Psych · General adult psychiatry — psychosis
Negative and cognitive symptoms of schizophrenia
Also known as Deficit syndrome · Primary negative symptoms · Secondary negative symptoms · Avolition-apathy · Diminished expression · Schizophrenia neurocognition · MATRICS cognitive domains
Exam-exhaustive fellowship reference on negative and cognitive symptoms of schizophrenia — primary versus secondary negatives, deficit syndrome, SANS/PANSS and NIMH domains, MATRICS cognition, functional outcome, limited pharmacotherapy evidence with careful cariprazine and clozapine nuance, cognitive remediation, and psychosocial rehabilitation. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Negative and cognitive domains are high-yield fellowship topics because examiners test whether you can stop calling every quiet patient "negative", prove secondary causes, name scales and domains, link cognition to function, and avoid marketing folklore about drugs that mainly treat positives. Broader psychosis care, TRS pathways, and clozapine monitoring minutiae live in linked topics; this leaf is self-sufficient for negative and cognitive mastery.[2][3][16]
Overview and definition
Negative symptoms are reductions or absences of normal emotional expression, speech productivity, motivation, pleasure, and social drive — not the presence of delusions or hallucinations.[2][3] The NIMH-MATRICS consensus framed five domains examiners expect by name: blunted affect, alogia, asociality, anhedonia, and avolition.[1]
Cognitive impairment in schizophrenia is multi-domain neurocognitive deficit relative to expected ability (often from premorbid or first-episode stages), spanning processing speed, attention/vigilance, working memory, learning, reasoning, and social cognition — it is not the same construct as intellectual disability or progressive dementia, though those differentials matter clinically.[9][10]
DSM-5-TR and ICD-11 incorporate negative features within schizophrenia spectrum diagnosis and description; they do not create a freestanding "negative symptom disorder" code. Exam language remains dimensional and measurement-based.[2][16]
Classification and staging
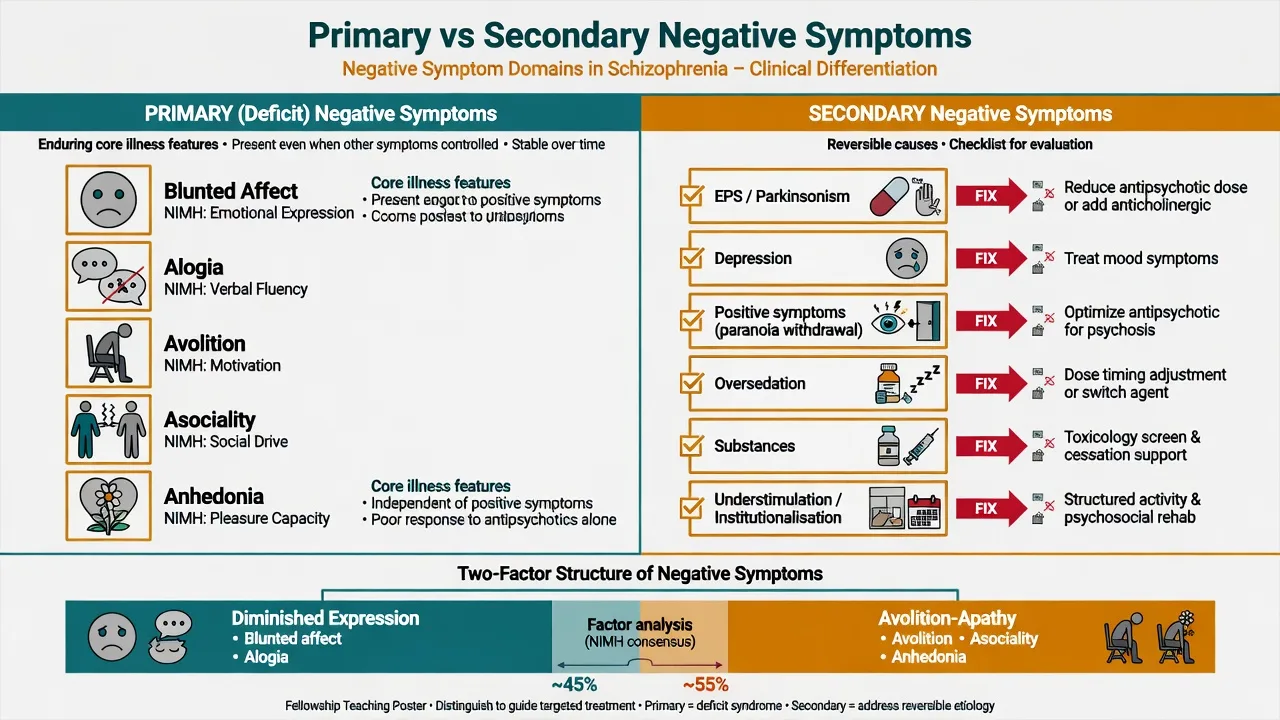
Primary negatives
- Core illness features
- Often enduring (deficit concept)
- Persist when positives controlled
- Poorly responsive to pure D2 blockade
Secondary negatives
- EPS / drug-induced akinesia
- Depression / demoralisation
