Psych · General adult psychiatry — personality disorders
Obsessive-compulsive personality disorder
Also known as OCPD · Anankastic personality disorder · Anankastia · Compulsive personality disorder · Cluster C personality — OCPD
Exam-exhaustive fellowship reference on obsessive-compulsive personality disorder (OCPD/anankastic PD) — DSM-5-TR ≥4/8 criteria, ICD-11 severity and anankastia, ego-syntonic vs OCD, comorbidity, CBT and schema therapy, limited pharmacotherapy of comorbidity. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Obsessive-compulsive personality disorder (OCPD; ICD legacy anankastic personality disorder) is a high-yield Cluster C topic because examiners test criteria accuracy, the OCPD versus OCD discriminator, and whether you can engage a rigid, often high-functioning patient without colluding with perfectionism or therapeutic nihilism.[1][2][4]
Overview and definition
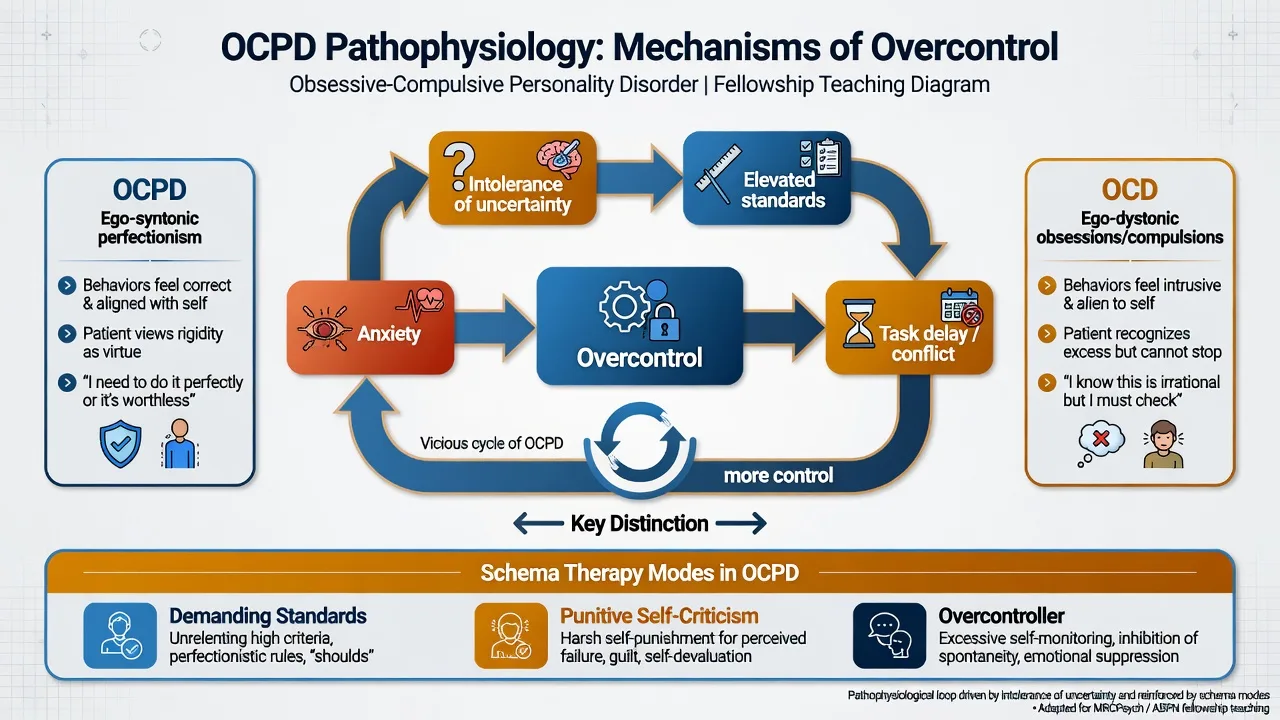
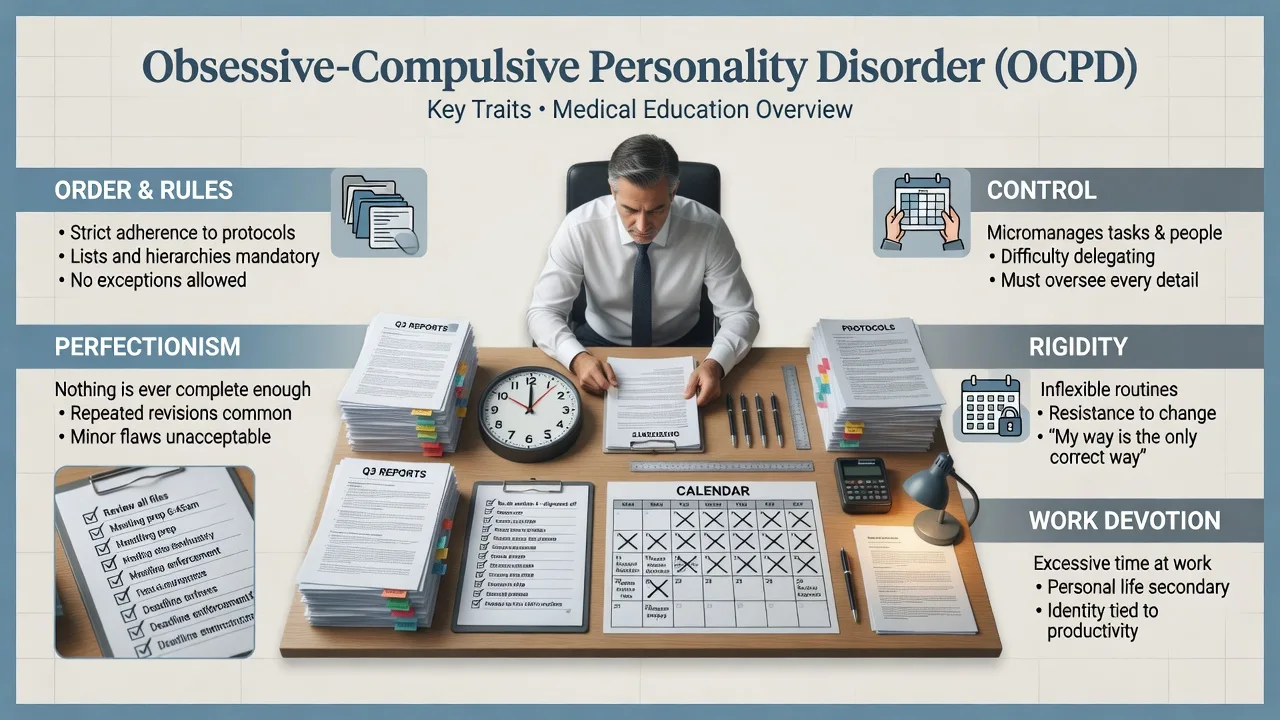
OCPD describes an enduring preoccupation with orderliness, perfectionism, and mental and interpersonal control at the expense of flexibility, openness and efficiency. Traits are frequently experienced as correct standards by the patient (ego-syntonic), while partners, colleagues and supervisors experience obstruction, delayed delivery and conflict. Diagnosis requires a longitudinal, cross-context pattern beginning by early adulthood — not a single stressful project, cultural work ethic, or acute anxiety episode.[1][2]
