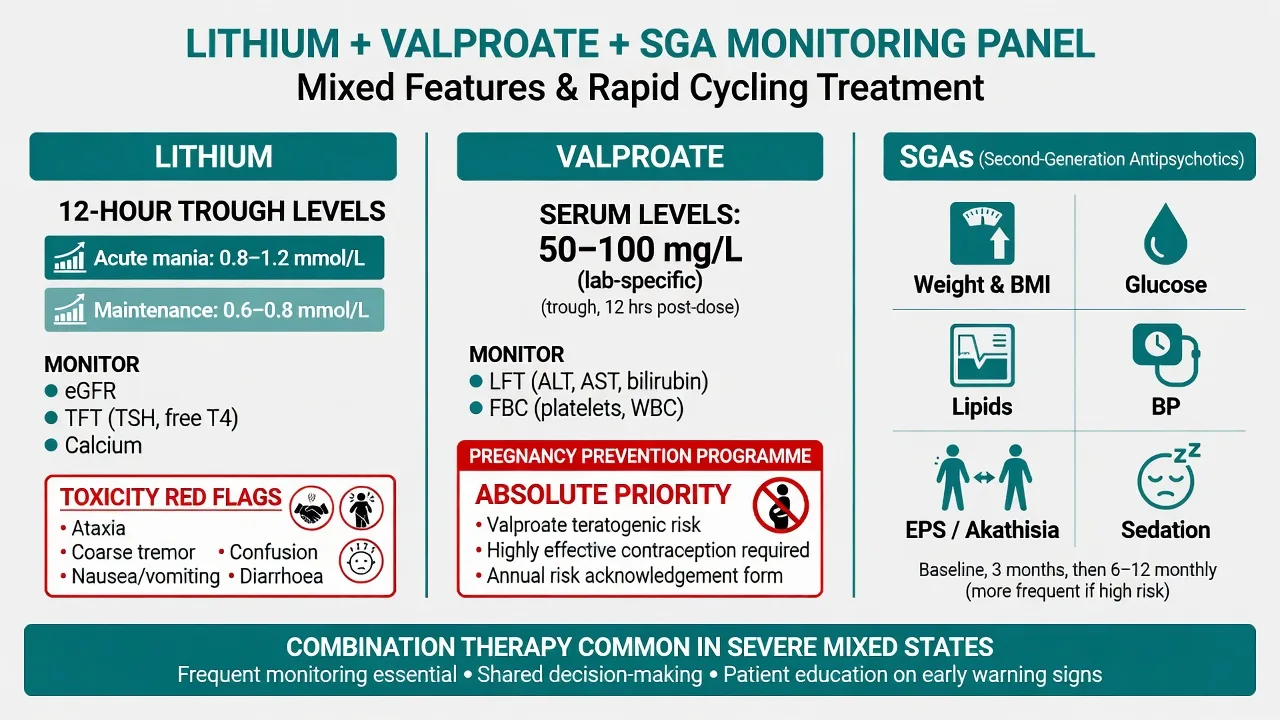
Lithium 12-hour troughs. Acute mania targets often about 0.8–1.2 mmol/L; maintenance commonly 0.6–0.8 mmol/L, individualised. Check 5–7 days after initiation or dose change. Toxicity risk rises as levels climb; severe toxicity may present above about 2.0 mmol/L.[18][15]
Valproate. Levels often interpreted around 50–100 mg/L (lab-specific); monitor LFT and FBC; pregnancy-prevention programme is absolute priority in people who can become pregnant.[13][14]
Management — acute / emergency
Priority order for acute mixed presentations.[13][14]
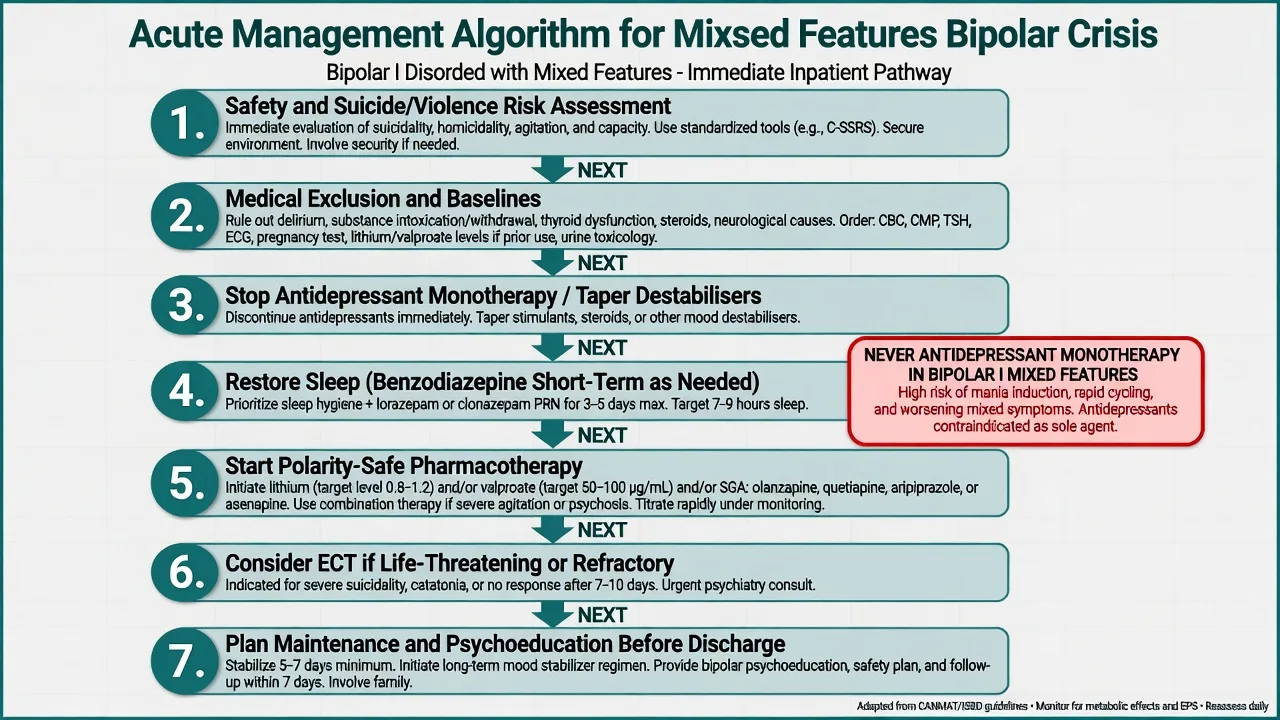
- Safety: suicide, violence, sexual disinhibition, financial ruin, absconding, child protection interface.
- Medical exclusion and baselines.
- Stop or carefully taper antidepressant monotherapy and other accelerators (stimulants, chaotic substance use) when clinically safe.
- Restore sleep — short-term benzodiazepine (for example lorazepam oral as needed per local protocol) while antimanic cover starts.
- Start polarity-safe pharmacotherapy (below).
- Legal status if incapacitous with high risk.
- Engage family and write an early-warning plan before discharge.[13][14][15]
Management — definitive and stepwise
Mixed mania or hypomania
