Psych · General adult psychiatry — anxiety disorders
Panic disorder and agoraphobia
Also known as Panic disorder · Agoraphobia · Panic attacks · Panic disorder with agoraphobia · PD · Panic neurosis · Situational panic
Exam-exhaustive fellowship reference on panic disorder and agoraphobia — DSM-5-TR and ICD-11 criteria; epidemiology; catastrophic misinterpretation and fear-circuit models; medical and psychiatric differentials; PDSS and GAD-7; CBT with interoceptive and in-vivo exposure; SSRI/SNRI dosing; short-term benzodiazepines only; stepped care (WFSBP/BAP/NICE); special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Panic disorder and agoraphobia are high-yield general adult anxiety topics across FRANZCP, MRCPsych, ABPN and MD/DNB. Examiners test operational criteria, the medical differential, named psychological mechanisms (catastrophic misinterpretation, safety behaviours, inhibitory learning), stepped care with agent, dose and duration, and why chronic benzodiazepines fail the fellowship standard of care.[16][17][19]
Overview and definition
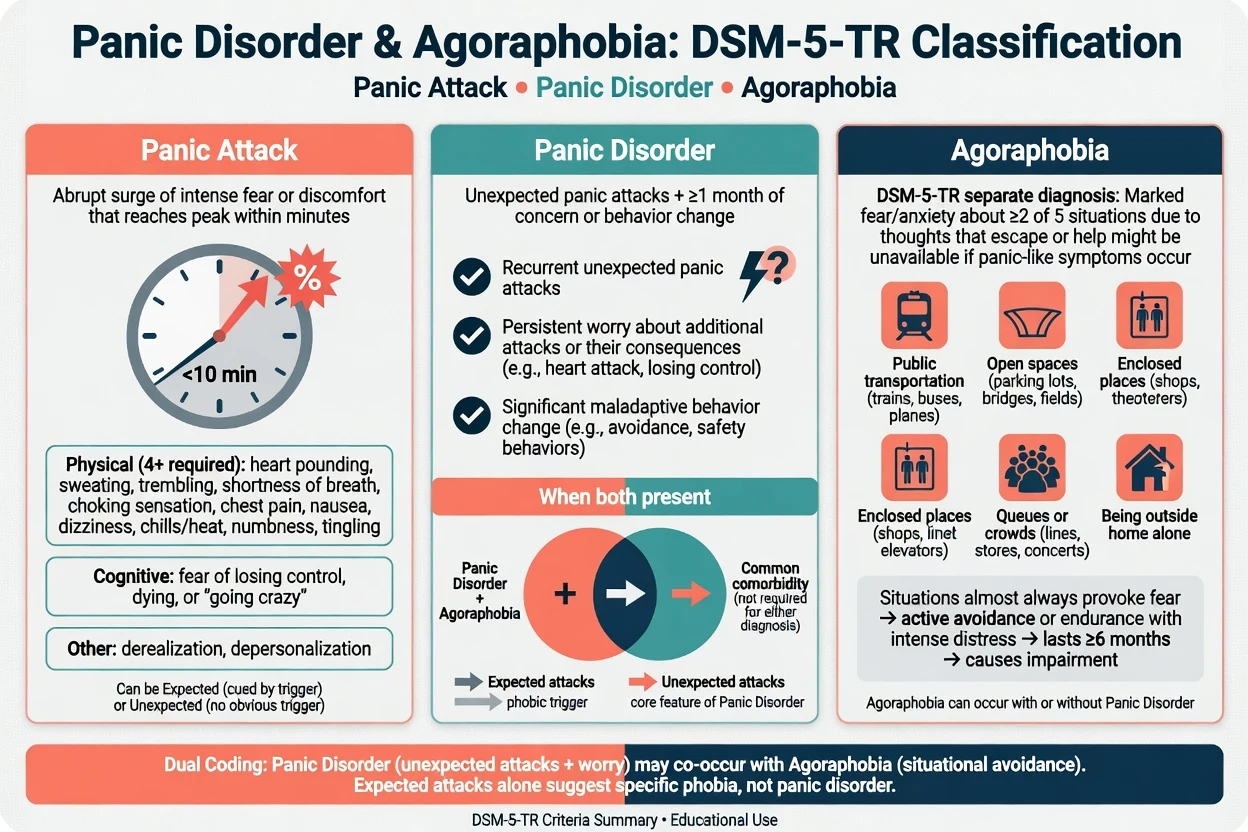
A panic attack is an abrupt surge of intense fear or intense discomfort that reaches a peak within minutes, during which a characteristic cluster of symptoms occurs (classic DSM-5-TR list of thirteen domains: palpitations/accelerated heart rate; sweating; trembling/shaking; shortness of breath or smothering; feelings of choking; chest pain or discomfort; nausea or abdominal distress; dizziness/unsteadiness/light-headedness/faintness; chills or heat sensations; paraesthesias; derealisation or depersonalisation; fear of losing control or "going crazy"; fear of dying). Attacks may be unexpected (out of the blue) or expected (cued by a phobic stimulus). A panic attack is a specifier and building block, not a freestanding disorder by itself.[19]
Panic disorder requires recurrent unexpected panic attacks plus, for at least one month, either persistent concern/worry about additional attacks or their consequences, and/or a significant maladaptive change in behaviour related to the attacks (for example avoidance of exercise, unfamiliar places, or being alone). The disturbance is not attributable to a substance or another medical condition and is not better explained by another mental disorder that better accounts for the attacks (for example social anxiety only in performance situations, specific phobia only with the phobic object, PTSD only with trauma cues).[1][19]
Agoraphobia in DSM-5-TR is a separate diagnosis. Marked fear or anxiety about two or more of five situation groups: using public transport; being in open spaces; being in enclosed places; standing in line or being in a crowd; being outside of the home alone. The individual fears or avoids these situations because of thoughts that escape might be difficult or help unavailable if panic-like, incapacitating, or embarrassing symptoms develop. Situations almost always provoke fear, are actively avoided or endured with intense fear, are out of proportion, persistent (typically six months or more in criterion language), and cause impairment. Agoraphobia may occur with or without panic disorder; when both are present, both are coded.[1][24]