- Paranoia-driven withdrawal
- Sedation, substances, understimulation
Deficit syndrome
- Carpenter concept
- Primary enduring negatives
- Stable trait-like pattern
- Distinct functional trajectory
Two-factor structure
- Diminished expression
- Avolition–apathy / motivation–pleasure
- Different outcome links
- Guides assessment focus
Primary versus secondary is the single most important clinical fork. Secondary negatives improve when you treat the driver; primary (including deficit syndrome) require honest prognosis plus rehabilitation-heavy plans.[3][4] Factor analyses support at least two negative dimensions: diminished expression and avolition–apathy, with differential functional prediction.[7][8]
Deficit versus non-deficit schizophrenia (Carpenter) separates primary enduring negatives from more state-related patterns — useful for research and for examiners who ask "what is deficit syndrome?" without inventing uncited prevalence numbers.[4]
Epidemiology and risk factors
Numbers and signals examiners expect
Clinically significant negative symptoms are common in schizophrenia and strongly associated with disability, unemployment, social isolation, and carer burden.[2][3] Cognitive impairment is likewise highly prevalent and often present early; it tends to be more stable than fluctuating positive symptoms and is a major driver of functional outcome.[9][10] Predictors of heavier negative burden include male sex, earlier onset, poorer premorbid function, and a deficit-type phenotype in classical descriptions — state these as teaching associations, not absolute rules.[3][4]
Pathophysiology and mechanisms
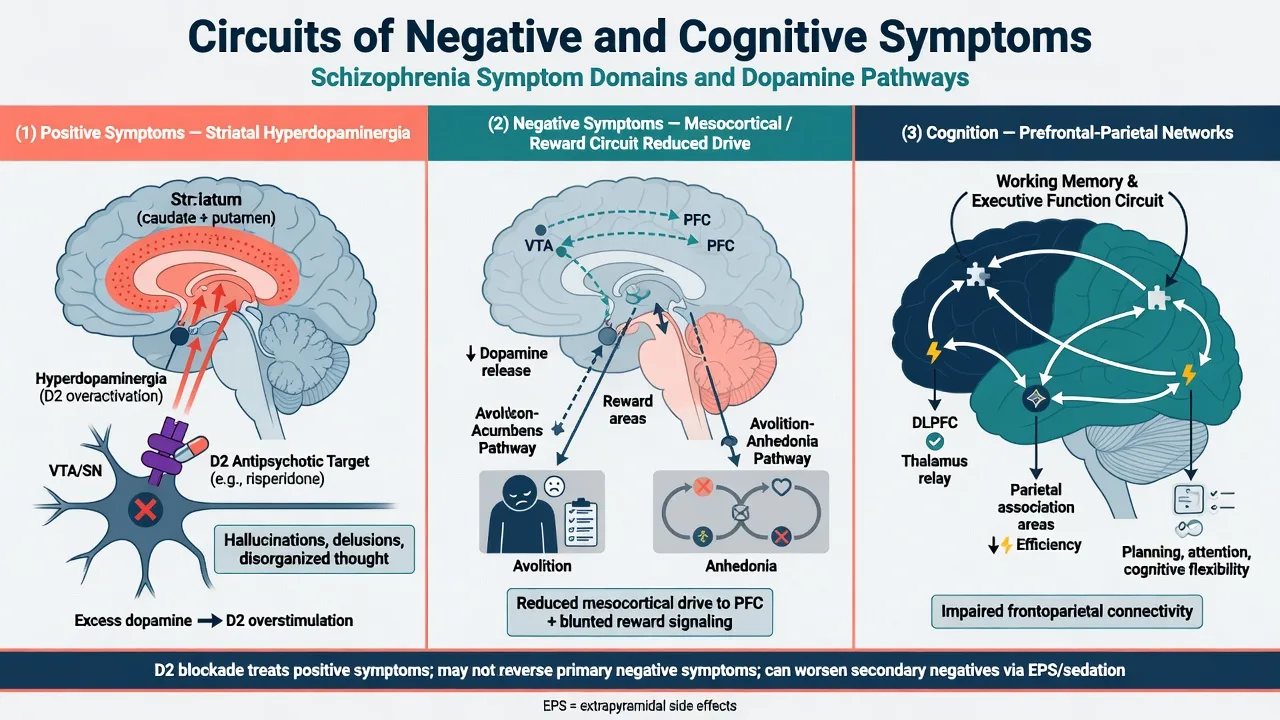
Dopamine hypothesis version III frames striatal hyperdopaminergia as a final common pathway for positive symptoms and D2-blocker response. Negative and cognitive domains map more convincingly onto mesocortical, reward-circuit, and prefrontal–parietal dysfunction, with glutamatergic contributions often discussed in research models.[18][3] Exam use: explain why pure D2 blockade treats voices and paranoia more reliably than primary avolition, and why high D2 occupancy or EPS can create secondary blunting and akinesia that look like negatives.[11][18]
Reward-processing and anticipatory pleasure deficits help explain avolition–anhedonia clusters; working memory and executive dysfunction track prefrontal network impairment relevant to MATRICS domains.[8][10] Social understimulation, poverty, and exclusion amplify secondary functional loss even when core biology is stable.[16]