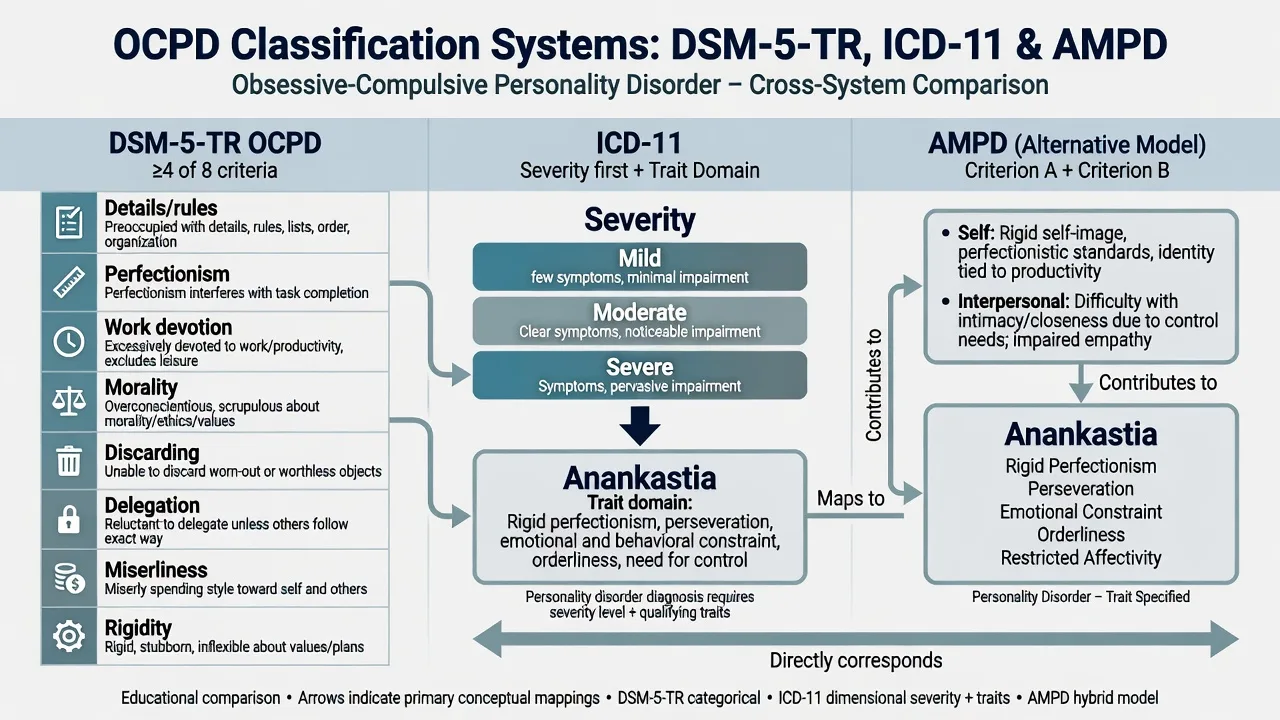
DSM-5-TR operational diagnosis (exam-critical). After general personality disorder criteria are met, OCPD requires a pervasive pattern indicated by four or more of eight features: (1) preoccupation with details, rules, lists, order, organisation or schedules to the extent that the major point of the activity is lost; (2) perfectionism that interferes with task completion; (3) excessive devotion to work and productivity to the exclusion of leisure and friendships (not accounted for by economic necessity); (4) overconscientious, scrupulous and inflexible morality, ethics or values (not accounted for by cultural or religious identification); (5) inability to discard worn-out or worthless objects even when they have no sentimental value; (6) reluctance to delegate tasks or to work with others unless they submit exactly to the person's way of doing things; (7) miserly spending style toward self and others, money viewed as something to be hoarded for future catastrophes; (8) rigidity and stubbornness.[1][2]
ICD-11 framing. Personality disorder is graded by severity (mild, moderate, severe) with trait domain qualifiers. Features historically labelled anankastic/OCPD map largely onto high anankastia (and often negative affectivity) within a severity rating. Fellowship answers should name which manual is in use: classic MCQs still test DSM's ≥4/8 list; formulation stations reward ICD-11 severity-plus-traits language.[12]