ICD-11 also recognises panic disorder and agoraphobia as distinct entities. State which manual you are using when duration thresholds or dual-coding language is examined. Cross-national survey work shows that DSM-5-style freestanding agoraphobia captures a meaningful clinical population that older DSM-IV framing (agoraphobia mainly as a panic-linked qualifier) under-emphasised.[24]
Classification
Panic attack
- Abrupt peak within minutes
- Expected or unexpected
- Not a freestanding diagnosis
- Can occur in many disorders
Panic disorder
- Recurrent unexpected attacks
- ≥1 month concern or behaviour change
- Not better explained by other anxiety/trauma disorders
- High ED and medical work-up use
Agoraphobia
- ≥2 of 5 situation clusters
- Fear escape/help unavailable
- Avoidance or endurance with distress
- May occur without panic disorder
Exam traps
- Calling every attack 'panic disorder'
- Treating agoraphobia as only a panic subtype
- Missing substance/medical attribution
- Ignoring comorbidity that drives course
Classification axes matter for dual coding and treatment planning.[1][24]
Epidemiology and risk factors
Headline epidemiology for exams
Headline epidemiology for exams is anchored to NCS-R-style community surveys and long-term course data.[1][2][20]
The National Comorbidity Survey Replication quantified lifetime and 12-month prevalence of panic attacks, panic disorder, and agoraphobia and documented substantial comorbidity and role impairment.[1] Broader US survey work on lifetime morbid risk of anxiety and mood disorders reinforces that anxiety disorders are common, early-onset, and frequently untreated for long periods.[2]
Risk factors include family history of anxiety/panic, anxiety sensitivity (fear of anxiety symptoms themselves), behavioural inhibition, childhood adversity, respiratory illness history, major stressors, and substance use (especially stimulants, high-dose caffeine, cannabis in susceptible people). Female sex associates with higher community prevalence; suicide risk rises sharply when major depression coexists.[1][19][20]
Pathophysiology
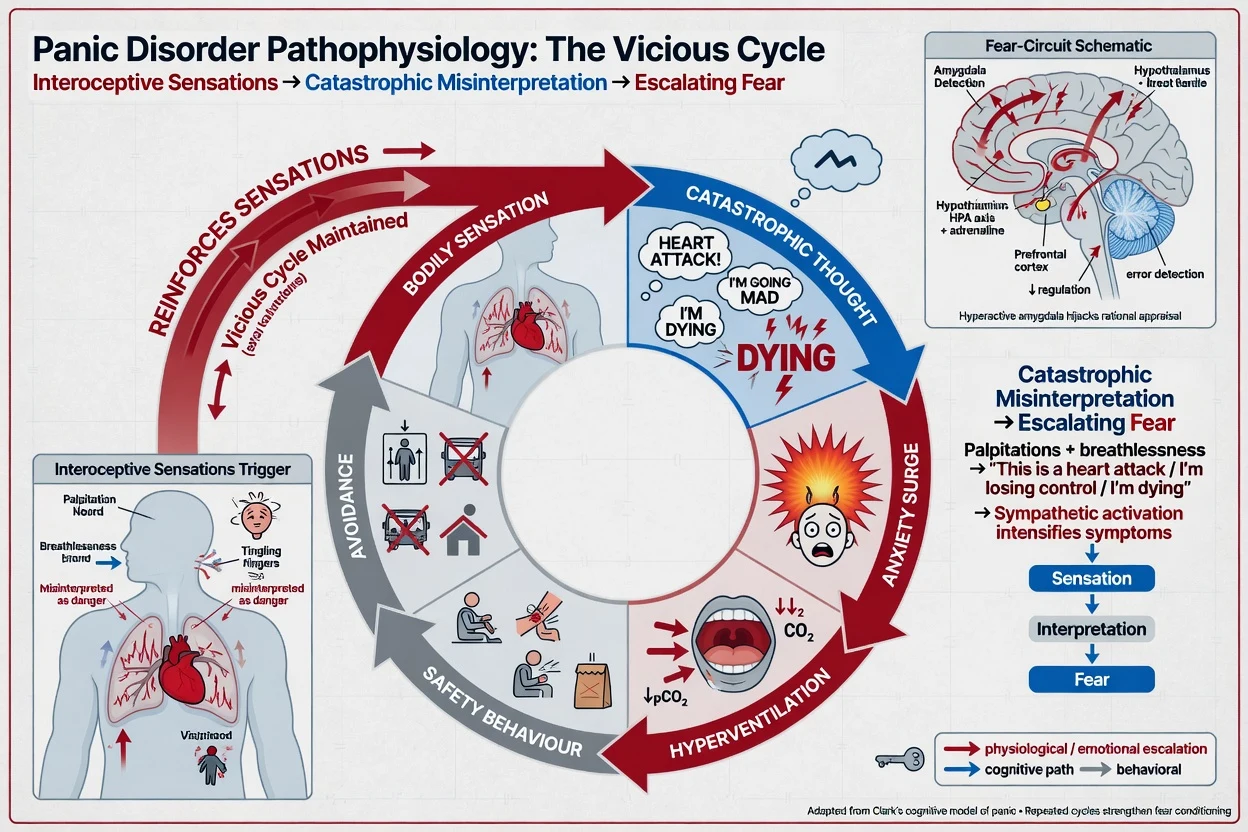
Cognitive model (Clark). Benign interoceptive sensations (palpitations, breathlessness, dizziness) are misinterpreted as evidence of imminent catastrophe (heart attack, suffocation, "going mad," dying). The resulting surge of fear amplifies autonomic arousal, generating more sensations and a vicious cycle. Safety behaviours (sitting near exits, carrying "rescue" medication without plan, checking pulse repeatedly, only going out with a partner) prevent disconfirmation of the catastrophic belief.[4][19]