Clinical presentation
Diminished expression. Reduced facial expression, gesture, and vocal prosody; alogia with sparse content; preserved consciousness and orientation distinguish this from delirium.[1][2]
Avolition–apathy and related domains. Reduced initiation of goal-directed activity, abandoned hygiene and goals, asociality, and anhedonia (teach consummatory versus anticipatory pleasure when asked). Patients are often mislabelled as lazy — correct that stigma in viva language.[1][8]
Cognitive presentation. Slowed processing, distractibility, working-memory failure (cannot hold multi-step plans), learning inefficiency, poor problem-solving, and social-cognition errors (misreading intent) that sabotage rehabilitation and employment.[9][10]
High-stakes faces. Silent severe self-neglect; suicide risk under flat affect; capacity questions about self-care, finances, and housing; TRS multi-domain non-recovery when positives persist alongside deep negatives.[16][17]
Differential diagnosis
Depression
- Mood congruence and guilt
- Diurnal variation teaching points
- Active suicidal ideation
- May respond to antidepressant strategy
EPS / drug effects
- Bradykinesia vs blunted affect
- Akathisia misread as agitation
- Sedation and anticholinergic fog
- Reduce dose / switch / anticholinergic carefully
Organic / neuro
- Progressive decline atypical
- Focal signs, seizure, late onset
- Hypothyroid, B12, autoimmune
- Image / investigate on red flags
Neurodevelopmental
- Autism social-communication pattern
- Lifelong trajectory before psychosis
- ID dual diagnosis baseline
- Do not equate ID with schizophrenia cognition
Discriminators beat lists. Depression can mimic avolition and anhedonia; EPS can mimic blunting; paranoia can produce "asociality" that is fear, not primary deficit; progressive dementia in later life is not residual schizophrenia until proven otherwise.[3][16]
Clinical and bedside assessment
Structure the interview: timeline of negatives versus positives and medication changes; premorbid function; typical day (activity schedule); pleasure and motivation; social contact; cognitive complaints from patient and collateral; risk (suicide, self-neglect, vulnerability); capacity for self-care and finances.[2][16]