Classification and nosology
DSM-5-TR OCPD
- ≥4 of 8 named features
- General PD criteria required
- Onset by early adulthood, cross-context
- Cluster C teaching scaffold
ICD-11 PD
- Severity first: mild / moderate / severe
- Trait domain: anankastia prominent
- Legacy ICD-10 anankastic PD in older stems
- Dimensional case discussion friendly
AMPD (DSM Section III)
- Criterion A: self and interpersonal impairment
- Criterion B: anankastia ± negative affectivity
- Useful for therapy targets even if categorical diagnosis used
- Avoid trait word-salad without impairment
vs OCD (OCRD)
- OCD: ego-dystonic obsessions/compulsions
- Time-consuming rituals, resistance, insight spectrum
- Y-BOCS tracks OCD severity
- Co-occurrence common — diagnose both
OCPD versus OCD — the viva trap
This is the highest-yield discriminator in the entire topic. OCPD perfectionism and control are often valued or defended as correct; OCD obsessions are unwanted, intrusive and resisted, with compulsions aimed at reducing distress or preventing a feared outcome. Co-occurrence is substantial in OCD samples — Pozza and colleagues' systematic review and meta-analysis quantify OCPD co-occurrence among people with OCD and highlight clinical complexity when both are present.[3][4]
High-yield discriminators for exams:[1][2][4][18]
- Ask: "Are these thoughts/rituals something you want to stop, or standards you believe others should share?"
