Psych · General adult psychiatry — personality disorders
Narcissistic and Cluster B spectrum
Also known as Narcissistic personality disorder · NPD · Cluster B personality disorders · Pathological narcissism · Histrionic personality disorder · Antisocial personality disorder spectrum · Malignant narcissism
Exam-exhaustive fellowship reference on narcissistic personality disorder and the Cluster B spectrum — grandiose and vulnerable narcissism; histrionic pointer diagnosis; overlap with BPD and ASPD/psychopathy; countertransference; management limits and structured psychotherapy options; risk after narcissistic injury. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
12 MCQs with explanations
Target exams
Red flags
Narcissistic and Cluster B presentations are high-yield across FRANZCP, MRCPsych, ABPN and MD/DNB examinations because they test whether you can use operational criteria without pejorative labelling, discriminate bipolar and organic mimics, hold a firm therapeutic frame under pressure, name realistic management limits, and still offer structured care and hope where evidence and engagement allow.[3][5][11]
Overview and definition
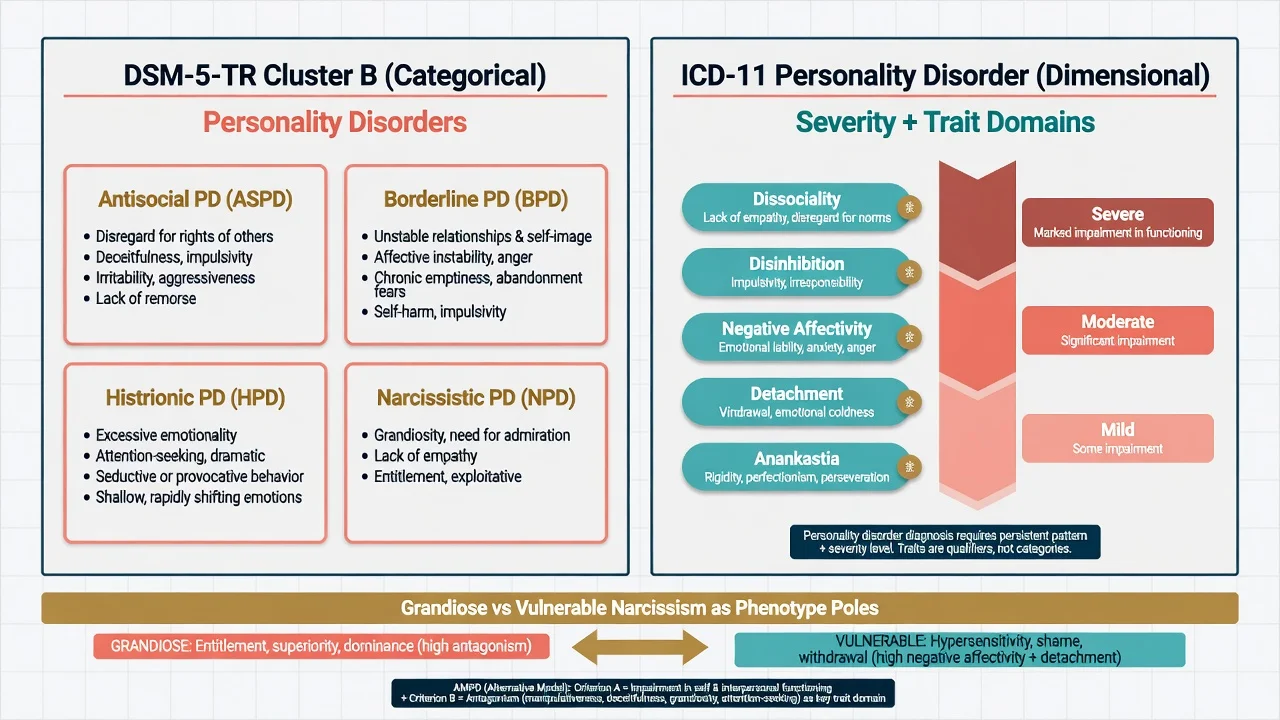
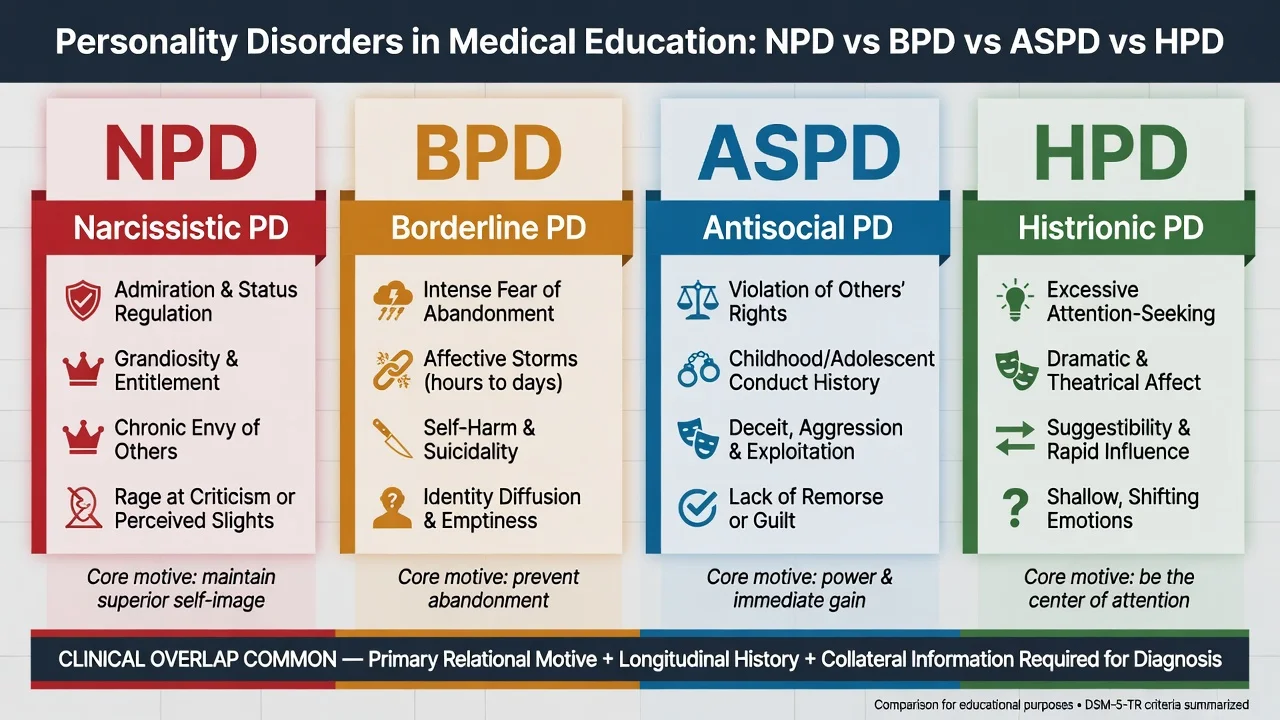
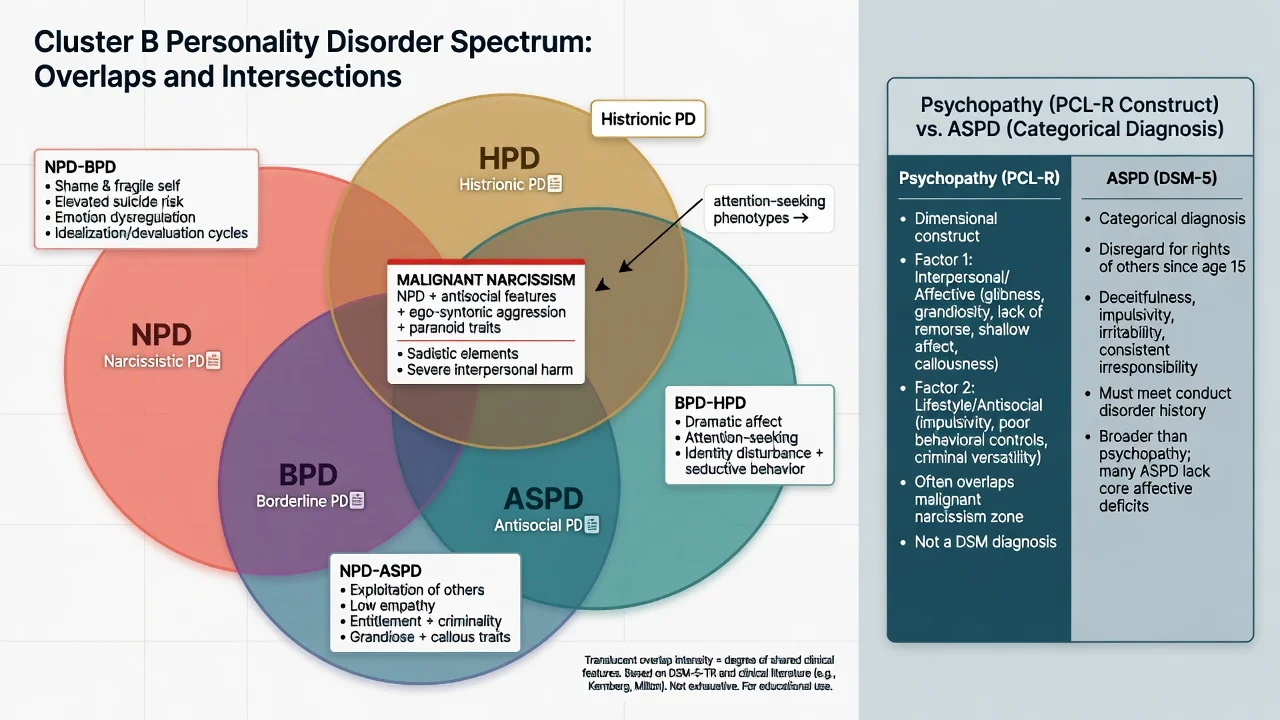
Cluster B in DSM-5-TR groups the dramatic/erratic personality disorders: antisocial, borderline, histrionic and narcissistic. Clusters are pedagogical scaffolding, not a proven shared aetiology. In practice, trait overlap is the rule; the clinical task is to identify the primary relational motive and longitudinal pattern while diagnosing comorbidity that changes risk and treatment.[3][4]
Narcissistic personality disorder (NPD) is a pervasive pattern of grandiosity (fantasy or behaviour), need for admiration, and lack of empathy, beginning by early adulthood and present across contexts. DSM-5-TR requires general personality disorder criteria plus five or more of nine features: grandiose sense of self-importance; fantasies of unlimited success, power, brilliance, beauty or ideal love; belief that one is special/unique and understood only by other special people; requires excessive admiration; sense of entitlement; interpersonally exploitative; lacks empathy; often envious or believes others are envious; arrogant, haughty behaviours or attitudes.[3][4]
Pathological narcissism (Pincus) is broader than the categorical NPD checklist: self-esteem dysregulation expressed as grandiose and/or vulnerable phenotypes that may oscillate in the same person. Examiners reward candidates who can describe both poles rather than equating NPD with cartoon arrogance alone.[4][12]
Histrionic personality disorder (HPD) is a pervasive pattern of excessive emotionality and attention-seeking. Treat it as a pointer diagnosis: construct validity is weaker than for BPD, and many “histrionic” presentations re-map onto borderline-spectrum emotion dysregulation, trauma-related presentations, or other patterns when carefully formulated.[13][14]
Antisocial personality disorder (ASPD) requires evidence of conduct disorder with onset before age 15 plus a pervasive adult pattern of disregard for and violation of the rights of others. Psychopathy is a related but not identical construct (interpersonal-affective traits plus lifestyle-antisocial behaviour; often operationalised with PCL tools by trained raters) — ASPD is not automatically “psychopathy.”[15][16][18]
