Psych · General adult psychiatry — OCRD
Obsessive-compulsive disorder
Also known as OCD · Obsessive compulsive disorder · Obsessional neurosis · Exposure and response prevention · ERP · Y-BOCS · OCRD · Treatment-refractory OCD
Exam-exhaustive fellowship reference on obsessive-compulsive disorder — DSM-5-TR and ICD-11 criteria and OCRD context; Y-BOCS; differentials (OCPD, psychosis, ASD, BDD); CSTC model; CBT/ERP first-line; high-dose SSRI and clomipramine; antipsychotic augmentation; deep TMS and neurosurgery pathway; PANDAS/PANS exam nuance. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
12 MCQs with explanations
Target exams
Red flags
Obsessive-compulsive disorder (OCD) is a high-yield general adult and child-interface fellowship topic. FRANZCP MEQs demand named first-line psychological and pharmacological plans with doses and duration. MRCPsych CASCs test explanation of ERP and medication to patients and families. ABPN items test Y-BOCS concept, high-dose SSRI logic, and refractory algorithms. A candidate who reads only this topic should defend diagnosis, differential, and stepped care at consultant depth.[8][9][17]
Overview and definition
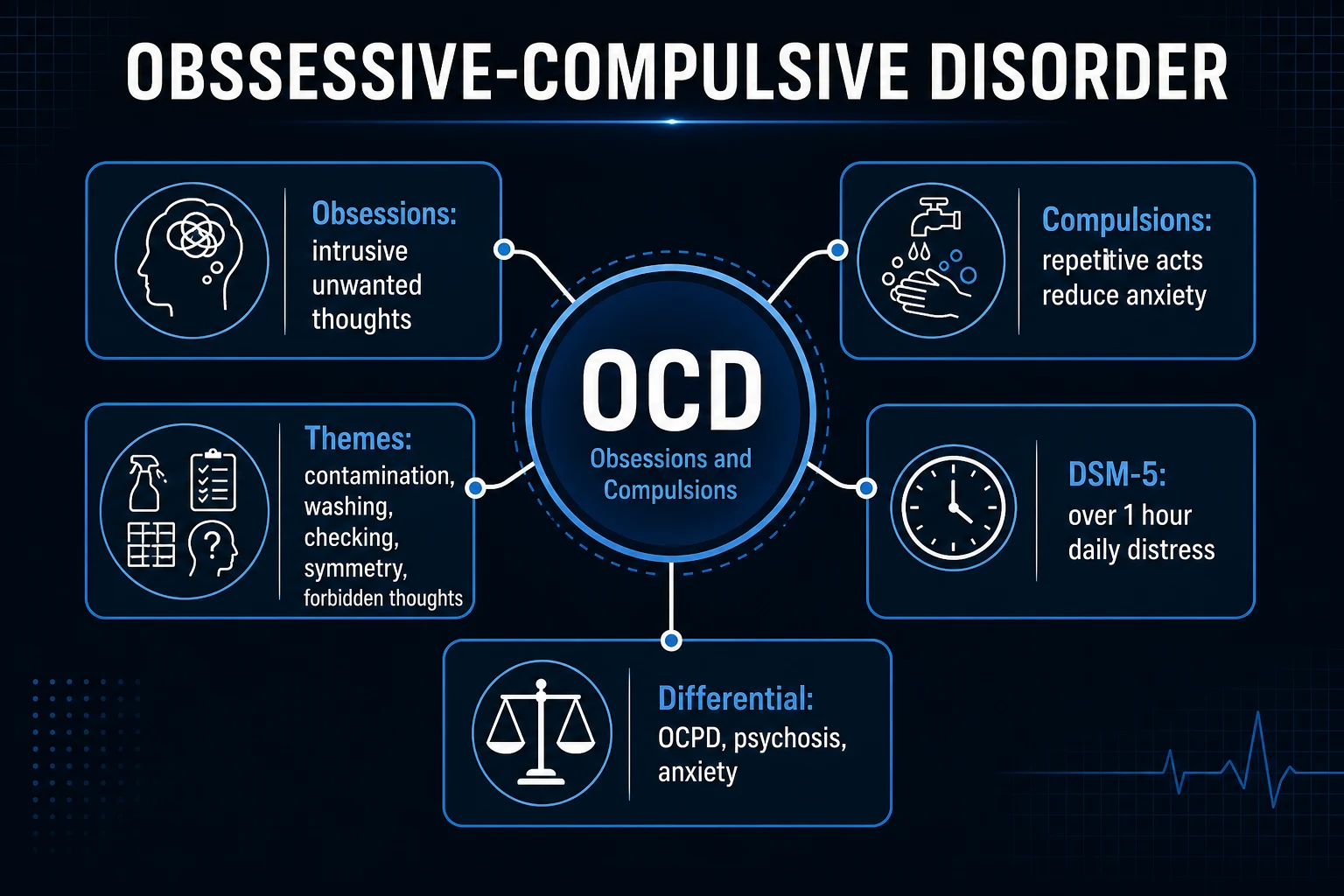
OCD is defined by obsessions (recurrent, intrusive, unwanted thoughts, images or urges that cause marked anxiety or distress) and/or compulsions (repetitive behaviours or mental acts the person feels driven to perform to neutralise distress or prevent a dreaded event), that are time-consuming or cause clinically significant impairment, and are not better explained by another mental disorder, substance, or medical condition.[8][9]
Clinical essence for viva. Obsessions are typically ego-dystonic (experienced as intrusive and not simply valued goals). Compulsions are maintained by negative reinforcement — short-term anxiety reduction that strengthens the ritual and prevents disconfirmation of the fear. Covert mental rituals (praying, counting, reviewing) count as compulsions even when no one can see them.[9][19]
DSM-5-TR placement. OCD sits in the obsessive-compulsive and related disorders (OCRD) chapter, not the anxiety disorders chapter. Related disorders include body dysmorphic disorder (BDD), hoarding disorder, trichotillomania, and excoriation disorder. Insight is specified (good/fair; poor; absent insight/delusional beliefs). A tic-related specifier is available when a current or past tic disorder is present.[9][17]
ICD-11. OCD is classified among obsessive-compulsive or related disorders with similar core features; always state which manual you are using when duration language or related-disorder boundaries are examined.[9]