Fear-circuit framing. Amygdala-centred threat detection, brainstem autonomic efferents, and interoceptive afferent pathways provide a neurobiological scaffold for the "false alarm." Group-level findings of CO2/lactate sensitivity are research anchors, not bedside diagnostic tests.[19]
Learning and maintenance. Interoceptive conditioning links internal cues to panic; situational conditioning generalises to agoraphobic contexts. Exposure works best when designed to build inhibitory learning (expectancy violation, varied contexts, removal of safety signals) rather than mere anxiety reduction within session.[23]
Pharmacology anchors. SSRIs/SNRIs modulate serotonergic (and for SNRIs noradrenergic) circuits relevant to threat processing and anticipatory anxiety; benzodiazepines potentiate GABA-A for rapid anxiolysis but risk dependence and may interfere with exposure-based learning if used as perpetual safety behaviours.[6][14][16]
Clinical presentation
Core attack phenomena: sudden cardiorespiratory and autonomic surge, neurological sensory symptoms, and catastrophic cognitions. Between attacks, anticipatory anxiety and situational avoidance dominate function. Patients often describe "I thought I was dying," "I could not get enough air," or "I had to leave the supermarket." MSE should quote these appraisals and map the avoidance radius (from mild queue discomfort to housebound).[1][19]
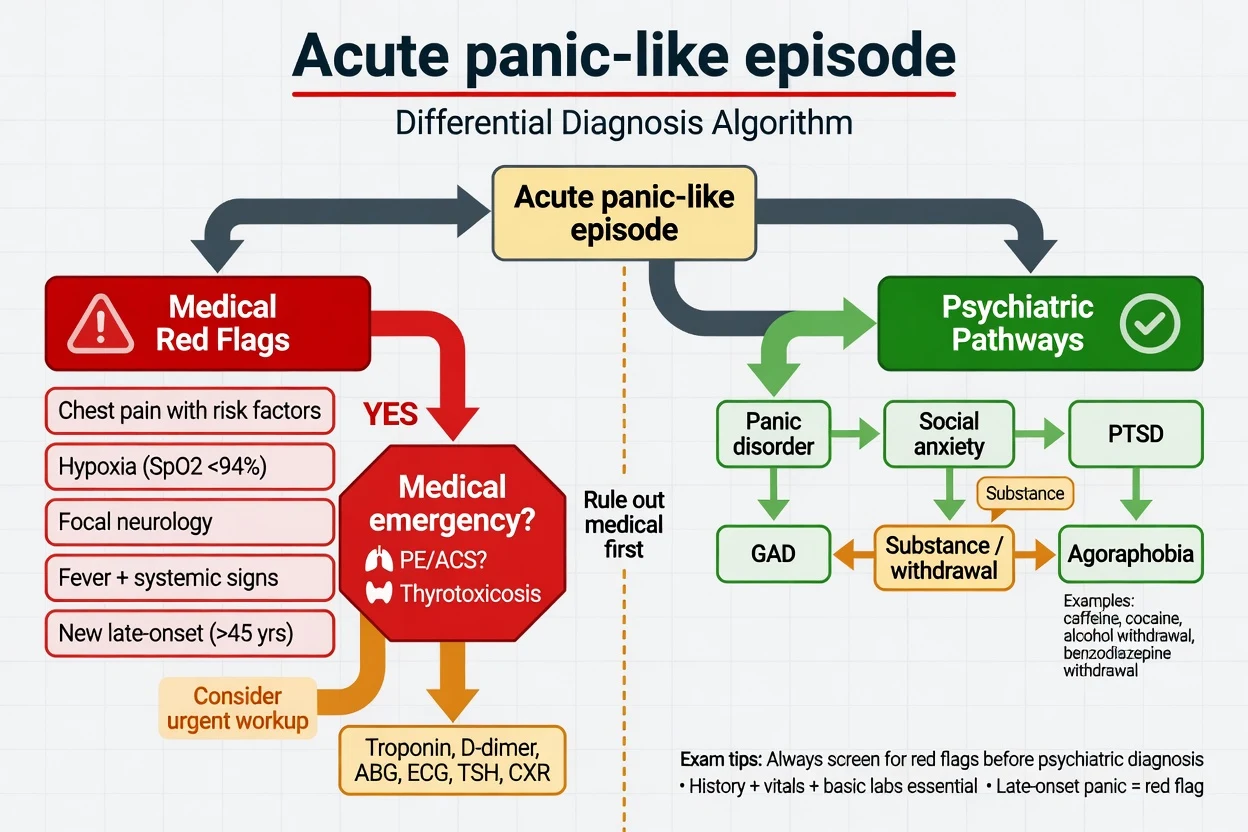
Nocturnal panic, limited-symptom attacks, and panic triggered by medical procedures (MRI, dental work, flying) are common exam variants. Late-life first onset, weight loss, fever, syncope with injury, or true exertional chest pain shift the work-up toward medical disease.[19]
Differential diagnosis
Medical can't-miss
- ACS, arrhythmia, PE
- Asthma/COPD flare, anaphylaxis
- Thyrotoxicosis, hypoglycaemia
- Substance intoxication/withdrawal
- Rare: phaeochromocytoma, seizure
Other anxiety
- Social anxiety: scrutiny/performance focus
- Specific phobia: narrow cue
- GAD: free-floating worry, not discrete unexpected clusters
- PTSD: trauma-cued hyperarousal
Mood / other psych
- MDD with panic attacks (common comorbidity)
- OCD: obsessional content drives rituals
- Illness anxiety / somatic symptom disorder
- Psychosis with panic-like distress
Discriminators
- Unexpectedness and inter-attack worry → panic disorder
- Situation map and escape fear → agoraphobia
- Timeline locked to substance → induced
- Focal neurology/hypoxia → medical first
Medical and psychiatric differentials must be stated with discriminators, not laundry lists.[16][19]
Clinical and bedside assessment