MSE. Document affect range and reactivity, speech quantity, spontaneous movement, self-care, motivation examples, insight into deficits, and cognitive bedside screen (orientation, attention, short-term memory, abstract reasoning) with limits acknowledged.[6]
Scales examiners name
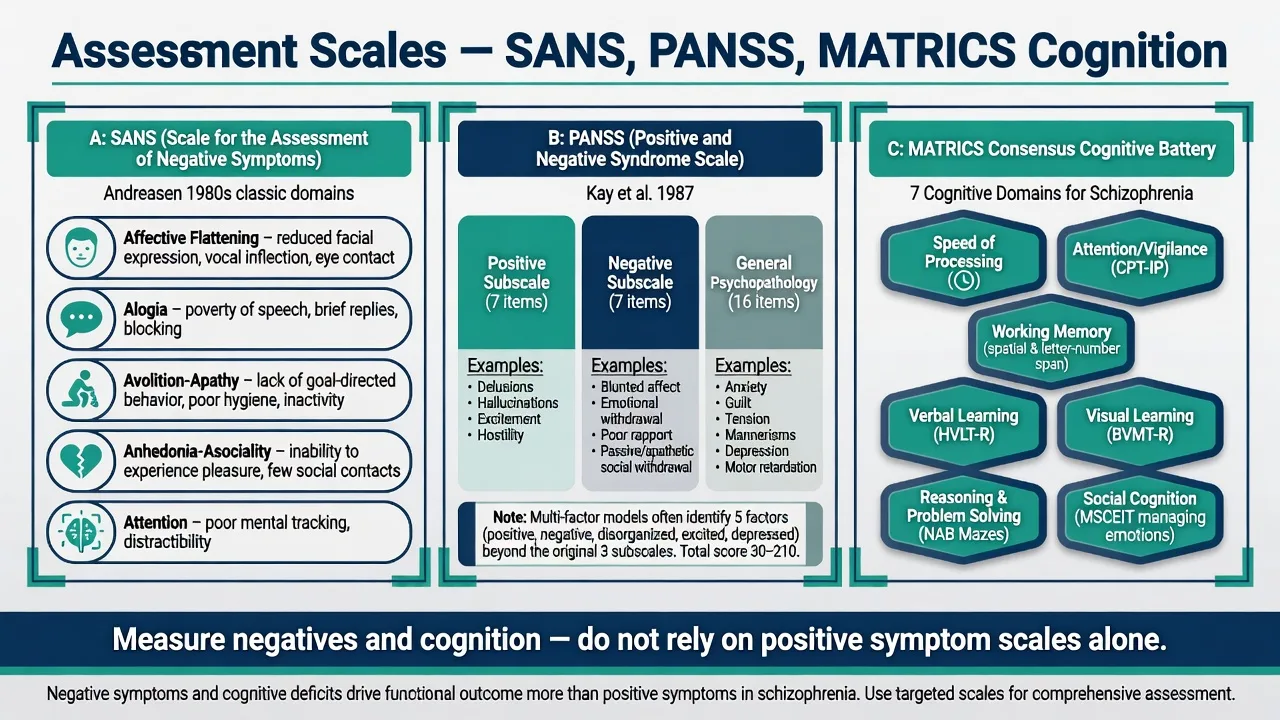
- SANS (Andreasen): classic detailed negative symptom assessment with conceptual foundations examiners still cite.[5]
- PANSS (Kay): Positive, Negative, and General psychopathology subscales; multi-factor models refine negative items in research use.[6]
- Modern negative interviews (for example BNSS/CAINS conceptual mention in advanced answers) refine expression versus motivation–pleasure without inventing uncited scoring rules.[2][7]
- MATRICS Consensus Cognitive Battery domains structure what "cognition" means for trials and specialist testing: speed of processing, attention/vigilance, working memory, verbal learning, visual learning, reasoning/problem-solving, social cognition.[10]
- Function and CGI remain essential — scale change without life change is incomplete success.[9][16]
Investigations
Baseline medical panel when changing treatment or excluding mimics: FBC, U&E, LFT, glucose/HbA1c, lipids, TSH, B12/folate as indicated, pregnancy test when relevant, urine drug screen when substances plausible. Review the medication chart for high EPS-risk agents, anticholinergic load, and polypharmacy sedation. Neuroimaging, EEG, or further organic work-up for progressive cognitive decline, new focal signs, seizures, or late atypical presentations — not automatic for every stable residual negative syndrome without red flags.[16][17]
Management — acute risk and resuscitation
Catatonia and NMS can be misread as extreme blunting or immobility — use medical emergency pathways. Legal status follows capacity, risk, and jurisdiction-specific Mental Health Act principles; do not invent section numbers.[16]
Management — definitive and stepwise
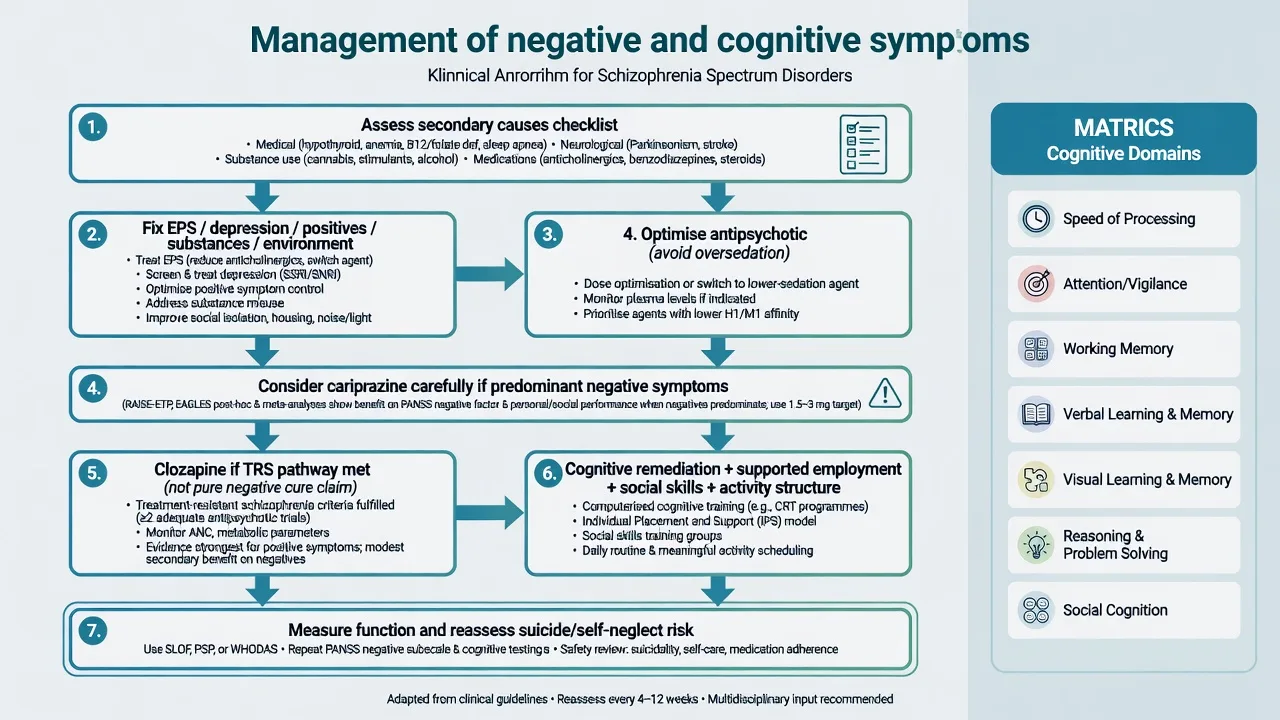
Step 1 — Treat secondary causes first (highest yield)
Optimise or switch antipsychotics if EPS or oversedation dominate; treat depression when present; control residual positives that drive withdrawal; address substances; enrich environment and structure activity; reduce anticholinergic cognitive toxicity when safe.[2][3][11]
Step 2 — Pharmacotherapy honesty