Classic teaching threshold: symptoms often occupy more than 1 hour per day, though impairment can qualify at lower absolute time if severity is high.[8][9]
Classification and symptom dimensions
Content dimensions
- Contamination / washing and cleaning
- Harm / checking and reassurance
- Symmetry / ordering / counting
- Forbidden thoughts (aggressive, sexual, religious/scrupulosity)
- Mental rituals and pure mental neutralising
Insight specifier
- Good or fair insight: knows beliefs may be excessive
- Poor insight: thinks beliefs are probably true
- Absent insight / delusional beliefs: convinced
- Does not automatically equal schizophrenia
OCRD neighbours
- BDD — appearance preoccupation
- Hoarding — difficulty discarding, clutter
- Trichotillomania / excoriation — body-focused repetitive behaviours
- Shared features ≠ same first-line ERP targets
Course patterns
- Childhood/adolescent onset common
- Often chronic-waxing without treatment
- Tic-related OCD subset
- Perinatal exacerbation possible
Symptom dimensions guide the ERP hierarchy (what is exposed and which responses are prevented) more than they create separate diseases. Comorbidity with depression, other anxiety disorders, tics, and OCPD traits is common and must be formulated, not ignored.[2][9]
Epidemiology and risk factors
Headline epidemiology (exam numbers)
In the National Comorbidity Survey Replication, OCD was uncommon but highly impairing, with substantial lifetime comorbidity and frequent delayed treatment contact after onset.[2] Genetic liability is well established from family and twin studies; genome-wide analyses show complex polygenic architecture rather than a single gene.[15][20]
Risk and burden factors examiners expect: first-degree family history, early adversity, comorbid tics, longer untreated duration, and secondary depression with elevated suicide risk. Functional costs include education interruption, occupational disability, relationship strain, and family accommodation (relatives performing rituals or providing reassurance), which maintains the disorder.[2][9]
Pathophysiology
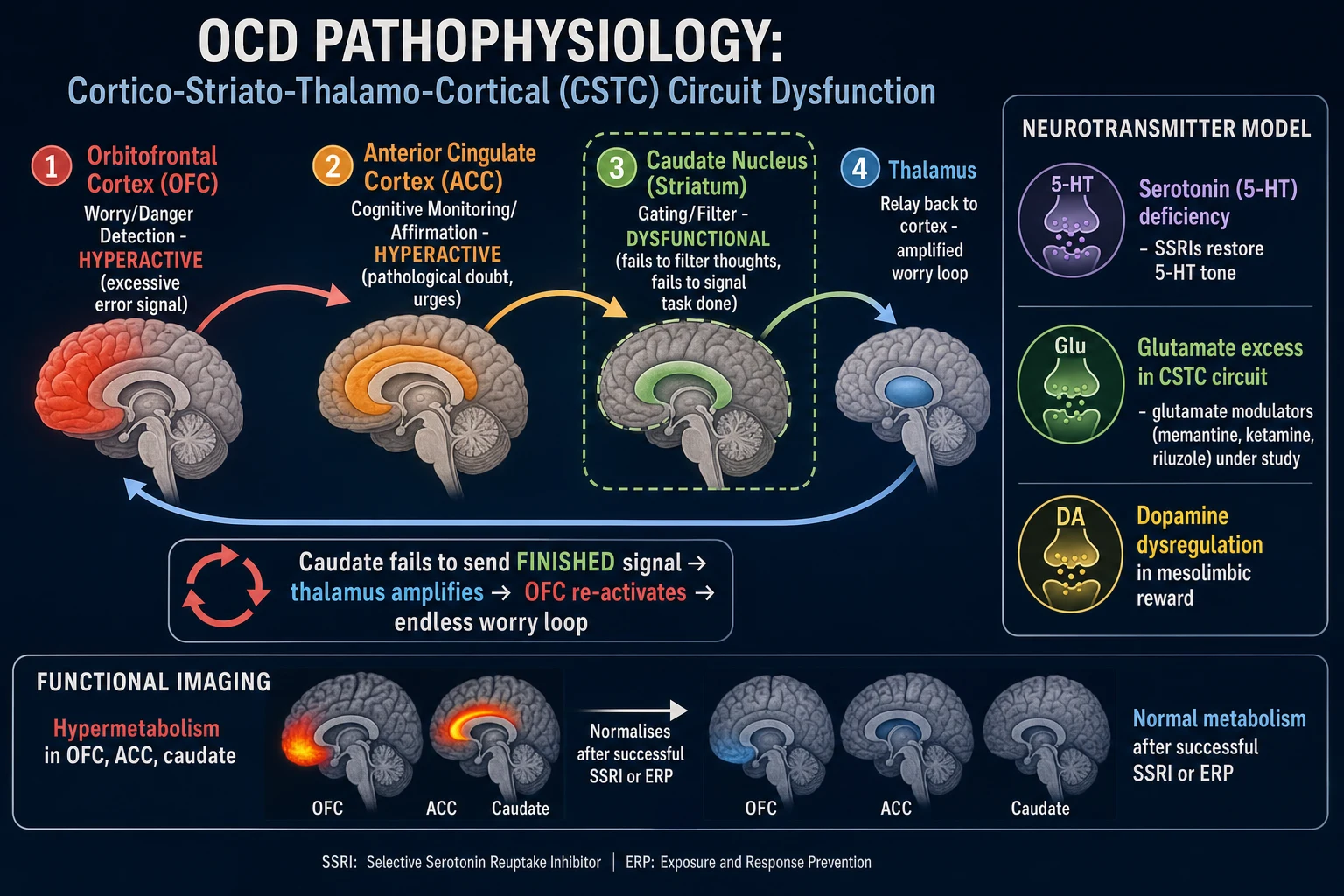
CSTC model (viva-ready). Dysfunction in cortico-striato-thalamo-cortical loops — classically orbitofrontal cortex, anterior cingulate, striatum (including caudate), and thalamus — is the dominant circuit framing. Group-level functional imaging may show hyperactivity in these nodes that can reduce with successful SSRI or ERP treatment. State clearly: imaging does not diagnose OCD in clinic.[9][14]
Serotonin. SSRIs and clomipramine (a potent serotonin reuptake inhibitor among TCAs) are effective, supporting serotonergic pharmacology as a treatment model — not proof of a simple “serotonin deficiency.” Response is often delayed and dose-dependent at higher ranges than typical depression doses.[4][5][14]