Structure the history: first attack (context, unexpectedness), peak symptoms, frequency, inter-attack worry, behaviour change, full avoidance map and safety behaviours, caffeine/substances, medical work-ups already completed, trauma screen, depression and suicide risk, family history, function (work, parenting, driving, public transport).[10][19]
MSE: fear/shame affect, catastrophic cognitions, insight (often good between attacks), risk. Capacity is usually intact for mild–moderate outpatient panic; reassess if severe depression, psychosis, or cognitive impairment coexists. Involuntary care uses local Mental Health Act principles when risk and capacity thresholds are met — do not invent section numbers for the wrong jurisdiction.[19]
PDSS (Panic Disorder Severity Scale). Clinician-rated severity across panic frequency, distress, anticipatory anxiety, agoraphobic fear/avoidance, interoceptive fear/avoidance, and occupational/social impairment — useful for baseline and response tracking in specialty care and trials.[22]
GAD-7. Brief self-report anxiety severity screen validated in primary care; elevated scores flag anxiety burden but do not diagnose panic disorder specifically. Use alongside clinical interview.[21]
Investigations
Targeted, not endless. For a first or atypical presentation: vital signs, ECG when cardiac symptoms or risk factors, capillary glucose, consider TSH, FBC, U&E; toxicology when substance contribution is plausible; pregnancy test when relevant. Escalate imaging or advanced labs only for red flags (hypoxia, focal neurology, high pretest probability of PE/ACS, systemic illness). Before antidepressants: baseline labs as for any SSRI/SNRI start; ECG when cardiac risk, older age, TCA planned, or high-dose citalopram/escitalopram context.[6][18]
Do not order diagnostic brain MRI for classic recurrent panic without neurological red flags.[19]
Management — acute / emergency
Arrange urgent mental health follow-up, provide a written crisis plan, address comorbid depression/suicide risk, and avoid reinforcing the idea that only emergency departments can keep the patient safe. Benzodiazepine withdrawal can itself produce panic-like states and requires medical management of withdrawal, not another open-ended as-needed script without a plan.[9][14]
Management — definitive and stepwise
Stepped care principles
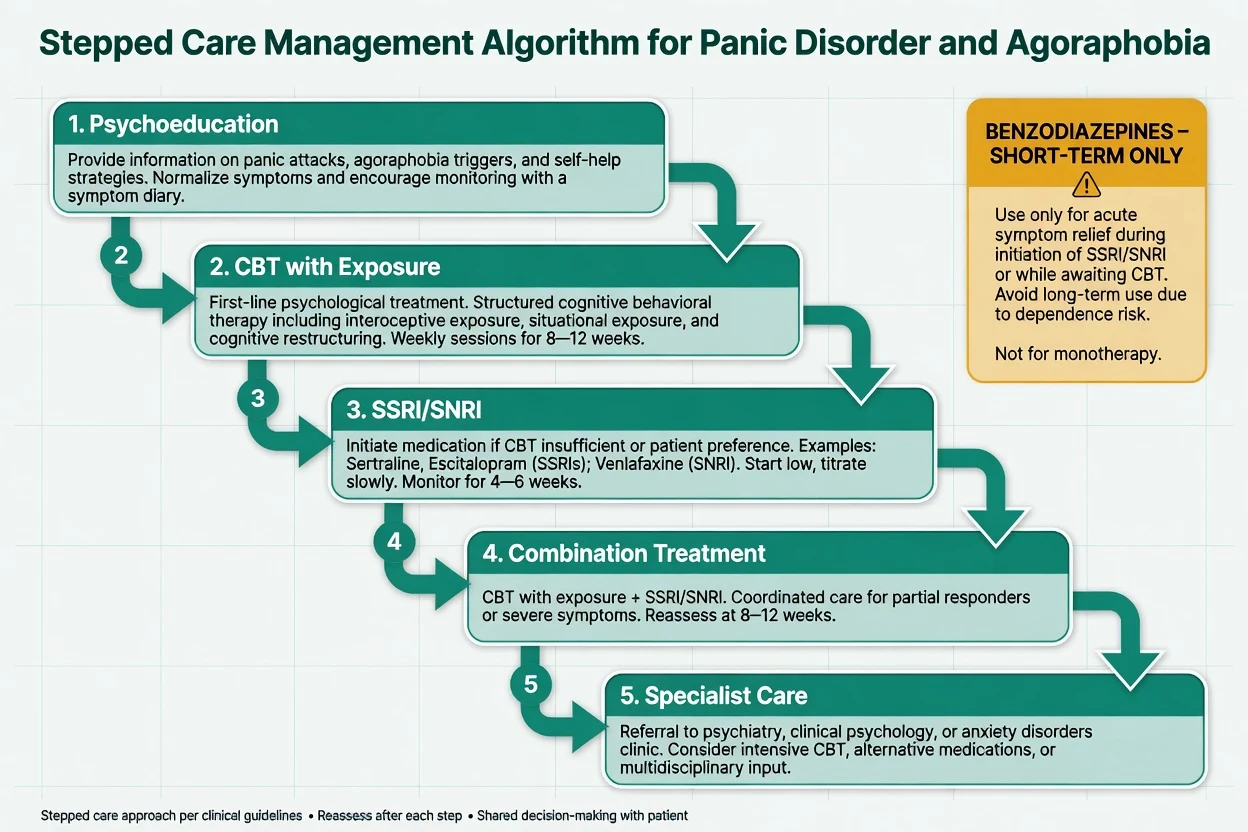
Psychoeducation and guided self-help for mild presentations with active monitoring; formal CBT with exposure as first-line psychological therapy; SSRI or SNRI as first-line pharmacotherapy when medication is preferred, severity is moderate–severe, or psychology access is delayed; combination for incomplete response or high severity; specialist escalation for treatment resistance, complex comorbidity, or severe agoraphobia needing intensive programmes.[12][16][17]