Classification and nosology
DSM-5-TR Cluster B
- NPD ≥5/9 grandiosity/admiration/empathy criteria
- ASPD: conduct history + adult rights violation
- BPD: ≥5/9 instability/self-harm criteria
- HPD: excessive emotionality and attention-seeking
- Clusters are teaching aids, not pure taxa
ICD-11 dimensional PD
- Severity first: mild / moderate / severe
- Trait domains (e.g. dissociality, disinhibition, negative affectivity)
- Narcissistic themes appear as severity + antagonism-like pattern
- Borderline pattern specifier remains available
- Better for dimensional formulation stations
AMPD (DSM Section III)
- Criterion A: self and interpersonal impairment
- Criterion B traits: antagonism (grandiosity, attention-seeking)
- Vulnerable presentations add negative affectivity
- Useful viva language even if you diagnose categorically
Related constructs
- Pathological narcissism: grandiose + vulnerable poles
- Psychopathy ≠ ASPD alone
- Malignant narcissism: NPD + antisocial + ego-syntonic aggression + paranoid features
- Do not use constructs as insults
ICD-11 forces a fellowship habit examiners like: state severity of personality dysfunction, then the trait flavour (for example high dissociality and disinhibition in ASPD-like presentations; antagonism with variable negative affectivity in narcissistic presentations). You still need DSM criteria fluency for classic MCQ stems.[3][4]
Epidemiology and risk factors
Headline epidemiology candidates must own
Community surveys (NESARC Wave 2) characterise DSM-IV NPD prevalence, disability and psychiatric comorbidity; systematic review work emphasises that prevalence estimates vary with instrument and that treatment data in the community are sparse relative to clinical rhetoric about narcissism.[1][2]
ASPD shows substantial association with alcohol and drug use disorders in large epidemiologic samples — dual diagnosis is expected, not exceptional.[15] Developmental risk factors include early conduct problems (ASPD pathway), temperamental low agreeableness and high reward sensitivity, childhood adversity, inconsistent overvaluation or neglect, and modelling of entitlement or aggression. Trauma is common in Cluster B broadly but does not equal any single PD diagnosis.[16][17]
Pathophysiology and mechanisms
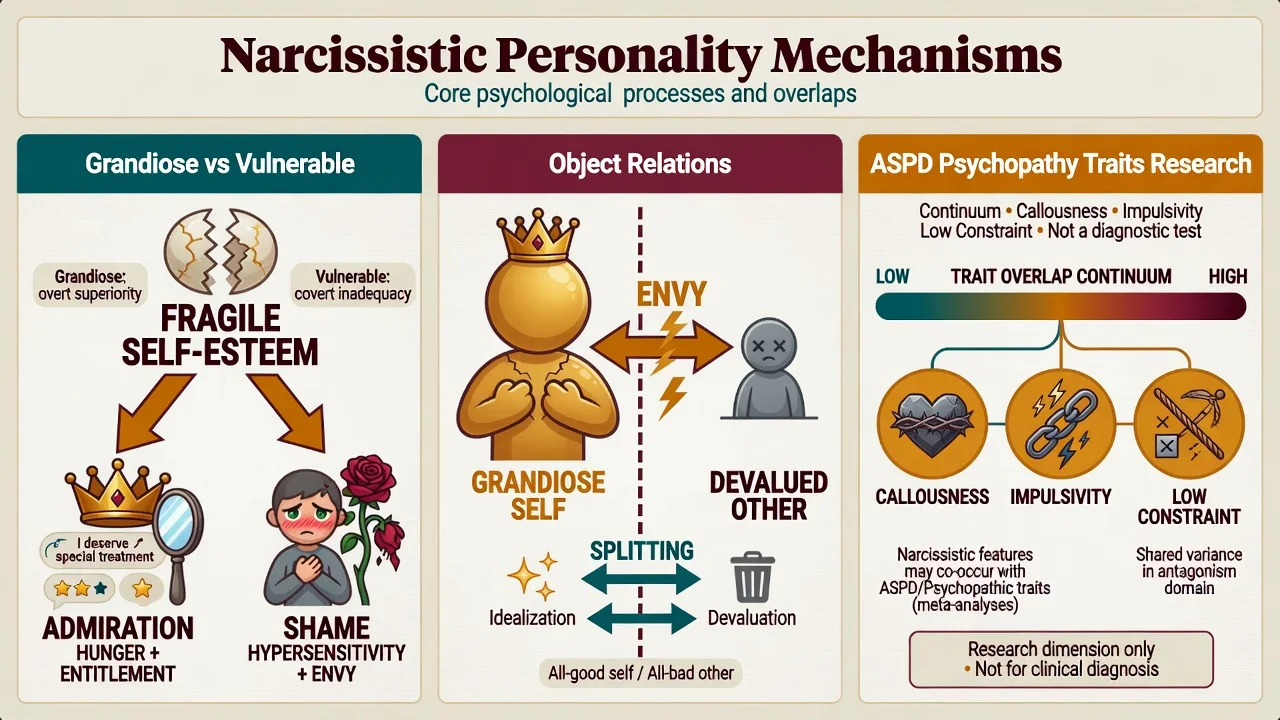
Grandiose versus vulnerable narcissism. Grandiose phenotypes regulate self-esteem through entitlement, status display and devaluation of critics. Vulnerable phenotypes present with shame, hypersensitivity, social withdrawal, envy and depression, often with covert grandiose fantasies. Emotion dysregulation co-travels with pathological narcissism in systematic review evidence — a bridge to BPD-spectrum presentations without collapsing categories.[4][12]
Object-relations (Kernberg tradition). A pathological grandiose self is maintained by devaluation of others, envy and primitive defences (splitting, projective identification). Malignant narcissism describes a severe configuration combining narcissistic pathology with antisocial behaviour, ego-syntonic aggression and paranoid features — clinically important for violence and treatment-limit discussions.[3][7]