Dopamine and glutamate. Low-dose antipsychotic augmentation for SRI-resistant OCD implicates dopaminergic modulation. Glutamatergic agents have been studied experimentally; they are not first-line exam answers for routine care.[6][14]
Psychological models that change therapy. Inflated responsibility, thought–action fusion, over-importance of thoughts, and intolerance of uncertainty maintain checking and mental rituals. Compulsions are negatively reinforced. ERP works by exposure without neutralising, allowing habituation and belief updating.[13][19]
Clinical presentation
Core MSE language: intrusive ego-dystonic thoughts (e.g. “I might have hit someone with the car”), mounting anxiety, ritualised checking or washing, and temporary relief followed by return of doubt. Time occupied, avoidance (not touching “contaminated” objects, not driving), and reassurance-seeking are part of the syndrome.[9]
Atypical and high-yield presentations. Primarily obsessional OCD with mental rituals only (“pure O” is a clinical descriptor, not a separate DSM diagnosis). Religious scrupulosity and sexual-orientation or harm obsessions in people who find the content abhorrent. Late-onset first presentation needs organic exclusion. Perinatal onset or exacerbation is examinable. Cultural content of obsessions varies; the structure (intrusion–anxiety–ritual) remains.[9][17]
Insight spectrum. Good insight is classic teaching, but poor or delusional insight occurs and still can be OCD if the content and ritual structure fit — distinguish carefully from primary psychotic disorders.[9]
Differential diagnosis
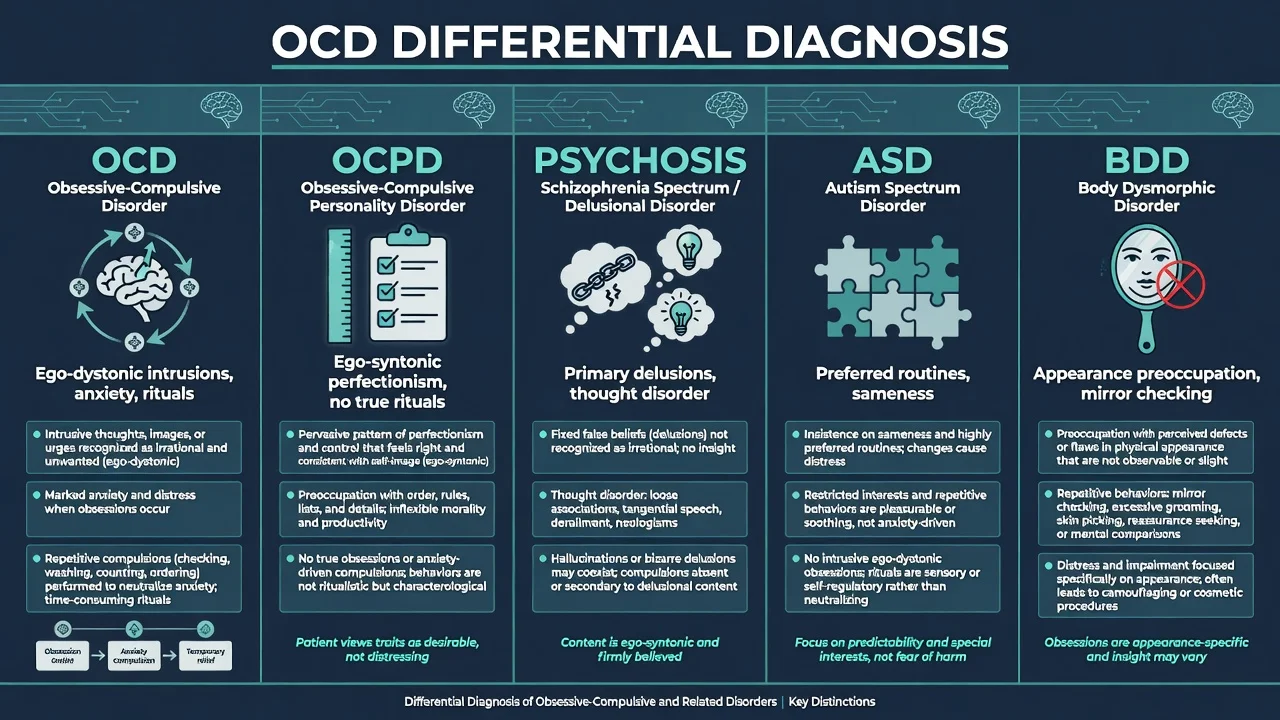
OCPD
- Ego-syntonic perfectionism, rigidity, control
- No true intrusive obsessions or anxiety-driven rituals
- Patient values orderliness as identity
- Can co-occur with OCD — treat both when present
Psychosis
- Primary delusions/hallucinations, thought disorder
- Bizarre content without OCD ritual structure
- OCD with absent insight still has compulsive logic
- Antipsychotic monotherapy is not OCD first-line
ASD routines
- Restricted interests often preferred, soothing
- Sameness for regulation rather than neutralising dread
- Can co-occur — adapt ERP carefully
- Do not pathologise all repetitive behaviour
BDD / hoarding
- BDD: appearance defect preoccupation, mirror checking
- Hoarding: discarding difficulty, clutter, attachment to items
- OCRD chapter neighbours with distinct targets
- Mislabeling delays correct ERP/med focus