Meta-analytic synthesis of many randomised trials for negative symptoms shows generally small effects across modalities — interpret marketing claims critically and set realistic expectations with patients and families.[11] Antipsychotics primarily treat positive symptoms; any negative-domain change may partly reflect secondary-cause improvement rather than true primary-negative reversal.[11][16]
Cariprazine nuance (cite carefully). Németh and colleagues compared cariprazine versus risperidone monotherapy in patients with predominant negative symptoms of schizophrenia in a randomised double-blind trial and reported greater improvement on negative symptom measures with cariprazine in that specific design and population. Exam answer: name the trial phenotype (predominant negatives, controlled positives context), the comparator, and that this is not a licence to claim cariprazine cures all primary deficit syndromes or replaces rehabilitation. Local formulary, indication, and product information govern prescribing; adult oral dosing follows approved titration (commonly start low, for example 1.5 mg orally daily, titrate as tolerated per product information — always confirm current local label and monitoring).[12]
Clozapine nuance (cite carefully). Kane established clozapine superiority in rigorously defined treatment-resistant schizophrenia, primarily framed around overall and positive-symptom non-response. Clozapine may help some multi-domain non-recovery in TRS, but do not market it as a proven, specific primary-negative-symptom cure; use the TRS pathway when TRRIP-style criteria are met and monitoring is real (see dedicated TRS and clozapine topics).[13][16]
Other agents. Antidepressant augmentation for co-morbid depression is clinically rational when depression is the secondary driver. Glutamatergic experimental strategies have a mixed-to-negative history in key cognitive/negative trials — do not overclaim failed or weak pipelines in exams.[11] Avoid stacking high-dose antipsychotics solely for primary negatives.
Step 3 — Cognitive remediation and psychosocial care
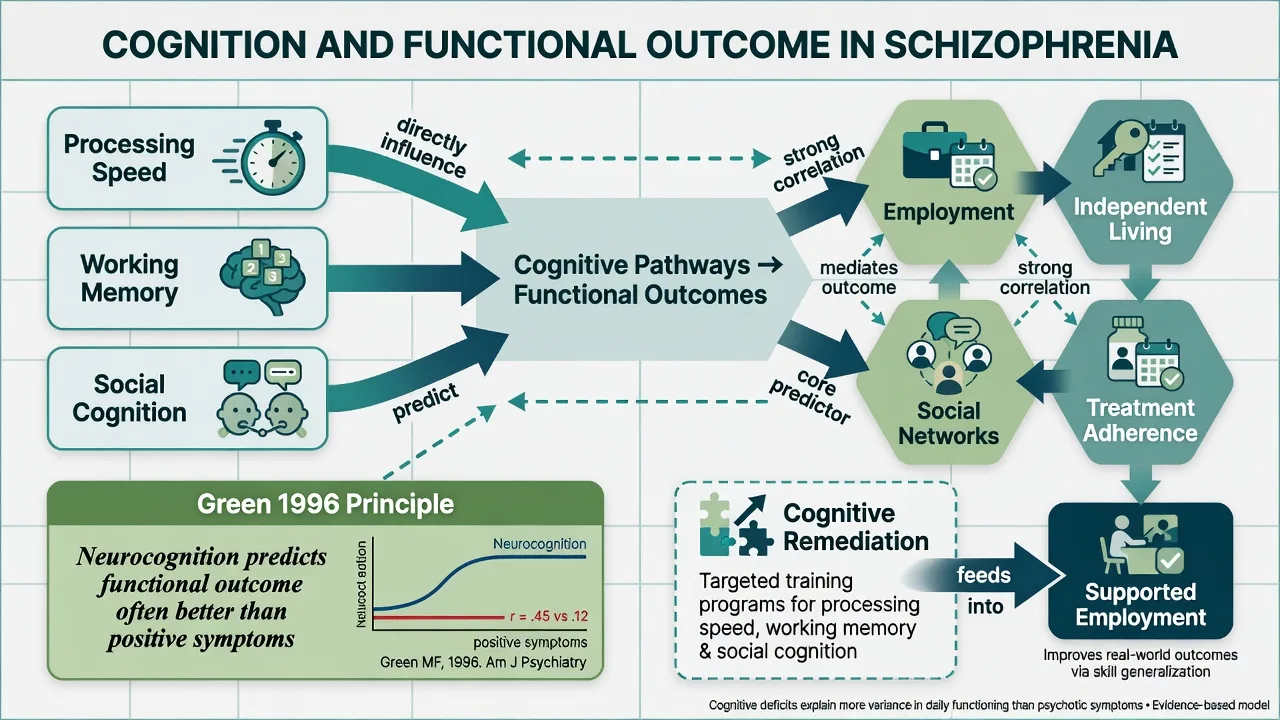
Cognitive remediation has meta-analytic support for cognitive gains, with effect sizes and functional transfer improved when programmes include active strategy coaching and are linked to psychosocial rehabilitation rather than drill-only computer tasks.[14][15] Wykes and colleagues quantified methodology and effect sizes; Vita and colleagues synthesised effectiveness, core elements, and moderators in a large randomised-trial meta-analysis.[14][15]