Self-psychology (Kohut). Emphasises developmental deficits in mirroring and idealising needs; narcissistic rage follows empathic failure or perceived humiliation. Useful for understanding why minor slights can precipitate disproportionate aggression or collapse.[3][8]
ASPD and psychopathy. Contemporary syntheses emphasise low constraint/impulsivity, callous-unemotional and boldness-related traits, and developmental pathways from early conduct problems. These are research-level models; imaging and psychophysiology do not diagnose individuals.[18][16]
Clinical presentation
Grandiose NPD. Arrogance, status preoccupation, entitlement, exploitative relationships, contempt for “ordinary” people, thin-skinned rage when criticised, and externalising explanations for every failure. Charm may be high on first contact.[3][4]
Vulnerable/covert NPD. Quiet superiority, chronic envy, social avoidance, shame-proneness, depressive emptiness after status loss, passive aggression, and sometimes suicidality when the false self collapses. These patients are over-represented in depression clinics and under-counted if you only look for swagger.[4][8][12]
HPD pointer. Dramatic, theatrical affect; discomfort when not the centre of attention; inappropriately seductive or provisional intimacy; rapidly shifting shallow emotions; impressionistic speech. Always ask: is this mania, BPD, trauma-related affect, or substance disinhibition?[13][14]
ASPD. Deceit, impulsivity, irritability/aggression, reckless disregard for safety, consistent irresponsibility, lack of remorse, and often forensic or addiction service contact. Collateral and records beat self-report.[15][17]
MSE language that scores marks. Affect (charm, contempt, brittle irritability, shame collapse), thought content (entitlement themes, persecutory ideas after humiliation), insight (externalising), judgement, alliance quality, and risk (to self after injury; to others via exploitation or violence).[3][5]
Differential diagnosis
NPD vs BPD
- NPD: status/admiration regulation, envy, devaluation of critics
- BPD: abandonment fear, emptiness, self-harm as affect regulation
- Shared: identity instability, rage, relationship chaos
- Dual diagnosis allowed when both criteria met
NPD vs ASPD
- Both may exploit and lack empathy
- ASPD requires conduct history and rights-violation pattern
- NPD may remain non-criminal yet deeply damaging interpersonally
- Malignant narcissism sits in the overlap zone
NPD vs bipolar
- Mania/hypomania: days–weeks, reduced sleep need, energy
- NPD grandiosity is lifelong interpersonal style
- Antidepressant-switching history and family history matter
- Do not miss true mania under a PD label
Organic / substance / other
- Late-onset change → TBI, FTD, epilepsy, endocrine
- Intoxication/withdrawal mimics disinhibition
- Autism social difference ≠ callous exploitation
- ADHD impulsivity ≠ full Cluster B pattern alone
HPD versus BPD is a classic validity trap: empirical work questions the coherence of HPD as a distinct category and highlights overlap with borderline and “hysterical” personality subtypes — use discriminators, not fashion labels.[13][14]
Clinical and bedside assessment