FRANZCP-facing practice aligns with international evidence: formulation-driven care, CBT access where possible, SSRI/SNRI pharmacotherapy with shared decision-making, and avoidance of long-term benzodiazepine monotherapy for panic. Local service models (GP shared care, private psychology, community mental health) determine delivery, not the evidence hierarchy itself.[16][17]
Psychological therapy — what to name in a viva
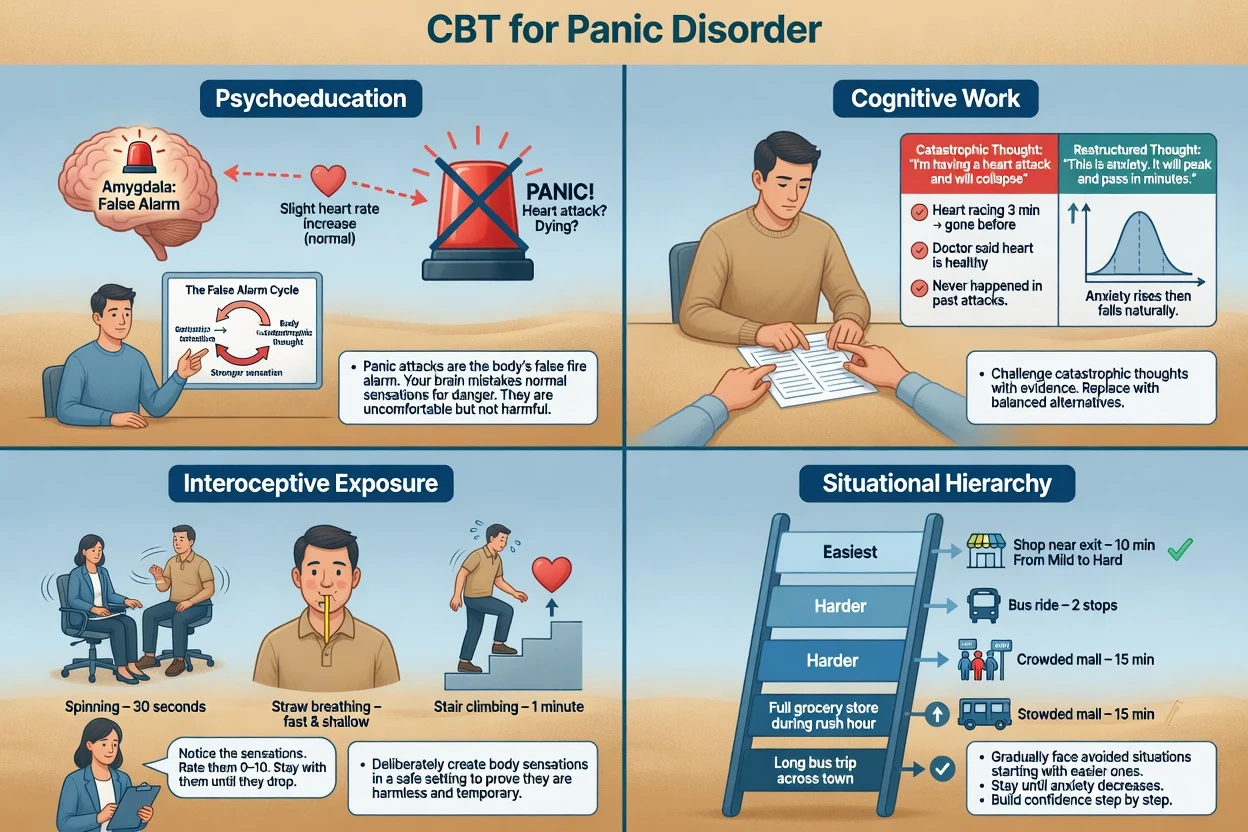
Core CBT package for panic: (1) psychoeducation of the false-alarm / vicious-cycle model; (2) cognitive restructuring of catastrophic misinterpretations; (3) interoceptive exposure (e.g. hyperventilation exercises, spinning, straw breathing, stair climbing) to break fear of bodily sensations; (4) in-vivo situational exposure along a graded hierarchy for agoraphobic avoidance; (5) elimination of safety behaviours; (6) relapse prevention.[4][11][12][23]
Landmark evidence: Clark and colleagues showed cognitive therapy highly effective versus applied relaxation and imipramine comparisons in classic trial work.[4] Barlow and colleagues' multicentre RCT found CBT and imipramine both effective acutely; combination helped some acute outcomes, with important maintenance lessons after treatment discontinuation.[3] Meta-analyses and Cochrane network meta-analysis support psychological therapies (especially exposure-based CBT packages) for panic with or without agoraphobia.[11][12] Primary-care collaborative care models delivering CBT elements plus medication management improve real-world outcomes versus usual care.[10]
Pharmacotherapy — agent, dose, monitoring
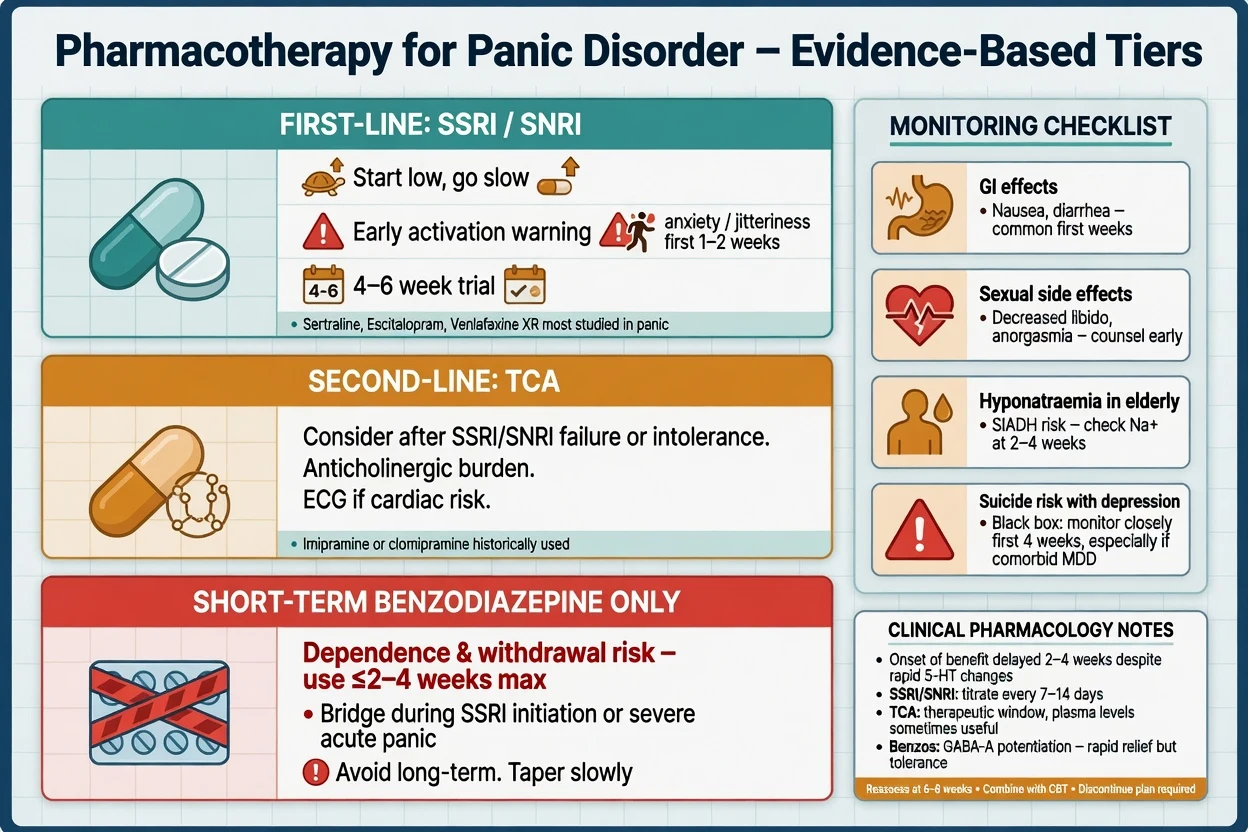
Antidepressants outperform placebo for panic disorder in Cochrane review; network meta-analysis of pharmacological options informs relative positioning without licensing every agent equally in every region.[13][15] SSRIs are generally preferred over TCAs for tolerability despite similar efficacy in meta-analytic comparisons.[5][6]
| Agent (class) | Typical adult start (panic) | Common therapeutic range | Key notes |
|---|---|---|---|
| Sertraline (SSRI) | 25–50 mg orally daily | 50–200 mg daily | Strong trial base; often start 25 mg if highly activation-sensitive |
| Escitalopram (SSRI) | 5–10 mg orally daily | 10–20 mg daily | QTc caution at higher doses; hyponatraemia risk in elderly |
| Paroxetine (SSRI) | 10 mg orally daily | 20–60 mg daily | Effective but more discontinuation symptoms and anticholinergic feel |
| Fluoxetine (SSRI) | 10 mg orally daily | 20–60 mg daily | Long half-life; activating for some |
| Venlafaxine XR (SNRI) | 37.5–75 mg orally daily | 75–225 mg daily | BP monitoring; useful SNRI option |
| Imipramine (TCA) | 10–25 mg orally daily | often titrated toward 100–300 mg under specialist caution | Classic efficacy (Barlow/Clark era); toxicity in overdose; ECG |
| Doses are typical adult exam anchors; individualise for age, hepatic/renal function, interactions, pregnancy, and local product information.[6][7][18] |