Network meta-analysis supports multiple antimanic agents (several SGAs, lithium, valproate) for acute mania; choice is individualised to prior response, pregnancy potential, metabolic risk, and suicide history.[11] Landmark divalproex versus lithium versus placebo mania data remain relevant, including for more dysphoric presentations in the broader mixed tradition.[16] Post-hoc and prospective analyses support olanzapine efficacy in mania with DSM-5-defined mixed features.[1][2]
| Agent | Typical acute adult approach | Monitoring / notes |
|---|---|---|
| Lithium carbonate | Often start 400–800 mg/day; titrate to 12-hour trough | eGFR, TFT, calcium, level, ECG as indicated |
| Sodium valproate / divalproex | Loading or titration in selected acute protocols; clinical response ± level | LFT, FBC, pregnancy prevention absolute |
| Olanzapine | Often 10–20 mg oral daily | Metabolic panel, weight, sedation |
| Quetiapine | Mania doses commonly titrated toward 400–800 mg/day | Sedation, metabolic, BP |
| Aripiprazole | Often 15–30 mg oral daily in mania trials | Akathisia |
| Asenapine / risperidone / others | Per product information and prior response | EPS, prolactin (risperidone), oral numbness (asenapine) |
| Dose ranges are illustrative adult frameworks — individualise and check local product information.[1][11][13][14][16] |
Severe mixed mania frequently needs combination mood stabiliser plus SGA. ECT remains highly effective for suicidal, catatonic, exhausted, or refractory mixed states.[13][14]
Depression with mixed features
Do not apply a unipolar antidepressant ladder.[8][13][14]