Structure the interview: developmental and attachment history; school conduct and legal history; work trajectory and responses to criticism/failure; relationship patterns (idealisation, exploitation, serial abandonment); substance use; prior treatments and therapy drop-outs; current crisis trigger (shame, public failure, legal threat, breakup); collateral from partners, family, employers, or records.[3][17]
Risk domains. (1) Suicide and self-harm — especially vulnerable collapse after narcissistic injury, depression, substance use, and NPD–BPD overlap.[8] (2) Violence and intimate partner violence. (3) Exploitation, financial abuse, and safeguarding of children or dependent adults. (4) Public-order and forensic risk in ASPD. Capacity is decision-specific. Involuntary care uses local Mental Health Act principles — least restrictive, statute-bound; do not invent section numbers for the wrong jurisdiction.[16][17]
Tools (conceptual). SCID-5-PD / IPDE for structured PD diagnosis; pathological narcissism constructs (e.g. PNI tradition) for phenotype; PCL-R/PCL-SV for psychopathy in trained forensic contexts — never casual “psychopath” labelling from a single interview.[4][18]
Investigations
There is no laboratory gold standard for Cluster B disorders. Investigate to exclude mimics and prepare for medication when used: TSH, FBC, U&E, LFT, glucose/lipids if antipsychotics considered, pregnancy test when relevant, urine drug screen when substances may explain behaviour, ECG when cardiac risk or QTc-risk drugs are planned. Neuroimaging or EEG when late-onset change, focal neurology, seizures or cognitive decline fire. Screen systematically for major depression, bipolar spectrum, PTSD, ADHD, substance use disorders and other personality pathology.[3][17]
Management — acute crisis and resuscitation
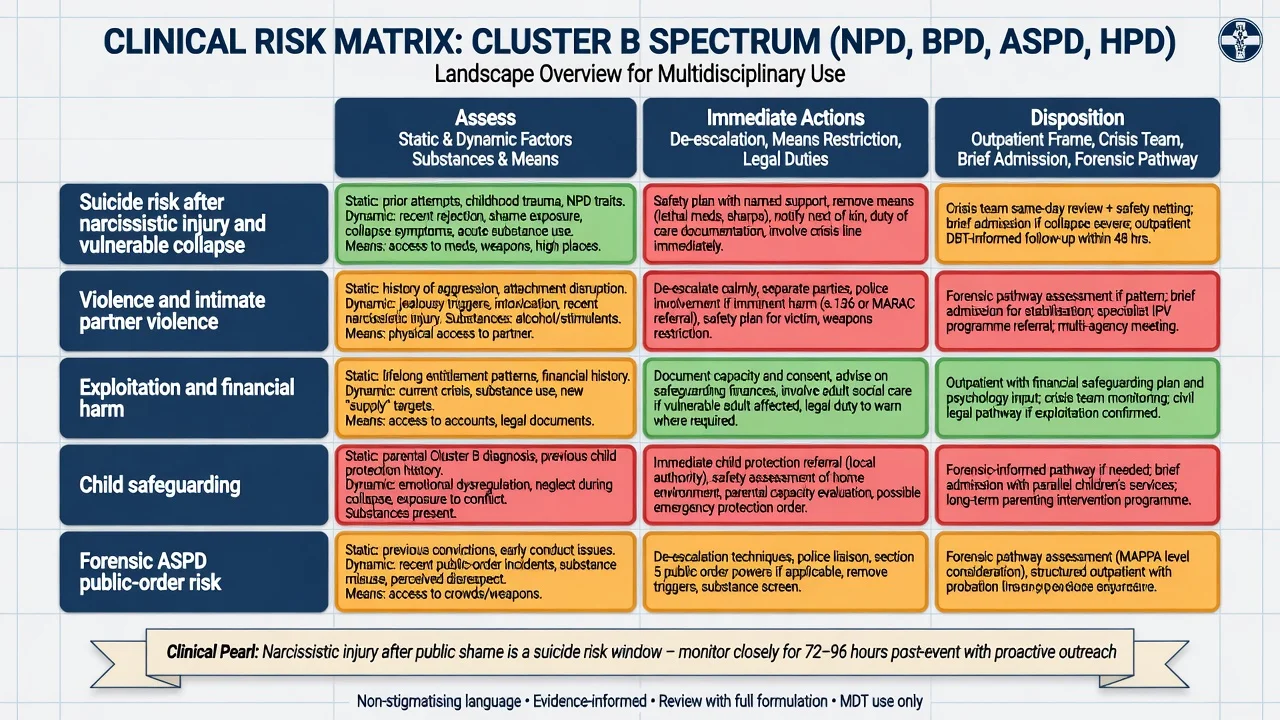
Crisis principles. Medical stabilisation first for overdose or injury. Validate the emotional pain of status loss without colluding with entitlement demands that break team rules. Means restriction. Time-limited safety plan. Least-restrictive setting that still manages risk. De-escalation before pharmacological restraint; if acute agitation threatens safety, use local emergency rapid-tranquillisation protocols with monitoring rather than inventing a long-term “narcissism sedative regimen.” For ASPD crises, clear behavioural limits and legal options sit alongside any psychiatric care of comorbidity or withdrawal.[8][17]
Management — definitive and stepwise (including honest limits)
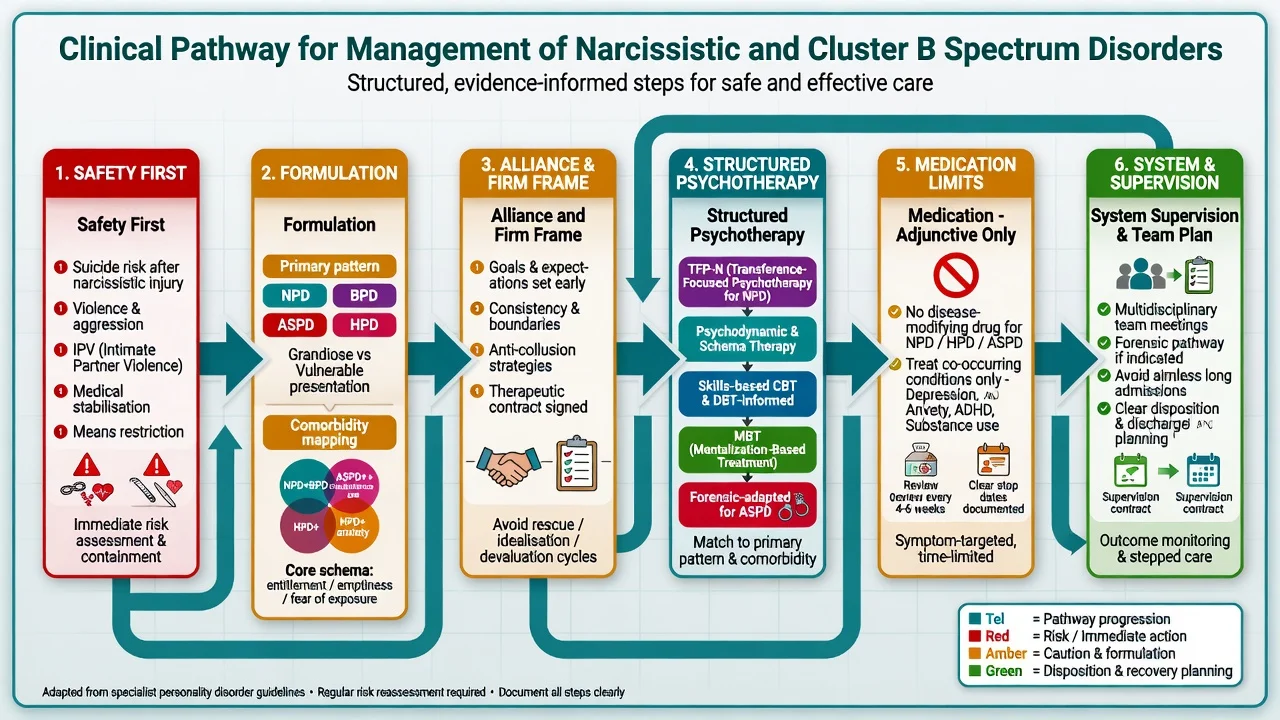
What the evidence can and cannot promise
Unlike BPD — where DBT, MBT, schema therapy, TFP and structured clinical management have a denser RCT base — NPD-specific randomised evidence is thinner. Fellowship answers that claim a miracle protocol fail. Competent answers state: engage where possible; hold a firm frame; treat comorbidity; use manualised approaches with theoretical and emerging clinical support; measure change; stop unhelpful polypharmacy.[3][10][11]
Alliance, frame and goals
Crisp and Gabbard outline psychodynamic treatment principles for NPD: expect idealisation and devaluation; protect the frame; work with shame as well as grandiosity; set explicit, collaborative goals; use supervision. Ronningstam describes patterns and indicators of change in long-term psychotherapy — engagement, increased reflective capacity, reduced exploitativeness and more stable self-esteem regulation are realistic targets, not instant “cure of narcissism.”[9][10]