Sertraline exemplars. Flexible-dose multicentre trial evidence supports efficacy in panic disorder; long-term data support continuation after acute response.[7][8]
Adequate trial. Therapeutic dose, roughly 4–6 weeks or longer at that dose (full panic freeness may lag), verified adherence, substances addressed, exposure work underway when possible — then decide switch versus optimise versus combine.[6][13][18]
Benzodiazepines — short-term only. Cochrane review shows benzodiazepines beat placebo acutely for panic, but dependence, sedation, falls, cognitive effects, and interference with exposure learning limit their role. Exam answer: bridge during SSRI initiation or for severe acute crises, time-limited (often days to a few weeks), with a written taper plan — not indefinite daily monotherapy.[14][16][18] Example short-term agents used in practice (region-dependent): alprazolam or clonazepam in divided doses for brief bridging — name dependence risk explicitly. CBT improves successful benzodiazepine discontinuation in panic patients.[9]
Maintenance. After remission, continue the effective antidepressant typically at least 6–12 months, longer if recurrent, severe, or highly comorbid; plan relapse prevention and graded return of avoided activities as functional outcomes.[8][16][18]
Specific subtypes and scenarios
Panic disorder without agoraphobia emphasises unexpected attacks and interoceptive fear; exposure still targets bodily sensations and residual situational fear.[1]
Panic disorder with agoraphobia (dual coding) needs both interoceptive work and a systematic situational hierarchy (transport, queues, open spaces, being alone).[1][24]
Primary agoraphobia without panic disorder still benefits from exposure-based CBT; do not withhold treatment because classic unexpected panic is absent.[24]
Panic with major depression is common; treat both, prioritise suicide risk, and expect slower recovery when comorbidity is high.[20]
Primary-care panic. Collaborative care with structured CBT elements and medication management outperforms usual care in effectiveness trials — relevant to FRANZCP rural/shared-care MEQs.[10]
Treatment-resistant panic. Re-check diagnosis (medical, substance, trauma, bipolarity), adherence, dose/duration, whether exposure actually occurred (not just "talking CBT"), safety behaviours, and alcohol/caffeine. Then switch antidepressant class, ensure high-quality CBT, or specialist intensive programmes — not endless benzodiazepine escalation.[6][16][17]
Complications and pitfalls
Prognosis and disposition
Many patients improve substantially with adequate CBT and/or SSRI/SNRI therapy, but residual symptoms and relapse are common, especially with psychiatric comorbidity over long-term follow-up.[3][20] Disposition ladder: GP with collaborative care; private or public psychology for CBT; community mental health for complex comorbidity; intensive community support for severe agoraphobia; inpatient care mainly for high suicide risk, inability to maintain safety, or severe mixed presentations — not for routine panic alone.[10][16]