- Time-consuming ego-dystonic rituals, contamination/harm/symmetry obsessions with response prevention needs → treat on an OCD pathway (ERP ± SSRI), even if OCPD is also present.[15][16][18]
- Pure OCPD without true obsessions still impairs via delay, rigidity, interpersonal control and work–life collapse.[1]
- Do not answer that "OCPD is mild OCD" or that every perfectionist has OCPD.[2]
Epidemiology and risk factors
Headline epidemiology candidates must own
Community prevalence estimates for any personality disorder and for specific PDs differ by instrument, threshold and culture, but OCPD repeatedly appears among the more common categorical PDs in major surveys (NESARC, NCS-R interview work, Torgersen community sampling), and global PD burden is substantial on systematic review and meta-regression.[7][8][9][10]
Risk and aetiology. Anankastic temperament, modelling of rigid standards, overcontrolling or highly rule-bound family environments, and genetic liability shared with broader personality structure contribute; none alone makes the diagnosis. Help-seeking is often delayed because traits feel adaptive until efficiency collapses, relationships rupture, or depression appears.[1][2]
Pathophysiology and mechanisms
Core maintaining loop. Intolerance of uncertainty and elevated personal standards drive overcontrol of self, tasks and others; incomplete control produces anxiety and criticism (internal or interpersonal); the response is more rules, checking and delayed completion — efficiency falls while moral certainty rises.[1][2]
Schema/mode language (therapy-ready). Demanding standards and punitive self-criticism modes, perfectionistic overcontroller coping, and fear of failure or moral error maintain rigidity. Schema therapy RCT evidence in mixed personality disorder samples (including Cluster C patterns) supports structured mode work as a viable pathway when CBT skills alone stall.[5][6]
Neurobiology (keep humble). Group-level findings on cognitive control, error monitoring and related systems are not diagnostic biomarkers. Imaging does not diagnose OCPD and must never replace history, collateral and functional assessment.[1][2]
Clinical presentation
Core adult presentation combines rule-bound order, perfectionism that delays completion, work devotion at the cost of leisure and intimacy, moral inflexibility, difficulty discarding, reluctance to delegate, miserly money attitudes in some, and stubborn rigidity. On MSE, expect formal affect, controlled speech, agenda-setting that monopolises the interview, limited spontaneous humour, and insight that is often partial ("I have high standards; other people are careless").[1][2]
Settings examiners use. Occupational health and general adult clinics see stalled promotions, incomplete projects and team conflict; couples work sees control battles over household standards; medical student/doctor pathways see burnout behind "excellent" performance; OCRD clinics see dual OCPD+OCD; ED and crisis teams see depression after public failure or criticism.[1][4]
"High-functioning" OCPD. Professional success does not exclude diagnosis if flexibility, relationships and efficiency are impaired across contexts. Impairment may be most visible to others until depression or a deadline collapse forces contact.[1]
Differential diagnosis
vs OCD
- OCD: ego-dystonic, resisted, ritualised
- OCPD: ego-syntonic standards, control
- Y-BOCS for OCD load
- Treat both when both present
vs ASD rigidity
- ASD: early social communication differences
- Restricted interests, sensory profile
- Social motivation quality differs
- Dual formulation possible
vs anorexia perfectionism
- AN: body-image/weight control core
- Medical risk pathway dominates
- Perfectionism may be shared trait
- Do not collapse AN into OCPD
vs hoarding disorder
- Hoarding: acquisition/clutter impairment focus