Named psychotherapy options
Transference-focused psychotherapy for narcissism (TFP-N). Object-relations approach adapted for pathological narcissism and NPD, focusing on identity diffusion, split object relations and the activation of grandiose/vulnerable transferences in the therapeutic relationship.[6][7]
Schema therapy. A multicentre RCT of schema therapy for personality disorders (including Cluster B pathways beyond BPD alone) found clinical effectiveness advantages over clarification-oriented psychotherapy — examiners want the trial name-level fact that structured schema therapy has PD RCT support, while still not overclaiming an NPD-only magic bullet.[20]
GPM-style psychoeducation. Blay and colleagues review and propose a Good Psychiatric Management–based brief psychoeducation package for pathologic narcissism/NPD — useful when specialised long-term therapy is unavailable and the task is shared formulation, limits and skills-oriented psychiatric management.[11]
MBT and ASPD. Mentalisation-based approaches have been extended into forensic-community ASPD populations; the multicentre MOAM randomised trial in males on community probation evaluates MBT for ASPD and is the contemporary named trial candidates should know when discussing psychological treatment of antisocial presentations (interpret results carefully against the published outcomes, not wishful memory).[19]
Skills/CBT and dual diagnosis care. Treat comorbid depression, anxiety, PTSD and substance use with the same standards as outside PD care. Contingency management, offence-focused programmes and substance treatment are often more outcome-relevant in ASPD than exploratory therapy alone.[17][19]
Pharmacotherapy — management limits made explicit
Example adult prescribing language when forced to name a plan (individualise; check local product information). For comorbid major depression without bipolarity after risk–benefit discussion: sertraline 50 mg orally daily, early review for activation and suicidality (especially post-narcissistic injury), titrate toward 50–150 mg as tolerated with measurement-based follow-up — this treats depression, not entitlement. Avoid chronic benzodiazepines for rage or shame. If a specialist considers a short antipsychotic trial for severe agitation or near-psychotic paranoid collapse, document the target symptom, baseline metabolic/ECG risk as indicated, and a stop date; do not convert crisis sedation into lifelong personality pharmacotherapy.[3][8]
Care system and disposition
Match intensity to risk and engagement: outpatient psychotherapy with clear frame; community mental health team for comorbidity and moderate risk; crisis teams for acute injury states; brief admission when suicide or violence risk is uncontainable; forensic pathways when ASPD/violence risk and legal status require them. Avoid aimless long admissions that become a status battle rather than a treatment plan.[3][17]
Australian and New Zealand services manage Cluster B presentations across community mental health, addiction, and forensic interfaces. Emphasise cultural safety, safeguarding, and local Mental Health Act principles without inventing section numbers. Personality disorder pathways (where present) stress formulation, stepped care and staff support for countertransference — not diagnostic nihilism.[3][17]