Also discriminate generalised anxiety (worry about real-life problems, not intrusive ego-dystonic images with rituals), illness anxiety, PTSD intrusive memories tied to trauma, substance-induced repetitive behaviours, and neurological conditions (e.g. complex tics, Sydenham chorea history in paediatric context).[9][16]
BDD specifically. Preoccupation with perceived appearance flaws, repetitive mirror checking or camouflaging, and high suicidality risk — related but not “just OCD of the face.” Treatment still often uses SSRI and specialised CBT, but formulation differs.[16]
Clinical and bedside assessment
Structure the interview: onset and course; content dimensions; hours per day; insight; avoidance; family accommodation; prior ERP (quality, not just “had CBT”); prior medication dose, duration, adherence; suicide risk; substances; medical history; perinatal status; tics; autism traits; depression comorbidity.[8][9]
Document full MSE with examples of obsessions and rituals in the patient’s words. Risk assessment is mandatory — OCD itself is associated with elevated suicidality, especially with depression and severe impairment.[2][9]
Capacity is decision-specific. Involuntary care uses local Mental Health Act principles when severe OCD with incapacity and risk warrants it — name the jurisdiction’s framework; do not invent section numbers for the wrong country.[8]
Investigations and measurement-based care
Baseline before high-dose SSRI or clomipramine (typical adult set). Full blood count; urea and electrolytes (hyponatraemia risk); liver function; consider glucose/lipids and BMI if antipsychotic augmentation planned; ECG before clomipramine and when cardiac risk or older age; pregnancy test when relevant. Neuroimaging only if late first onset, focal neurology, or cognitive red flags — not routinely for classic young-adult OCD.[8][14]
Y-BOCS — the scale every candidate must own
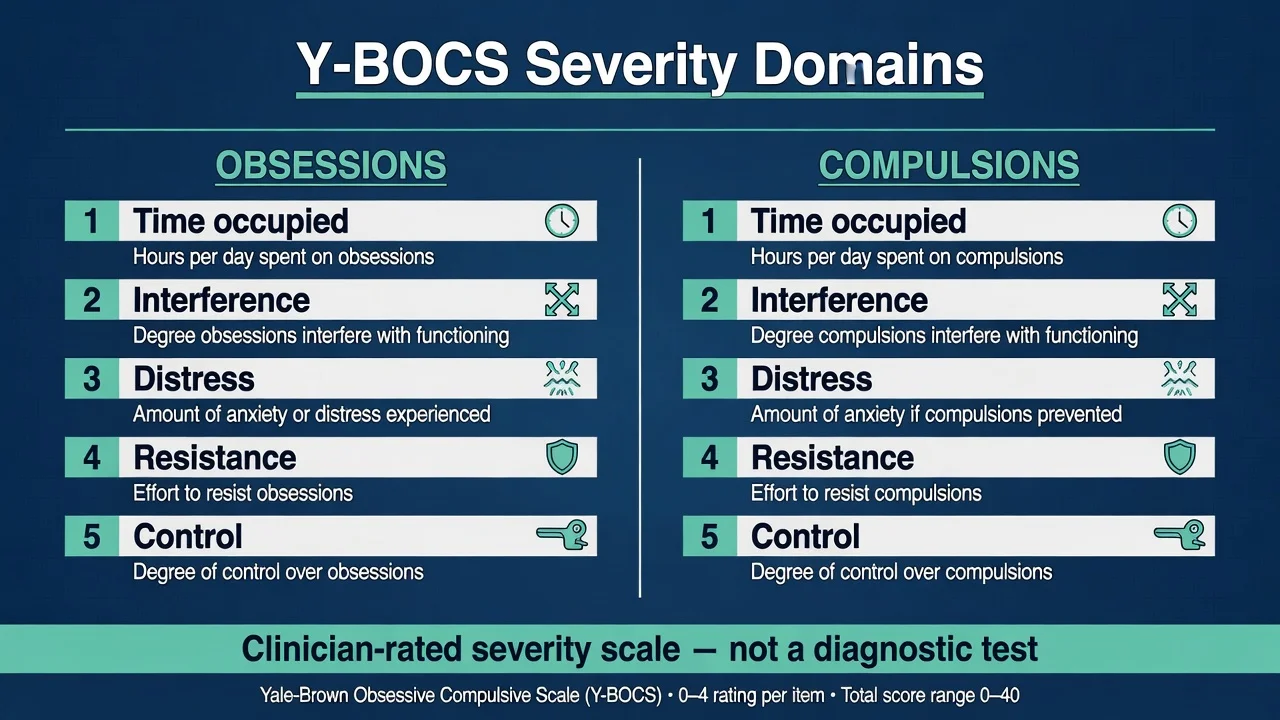
The Yale–Brown Obsessive Compulsive Scale (Y-BOCS) is a clinician-rated severity measure developed with separate obsession and compulsion item clusters (classic 10-item total score structure: time occupied, interference, distress, resistance, control for each domain).[1]
| Domain (concept) | What is rated | Exam use |
|---|---|---|
| Time occupied | Hours consumed by obsessions/compulsions | Severity and impairment |
| Interference | Function at work/home/social | Disposition intensity |
| Distress | Subjective anxiety/discomfort | Risk and urgency |
| Resistance | Effort to resist | Insight/engagement |
| Control | Success controlling symptoms | Treatment response tracking |
| Y-BOCS measures severity, not diagnosis. Common research bands (approximate teaching values): subclinical low scores; mild, moderate, severe, and extreme ranges used in trials — quote ranges as approximate and pair with clinical judgment. Serial Y-BOCS supports measurement-based care during SSRI titration and ERP.[1][9] |