- Prefer polarity-safe options with antimanic or bipolar-depression evidence: quetiapine, olanzapine-containing strategies, lithium, and carefully selected SGAs per guideline and availability.[13][14]
- Olanzapine–fluoxetine combination has bipolar I depression RCT support but carries olanzapine metabolic cost; mixed-feature depression still requires extreme caution with the fluoxetine component and is not a licence for SSRI monotherapy.[17]
- STEP-BD found adjunctive antidepressants (paroxetine or bupropion) added to mood stabilisers did not outperform mood stabiliser plus placebo for durable recovery — foundational evidence against casual antidepressant use.[8]
- If an antidepressant is used at all in bipolar illness, cover with a mood stabiliser, avoid monotherapy in bipolar I, keep duration short, and monitor sleep and activation daily in the early phase.[8][9][13]
Rapid cycling — treat the drivers
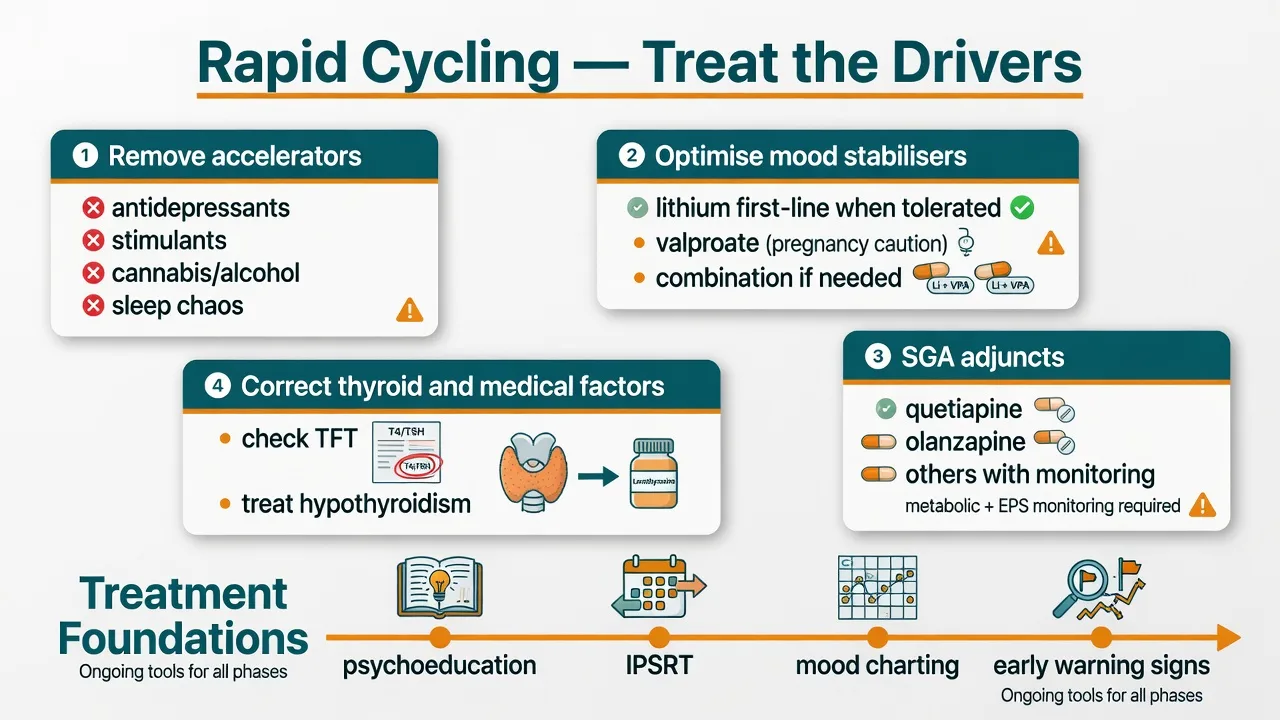
Evidence-based strategies synthesised in systematic reviews emphasise removing cycle accelerators and optimising mood-stabilising regimens rather than stacking antidepressants.[6][7][20] Wehr’s classic observations remain exam gold: antidepressants and thyroid factors are treatable contributors.[5]
Practical ladder for rapid cycling.[6][7]
- Stop or taper antidepressants when they are fuelling switches; avoid restarting as monotherapy.