Specific subtypes and scenarios
Grandiose, vulnerable and oscillating phenotypes. Same person may present as entitled executive at work and shame-collapsed suicidal patient after exposure. Formulate both poles.[4][12]
Malignant narcissism. High interpersonal harm; low motivation for change; risk of retaliatory violence; treatment goals may prioritise risk management and collateral protection over personality “cure.”[3][7]
NPD–BPD overlap. Emotion dysregulation plus status regulation yields high suicide and self-harm signal — do not under-treat risk because “they are just narcissistic.”[8][12]
HPD as pointer. Re-evaluate for BPD, trauma, somatic symptom presentations and mania; do not let a fashion label stop a proper longitudinal diagnosis.[13][14]
Workplace and medical-colleague scenarios. Privilege, status and institutional power amplify boundary risk — document, use hierarchy and professional standards pathways, and avoid private special arrangements.[5][9]
Forensic ASPD. Static and dynamic risk factors, substance use, and contextual triggers drive formulation. Natural history data show some age-related behavioural burn-down for subgroups, but high-psychopathy and persistent substance-using pathways remain high risk — neither nihilism nor naive optimism.[16][17][18]
Complications and pitfalls — countertransference central
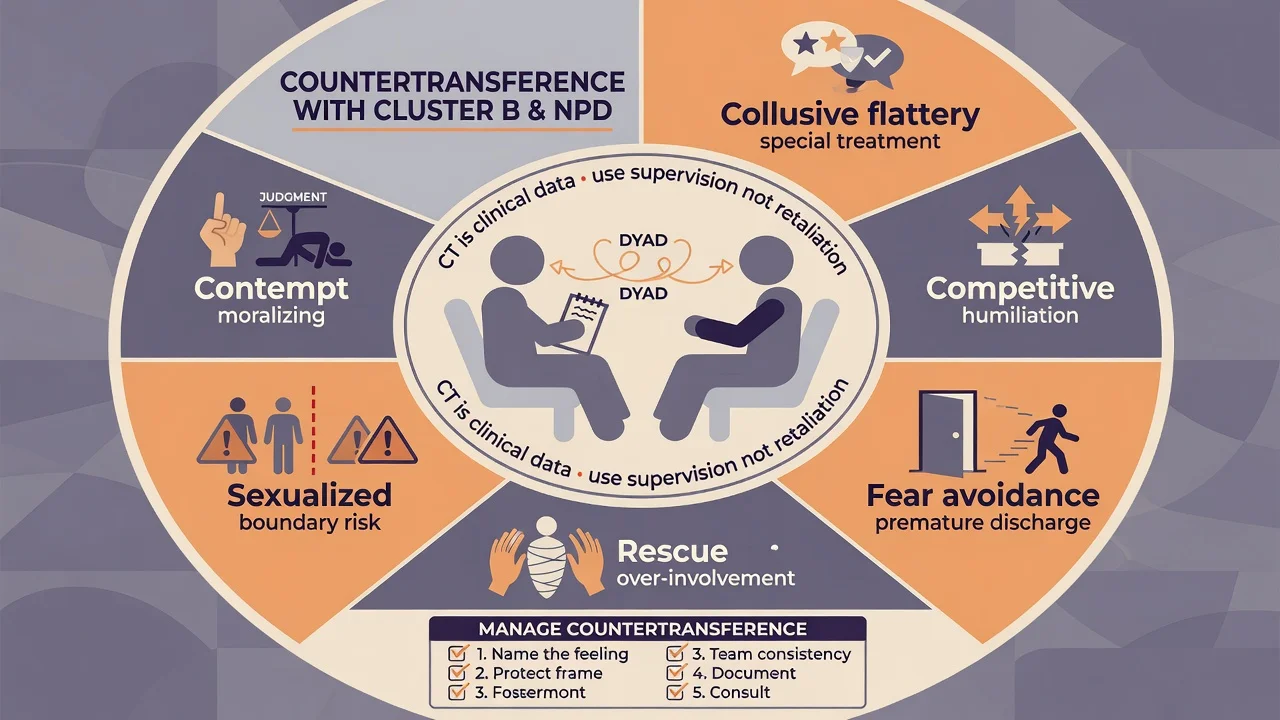
Other classic pitfalls: missing depression and suicide under arrogance; pejorative labelling without formulation; endless polypharmacy; confusing psychopathy construct with casual insult; forensic misuse of diagnosis as pure destiny; ignoring collateral.[3][8][18]
Prognosis and disposition
NPD course is heterogeneous. Some grandiose features attenuate with age and role change; vulnerable depression, relationship failure and occupational collapse often drive later help-seeking. Meaningful change in long-term psychotherapy is possible for engaged patients, with indicators including improved reflective function and less destructive interpersonal patterns — not overnight personality transplant.[10][3]
ASPD natural history includes partial behavioural improvement for some with age, alongside persistent high-risk subgroups with psychopathy traits and substance use. Disposition should match risk and treatable comorbidity rather than the pejorative assumption that “nothing works.” Structured interventions, dual diagnosis care and, where appropriate, forensic frameworks are the realistic ladder.[16][17][19]
HPD diagnoses are often longitudinally unstable; treat functional impairment and the better-validated comorbid pattern you actually find.[13][14]
Special populations
Adolescents. Emerging narcissistic or antisocial traits require developmental formulation. Conduct disorder is the ASPD pathway signal; full adult PD labels need caution but early intervention for aggression, substance use and family patterns should not wait for a birthday.[16][17]
Older adults. Late-onset personality change is organic or mood disease until proven otherwise. Lifelong NPD may present with depression after retirement, widowhood or status loss — assess suicide risk carefully.[8]