- OCPD criterion 5 is discarding difficulty
- May co-occur
- Assess clutter risk and safety
Also keep GAD/worry (anxiety content without full PD pattern), BDD (appearance-focused OCRD), narcissistic achievement focus (admiration/status rather than order/morality), avoidant PD (rejection fear rather than control), and late-onset personality change (organic, mood, substance, frontotemporal) on the board. The exam skill is discriminators plus comorbidity, not exclusive single labels.[1][2][11]
Clinical and bedside assessment
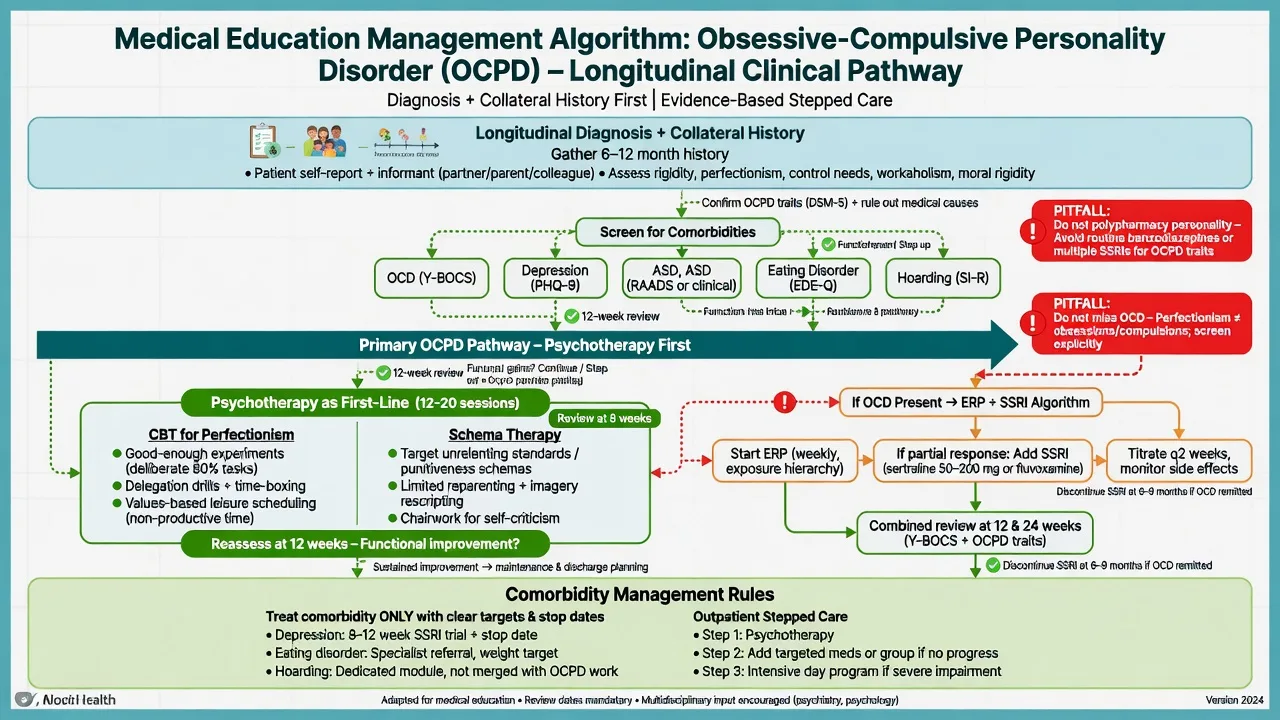
Structure the interview: developmental perfectionism from school age; friendships and leisure (often thin); occupational performance under evaluation; moral/scrupulosity themes; discarding behaviour; delegation history; money style; relationship conflict about control; substance use (alcohol to "switch off"); prior OCD, ASD or eating-disorder assessments; what the patient wants help with today (often depression, insomnia, work conflict — not "my personality"). Obtain collateral early; patients may minimise interpersonal impact.[1][2]
Mental State Examination. Formality, control of the interview process, limited affective range, thought content focused on standards/errors/fairness, insight (traits as virtues), judgement about trade-offs (leisure, relationships). Document capacity as decision-specific.[1]
Risk domains examiners expect. Suicide and self-harm risk rises with comorbid depression after failure, criticism, job loss or relationship rupture — controlled outward affect can mask severity. Occupational ruin, family breakdown, and neglect of health/leisure are morbidity endpoints. Vulnerability is less about exploitation than about isolation and untreated mood disorder. Capacity and safeguarding follow local statute when dependents or self-neglect feature.[1][2]
Tools. SCID-5-PD / IPDE conceptually for categorical diagnosis; ICD-11 severity and anankastia ratings for dimensional formulation; Y-BOCS when OCD is suspected; structured ASD and eating-disorder screens when history fires.[1][18]
Investigations
OCPD has no laboratory gold standard. Investigate to exclude mimics and prepare for any medication: TSH, FBC, U&E, LFT, glucose/lipids as baseline; pregnancy test when applicable; urine drug screen when relevant; ECG before selected agents. Cognitive screen and neuroimaging or EEG when late-onset change, focal neurology, seizures or significant TBI history fire. Screen systematically for OCD, major depression, anxiety disorders, ASD traits, eating disorders and substance use because they change treatment more than the personality label alone.[1][2][18]
Management — acute crisis and resuscitation
Immediate priorities. Acute presentations are usually comorbidity-driven: major depression with suicidal ideation, severe OCD impairment, or panic after public failure. Medical stabilisation of overdose or self-harm injuries comes first. Validate distress without colluding with impossible standards; collaborative safety planning; means restriction; least-restrictive disposition with named follow-up.[1][2]
Stance. Avoid pejorative dismissal ("just a perfectionist") and avoid open-ended admission without a plan. Legal status is jurisdiction-specific when imminent risk and incapacity meet statutory criteria — state principles rather than inventing foreign section numbers.[1]
Management — definitive and stepwise
Psychotherapy first-line
Structured psychological therapy is the core pathway for OCPD features that impair function.[1][2]