Management — acute risk and resuscitation
Medical emergencies of treatment. Serotonin syndrome with serotonergic polypharmacy; symptomatic hyponatraemia on SSRI (especially older adults); clomipramine cardiotoxicity and seizures in overdose — manage on medical pathways with cardiac monitoring as indicated.[14]
Management — definitive and stepwise
First-line psychological treatment — CBT with ERP
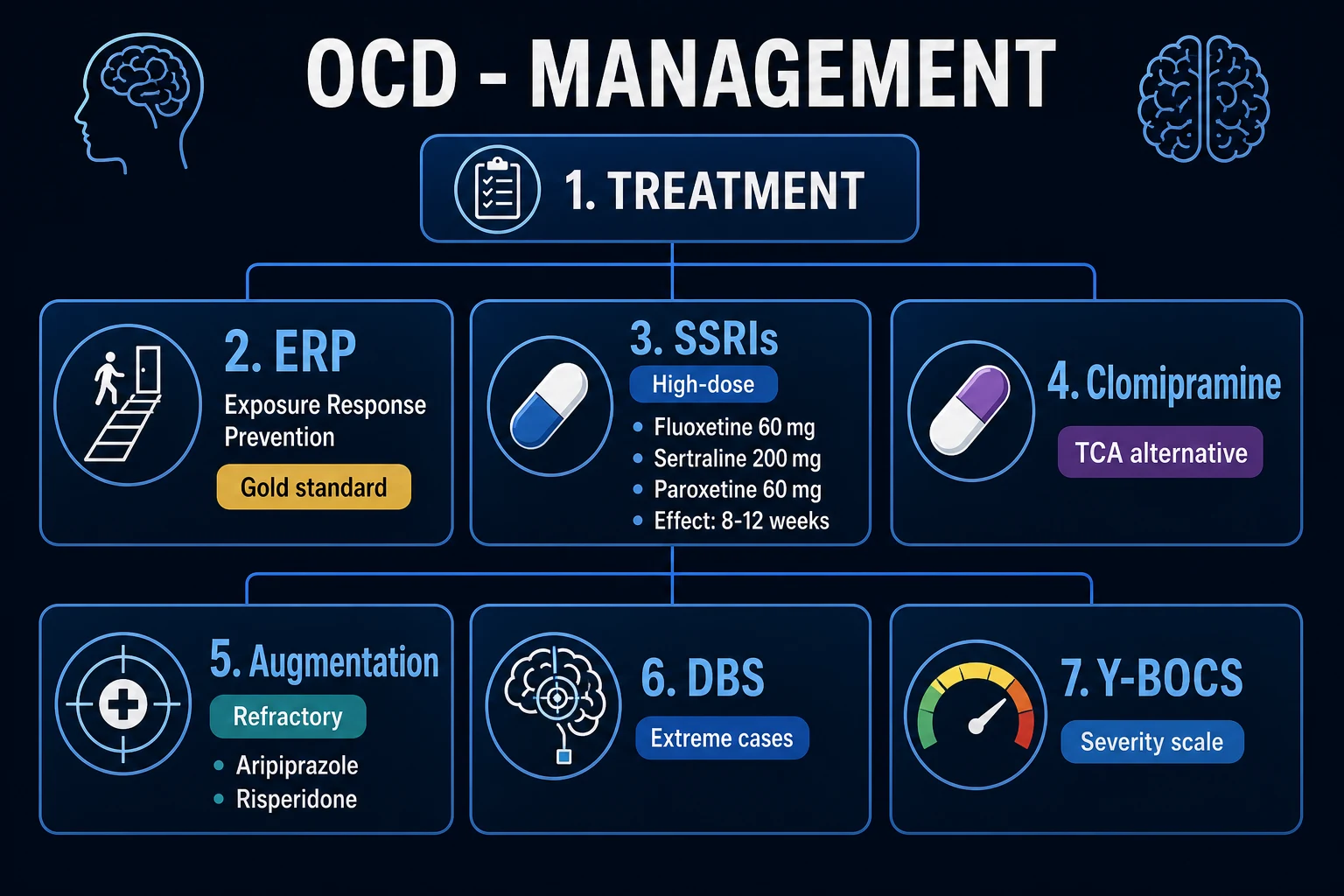
Exposure and response prevention (ERP) is the gold-standard psychological treatment for OCD. The patient confronts feared stimuli (in vivo, imaginal, or interoceptive as appropriate) while refraining from rituals and neutralising, including mental rituals and reassurance. Sessions build a hierarchy from lower- to higher-anxiety items. Family accommodation is reduced collaboratively.[3][13][19]
Landmark evidence: Foa and colleagues showed robust efficacy of exposure and ritual prevention versus clomipramine and placebo conditions in a rigorous randomised design — ERP is not optional soft therapy.[3] Meta-analyses of cognitive-behavioural treatments support large effects for CBT/ERP protocols in OCD.[13] Network meta-analysis of pharmacological and psychotherapeutic interventions supports efficacy of both classes of intervention in adults.[10]
Generic “supportive CBT” without ERP is a classic exam failure mode. Specialist OCD therapists or protocols improve fidelity.[8][17]
First-line pharmacotherapy — SSRI at OCD doses
SSRIs are first-line medications. Doses are often higher than typical depression doses, and an adequate trial is longer — commonly taught as 8–12 weeks at the maximum tolerated therapeutic dose before declaring non-response, after adherence is verified.[4][5][8][14]
Cochrane review supports SSRI superiority over placebo in OCD.[4] Dose–response meta-analysis supports higher SSRI dosing ranges for OCD response.[5]
| Agent (class) | Typical adult start (oral) | Common OCD therapeutic range (exam teaching) | Key notes |
|---|---|---|---|
| Sertraline (SSRI) | 50 mg daily | 50–200 mg daily | Often preferred; titrate; sexual/GI effects |
| Fluoxetine (SSRI) | 20 mg daily | 20–80 mg daily | Long half-life; activating |
| Fluvoxamine (SSRI) | 50 mg daily | 100–300 mg daily | CYP interactions (e.g. clozapine, theophylline) |
| Paroxetine (SSRI) | 20 mg daily | 20–60 mg daily | Discontinuation symptoms; anticholinergic edge |
| Escitalopram (SSRI) | 10 mg daily | 10–20 mg daily (some use higher under specialist caution) | QTc caution at higher doses |