Pregnancy, parenting and safeguarding. Exploitative or violent patterns trigger child-protection duties. Coordinate perinatal mental health when mood comorbidity is present; medication decisions follow general perinatal principles for the treated comorbidity, not “NPD pharmacotherapy.”[17]
Cultural formulation. Pride, honour, status hierarchies and help-seeking norms shape what counts as “grandiosity” versus culturally congruent self-presentation. In ANZ practice, Indigenous cultural safety is part of competent care.[3]
High-status patients (including health professionals). Expect pressure for VIP pathways; the clinical intervention is equal frame, not special deals.[5][9]
Evidence, guidelines and controversies
Epidemiology and nosology. Stinson NESARC NPD; Dhawan systematic review of prevalence/treatment; Compton NESARC ASPD–substance comorbidity; Black natural history and update reviews; Patrick psychopathy synthesis.[1][2][15][16][17][18]
Constructs. Pincus pathological narcissism; Caligor clinical challenges; Blagov/Bakkevig HPD validity critiques; psychopathy versus ASPD distinction.[3][4][13][14][18]
Treatment and process. Diamond TFP-N; Crisp/Gabbard psychodynamic principles; Ronningstam change indicators; Blay GPM psychoeducation proposal and emotion-dysregulation review; Bamelis schema therapy multicentre RCT; Fonagy MOAM MBT ASPD trial; Gabbard on narcissism and suicide risk; Betan on countertransference–PD associations.[5][6][7][8][9][10][11][12][19][20]
Controversies to discuss maturely. Whether HPD should remain a category; how fully ICD-11 severity replaces Cluster B boxes; how far specialised BPD therapies generalise to NPD; whether ASPD is “treatable” versus “manageable”; the ethics of working with low-remorse patients who harm others.[13][14][17][19]
Exam pearls
NARCISS — viva checklist
NARCISS
Nosology: DSM Cluster B + ICD-11 severity/traits + grandiose/vulnerable poles
Assess collateral, conduct history, substances, organic red flags
Risk after narcissistic injury — suicide, rage, IPV, safeguarding
Countertransference is data (Betan) — supervise, do not enact
Interventions: frame + TFP-N/schema/psychodynamic/GPM; MBT context in ASPD
Stop disease-modifying drug fantasies; treat comorbidity with review dates
Spectrum overlap with BPD/ASPD/HPD — primary motive + dual diagnosis allowed
60-second oral summary
Cluster B spans NPD, BPD, ASPD and HPD — pedagogical cluster, high trait overlap. NPD is DSM ≥5/9 grandiosity/admiration/empathy pattern, but pathological narcissism also has a vulnerable pole. HPD is a low-validity pointer; ASPD requires conduct history and is not identical to psychopathy. Assess collateral, substances, organic late-onset change, and risk after narcissistic injury. Hold a firm frame; treat countertransference as data. Psychotherapy options include TFP-N, psychodynamic principles, schema therapy RCT support for PDs, GPM-style psychoeducation, and MBT-informed ASPD work (MOAM). No drug cures NPD/HPD/ASPD — treat comorbidity with review dates. Realistic limits plus structured care beats nihilism and collusion.[3][4][5][8][19][20]
References
- [1]Stinson FS, Dawson DA, Goldstein RB, Chou SP, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV narcissistic personality disorder: results from the wave 2 national epidemiologic survey on alcohol and related conditions J Clin Psychiatry, 2008.PMID 18557663