CBT for perfectionism and rigidity. Targets elevated standards, all-or-nothing rules, procrastination driven by fear of imperfect completion, and interpersonal control. Techniques include collaborative goal-setting of "good enough" criteria, behavioural experiments (submit a 90 percent draft; leave a minor task unfinished intentionally), graded exposure to uncertainty, values-based scheduling of leisure and relationships, and delegation experiments with outcome monitoring. Session structure should be clear (OCPD patients often demand agendas) without recreating a control battle.[1][2]
Schema therapy. Multicenter RCT evidence (Bamelis 2014) supports schema therapy's clinical effectiveness for personality disorders in mixed samples that include Cluster C patterns; economic evaluation supported cost-effectiveness relative to clarification-oriented therapy in that programme of work. Use mode work for demanding parent, punitive critic and overcontroller patterns when pure skills CBT stalls.[5][6]
Adapted psychodynamic / supportive strategies. Address harsh superego, affect intolerance and relational control carefully; alliance ruptures often re-enact control–criticism cycles. Consistency of formulation across the treating team reduces iatrogenic power struggles.[1][2]
When OCD co-occurs
Prioritise exposure and response prevention and evidence-based SSRI algorithms for OCD rather than personality-focused work alone. Foa and colleagues' randomised trial supports EX/RP (and combination pathways) for OCD; APA OCD practice guidance and subsequent reviews remain exam anchors for stepped OCD care.[15][16][18]
Example pharmacotherapy when comorbid OCD requires medication (individualise; treat OCD, not "cure OCPD"). Fluoxetine is often started around 20 mg orally daily, titrated toward higher OCD ranges under specialist review (commonly toward 40–60 mg daily as tolerated; sometimes higher under specialist care), with counselling on sexual side effects, activation, GI effects and suicidality risk especially early and in younger adults, and a clear response review at 8–12 weeks at an adequate dose. Cochrane and dose-response meta-analytic evidence support SSRIs for OCD and higher-dose ranges for many patients — document target symptoms (obsessions/compulsions, Y-BOCS trajectory), not vague "rigidity."[13][14][16]
Pharmacotherapy principles for OCPD itself
No medication is disease-modifying for OCPD as a whole. Treat major depression, anxiety disorders and true OCD with standard agents, named targets and stop/review dates. Avoid chronic benzodiazepines for intolerance of uncertainty. Avoid polypharmacy for personality-related dissatisfaction.[1][2][13]
Care system and disposition
Most patients are managed in outpatient psychotherapy and general adult pathways. Step up for acute suicide risk, severe OCD functional collapse, or medical risk (e.g. eating disorder). Step down when flexibility generalises and risk stabilises. Occupational liaison and couple sessions help when control conflicts dominate the presentation.[1][2]
Australian and New Zealand practice emphasises stepped mental health care, access to psychological therapies where available, and culturally safe formulation. Local Mental Health Act provisions govern involuntary care — name least-restrictive principles, not invented foreign section numbers. Coordinate with OCRD-capable services when true OCD is present.[12][18]
Specific subtypes and scenarios
OCPD professional with burnout. High standards masking incomplete work, marital conflict and anhedonia outside work. Therapy targets values-based flexibility; screen depression and OCD carefully.[1][2]
OCPD + OCD dual diagnosis. Ego-syntonic perfectionism plus ego-dystonic rituals. Sequence ERP/SSRI for OCD while addressing interpersonal control in therapy; dual formulation, dual plan.[3][4][15]
OCPD with major depression after workplace failure. Treat the depressive episode fully; do not attribute all anhedonia to "personality."[1]
Adult autism dual formulation. Developmental social communication history and sensory profile prevent automatic OCPD labelling of rigidity; both can inform supports.[11]