| Clomipramine (TCA/SRI) | 25 mg daily | 100–250 mg daily (individualise) | After SSRI failure or specialist choice; ECG, anticholinergic, seizure risk |
| Typical adult oral ranges for exam use; individualise for age, hepatic/renal function, interactions, pregnancy; check local product information.[5][8][14] |
Monitoring. Early activation/anxiety increase; sexual dysfunction (major adherence driver); GI effects; hyponatraemia in elderly; drug interactions; suicide risk with comorbid depression. Educate that benefit may lag weeks despite early side-effects.[8][14]
Clomipramine
Clomipramine remains a potent option, often after two SSRI failures or when specialist preference and monitoring capacity exist. Anticholinergic effects, weight gain, sexual dysfunction, orthostasis, seizure risk, and cardiac conduction effects require baseline ECG and careful titration. Do not combine casually with other serotonergic agents without expertise.[3][8][14]
Augmentation after SRI non-response
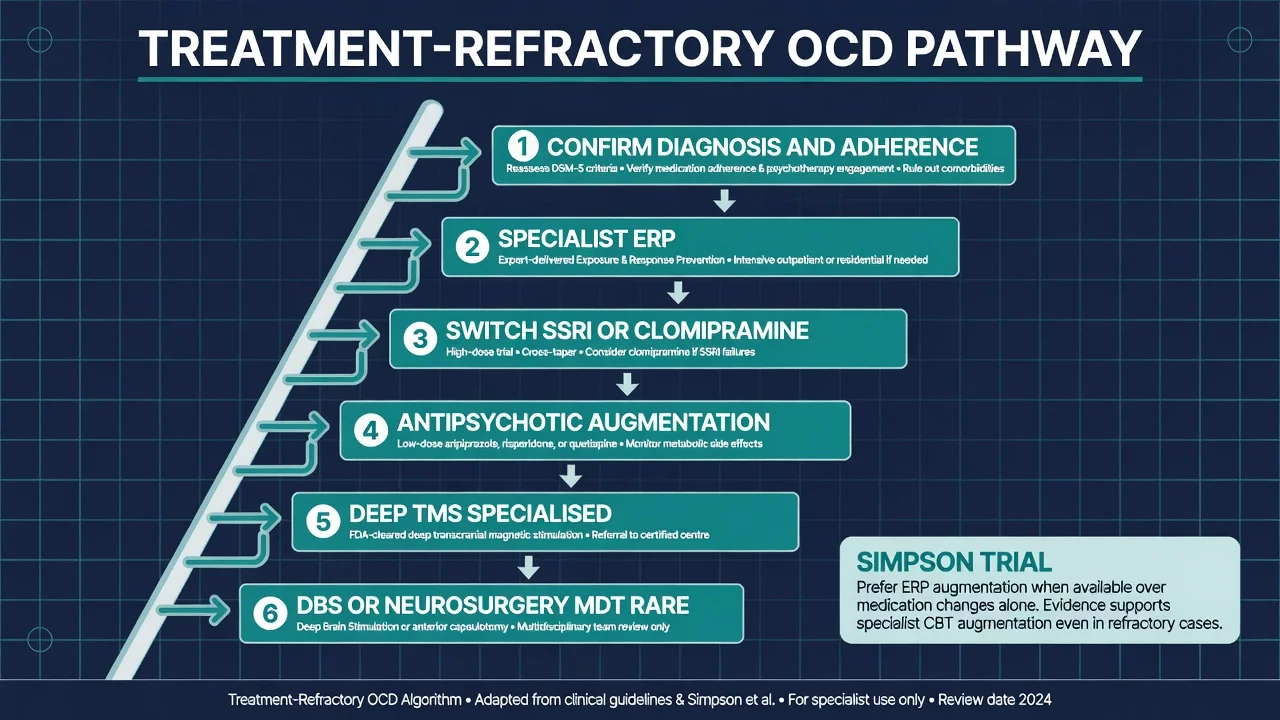
Confirm diagnosis, adherence, dose, duration, substance use, and whether true ERP was delivered, then: (1) augment with ERP if medication alone was used — often more effective than adding risperidone in the Simpson randomised comparison of CBT versus risperidone augmentation of SRIs; (2) low-dose antipsychotic augmentation (evidence strongest historically for risperidone, later practice includes aripiprazole) for SRI-resistant OCD — monitor metabolic effects, EPS/akathisia, prolactin, and QTc context; (3) example exam-level adult starts (individualise): risperidone 0.5 mg orally at night, titrate cautiously often in the 0.5–2 mg range used in OCD augmentation literature; aripiprazole often 2–5 mg daily initially with a monitoring plan. Systematic review supports antipsychotic augmentation in treatment-refractory OCD after SRI failure.[6][7][14]
Deep TMS, rTMS, and neurosurgery pathway
Deep transcranial magnetic stimulation (deep TMS) has randomised double-blind placebo-controlled evidence of efficacy and safety in OCD and is an FDA-cleared specialised option for patients who have not responded adequately to medication and CBT pathways — not a first-line community intervention.[11]
Deep brain stimulation (DBS) and other neurosurgical approaches (historical capsulotomy/cingulotomy in highly selected centres) are reserved for severe, chronic, treatment-refractory OCD after exhaustive specialised trials. Meta-analysis supports meaningful response rates in carefully selected DBS cohorts, with neurosurgical risk and ethical consent requirements.[18] Exam stance: know the existence of the pathway; do not offer DBS as a casual outpatient suggestion.