- [2]Dhawan N, Kunik ME, Oldham J, Coverdale J Prevalence and treatment of narcissistic personality disorder in the community: a systematic review Compr Psychiatry, 2010.PMID 20579503
- [3]Caligor E, Levy KN, Yeomans FE Narcissistic personality disorder: diagnostic and clinical challenges Am J Psychiatry, 2015.PMID 25930131
- [4]Pincus AL, Lukowitsky MR Pathological narcissism and narcissistic personality disorder Annu Rev Clin Psychol, 2010.PMID 20001728
- [5]Betan E, Heim AK, Zittel Conklin C, Westen D Countertransference phenomena and personality pathology in clinical practice: an empirical investigation Am J Psychiatry, 2005.PMID 15863790
- [6]Diamond D, Yeomans F, Keefe JR Transference-Focused Psychotherapy for Pathological Narcissism and Narcissistic Personality Disorder (TFP-N) Psychodyn Psychiatry, 2021.PMID 34061655
- [7]Diamond D, Yeomans F, Stern B, Kernberg OF Transference-Focused Psychotherapy for Narcissistic Personality Disorder: An Object Relations Approach J Pers Disord, 2020.PMID 32186988
- [8]Gabbard GO Narcissism and suicide risk Ann Gen Psychiatry, 2022.PMID 35065658
- [9]Crisp H, Gabbard GO Principles of Psychodynamic Treatment for Patients With Narcissistic Personality Disorder J Pers Disord, 2020.PMID 32186987
- [10]Ronningstam E Narcissistic Personality Disorder: Patterns, Processes, and Indicators of Change in Long-Term Psychotherapy J Pers Disord, 2023.PMID 37367820
- [11]Blay M, Duarte M, Benmakhlouf I, et al. Psychoeducation for Pathologic Narcissism and Narcissistic Personality Disorder: A Review and Proposal for a Good Psychiatric Management-based Six-week Intervention J Psychiatr Pract, 2024.PMID 39058523
- [12]Blay M, Duarte M, et al. Association between Pathological Narcissism and Emotion Dysregulation: A Systematic Review Psychopathology, 2024.PMID 38870915
- [13]Blagov PS, Westen D Questioning the coherence of histrionic personality disorder: borderline and hysterical personality subtypes in adults and adolescents J Nerv Ment Dis, 2008.PMID 19008729
- [14]Bakkevig JF, Karterud S Is the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, histrionic personality disorder category a valid construct? Compr Psychiatry, 2010.PMID 20728002
- [15]Compton WM, Conway KP, Stinson FS, Colliver JD, Grant BF Prevalence, correlates, and comorbidity of DSM-IV antisocial personality syndromes and alcohol and specific drug use disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions J Clin Psychiatry, 2005.PMID 15960559
- [16]Black DW The Natural History of Antisocial Personality Disorder Can J Psychiatry, 2015.PMID 26175389
- [17]Black DW Update on Antisocial Personality Disorder Curr Psychiatry Rep, 2024.PMID 39230801
- [18]Patrick CJ Psychopathy: Current Knowledge and Future Directions Annu Rev Clin Psychol, 2022.PMID 35119947
- [19]Fonagy P, Simes E, Yirmiya K, et al. Mentalisation-based treatment for antisocial personality disorder in males convicted of an offence on community probation in England and Wales (Mentalization for Offending Adult Males; MOAM): a multicentre, assessor-blinded, randomised controlled trial Lancet Psychiatry, 2025.PMID 39978982
- [20]Bamelis LL, Evers SM, Spinhoven P, Arntz A Results of a multicenter randomized controlled trial of the clinical effectiveness of schema therapy for personality disorders Am J Psychiatry, 2014.PMID 24322378