- Optimise lithium when tolerated (anti-relapse and anti-suicide evidence; BALANCE supports lithium over valproate monotherapy for bipolar I maintenance, with combination also effective).[10][12]
- Consider valproate when lithium is unsuitable and pregnancy risk is managed; combination lithium–valproate is sometimes required for difficult courses.[10][16]
- Add an SGA for residual mixed or manic symptoms (olanzapine, quetiapine, and others with antimanic evidence).[1][11]
- Correct thyroid dysfunction; re-check TFT on lithium.[5][18]
- Enforce sleep regularity; offer psychoeducation, IPSRT, CBT-bipolar, and family-focused work as adjuncts.[13][14][15]
Monitoring panel
McKnight’s systematic review quantifies lithium’s renal, thyroid, and parathyroid long-term risks — monitor rather than mythologise.[18] Cipriani’s meta-analysis supports lithium for suicide prevention in mood disorders, highly relevant when mixed features elevate risk.[12]
Specific subtypes and scenarios
Bipolar I mania with mixed features. Admit if risk or exhaustion demands it. Combination antimanic therapy; no antidepressant; sleep restoration; ECT if life-threatening.[1][13]
Depression with mixed features as first presentation. Screen lifetime hypomania meticulously with collateral. If bipolar spectrum is likely, treat as polarity-unsafe depression.[3][14]
Bipolar II rapid cycling, depression-predominant. Still avoid AD monotherapy. Lithium, lamotrigine (slow titration for depression prevention — not a rapid acute fix), quetiapine, and psychosocial rhythm therapy are common tools; individualise to evidence and comorbidity.[13][14]
Antidepressant-induced mixed state. Stop or taper the antidepressant, cover with mood stabiliser/SGA, restore sleep, reassess diagnosis.[8][9]
Lithium-related hypothyroidism with rapid cycling. Treat thyroid disease; do not abandon lithium solely for mild TSH rise without endocrine reasoning.[5][18]
Perinatal mixed features. Peak relapse risk postpartum; protect sleep; avoid valproate hierarchy in people who can become pregnant; lithium decisions require cardiac-risk counselling in pregnancy context and specialist shared care.[14]
Older adult mixed agitation. Lower starting doses, renally cautious lithium, intensified organic differential, fall and QTc risk.[14][18]
Complications and pitfalls
- Treating mixed depression as unipolar agitated depression with SSRI/SNRI alone.[8][14]
- Underestimating suicide because the patient is activated rather than retarded.[3]
- Labelling every mood swing “rapid cycling” without four full episodes in 12 months.[4][6]
- Ignoring thyroid, substances, and sleep as reversible drivers.[5]
- Valproate without pregnancy-prevention safeguards.[14]
- Lithium under-monitoring and interaction-precipitated toxicity (NSAIDs, ACEI/ARB, thiazides, dehydration).[18]
- Collapsing borderline interpersonal crises into bipolar labels — or the reverse — without tempo and sleep-need discriminators.[14]
Prognosis and disposition
Mixed features predict greater acute severity, more suicidality, and often harder short-term response than pure poles.[2][3] Rapid cycling is associated with higher morbidity but frequently remits when drivers are removed and stabilisers are optimised — it is not always a lifelong fixed subtype.[4][6]
Disposition. Admission for active high-risk mixed states, psychosis, exhaustion, or inadequate supports. Intensive community follow-up with early review after medication changes. Functional recovery often lags syndromal recovery; plan occupational and relationship rehabilitation, not only symptom checklists.[13][14]
Special populations
Youth. Irritability alone is not mania. Require operational episode criteria, collateral, and developmental formulation. Family psychoeducation is essential.[14][19]
Older adults. Secondary mixed states, drug interactions, renal lithium caution, lower starting SGA doses.[14][18]
Pregnancy and lactation. Valproate avoidance hierarchy is non-negotiable for people who can become pregnant. Lithium requires specialised counselling on cardiac malformation risk magnitude and monitoring. SGA choice individualised to metabolic and neonatal adaptation concerns.[14]
Intellectual disability and autism. Behavioural phenocopies are common; chart duration, sleep need, and autonomous polarity carefully.[14][19]
Cultural formulation. Interpret dysphoric activation and grandiosity with cultural humility without lowering the suicide threshold.[14]