Functional recovery targets: using public transport, shopping, returning to work, and reducing partner-as-safety-signal dependence — not only "panic-free weeks" on a diary.[22]
Special populations
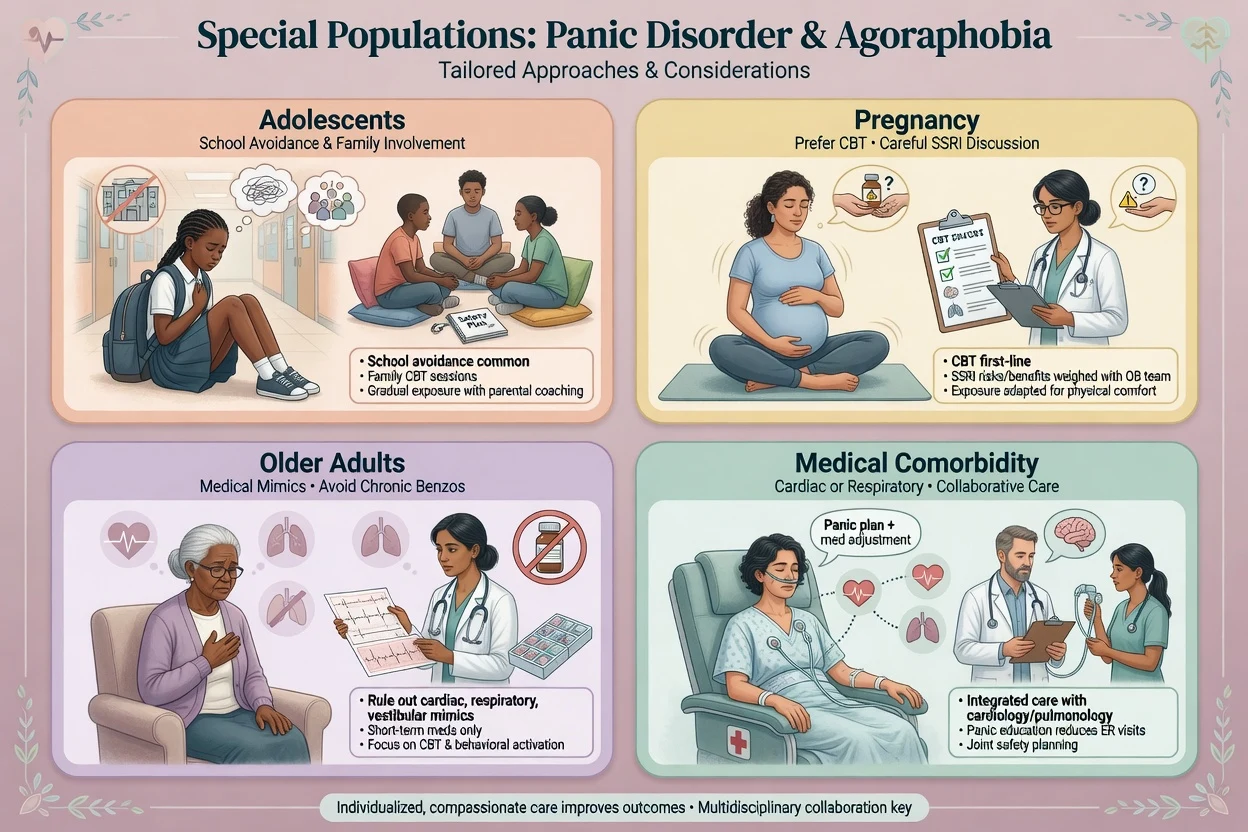
Adolescents
- School avoidance common
- Family involvement essential
- SSRI: start low, monitor activation
- Developmentally adapted CBT
Pregnancy / lactation
- Untreated severe panic/agoraphobia impairs function and care access
- Prefer CBT when accessible
- If medication needed, agents with more reproductive data (e.g. sertraline) often discussed
- Avoid initiating chronic benzos
Older adults
- Heavier medical differential
- Hyponatraemia, falls, polypharmacy on SSRIs
- Avoid chronic benzodiazepines
- Slower titration
Medical comorbidity
- Cardiac/respiratory disease: collaborative care
- Do not dismiss panic or miss real disease
- Psychoeducation reduces ED cycling
- Coordinate with physicians
Cultural formulation and FRANZCP cultural safety expectations apply: use interpreters, explore explanatory models, and avoid pathologising culturally normative distress while still treating impairing panic and avoidance.[16][19]
Evidence, guidelines and regional differences
Pillars for exams: Kessler NCS-R epidemiology of panic attacks, panic disorder, and agoraphobia;[1] Barlow 2000 JAMA CBT vs imipramine vs combination;[3] Clark 1994 cognitive therapy comparisons;[4] Bakker SSRI vs TCA meta-analysis and EBM pharmacotherapy reviews;[5][6] Pollack/Rapaport sertraline acute and long-term;[7][8] Otto CBT for benzodiazepine discontinuation;[9] Roy-Byrne primary-care effectiveness;[10] Sánchez-Meca and Pompoli Cochrane psychological meta-analyses;[11][12] Bighelli/Breilmann/Guaiana Cochrane antidepressant, benzodiazepine, and pharmacological network evidence;[13][14][15] Bandelow treatment reviews and WFSBP 2023 guidelines;[16][17] BAP 2014 Baldwin pharmacological guidance;[18] Craske and Stein Lancet anxiety overview and inhibitory learning exposure optimisation;[19][23] Bruce 12-year comorbidity and course;[20] PDSS and GAD-7 measurement tools;[21][22] Roest DSM-5 vs DSM-IV agoraphobia in World Mental Health Surveys.[24]
Controversies to handle calmly: how long benzodiazepine bridging is ever justified; combination CBT+drug versus sequential stepped care; and when "treatment resistance" is actually pseudo-resistance (no real exposure, subtherapeutic SSRI, ongoing cannabis).[3][14][17]
Exam pearls
PANICS
PANICS is a memory scaffold — still apply full operational criteria and medical exclusion.[4][19]
Self-test: what is wrong with 'diazepam 5 mg three times daily ongoing' as sole therapy for new panic disorder?