Psychosocial package. Supported employment (Individual Placement and Support models), social skills training, structured behavioural activation principles for avolition, family psychoeducation, CBTp for residual positives, housing support, and day programmes. RANZCP and APA guidance frame psychosocial interventions as core schizophrenia care, not optional decoration.[16][17]
Regional guideline deltas
RANZCP schizophrenia guidelines emphasise physical health, psychosocial packages, early intervention, and realistic multi-domain recovery goals within Australian and New Zealand service models. Use measurement-based care and avoid stigma language that blocks rehabilitation funding.[16]
Specific subtypes and scenarios
Deficit syndrome / primary enduring negatives. Stable primary pattern; prioritise environment, structure, remediation, and honest prognosis; avoid endless high-dose antipsychotic stacking.[4]
Predominant negatives with controlled positives. Closest phenotype to specialised pharmacological trials such as Németh; still run secondary-cause checklist and rehabilitation in parallel.[12]
First-episode with early cognitive impairment. Early vocational/educational support and cognitive remediation principles; avoid oversedation that worsens cognition.[10][16]
Chronic institutional understimulation. Treat as secondary until proven otherwise — activity programmes and community placement can reverse pseudo-negatives.[3]
TRS multi-domain non-recovery. Apply TRRIP/clozapine logic for positives/resistance; still use remediation for cognition and do not expect clozapine alone to restore employment.[13][15]
Older adults. Exclude evolving dementia and medical causes; fall risk and anticholinergic cognitive toxicity matter.[16]
Complications and pitfalls
Classic viva failures: increasing risperidone for primary avolition without checking EPS; declaring "no treatment exists" and discharging without remediation or employment support; confusing intellectual disability with schizophrenia-related cognitive impairment.[9][14]
Prognosis and disposition
Neurocognitive deficits are among the strongest predictors of functional outcome in schizophrenia — often more than residual positive symptoms alone.[9] Primary negatives and untreated secondary causes both predict poor social and occupational recovery.[8][3] Disposition ladder: outpatient CMHT with rehabilitation focus → day programmes → supported employment → intensive outreach for self-neglect → inpatient when risk or capacity thresholds are met under local law → supported accommodation. Communicate realistic hope: function can improve even when some primary deficits persist if secondary causes are fixed and rehabilitation is active.[15][16]