Evidence, guidelines and regional differences
RANZCP mood disorder guidance emphasises polarity-safe treatment, careful antidepressant use, lithium’s central role when appropriate, and structured risk management — the spine of ANZ fellowship answers on mixed and rapid-cycling presentations.[14]
Landmark anchors: STEP-BD adjunctive antidepressants;[8] STEP-BD manic symptoms during depression;[3] olanzapine in DSM-5 mixed-feature mania;[1] McIntyre mixed-specifier outcome analyses;[2] Kupka rapid versus non-rapid prospective comparison;[4] Wehr contributing factors;[5] Carvalho and Roosen rapid-cycling reviews;[6][7] BALANCE lithium/valproate maintenance;[10] Cipriani antimanic NMA and lithium suicide meta-analysis;[11][12] Bowden divalproex mania RCT;[16] OFC bipolar depression trial.[17]
Exam pearls
MIXED-RC
Self-test: 90-second viva answer
Define mixed features (opposite-pole symptoms during a full episode; typically at least three). Define rapid cycling (at least four full episodes in 12 months). State the high-risk phenotype (depression + energy/agitation). State three drivers of rapid cycling (antidepressants, thyroid dysfunction, substances/sleep loss). Name acute agents (lithium, valproate, olanzapine/quetiapine/aripiprazole) with monitoring. Cite the STEP BD antidepressant trial against casual antidepressants and lithium’s anti-suicide signal. Close with pregnancy-prevention for valproate.[8][12][13][14]
References
- [1]Tohen M, McIntyre RS, Kanba S, et al. Efficacy of olanzapine in the treatment of bipolar mania with mixed features defined by DSM-5 J Affect Disord, 2014.PMID 25046739
- [2]McIntyre RS, Tohen M, Berk M, et al. DSM-5 mixed specifier for manic episodes: evaluating the effect of depressive features on severity and treatment outcome J Affect Disord, 2013.PMID 23712026
- [3]Goldberg JF, Perlis RH, Bowden CL, et al. Manic symptoms during depressive episodes in 1,380 patients with bipolar disorder: findings from the STEP-BD Am J Psychiatry, 2009.PMID 19122008
- [4]Kupka RW, Luckenbaugh DA, Post RM, et al. Comparison of rapid-cycling and non-rapid-cycling bipolar disorder based on prospective mood ratings in 539 outpatients Am J Psychiatry, 2005.PMID 15994709
- [5]Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients Am J Psychiatry, 1988.PMID 3341463
- [6]Carvalho AF, Dimellis D, Gonda X, et al. Rapid cycling in bipolar disorder: a systematic review J Clin Psychiatry, 2014.PMID 25004199
- [7]Roosen L, Sienaert P Evidence-based treatment strategies for rapid cycling bipolar disorder, a systematic review J Affect Disord, 2022.PMID 35545157
- [8]Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression N Engl J Med, 2007.PMID 17392295
- [9]Perlis RH, Ostacher MJ, Goldberg JF, et al. Transition to mania during treatment of bipolar depression Neuropsychopharmacology, 2010.PMID 20827274
- [10]BALANCE investigators and collaborators, Geddes JR, Goodwin GM, et al. Lithium plus valproate combination therapy versus monotherapy for relapse prevention in bipolar I disorder (BALANCE): a randomised open-label trial Lancet, 2010.PMID 20092882
- [11]Cipriani A, Barbui C, Salanti G, et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis Lancet, 2011.PMID 21851976
- [12]Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104
- [13]Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder Bipolar Disord, 2018.PMID 29536616
- [14]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [15]Goodwin GM, Haddad PM, Ferrier IN, et al. Evidence-based guidelines for treating bipolar disorder: Revised third edition recommendations from the British Association for Psychopharmacology J Psychopharmacol, 2016.PMID 26979387
- [16]Bowden CL, Brugger AM, Swann AC, et al. Efficacy of divalproex vs lithium and placebo in the treatment of mania. The Depakote Mania Study Group JAMA, 1994.PMID 8120960
- [17]Tohen M, Vieta E, Calabrese J, et al. Efficacy of olanzapine and olanzapine-fluoxetine combination in the treatment of bipolar I depression Arch Gen Psychiatry, 2003.PMID 14609883
- [18]McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis Lancet, 2012.PMID 22265699
- [19]Grande I, Berk M, Birmaher B, et al. Bipolar disorder Lancet, 2016.PMID 26388529
- [20]Mackin P, Young AH Rapid cycling bipolar disorder: historical overview and focus on emerging treatments Bipolar Disord, 2004.PMID 15541068