Discarding difficulty vs hoarding disorder. Criterion 5 is not automatic hoarding disorder; assess clutter, acquisition, safety and functional impact separately.[1][2]
Anorexia interface. Weight/shape-driven control needs eating-disorder pathway priority; shared perfectionism is not an excuse to miss medical risk.[1]
Retirement decompensation. Lifelong anankastia may present when structure collapses; late-onset new rigidity still needs organic work-up.[1][12]
Complications and pitfalls
Classic pitfalls: missing OCD under an OCPD label; colluding with perfectionism as virtue; power struggles that recreate control battles; polypharmacy without targets; missing depression/suicide risk behind controlled affect; misdiagnosing ASD as OCPD without developmental history; claiming no treatment exists; starting SSRIs for "personality rigidity" without OCD/depression indication; inventing Mental Health Act section numbers.[1][3][4][11]
Prognosis and disposition
Personality psychopathology is more plastic than older textbooks claimed. Longitudinal PD research (including CLPS ten-year course teaching on symptomatic change and functional lag) supports hope with structured engagement — functional recovery in intimacy and flexibility may trail symptom change. Untreated rigidity plus untreated OCD or depression predicts chronic impairment. Disposition is usually outpatient; hospitalisation is for acute risk or severe comorbidity, not for "having OCPD."[1][5][17]
Special populations
Youth. Distinguish emerging perfectionism from adaptive high achievement. Avoid premature lifelong PD labels. Screen OCD and ASD. Early skills for flexibility can prevent entrenchment.[1][11]
Older adults. New late-life rigidity is organic/mood/substance until proven otherwise. Lifelong OCPD may decompensate after retirement, bereavement or loss of work structure.[1][12]
Pregnancy and parenting. Treat anxiety and depression carefully; assess rigid parenting styles and family impact; minimise unnecessary polypharmacy.[1]
Cultural formulation. Conscientiousness, duty and work ethic can be culturally adaptive. Diagnose OCPD only when inflexibility causes clinically significant impairment across contexts — not for culturally valued diligence alone.[1][10]
Evidence and guidelines
OCPD-specific reviews: Diedrich 2015 and Pinto 2022 for symptomatology, impact and treatment overview; Mancebo 2005 for clinical interface with OCD; Pozza 2021 for comorbidity meta-analysis.[1][2][3][4]
Epidemiology anchors: Torgersen 2001; Lenzenweger NCS-R 2007; Grant NESARC 2004; Shadid 2025 global meta-regression.[7][8][9][10]
Treatment anchors: Bamelis 2014 schema therapy RCT and 2015 economic evaluation; when OCD coexists — Foa EX/RP trial, SSRI Cochrane and dose-response meta-analysis, APA OCD practice guideline, Hirschtritt JAMA advances review.[5][6][13][14][15][16][18]
Nosology: Kim/Tyrer line on ICD-11 dimensional progress; Lugnegård 2012 for PD–ASD links; CLPS longitudinal plasticity teaching (Gunderson 2011).[11][12][17]
Controversies worth a mature viva sentence. Whether OCPD is better framed purely as ICD-11 anankastia than as a discrete category; how aggressively to pursue ERP when insight into perfectionism is low; whether high-functioning professionals with impairment mainly visible to others still meet PD thresholds (they can).[1][12]
Exam pearls
OCPD viva checklist
CONTROL
Count ≥4 of 8 DSM features + general PD criteria
OCD discrimination: ego-dystonic rituals vs ego-syntonic standards
Nosology: ICD-11 anankastia + severity
Therapy first: CBT perfectionism / schema therapy
Rule out ASD, AN, organic late-onset change
Only medicate comorbidity/OCD with named dose and review
Longitudinal collateral — not one rigid interview
60-second oral summary