Maintenance
Continue an effective SSRI for a prolonged period after response (commonly at least 1–2 years, longer if highly recurrent or severe — individualise). Plan ERP booster sessions. Relapse is common with abrupt stop. Withdraw medication slowly with a plan.[8][14][17]
Specific subtypes and scenarios
Contamination/washing. Graded exposure to contaminants with strict response prevention of washing; address cleaning product rituals and family cleaning accommodation.[13]
Forbidden thoughts. Imaginal exposure and mental-ritual prevention; do not collude with endless “proof” of morality; distinguish from risk of actual harm (clinical risk assessment still required when content is aggressive).[19]
Tic-related OCD. Screen for Tourette spectrum; may influence antipsychotic augmentation choices and dual formulation.[9]
Treatment-refractory algorithm (exam ladder). Adequacy check → switch SSRI → second SSRI or clomipramine → ERP ± meds → antipsychotic augmentation → specialist centre (deep TMS) → multidisciplinary review for DBS/neurosurgery candidacy.[8][11][17][18]
Complications and pitfalls
- Misdiagnosing OCD as psychosis or “personality” and withholding ERP/SSRI.[9]
- Under-dosing SSRI or declaring failure after 2–3 weeks at half-dose.[5]
- Labelling any CBT as ERP when no exposures or response prevention occurred.[3]
- Family accommodation silently defeating treatment.[19]
- Ignoring sexual side-effects and non-adherence.[14]
- Over-applying PANDAS work-up to chronic adult OCD without paediatric acute phenotype.[12]
Prognosis and disposition
Without treatment, course is often chronic with waxing and waning. With ERP and/or adequate SSRI, many patients achieve clinically meaningful reduction in Y-BOCS and function, though residual symptoms are common.[2][9][13]
Poorer response predictors: longer duration untreated, early onset, poor insight, severe accommodation, multiple comorbidities, incomplete ERP. Disposition ladder: guided self-help/primary care for mild with access to protocolised CBT; secondary CMHT; specialist OCD service; intensive outpatient or inpatient ERP programmes for severe disability; rare neurosurgical pathway.[8][17]
Special populations
Children and adolescents. Family-based CBT/ERP is first-line emphasis; SSRIs when indicated with careful monitoring of activation and suicidality risk discussion; involve carers in reducing accommodation.[8][17]
Pregnancy and lactation. Untreated severe OCD impairs parenting and self-care; sertraline is frequently discussed among SSRI options when medication is needed — shared decision-making with perinatal psychiatry input when available. Prefer ERP when accessible and sufficient.[8]
Older adults. Hyponatraemia, falls, polypharmacy, and late-onset organic screen; start lower, titrate slower; ECG before clomipramine.[14]
ASD / intellectual disability. Adapt ERP language and hierarchy; distinguish preferred routines from ego-dystonic OCD; avoid over-medication of sameness behaviours.[9]
PANDAS / PANS — exam-aware nuance
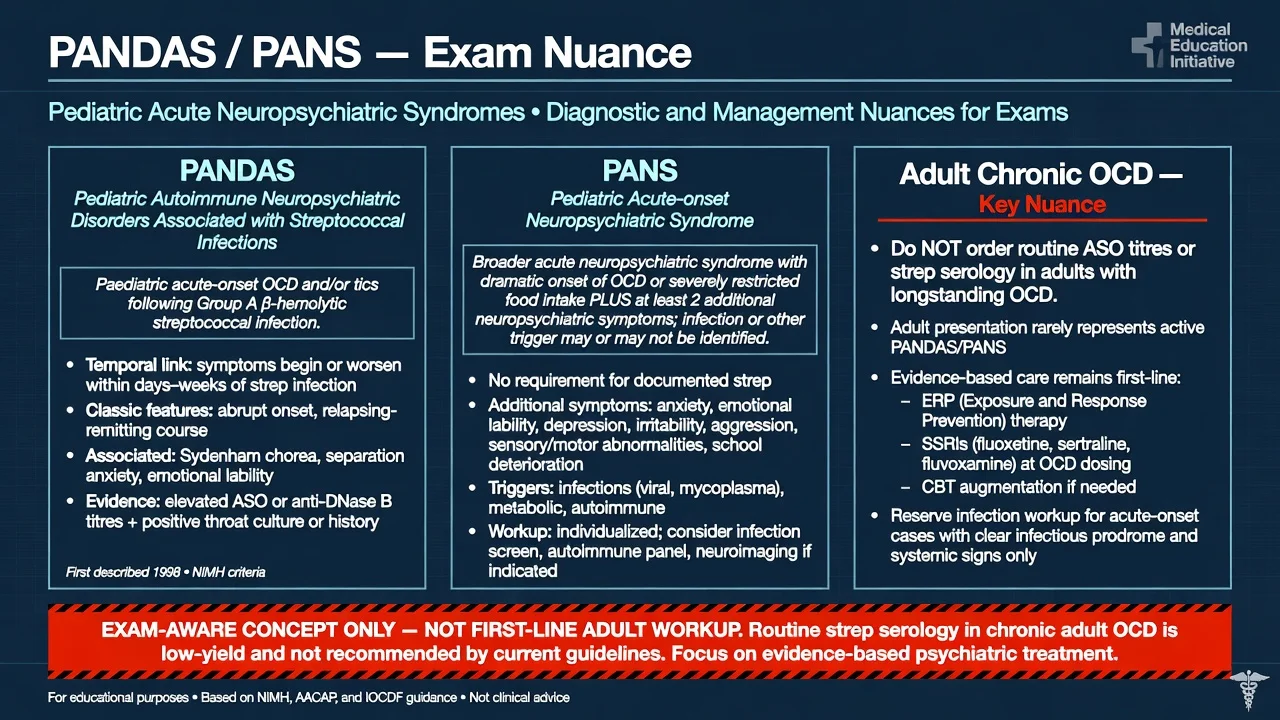
PANDAS (paediatric autoimmune neuropsychiatric disorders associated with streptococcal infections) describes an acute paediatric-onset phenotype of OCD and/or tics temporally linked to group A streptococcal infection, as characterised in Swedo’s early clinical series.[12] PANS is a broader acute neuropsychiatric syndrome framework. Exam stance: know the concept, the acute paediatric temporal story, and that management of the psychiatric syndrome still centres on evidence-based OCD care plus appropriate medical evaluation — do not order routine ASO titres on every adult with chronic OCD, and do not promise immunomodulation as standard fellowship first-line outside specialist paediatric pathways.[12][17]
Evidence, guidelines and regional differences
Landmark pillars: Goodman Y-BOCS development;[1] Ruscio epidemiology;[2] Foa ERP vs clomipramine;[3] Soomro SSRI Cochrane;[4] Bloch dose–response;[5] Bloch antipsychotic augmentation;[6] Simpson ERP vs risperidone augmentation;[7] APA practice guideline;[8] Hirschtritt JAMA review;[9] Skapinakis network meta-analysis;[10] Carmi deep TMS trial;[11] Swedo PANDAS series;[12] Öst CBT meta-analysis;[13] Fineberg ICOCS position;[17] Alonso DBS meta-analysis.[18]