Special populations
Youth / EIS
- Early cognitive and vocational support
- Avoid oversedating first choices when possible
- Family engagement
- Substance formulation
Older adults
- Exclude dementia and medical mimics
- Falls and anticholinergic load
- Lower sedation goals
- Caregiver capacity
Pregnancy
- Self-care capacity for infant
- Specialist perinatal psychiatry
- Risk–benefit of untreated multi-domain illness
- Rehabilitation-compatible plans
Cultural safety
- Reserved affect may be normative
- Interpreters and collateral
- Do not pathologise cultural silence
- FRANZCP cultural safety expectations
State population-specific secondary-cause risks explicitly at viva.[16][17]
Evidence, guidelines and controversies
Landmark pillars: Kirkpatrick NIMH-MATRICS negative consensus;[1] Marder and Galderisi conceptualisation reviews;[2][3] Carpenter deficit syndrome;[4] SANS and PANSS;[5][6] two-factor structure (Blanchard, Strauss);[7][8] Green functional consequences of neurocognition;[9] Nuechterlein MATRICS battery;[10] Fusar-Poli treatments meta-analysis;[11] Németh cariprazine predominant-negatives RCT;[12] Kane clozapine TRS context;[13] Wykes and Vita cognitive remediation meta-analyses;[14][15] RANZCP 2016 and APA 2020 guidelines;[16][17] Howes–Kapur dopamine framework.[18]
Controversies to handle calmly: how much of antipsychotic "negative symptom benefit" is secondary-cause removal; generalisability of predominant-negatives drug trials; access equity for cognitive remediation and supported employment; and the risk of therapeutic nihilism versus over-promising drugs.[11][12][15]
Exam pearls
SECONDARY
SECONDARY is a memory scaffold for the negative-symptom reassessment sequence — still complete full risk and capacity assessment.[2][3][16]
References
- [1]Kirkpatrick B, Fenton WS, Carpenter WT Jr, et al. The NIMH-MATRICS consensus statement on negative symptoms Schizophr Bull, 2006.PMID 16481659
- [2]Marder SR, Galderisi S The current conceptualization of negative symptoms in schizophrenia World Psychiatry, 2017.PMID 28127915