OCPD is Cluster C anankastia: order, perfectionism and control at the expense of flexibility and efficiency, DSM ≥4/8 with general PD criteria, ICD-11 severity plus anankastia. Discriminate from ego-dystonic OCD, ASD rigidity, anorexia perfectionism and hoarding. Assess longitudinally with collateral; screen depression and OCRDs. First-line is CBT for perfectionism/rigidity and schema therapy (Bamelis-level PD evidence); if OCD coexists, add ERP and SSRI algorithms with named doses and review dates. No drug cures OCPD. Hope and structure beat stigma.[1][3][5][12][15]
References
- [1]Pinto A, Teller J, Wheaton MG Obsessive-Compulsive Personality Disorder: A Review of Symptomatology, Impact on Functioning, and Treatment Focus (Am Psychiatr Publ), 2022.PMID 37200888
- [2]Diedrich A, Voderholzer U Obsessive-compulsive personality disorder: a current review Curr Psychiatry Rep, 2015.PMID 25617042
- [3]Pozza A, Starcevic V, Ferretti F, Pedani C, et al. Obsessive-Compulsive Personality Disorder Co-occurring in Individuals with Obsessive-Compulsive Disorder: A Systematic Review and Meta-analysis Harv Rev Psychiatry, 2021.PMID 33666394
- [4]Mancebo MC, Eisen JL, Grant JE, Rasmussen SA Obsessive compulsive personality disorder and obsessive compulsive disorder: clinical characteristics, diagnostic difficulties, and treatment Ann Clin Psychiatry, 2005.PMID 16402751
- [5]Bamelis LL, Evers SM, Spinhoven P, Arntz A Results of a multicenter randomized controlled trial of the clinical effectiveness of schema therapy for personality disorders Am J Psychiatry, 2014.PMID 24322378
- [6]Bamelis LL, Arntz A, Wetzelaer P, Verdoorn R, et al. Economic evaluation of schema therapy and clarification-oriented psychotherapy for personality disorders: a multicenter, randomized controlled trial J Clin Psychiatry, 2015.PMID 26579561
- [7]Grant BF, Hasin DS, Stinson FS, Dawson DA, et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions J Clin Psychiatry, 2004.PMID 15291684
- [8]Lenzenweger MF, Lane MC, Loranger AW, Kessler RC DSM-IV personality disorders in the National Comorbidity Survey Replication Biol Psychiatry, 2007.PMID 17217923
- [9]Torgersen S, Kringlen E, Cramer V The prevalence of personality disorders in a community sample Arch Gen Psychiatry, 2001.PMID 11386989
- [10]Shadid J, Ferrari AJ, Bach B, Sellbom M, et al. The global epidemiology of personality disorder: a systematic review and meta-regression Lancet Psychiatry, 2025.PMID 41197646
- [11]Lugnegård T, Hallerbäck MU, Gillberg C Personality disorders and autism spectrum disorders: what are the connections? Compr Psychiatry, 2012.PMID 21821235
- [12]Kim YR, Tyrer P, Mulder R, King JD, et al. ICD-11 classification of personality disorder: there is no other way forward Br J Psychiatry, 2026.PMID 41906979
- [13]Soomro GM, Altman D, Rajagopal S, Oakley-Browne M Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD) Cochrane Database Syst Rev, 2008.PMID 18253995
- [14]Bloch MH, McGuire J, Landeros-Weisenberger A, Leckman JF, et al. Meta-analysis of the dose-response relationship of SSRI in obsessive-compulsive disorder Mol Psychiatry, 2010.PMID 19468281
- [15]Foa EB, Liebowitz MR, Kozak MJ, Davies S, et al. Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive-compulsive disorder Am J Psychiatry, 2005.PMID 15625214
- [16]Koran LM, Hanna GL, Hollander E, Nestadt G, et al. Practice guideline for the treatment of patients with obsessive-compulsive disorder Am J Psychiatry, 2007.PMID 17849776
- [17]Gunderson JG, Stout RL, McGlashan TH, et al. Ten-year course of borderline personality disorder: psychopathology and function from the Collaborative Longitudinal Personality Disorders study Arch Gen Psychiatry, 2011.PMID 21464343
- [18]Hirschtritt ME, Bloch MH, Mathews CA Obsessive-Compulsive Disorder: Advances in Diagnosis and Treatment JAMA, 2017.PMID 28384832