In Australian and New Zealand practice, access to specialist ERP is often the rate-limiting step. Use public secondary services, private psychologists with ERP competence, and stepped digital/protocolised CBT where fidelity is acceptable. Prescribing follows TGA product information; clomipramine and antipsychotic augmentation require metabolic and cardiac risk discussion. Mental Health Act frameworks are state/territory-specific.[8][17]
Exam pearls
OCD treatment ladder (exam)
References
- [1]Goodman WK, Price LH, Rasmussen SA, Mazure C, Fleischmann RL, Hill CL, et al. The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability Arch Gen Psychiatry, 1989.PMID 2684084
- [2]Ruscio AM, Stein DJ, Chiu WT, Kessler RC The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication Mol Psychiatry, 2010.PMID 18725912
- [3]Foa EB, Liebowitz MR, Kozak MJ, Davies S, Campeas R, Franklin ME, et al. Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive-compulsive disorder Am J Psychiatry, 2005.PMID 15625214
- [4]Soomro GM, Altman D, Rajagopal S, Oakley-Browne M Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD) Cochrane Database Syst Rev, 2008.PMID 18253995
- [5]Bloch MH, McGuire J, Landeros-Weisenberger A, Leckman JF, Pittenger C Meta-analysis of the dose-response relationship of SSRI in obsessive-compulsive disorder Mol Psychiatry, 2010.PMID 19468281
- [6]Bloch MH, Landeros-Weisenberger A, Kelmendi B, Coric V, Bracken MB, Leckman JF A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder Mol Psychiatry, 2006.PMID 16585942
- [7]Simpson HB, Foa EB, Liebowitz MR, Huppert JD, Cahill S, Maher MJ, et al. Cognitive-behavioral therapy vs risperidone for augmenting serotonin reuptake inhibitors in obsessive-compulsive disorder: a randomized clinical trial JAMA Psychiatry, 2013.PMID 24026523
- [8]Koran LM, Hanna GL, Hollander E, Nestadt G, Simpson HB, American Psychiatric Association Practice guideline for the treatment of patients with obsessive-compulsive disorder Am J Psychiatry, 2007.PMID 17849776
- [9]Hirschtritt ME, Bloch MH, Mathews CA Obsessive-Compulsive Disorder: Advances in Diagnosis and Treatment JAMA, 2017.PMID 28384832
- [10]Skapinakis P, Caldwell DM, Hollingworth W, Bryden P, Fineberg NA, Salkovskis P, et al. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: a systematic review and network meta-analysis Lancet Psychiatry, 2016.PMID 27318812
- [11]Carmi L, Tendler A, Bystritsky A, Hollander E, Blumberger DM, Daskalakis J, et al. Efficacy and Safety of Deep Transcranial Magnetic Stimulation for Obsessive-Compulsive Disorder: A Prospective Multicenter Randomized Double-Blind Placebo-Controlled Trial Am J Psychiatry, 2019.PMID 31109199
- [12]Swedo SE, Leonard HL, Garvey M, Mittleman B, Allen AJ, Perlmutter S, et al. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: clinical description of the first 50 cases Am J Psychiatry, 1998.PMID 9464208
- [13]Öst LG, Havnen A, Hansen B, Kvale G Cognitive behavioral treatments of obsessive-compulsive disorder. A systematic review and meta-analysis of studies published 1993-2014 Clin Psychol Rev, 2015.PMID 26117062
- [14]Pittenger C, Bloch MH Pharmacological treatment of obsessive-compulsive disorder Psychiatr Clin North Am, 2014.PMID 25150568
- [15]Pauls DL The genetics of obsessive-compulsive disorder: a review Dialogues Clin Neurosci, 2010.PMID 20623920
- [16]Phillips KA Body dysmorphic disorder: recognizing and treating imagined ugliness World Psychiatry, 2004.PMID 16633443
- [17]Fineberg NA, Hollander E, Pallanti S, Walitza S, Grünblatt E, Dell'Osso BM, et al. Clinical advances in obsessive-compulsive disorder: a position statement by the International College of Obsessive-Compulsive Spectrum Disorders Int Clin Psychopharmacol, 2020.PMID 32433254
- [18]Alonso P, Cuadras D, Gabriëls L, Denys D, Goodman W, Greenberg BD, et al. Deep Brain Stimulation for Obsessive-Compulsive Disorder: A Meta-Analysis of Treatment Outcome and Predictors of Response PLoS One, 2015.PMID 26208305
- [19]Abramowitz JS, Abramovitch A, McKay D, Draffin A Management of obsessive-compulsive disorder in adults BMJ, 2026.PMID 41698714
- [20]International Obsessive Compulsive Disorder Foundation Genetics Collaborative (IOCDF-GC) and OCD Collaborative Genetics Association Studies (OCGAS) Revealing the complex genetic architecture of obsessive-compulsive disorder using meta-analysis Mol Psychiatry, 2018.PMID 28761083