- [3]Galderisi S, Mucci A, Buchanan RW, et al. Negative symptoms of schizophrenia: new developments and unanswered research questions Lancet Psychiatry, 2018.PMID 29602739
- [4]Carpenter WT Jr, Heinrichs DW, Wagman AM Deficit and nondeficit forms of schizophrenia: the concept Am J Psychiatry, 1988.PMID 3358462
- [5]Andreasen NC The Scale for the Assessment of Negative Symptoms (SANS): conceptual and theoretical foundations Br J Psychiatry Suppl, 1989.PMID 2695141
- [6]Kay SR, Fiszbein A, Opler LA The positive and negative syndrome scale (PANSS) for schizophrenia Schizophr Bull, 1987.PMID 3616518
- [7]Blanchard JJ, Cohen AS The structure of negative symptoms within schizophrenia: implications for assessment Schizophr Bull, 2006.PMID 16254064
- [8]Strauss GP, Horan WP, Kirkpatrick B, et al. Deconstructing negative symptoms of schizophrenia: avolition-apathy and diminished expression clusters predict clinical presentation and functional outcome J Psychiatr Res, 2013.PMID 23453820
- [9]Green MF What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry, 1996.PMID 8610818
- [10]Nuechterlein KH, Green MF, Kern RS, et al. The MATRICS Consensus Cognitive Battery, part 1: test selection, reliability, and validity Am J Psychiatry, 2008.PMID 18172019
- [11]Fusar-Poli P, Papanastasiou E, Stahl D, et al. Treatments of Negative Symptoms in Schizophrenia: Meta-Analysis of 168 Randomized Placebo-Controlled Trials Schizophr Bull, 2015.PMID 25528757
- [12]Németh G, Laszlovszky I, Czobor P, et al. Cariprazine versus risperidone monotherapy for treatment of predominant negative symptoms in patients with schizophrenia: a randomised, double-blind, controlled trial Lancet, 2017.PMID 28185672
- [13]Kane J, Honigfeld G, Singer J, et al. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine Arch Gen Psychiatry, 1988.PMID 3046553
- [14]Wykes T, Huddy V, Cellard C, et al. A meta-analysis of cognitive remediation for schizophrenia: methodology and effect sizes Am J Psychiatry, 2011.PMID 21406461
- [15]Vita A, Barlati S, Ceraso A, et al. Effectiveness, Core Elements, and Moderators of Response of Cognitive Remediation for Schizophrenia: A Systematic Review and Meta-analysis of Randomized Clinical Trials JAMA Psychiatry, 2021.PMID 33877289
- [16]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [17]Keepers GA, Fochtmann LJ, Anzia JM, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia Am J Psychiatry, 2020.PMID 32867516
- [18]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164