It may blunt acute anxiety but risks dependence, cognitive/falls harms, and can become a safety behaviour that blocks exposure-based recovery. Fellowship-standard care uses psychoeducation, CBT with exposure, and/or an SSRI/SNRI with an adequate trial, reserving benzodiazepines for short-term bridging with a taper plan.[9][14][16]
References
- [1]Kessler RC, Chiu WT, Jin R, Ruscio AM, et al. The epidemiology of panic attacks, panic disorder, and agoraphobia in the National Comorbidity Survey Replication Arch Gen Psychiatry, 2006.PMID 16585471
- [2]Kessler RC, Petukhova M, Sampson NA, et al. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States Int J Methods Psychiatr Res, 2012.PMID 22865617
- [3]Barlow DH, Gorman JM, Shear MK, Woods SW Cognitive-behavioral therapy, imipramine, or their combination for panic disorder: A randomized controlled trial JAMA, 2000.PMID 10815116
- [4]Clark DM, Salkovskis PM, Hackmann A, Middleton H, et al. A comparison of cognitive therapy, applied relaxation and imipramine in the treatment of panic disorder Br J Psychiatry, 1994.PMID 7952982
- [5]Bakker A, van Balkom AJ, Spinhoven P SSRIs vs. TCAs in the treatment of panic disorder: a meta-analysis Acta Psychiatr Scand, 2002.PMID 12197851
- [6]Bakker A, van Balkom AJ, Stein DJ Evidence-based pharmacotherapy of panic disorder Int J Neuropsychopharmacol, 2005.PMID 15804373
- [7]Pollack MH, Otto MW, Worthington JJ, Manfro GG, et al. Sertraline in the treatment of panic disorder: a flexible-dose multicenter trial Arch Gen Psychiatry, 1998.PMID 9819070
- [8]Rapaport MH, Wolkow R, Rubin A, Hackett E, et al. Sertraline treatment of panic disorder: results of a long-term study Acta Psychiatr Scand, 2001.PMID 11722304
- [9]Otto MW, Pollack MH, Sachs GS, Reiter SR, et al. Discontinuation of benzodiazepine treatment: efficacy of cognitive-behavioral therapy for patients with panic disorder Am J Psychiatry, 1993.PMID 8379551
- [10]Roy-Byrne PP, Craske MG, Stein MB, Sullivan G, et al. A randomized effectiveness trial of cognitive-behavioral therapy and medication for primary care panic disorder Arch Gen Psychiatry, 2005.PMID 15753242
- [11]Sánchez-Meca J, Rosa-Alcázar AI, Marín-Martínez F, Gómez-Conesa A Psychological treatment of panic disorder with or without agoraphobia: a meta-analysis Clin Psychol Rev, 2010.PMID 19775792
- [12]Pompoli A, Furukawa TA, Imai H, Tajika A, et al. Psychological therapies for panic disorder with or without agoraphobia in adults: a network meta-analysis Cochrane Database Syst Rev, 2016.PMID 27071857
- [13]Bighelli I, Castellazzi M, Cipriani A, Girlanda F, et al. Antidepressants versus placebo for panic disorder in adults Cochrane Database Syst Rev, 2018.PMID 29620793
- [14]Breilmann J, Girlanda F, Guaiana G, Barbui C, et al. Benzodiazepines versus placebo for panic disorder in adults Cochrane Database Syst Rev, 2019.PMID 30921478
- [15]Guaiana G, Meader N, Barbui C, Davies SJ, et al. Pharmacological treatments in panic disorder in adults: a network meta-analysis Cochrane Database Syst Rev, 2023.PMID 38014714
- [16]Bandelow B, Michaelis S, Wedekind D Treatment of anxiety disorders Dialogues Clin Neurosci, 2017.PMID 28867934
- [17]Bandelow B, Allgulander C, Baldwin DS, Costa DLDC, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for treatment of anxiety, obsessive-compulsive and posttraumatic stress disorders - Version 3 World J Biol Psychiatry, 2023.PMID 35900161
- [18]Baldwin DS, Anderson IM, Nutt DJ, Allgulander C, et al. Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive-compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology J Psychopharmacol, 2014.PMID 24713617
- [19]Craske MG, Stein MB Anxiety Lancet, 2016.PMID 27349358
- [20]Bruce SE, Yonkers KA, Otto MW, Eisen JL, et al. Influence of psychiatric comorbidity on recovery and recurrence in generalized anxiety disorder, social phobia, and panic disorder: a 12-year prospective study Am J Psychiatry, 2005.PMID 15930067
- [21]Spitzer RL, Kroenke K, Williams JB, Löwe B A brief measure for assessing generalized anxiety disorder: the GAD-7 Arch Intern Med, 2006.PMID 16717171
- [22]Shear MK, Brown TA, Barlow DH, Money R, et al. Multicenter collaborative panic disorder severity scale Am J Psychiatry, 1997.PMID 9356566
- [23]Craske MG, Treanor M, Conway CC, Zbozinek T, et al. Maximizing exposure therapy: an inhibitory learning approach Behav Res Ther, 2014.PMID 24864005
- [24]Roest AM, de Vries YA, Lim CCW, Wittchen HU, et al. A comparison of DSM-5 and DSM-IV agoraphobia in the World Mental Health Surveys Depress Anxiety, 2019.PMID 30726581